
Abstract
West syndrome (infantile spasms) is an epileptic encephalopathy that includes psychomotor deterioration. In rare cases, it is due to an inherited, progressive metabolic disease. More than 25 inborn errors of metabolism have been considered etiologic or predisposing factors for infantile spasms. This is a review of the literature on reported cases of children diagnosed with a metabolic disease who developed infantile spasms. This article presents in brief the most frequent inborn errors of metabolism that have been associated with West syndrome and also illustrates the importance of screening for inborn errors of metabolism in infantile spasms.
Epilepsy is a frequent symptom in metabolic diseases, although it remains incompletely described in some of them. Myoclonus is the most frequent seizure type in children with metabolic diseases and often leads to metabolic investigations in newborns and infants. Infantile spasms are uncommonly reported in inborn metabolic disorders, but they are probably underestimated. More than 25 inborn errors of metabolism have been considered etiologic or predisposing factors for infantile spasms. They are mostly associated with conditions such as phenylketonuria (PKU), 1 pyruvate dehydrogenase complex (PDHC) deficiency, 2 or mitochondrial diseases. 3,4
In this review of the literature, we present the most frequent inborn errors of metabolism that have been associated with West syndrome and also, when available, the mechanism by which these diseases cause brain dysfunction. There is no such review in the literature, although there are many case reports of children diagnosed with metabolic disease and also presenting with infantile spasms. This review also illustrates the importance of screening for inborn errors of metabolism in seizure disorders, especially in those that do not respond adequately to antiepileptic treatment or have a poor prognosis.
West Syndrome
West syndrome, or infantile spasms, is an age-dependent epileptic syndrome, quite specific to infancy, frequently with poor prognosis. The incidence of West syndrome in Western countries has been estimated to be 0.24 to 0.42%. 5 It affects half the infants with severe epilepsy, 60% being boys. 6,7
Although the peak age of onset is in the middle of the first year of life, onset of West syndrome may be delayed to after the age of 1 year in 2% of the patients. 8 The disease combines features of a triad: sudden axial muscle contraction occurring in clusters, psychomotor delay or deterioration, and major diffuse paroxysmal activity on the electroencephalogram (EEG). Attacks of spasms are characterized by a series of sudden muscular contractions by which the head is flexed, arms are extended, and legs are drawn up. Less commonly, attacks include head nodding extensor spasms characterized by extension rather than flexion of arms, legs, and trunk. Rarely, the attacks are concluded by a brief clonic seizure. 9
In approximately 50% of children with West syndrome, infantile spasms will have ceased by 3 years of age. However, in a majority of children, infantile spasms are replaced by other seizure types, mainly by generalized tonic seizures with atypical absences combined with slow spike waves in electroencephalogram (Lennox-Gastaut syndrome). 10
According to the presence or absence of underlying pathology, West syndrome has been classified into 2 groups: cryptogenic and symptomatic. The etiology of West syndrome varies, with nonprogressive prenatal-perinatal lesions being the leading cause and a small proportion resulting from inborn errors of metabolism or brain tumors, usually benign. However, in more than 20% of the cases, no cause can be identified. 11 More than 25 inborn errors of metabolism have been considered etiologic or predisposing factors. Of the inborn errors of metabolism, Menkes disease is the condition that causes the highest incidence of infantile spasms; moreover, West syndrome affects most patients in the course of this disease. Other hereditary metabolic diseases such as phenylketonuria have been observed in some patients with symptomatic West syndrome. 12
