
Abstract
Lacosamide is a US Food and Drug Administration (FDA)–approved antiepileptic drug for patients 17 years or older with partial epilepsy. There are sparse data on children. The objective of our study was to evaluate its efficacy/safety in children with refractory epilepsy. Forty children (mean age 14.3 years) were treated with lacosamide at our institution (adjunctive therapy in 36, monotherapy in 4). Fifteen patients had symptomatic focal epilepsy, 2 had cryptogenic focal epilepsy, 20 had symptomatic generalized epilepsy, and 3 had cryptogenic generalized epilepsy. Two had juvenile myoclonic epilepsy and 5 had Lennox-Gastaut syndrome. Forty-two percent had at least >50% reduction in seizure frequency, and 6 became seizure free. Average dose was 7 mg/kg/d and average follow-up was 9.2 months. Responders had a 76.5% mean decrease in seizures. Fifteen children experienced an adverse reaction and 7 discontinued lacosamide (4: Ineffective, I: insurance denial, 1: tremor, 1: behavior). Lacosamide is effective and well-tolerated in children with refractory epilepsy.
Keywords
Lacosamide is a novel antiepileptic drug approved as adjunctive treatment of refractory partial-onset epilepsy in patients 17 years of age or older. 1 Lacosamide is a functionalized amino acid compound that, in adults, has 100% oral absorption with linear pharmacokinetics, low protein binding (<19%), peak blood concentration in 1 to 2 hours with a 13-hour half-life, renal clearance, limited hepatic metabolism, and no known significant drug interactions. 2 Considering the encouraging pharmacokinetics, lacosamide should be a favorable option for treatment in children as well.
Lacosamide selectively enhances the slow inactivation of voltage-gated sodium channels. 3 Sodium channels are responsible for the generation and propagation of nerve action potentials and control of overall neuronal excitability. Lacosamide action on the slow inactivation of the voltage-gated sodium channel is a new area of attack on an ion channel that has long been the target of many of the older antiepileptic drugs. It is well known that some seizure phenotypes have specific neuronal membrane or ion channel defects that can predispose to excessive cortical excitability. 4 This will undoubtedly lead to many targeted treatment approaches to these channelopathies. It is not yet well delineated whether antiepileptic drugs with actions on distinct ion channels have better response rates when treating epilepsies associated with channelopathies. On the other hand, it has been previously shown that some medications that act on sodium channels, such as lamotrigine and carbamazepine, can worsen seizures associated with Dravet syndrome, a defect of the SCN1A channel. 5,6
Initial studies also found that lacosamide modulates collapsin response mediator protein-2 (CRMP-2), a phosphoprotein involved in axonal outgrowth and neuronal differentiation. 7 It is unclear whether this interaction has an impact on epileptogenesis, as unregulated or disorganized neuronal connections are hypothesized to be involved in seizure propagation. This interaction with collapsin response mediator protein-2 also causes concern about potential adverse effects on the developing brain. This mechanism of action warrants further investigation, as most recent evidence suggests that lacosamide does not actually bind to this protein. 8
Despite treatment with many of the classic and new antiepileptic drugs, more than 30% of patients with epilepsy become refractory to current treatments. 9 Surgical intervention, vagal nerve stimulation, and the ketogenic diet can also fail in these patients. New pharmaceutical approaches for the treatment of seizures are important for these individuals who have failed other therapies.
Clinical studies have shown that lacosamide has a good response rate in adults with a favorable side-effect profile. 10,11 There is a sparse amount of data that exists on the efficacy of lacosamide in the pediatric population. The present single-center retrospective study reviews the efficacy and tolerability of lacosamide as adjunctive treatment or monotherapy in children with epilepsy.
Methods
This study was approved by the Institutional Review Board of St. Christopher’s Hospital for Children, Drexel University College of Medicine. We retrospectively reviewed the records of children and adolescents with epilepsy treated with lacosamide as adjunctive treatment and as monotherapy at our institution between 2009 and 2011. Patients younger than 21 years of age with refractory epilepsy (generalized or focal) at the time of the initiation of treatment with lacosamide were included in the study. The daily dose of lacosamide was the optimal dose determined individually for each patient as required to improve efficacy and/or reduce adverse effects. The following data were collected: gender, age, developmental/cognitive level, seizure type and etiology, age at seizure onset and at initiation of lacosamide treatment, number of antiepileptic drugs used, lacosamide dose and dosing schedule, previous use of vagal nerve stimulator or ketogenic diet, follow-up duration, treatment response, and adverse events.
