
Abstract
Macrocephaly-capillary malformation syndrome is characterized by cutaneous vascular malformations with associated anomalies as macrocephaly, macrosomia, hemihypertrophy, hypotonia, developmental delay, lax joints, loose skin, polysyndactyly, and neuroimaging abnormalities. We present a newborn with a prenatal diagnosis of macrosomia and tetralogy of Fallot. He also had macrocephaly; a high forehead; capillary hemangioma on the forehead, upper lip, and philtrum; generalized loose skin; postaxial polydactyly of both hands and feet, with neuroimaging findings of polymicrogyria and thrombosis in sagittal sinus and sinus rectus. His condition was diagnosed as macrocephaly-capillary malformation syndrome in the neonatal period and he died suddenly during sleep at 6 months of age. The clinical course in this syndrome is not as benign as was previously thought. Careful follow-up of these patients with particular emphasis on neuroradiologic and cardiologic evaluation might help decrease the risk of sudden death and to improve long-term outcome.
Keywords
Macrocephaly-capillary malformation syndrome is a well-known syndrome that was first reported independently by Moore et al 1 and Clayton-Smith et al 2 in 1997. This syndrome traditionally has been called macrocephaly-cutis marmorata telangiectatica congenita because the syndrome was characterized by cutaneous vascular malformations, including cutis marmorata telangiectatica congenita and hemangiomas with associated anomalies, such as macrocephaly, macrosomia, hemihypertrophy, frontal bossing, hypotonia, developmental delay, lax joints, loose skin, polysyndactyly, and neuroimaging abnormalities. However, recently Toriello and Mulliken 3 renamed the disorder as macrocephaly-capillary malformation because the vascular lesions in this syndrome as they proposed are neither cutis marmorata nor cutis marmorata telangiectatica congenita. The lesions are patchy and reticular, representing a capillary malformation that mostly occurs on the nose and philtrum and can be scattered over the limbs and trunk. 3
Macrocephaly-capillary malformation syndrome has been reviewed regarding its more and less frequent general findings and brain and neuroimaging abnormalities. 4,5 Heart malformations have been reported to be seen infrequently. 4 The presence of tetralogy of Fallot has been described in only 1 patient so far in the report of Duenas-Arias et al. 6 Venous thrombosis and cerebral arterial vascular accidents have also been reported infrequently by some authors. 1,2,5,7,8 We present a newborn with the diagnosis of macrocephaly-capillary malformation syndrome and tetralogy of Fallot who also had a sagittal sinus thrombosis on initial magnetic resonance imaging (MRI).
Case Summary
The boy was born as the first child to a nonconsanguineous Turkish couple at 36 weeks’ gestation by cesarean section. The family history was unremarkable. Fetal macrosomia and tetralogy of Fallot were detected by prenatal ultrasound. His apgar scores were 3 and 5 at the first and fifth minute, respectively. He was admitted to the neonatal intensive care unit because of tachypneic breathing and minimal respiratory distress.
His birth weight was 4160 g (>97th centile), birth length 50 cm (90th centile), and occipitofrontal circumference 41 cm (>97th centile, +7.3 SD). He was hypotonic. He had macrocephaly and atypical facies with a high forehead; a broad depressed nasal bridge; hypertelorism; and capillary hemangioma on the forehead, upper lip, and philtrum (Figure 1A). Other clinical findings included generalized loose skin especially prominent in the axillary regions and around the knees, with numerous skin folds of subcutaneous tissue, high arched palate, and postaxial polydactyly of both hands and feet (Figure 1B-F). Neither cutis marmorata nor cutis marmorata telangiectatica congenita was noted over the body.

(A) Newborn boy with macrocephaly-capillary malformation syndrome. Macrocephaly, a high forehead, a broad depressed nasal bridge, hypertelorism, capillary hemangioma on the forehead, upper lip, and philtrum. (B) Generalized loose skin, especially prominent in axillary regions and around knees with numerous skin folds of subcutaneous tissue around knees and axilla. (C, D) Postaxial polydactyly of both hands. (E, F) Postaxial polydactyly of both feet.