Although the relationship between treatment regimens and outcome is controversial, hormonal therapy (with corticosteroids and adrenocorticotropic hormone), topiramate, zonisamide and vigabatrin are considered the treatment of choice. 13 The mainstay of treatment for infantile spasms is adrenocorticotropic hormone; however, vigabatrin (a vinyl derivative of γ-aminobutyric acid [GABA]) has been used for the treatment of infantile spasms in Europe since 1989. In 2009, vigabatrin was approved by the US Food and Drug Administration (FDA) for use as monotherapy in the treatment of infantile spasms for patients aged 1 month to 2 years when the benefits of treatment outweigh the risks. 14 Fifty-four percent of the experts chose adrenocorticotropic hormone as the treatment of choice. Topiramate, zonisamide, and vigabatrin were chosen by 18%, 13%, and 27% of the experts, respectively. Although adrenocorticotropic hormone and vigabatrin were both evaluated and rated as effective for short-term treatment of infantile spasms, there have been few large-scale randomized controlled trials to convincingly confirm their reported effectiveness. 15 Many regimens for adrenocorticotropic hormone treatment have been proposed. At higher adrenocorticotropic hormone doses, there is a greater proportion of remissions but also a higher incidence of major adverse reactions. One convenient treatment schedule follows: adrenocorticotropic hormone is given intramuscularly in a daily dose of 80 to120 U. This dose is maintained until spasms and hypsarrhythmia disappear. If a response is noted, the dose is changed to 40 to 80 U every other day and the n gradually reduced to half that dose. This is maintained for approximately 3 more months. Thereafter, the dosage is reduced further by 10 U at 2-month intervals until the drug is completely withdrawn or the minimal dosage for seizure control is reached. Side reactions to adrenocorticotropic hormone include hypertension, gastroenteritis, sepsis, osteoporosis, and unexplained central nervous system hemorrhage. 9,15
The prognosis of infantile spasms is generally poor, especially in symptomatic cases. In most children, the outlook for normal intellectual development is poor, even though in approximately 50%, infantile spasms have ceased by 3 years of age or are replaced by the Lennox-Gastaut syndrome or by major motor attacks. In children whose infantile spasms are attributed to tuberous sclerosis, the long-term prognosis is worse than in other symptomatic or cryptogenic cases of infantile spasms. By contrast, the prognosis is relatively good when infantile spasms accompany neurofibromatosis. Even with the advent of many new treatment strategies ranging from drug development to surgical intervention, West syndrome is still one of the most refractory epileptic syndromes. 9
Inborn Errors of Metabolism
Inborn errors of metabolism comprise a heterogeneous group of conditions that result from a single mutant gene which codes for an enzymatic protein that in most instances is involved in a catabolic pathway. The consequent homeostatic disturbances produce a neurologic or developmental abnormality. The mechanisms by which inborn errors of metabolism cause brain dysfunction remain uncertain, although for some conditions a theory of pathogenesis has been proposed.
The main groups of metabolic disorders that have been associated with West syndrome are the following: (1) disorders of amino acid metabolism (phenylketonuria, dihydropteridine reductase deficiency), (2) organic acidurias (
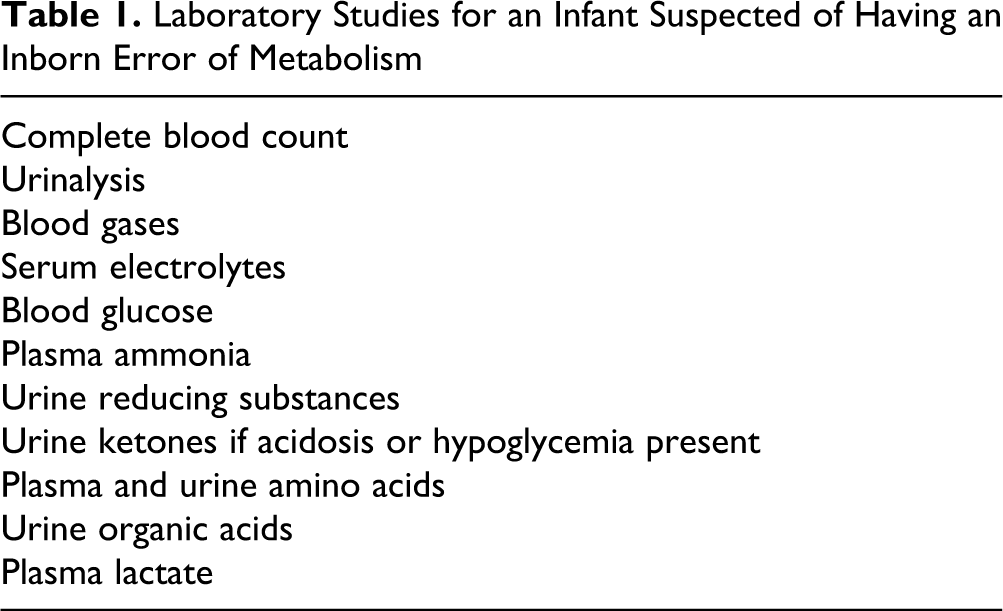
Laboratory Studies for an Infant Suspected of Having an Inborn Error of Metabolism
Neuroimaging techniques are essential for assessing brain structures. Neuroradiologic features of many inborn errors of metabolism overlap and are stage-dependent. Patients occasionally show distinctive patterns of central nervous system involvement in magnetic resonance imaging (MRI). These patterns may characterize some disorders, especially during the early stages. In later phases, the MRI findings are similar for most inborn errors of metabolism with neurologic involvement, often presenting diffuse loss of brain tissue and increased water in the remaining tissue. For this reason, it is important to take an MRI of the brain early in the course of the disease, when some key features will be more evident. According to brain MRI in early stages, inborn errors of metabolism can be classified into disorders primarily involving gray matter, those involving white matter, and those involving both gray and white matter. 16
Disorders of Amino Acid Metabolism
Phenylketonuria
The association of West syndrome with phenylketonuria has long been recognized in the literature since the first report by Low et al 17 in 1957. However, this association of phenylketonuria and West syndrome had scarcely been studied systematically based on a large number of patients, although there have been numerous short notes or case reports in the literature. 18 –22