The response to treatment was quantified using data on seizure frequency before and while on lacosamide treatment. It was based on caregiver reports during follow-up visits and classified as seizure free, >75% reduction, >50% reduction, and ineffective (all <50% responders). Children and adolescents with more than 50% reduction in seizure frequency were considered responders. Adverse events were also collected based on caregiver reports at each follow-up visit.
Categorical data were expressed as percentages and quantitative data as mean, standard deviation (SD), and range. Categorical variables were compared between groups with chi-square test and quantitative variables with student’s t test. Statistical significance was set at P <.05. All statistical analyses were performed with the SPSS statistical software package (SPSS for Windows, v.19, SPSS, Inc., Chicago, IL).
Results
We identified 40 children with refractory epilepsy treated with lacosamide (Table 1). There were 55% boys and 45% girls with a mean age of 12.3 years (SD 4.8; range 1.4-20.8 years) at the initiation of treatment. The mean age of onset of seizures was 4.1 years (SD 4.6; range birth to 15.4 years). The average follow-up was 9.2 months (SD 4.7; range 1.7-28.3 months) after starting treatment with lacosamide.
Patient Demographics and Epilepsy Characteristics (n = 40)
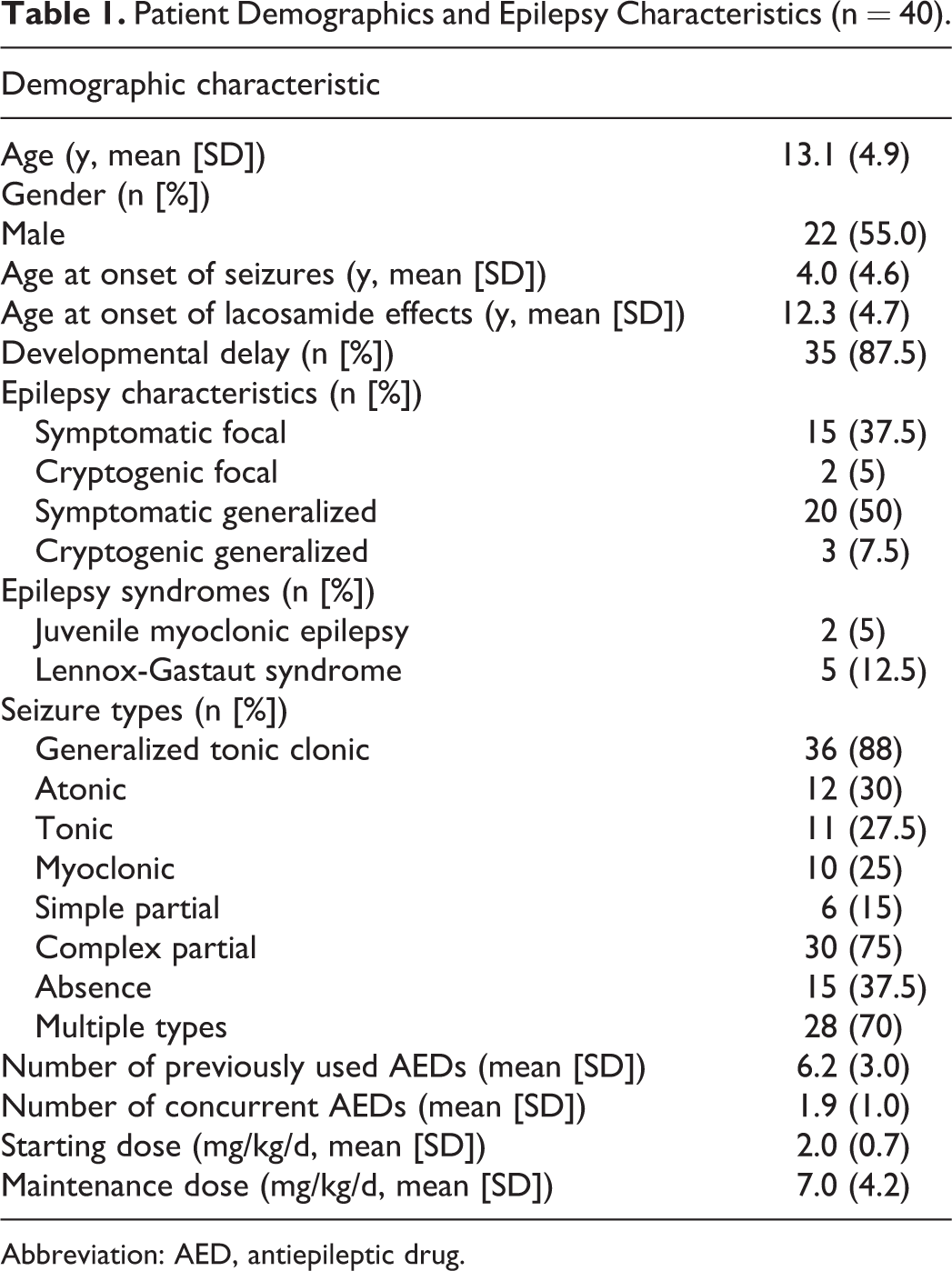
Abbreviation: AED, antiepileptic drug.