Chest radiograph performed because of his respiratory distress was unremarkable. He was given oxygen therapy by hood. Postnatal echocardiography revealed tetralogy of Fallot, atrial septal aneurysm, and minimal aortic regurgitation. He was given orogastric feedings until the sixth postnatal day because of feeding difficulties, after which he was bottle-fed. His abdominal ultrasonography was normal. The karyotype was normal, with 46,XY. On cranial MRI performed at age 35 days, cavum septum pellucidum; cavum vergae; polymicrogyria in the frontal operculum, insular and temporal regions; and total thrombosis of the superior sagittal sinus and sinus rectus were detected (Figure 2A-D). His condition was diagnosed as macrocephaly-capillary malformation syndrome based on the characteristic physical findings and neuroimaging abnormalities. He was given enoxaparin therapy for his venous sinus thrombosis. His repeat cranial MRI at age 47 days revealed a regression of the thrombosis, and he was discharged at age 47 days on enoxaparin therapy.
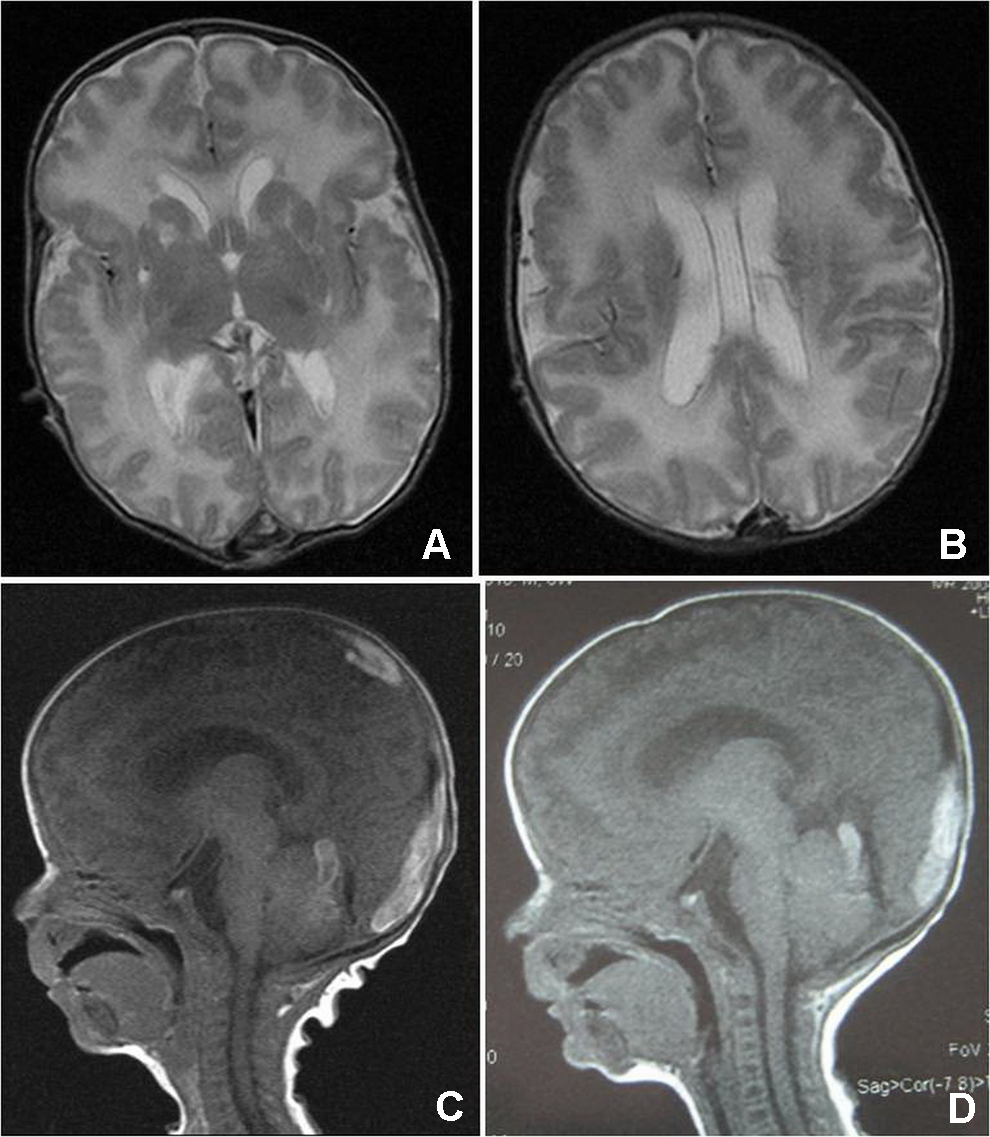
(A) Axial T2-weighted image shows bilateral symmetric perisylvian polymicrogyria and shallow sulci. (B) Axial T2- weighted, more caudad section image shows cavum septum pellucidum and vergae. (C) Sagittal T1- weighted image showing hyperintense thrombosis within the superior sagittal sinus. (D) Regression of the thrombosis within the superior sagittal sinus.