The exact pathogenesis of West syndrome in children with phenylketonuria is not known, but the following factors have been considered to be relevant: (1) high serum level of phenylalanine influences microenvironment and molecular system maintaining normal brain function, (2) Hyperphenylalaninemia disturbs the other metabolic ways so as to change brain function. For example, inhibition of glutamate dehydrogenase reduces GABA synthesis. It was reported that GABA is apparently reduced in the cerebrospinal fluid of West syndrome patients. 5-Hydroxytryptamine (5-HT) synthesis is obstructed by inhibited tryptophan hydroxylase because of high phenylalanine, and a reduction of dopamine contributes to inhibit related enzymes. Reduction of γ-isobutyric acid and glutamine is possibly relevant to the effect on neural system function. (3) Hyperphenylalaninemia influences cerebroside metabolism through fatty acid desaturase and it induces the disturbance of carbohydrate metabolism. (4) High phenylalanine level inhibits amino acid transport, decreases amino acid intake by the brain, creates imbalance of various amino acids, and influences the synthesis of protein and corresponding neurotransmitters. Through multifaceted channels working together, hyperphenylalaninemia eventually results in brain dysfunction and seizures. 23,24
A recent study in Japan that enrolled 503 phenylketonuria patients, among them 62 patients (12.3%, 41 boys and 21 girls) diagnosed with West syndrome, 1 concluded that the incidence of West syndrome was higher among phenylketonuria patients than among the general population (0.24‰-0.42‰). 5 It was also demonstrated that the incidence of West syndrome complications in phenylketonuria patients increases corresponding to the increasing age of starting a low phenylalanine diet therapy.
Dihydropteridine Reductase Deficiency
Dihydropteridine reductase deficiency is the second most frequent group among tetrahydrobiopterin synthesis deficiencies. In biopterin deficiency, a rare cause of hyperphenylalaninemia, an insufficient supply of endogenous tetrahydrobiopterin cofactor impairs the function of phenylalanine, tyrosine, and tryptophan hydroxylases. Symptoms result more from defective synthesis of neurotransmitters (dopamine, serotonin, noradrenalin, and adrenalin), resulting in low level of homovanillic acid and 5-hydroxyindolacetic acid in the cerebrospinal fluid, than from phenylalanine accumulation, which may be very mild. To date, about 150 cases of dihydropteridine reductase deficiency are recorded in the International Register.
Epilepsy is more frequently reported in dihydropteridine reductase deficiency than in other biopterin deficiencies. In the International Register, electroencephalogram before 1 year of age is normal in 38% of dihydropteridine reductase deficient patients, whereas 46% have hypsarrhythmia, sharp waves, or epileptic discharges. 25 The association of West syndrome with biopterin metabolism deficiency is less frequently reported, which may be explained by the fact that there is no systematic or epidemiologic study. Three cases of dihydropteridine reductase deficiency with severe epilepsy and hypsarrhythmia were reported to the International Register. 26
In a recent article, Mikaeloff et al report a case of a 2-year-old child with dihydropteridine reductase deficiency who developed hypsarrhythmia and infantile spasms. Partial efficacy on tone and communication was observed with diet and neurotransmitter precursor therapy, but no effect on the epilepsy. The administration of hydrocortisone eventually controlled both seizures and hypsarrhythmia with improved general clinical status. 22
Organic Acidurias
d -Glyceric Aciduria
Methylmalonic Aciduria
West syndrome occurs occasionally in patients with branched-chain organic acidurias. Methylmalonic aciduria is one of the most frequent organic acidurias (1:115 000 in Italy, 1:169 000 in Germany). 32,33 It is caused by a deficiency in methylmalonyl coenzyme A mutase, a mitochondrial enzyme that requires adenosylcobalamin as a cofactor and performs an essential reaction in the transformation of propionyl coenzyme A to succinyl coenzyme A. 34 Accumulation of methylmalonic acid can cause severe metabolic acidosis and long-term complications such as renal failure and brain toxicity, involving in particular the basal ganglia. Epilepsy rarely occurs as a long-term complication of methylmalonic aciduria. 35
Two patients with methylmalonic aciduria were previously described with myoclonic convulsions, psychomotor retardation, and hypsarrhythmia, 36 a patient from Japan with methylmalonic aciduria was described with brief tonic seizures and polyspike bursts on electroencephalogram 37 and a patient with vitamin B12 deficiency and secondary methylmalonic aciduria also had West syndrome. 38 The most recent case report by Campeau et al describes a patient diagnosed with methylmalonic aciduria at 4.5 months of age. The child was developmentally delayed and hypotonic and his electroencephalogram showed hypsarrhythmia. Following the failure of vigabatrin and lamotrigine to control the spasms, hydrocortisone was introduced. This article demonstrates that the management of methylmalonic aciduria with concurrent steroid therapy is possible and also beneficial. 39