There was a positive family history of seizures in 27.5% of patients. Nineteen children (47.5%) had tried treatment with vagal nerve stimulator and 9 (22.5%) were previously treated with ketogenic diet. Seizure types are shown in Table 1. Most patients (70%) experienced multiple seizure types.
A total of 17 patients (42.5%) had at least a >50% decrease in the frequency of seizures with a mean decrease in seizure frequency of 76.5% (Figure 1). Six of these patients (15%) were seizure free at the latest follow-up. Patients who had generalized epilepsy had a similar reduction in seizure frequency as compared to patients with partial-onset epilepsy (χ2 = 2.796, df = 5, P = .731). The average lacosamide starting dose was 2.03 mg/kg (SD 0.73) and maintenance dosing at follow-up was 7.04 mg/kg (SD 4.23). All patients in the study had their medicine dosed twice a day. Seizure response was not significantly determined by average dosing, although we did find a tendency toward an inverse relationship between average maintenance dosing and seizure frequency reduction. Patients who were nonresponders on lacosamide averaged 7.5 mg/kg/d while patients who were seizure free averaged 5.4 mg/kg/d. Those patients who responded the poorest to lacosamide were more likely to have tried at least 6 or more antiepileptic drugs in the past (χ2 = 4.269, df = 1, P = .039) compared to patients who had tried fewer than 6 medications prior to lacosamide. Linear regression analysis was conducted between each antiepileptic drug combined with lacosamide and there was no statistically significant reduction in seizure frequency with any particular combination.
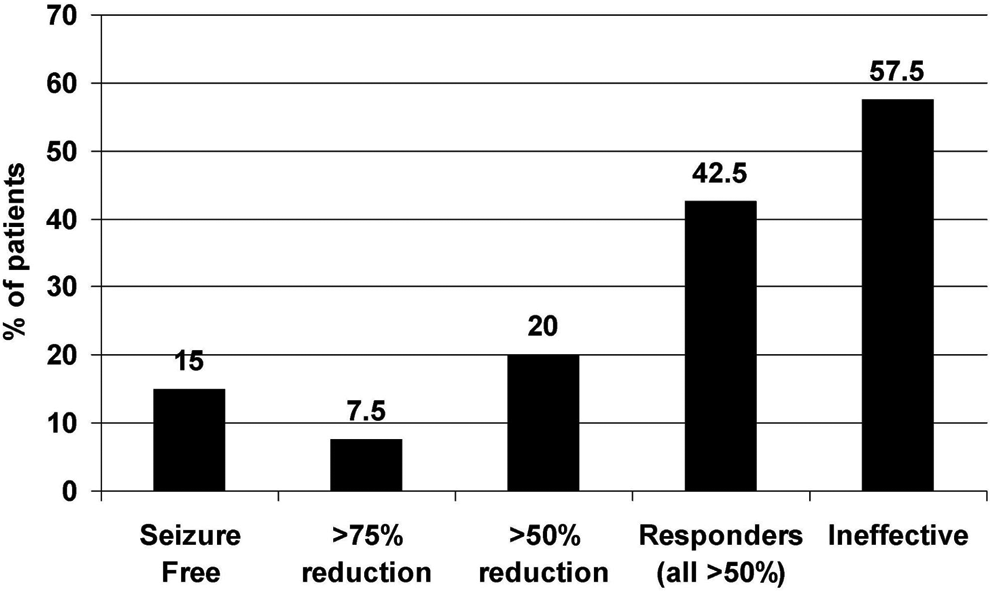
Seizure frequency reduction.
Side effects of lacosamide were seen in 15 patients (37.5%) and included lethargy in 4 (10%), worsening behavior in 4 (10%), weight loss in 2 (5%), dizziness in 2 (5%), mild memory impairment in 1 (2.5%), depression in 1 (2.5%), and tremor in 1 (2.5%). Seven patients (17.5%) discontinued lacosamide during the study, 4 for lack of efficacy (10%), 1 for head tremor (2.5%), and 1 for worsening behavior (2.5%), and 1 for lack of insurance approval (2.5%). Of the 3 patients who had worsening seizures, one had an increase in seizure frequency of 20%, and the other 2 had reported longer seizures than usual with preserved frequency. Patients who experienced side effects were taking maintenance lacosamide at an average dose of 8.07 mg/kg/d, whereas those who did not have any received an average dose of 5.5 mg/kg/d.