His neuromotor development was delayed with no head control until 6 months of age, and he died suddenly during sleep at 6 months of age.
Discussion
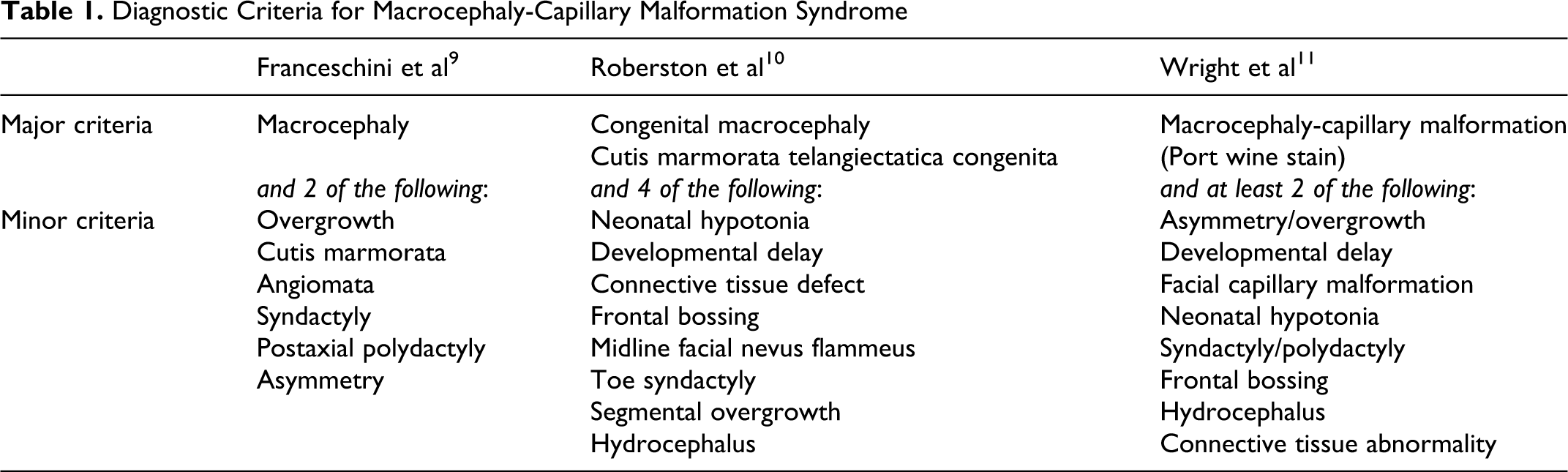
The diagnostic criteria for macrocephaly-capillary malformation syndrome (MCM) were proposed by Franceschini et al, 9 Robertson et al, 10 and Wright et al, 11 who recently have revised the clinical criteria (Table 1). The patient presented here had the typical clinical features consistent with macrocephaly-capillary malformation syndrome satisfying the diagnostic criteria proposed by Franceschini et al 9 and Wright et al 11 with regard to major and minor criteria. But he did not completely satisfy the major criteria proposed by Robertson et al, 10 since he had neither cutis marmorata nor cutis marmorata telangiectatica congenita. Only a capillary malformation was noted over the forehead, upper lip, and philtrum. One of the cases in the report of Franceschini et al 9 and 2 of 17 patients in the cohort of Conway et al 5 had only capillary hemangiomas on the philtrum and upper lip without any cutis marmorata as in our patient. Robertson’s criteria 10 are more specific and restrictive, making the diagnosis less definitive in a group of patients whose condition would be otherwise diagnosed as macrocephaly-capillary malformation syndrome.
Diagnostic Criteria for Macrocephaly-Capillary Malformation Syndrome
In addition to the proposed clinical criteria, there are also associated anomalies reported in macrocephaly-capillary malformation syndrome among which complex cardiac malformations have been reported less frequently. 2,4,8,12 Duenas-Arias et al 6 presented the first documented case of macrocephaly-capillary malformation syndrome with tetralogy of Fallot in a newborn girl who died suddenly in infancy. In our patient, tetralogy of Fallot was also detected with other defects, namely, atrial septal aneurysm and minimal aortic regurgitation.