Propionic Acidemia
Propionic acidemia is a disorder of branched-chain amino acids, the side chain of cholesterol, and odd-chain fatty acid metabolism that leads to the accumulation of toxic acid metabolites. The clinical features typically begin shortly after birth, although they can also appear in young adulthood. 40 To our knowledge, there are very few references in the international literature of children with propionic acidemia who developed West syndrome. Among them, the case of a 3-year-old boy who at 6 months of age presented bursts of infantile spasms and a hypsarrhythmic electroencephalogram, and also the case of a 4-month-old girl who presented with myoclonic seizures and an electroencephalogram showing hypsarrhythmia. Both children had previously been diagnosed with propionic acidemia. 40,41
Disorders of Fatty Acid Oxidation
Short-Chain Acyl-Coenzyme A Dehydrogenase Enzyme Deficiency
Short-chain acyl-coenzyme A dehydrogenase enzyme deficiency is a rare fatty acid oxidation disorder with variable clinical presentations. There are only 21 patients reported in the literature. Short-chain acyl-coenzyme A dehydrogenase enzyme deficiency may initially have no clinically observable symptoms and can become apparent only during metabolically demanding circumstances. Although this deficiency has been associated with seizures, there has been only one report of short-chain acyl-coenzyme A dehydrogenase enzyme deficiency presenting with infantile spasms and brain malformation. The reported female infant developed repeated tonic-clonic seizures at the age of 3.5 months. She subsequently developed West syndrome at the age of 4 months. 42 The possible association between West syndrome and short-chain acyl-coenzyme A dehydrogenase enzyme deficiency has not been described as further experience with this rare disorder needs to be taken into consideration.
Mitochondrial Disorders
Pyruvate Dehydrogenase Complex Deficiency
Pyruvate dehydrogenase complex is an enzyme complex consisting of 5 enzymes. The first enzyme of the complex, pyruvate dehydrogenase (E1), is a tetramer consisting of 2 a-subunits and 2 b-subunits. A deficiency of a-subunit (E1a) is the most common cause of congenital pyruvate dehydrogenase complex deficiency with lactic acidemia. 43 E1a deficiency is often associated with various types of brain damage and neurologic symptoms, with a significant difference in symptoms between female and male patients, as infantile spasms have been encountered almost exclusively in female patients. 44
Seizures are a major clinical problem in more than 50% of patients with pyruvate dehydrogenase complex deficiency. In a few patients, seizures take the form of infantile spasms, associated with the typical electroencephalogram pattern of hypsarrhythmia. To our knowledge, 7 described patients with pyruvate dehydrogenase complex deficiency have displayed the West syndrome. 45 –50 All these patients were female, even though overall West syndrome occurs more frequently in males. By molecular analysis, most of the female patients have mutations located in the E1a gene.
It has been postulated that in female patients with E1a deficiency, significant retardation of fetal brain development occurs as early as the end of the second trimester. Additional damage to the brain would be superimposed between that time and delivery because development of the fetal brain becomes more dependent on pyruvate dehydrogenase complex E1a activity after the mid-organogenesis stage. 51
Lysosomal Disorders
Hurler Syndrome
Mucopolysaccharidosis I (Hurler syndrome) is a metabolic disease of autosomal recessive inheritance caused by deficient activity of alpha-
Gudiño et al made the first clinical observation of Hurler syndrome with an unusual presentation for its association with West syndrome, vitamin D–dependent rickets, and early hydrocephalus. According to the authors, the interaction of Hurler syndrome with vitamin D–dependent rickets, along with early hydrocephalus, produced a synergic action that favors the evolution of West syndrome in this patient. 52
GM2 Gangliosidosis
GM2 gangliosidosis is a group of inherited neurodegenerative diseases caused by deficiency of lysosomal β-hexosaminidase, resulting in GM2 ganglioside accumulation in brain. The resulting accumulation of ganglioside GM2 occurs primarily in neuronal cells and coincides with a progressive broad spectrum of neurologic deterioration. Epileptic seizures are rare in patients with GM2 gangliosidosis and generally appear later, although spasms sometimes appear around 6 months. These patients usually present with myoclonic epilepsies that can sometimes progress to West syndrome.
Disorders of Metal Metabolism
Menkes Disease
Menkes disease is a rare X-linked recessive disorder with a primary generalized defect in copper transport. It is characterized by progressive cerebral degeneration with psychomotor deterioration and seizures, connective tissue alteration with hypopigmentation of skin and hair, and recurrent episodes of hypothermia with failure to thrive. 53 Menkes disease is related to the loss of a copper transporting adenosine triphosphatase (ATPase) involved in the export of dietary copper from the gastrointestinal tract and its transport into organelles. 54 Biochemically, the disease is characterized by low serum, liver and brain copper levels, whereas the copper content in nearly all other organs is increased. 55 Epileptic seizures are frequently associated with Menkes disease, but details of type of seizures and electroencephalogram patterns are rarely reported. Myoclonus is considered the usual seizure type and often leads to metabolic investigations in newborns and infants. Infantile spasms are uncommonly reported in inborn metabolic disorders, but probably are underestimated because of the lack of polygraphic electroencephalogram recording.
Kreuder et al reported a patient with Menkes disease who developed infantile spasms with typical hypsarrhythmia when dose levels of copper-histidine therapy were reduced. 56 White et al suggested that in some patients with Menkes disease, cerebral electrical activity may be influenced by the level of circulating copper. 57
In another study by Sfaello et al, the authors evaluated the evolution of infantile spasms in 2 patients with Menkes disease and the relation with copper-histidine treatment. They observed that infantile spasms can be a presenting or late feature of Menkes disease and may not be amenable to therapy with copper-histidine. 12
In a more recent study conducted by Bahi-Buisson et al, the authors analyzed the evolution of electroclinical features of 12 patients with confirmed Menkes disease and a quite prolonged survival. The authors individualized 3 successive periods in the course of epilepsy in these patients with Menkes disease: early focal status, then infantile spasms, and then myoclonic and multifocal epilepsy after age 2 years. 58
Nonketotic Hyperglycinemia
Nonketotic hyperglycinemia, also known as glycine encephalopathy, is an autosomal recessive metabolic disorder characterized by the accumulation of glycine in the brain due to a defect in the glycine cleavage enzyme system. The neonatal form presents in the first few days of life with progressive lethargy, hypotonia, hiccups, and seizures and progresses to central apnea and often death. Surviving infants often have profound developmental delay and intractable seizures. The infantile form presents in the first few months of life and is also characterized by hypotonia, developmental delay, and seizures. The initial electroencephalogram typically shows a burst-suppression pattern that evolves into hypsarrhythmia or multifocal spikes over the next few months. 59
Pyridoxine-Dependent Epilepsy
Pyridoxine-dependent epilepsy is a rare autosomal recessive disorder, localized to chromosome 2q31, that usually presents with neonatal intractable seizures. This syndrome results from an inborn abnormality of the enzyme glutamic acid decarboxylase, which results in reduced pyridoxine-dependent synthesis of the inhibitory neurotransmitter GABA. The full range of symptomatology is unknown, but it can be associated with autism, breath holding and severe mental retardation, bilious vomiting, transient visual agnosia, severe articulatory apraxia, motor dyspraxia, microcephaly, and intrauterine seizures. Most common seizure type is generalized tonic clonic seizures that progress to status epilepticus. Other types of seizures reported in the literature include brief partial seizures, atonic and myoclonic seizures, and infantile spasms. Although a regional variation in its incidence exists, pyridoxine dependency has been said to be a rare cause of neonatal seizures. Since the initial description of this disorder in 1954, fewer than 100 patients with pyridoxine-dependent seizures have been reported. 60,61
Conclusions
Although it has been underestimated, West syndrome is usually caused or predisposed by an underlying inborn error of metabolism. To our knowledge, there are no large studies on children with metabolic diseases who developed West syndrome, although there are many separate case reports of such patients. We briefly described the most frequent inborn errors of metabolism which so far have been associated with West syndrome, illustrating the importance of early diagnosis and consequently the initiation of the adequate treatment.
Footnotes
Author Contributions
Both authors contributed equally to the preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This being a review paper with no primary experiments, ethical approval was not applicable.