Macrocephaly-capillary malformation syndrome also has a certain central nervous system phenotype that helps support the clinical diagnosis of the syndrome in addition to its recognizable clinical phenotype. 5 In fact, Conway et al 5 proposed that a completely normal neuroimaging study in a suspected macrocephaly-capillary malformation syndrome case should prompt the clinician to reassess the diagnosis. In our patient, typical MRI findings were polymicrogyria, which was prominent in the frontal, temporal, and insular region; cavum septum pellucidum and cavum vergae; and thrombosis of the superior sagittal sinus and sinus rectus. In the cohort of Conway et al, 5 central nervous system pathologies seen with a high frequency were brain asymmetry, polymicrogyria, and cortical dysgenesis, ventriculomegaly, white matter abnormalities with increased T2 signal, and cerebellar tonsil herniation. Commonly reported central nervous system findings in a literature review of 65 cases by Conway et al 5 were ventriculomegaly, cerebral asymmetry, increased white matter signal, and cerebellar tonsil herniation or Chiari 1. Only in a small number of patients with macrocephaly-capillary malformation syndrome, both venous sinus thrombosis and cerebral arterial vascular events have been reported. 1,2,5,7,8 Only 1 patient in a cohort of 17 patients in Conway’s report 5 and 2 patients in his review of 65 cases were found to have a venous sinus thrombosis.
Early and sudden deaths have also been reported in macrocephaly-capillary malformation syndrome. 2,6,8,13 Our patient died at 6 months of age during sleep without an identifiable cause. Although reported deaths could be attributed to congenital cardiac malformations and arrhythmia, cerebellar tonsil herniation that may be an acquired and progressive process, as proposed by Conway et al, could be a significant potential risk for sudden death due to brain stem compression. 5 Franklin et al 14 reported on a patient with macrocephaly-capillary malformation syndrome who had occasional apneic spells with MRI findings of left cerebellar tonsillar herniation, leading to full occlusion of the cisterna magna and a narrowed foramen magnum suggestive of cervicomedullary cord compression with a risk for sudden death. This patient also had unilateral hypertrophy of the vocal cords leading to airway obstruction. This finding in addition to brainstem compromise was reported as a potential underlying etiology of apnea in macrocephaly-capillary malformation syndrome patients presenting with signs and symptoms of cervicomedullary cord compression.
There are also reports of patients with macrocephaly-capillary malformation syndrome who survive with some motor and cognitive delay. 11,12,15,16
Since the first description of this syndrome in 1997, more than 130 cases have been reported. 16 Macrocephaly-capillary malformation syndrome seems to show a sporadic occurrence without an identifiable genetic cause, and the diagnosis is based on clinical findings.
In conclusion, the name “macrocephaly-capillary malformation” is a better terminology for this disorder. This syndrome should be included in the differential diagnosis of macrosomic newborns. A less restrictive set of criteria would be more appropriate to use to facilitate the diagnosis. The clinical course in this syndrome is not as benign as was previously thought. So, a careful follow-up of these patients with an emphasis on neuroradiologic and cardiologic evaluation might be helpful to decrease the risk of sudden death and to improve the long-term outcome of these patients.
Footnotes
Acknowledgment
The work was done in Istanbul University, Cerrahpasa Medical School, Department of Neonatology and Department of Pediatric Genetics.
Author Contributions
TEE and BT were the first authors who contributed equally to this work. TEE was the primary care physician of the presented case during the stay in the neonatal intensive care unit and contributed to the writing of the manuscript. BT was the leading physician who diagnosed the condition as macrocephaly-capillary malformation syndrome and contributed to the writing of the manuscript and was responsible in the development of the framework of the manuscript. FO was the physician who did the prenatal and postnatal echocardiography and contributed to the diagnosis of the patient. TC was the physician who contributed to the treatment of the patient during his hospital stay. MB was the physician who followed up the patient during his admission to the pediatric genetics department and contributed to the literature review of the macrocephaly-capillary malformation syndrome. OK and CI were mentors who contributed equally to this work. They contributed to the radiologic diagnosis of the patient and to the selection of magnetic resonance images of the patient during the preparation of the manuscript. MV and YP were mentors who contributed equally to this work. They were the physicians in charge of the neonatal intensive care unit and provided the support and mentorship during the preparation of the manuscript and proofread the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Informed consent of the parents of the presented case was taken before the preparation of this case report. All of the work meets the ethical guidelines.