Lacosamide was used as monotherapy in 4 patients (10%), but was never used as first-line treatment. They had an average age of seizure onset of 9.6 years and started lacosamide at an average age of 11.1 years. Two of them had cryptogenic generalized epilepsy, 1 had symptomatic generalized epilepsy, and 1 cryptogenic partial-onset epilepsy. The average number of antiepileptic drugs tried prior to lacosamide was 3.8, and the average dosing in these children was 6.34 mg/kg/d. Three became seizure free on lacosamide and one had 80% of seizure reduction, which was a significantly better response than our adjunctive therapy cohort (χ2 = 15.962, df = 5, P = .007). Mild memory impairment was reported as a side effect in one of these patients, but it did not lead to discontinuing the treatment.
Discussion
Three randomized, multicenter, placebo-controlled studies were completed to test the efficacy of lacosamide in adults with refractory partial-onset epilepsy. 10,11,12 Simoens et al 13 published the accumulated data from these studies and their economic impact. The median percentage reduction in seizure frequency from baseline was 18.4% for placebo, 33.3% for lacosamide 200 mg/d (P < .01), 36.8% for lacosamide 400 mg/d (P < .001) and 9.4% for lacosamide 600 mg/d. The percentage of patients with a seizure frequency reduction of ≥50% was 22.6% for placebo, 34.1% with lacosamide 200 mg/d (P < .05), 39.7% with lacosamide 400 mg/d (P < .001), and 39.6% with lacosamide 600 mg/d. One study showed that 30% to 50% of adults had up to a 96% decrease in frequency of partial seizures with secondary generalization. 10
The experience with the use of oral lacosamide in children has been limited, so far, to 4 recent retrospective studies, totaling 67 patients (Table 2). 14 –17 In our study, the response rate of >50% seizure reduction was slightly higher, 42% versus a mean of 37% of the 4 pediatric studies 14 –17 and 39% from the best results of adult studies. The percentage of patients experiencing side effects (37.5%) was similar to the other pediatric studies except Heyman et al, 16 who reported a 59% rate of side effects. Our 17.5% lacosamide discontinuation rate was lower than the mean of 36% from the other pediatric studies. 14 –17
Summary of Studies Assessing the Effects of Lacosamide on Epilepsy in Children
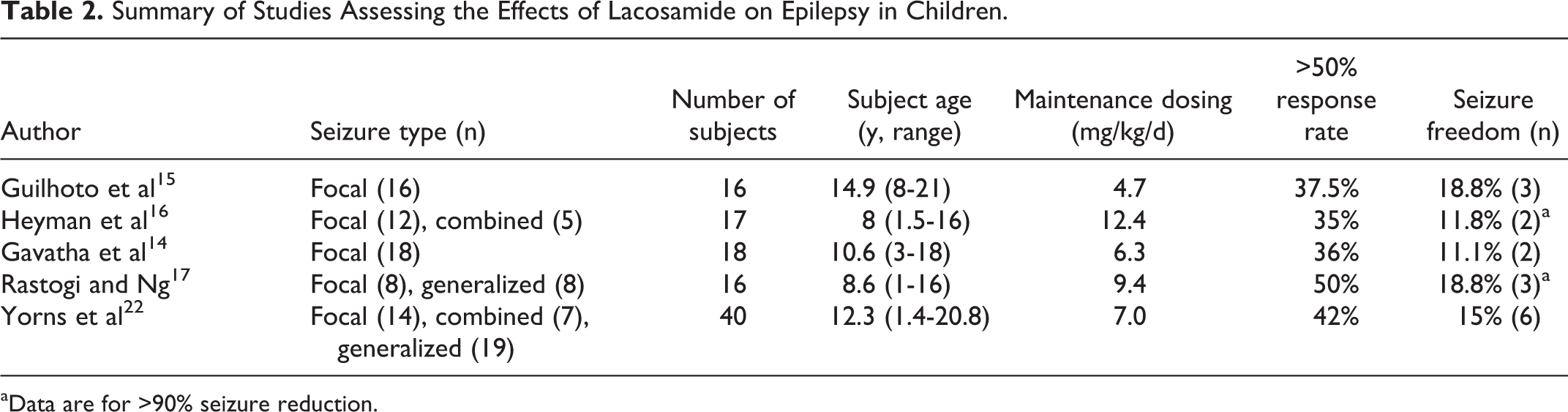
aData are for >90% seizure reduction.
The FDA indication for the use of lacosamide is for adjunctive therapy for partial epilepsy only. There have been previous data showing seizure frequency reduction following lacosamide administration in some rat models of generalized seizure disorders. 18 Rastogi and Ng 17 used lacosamide in 8 patients with generalized epilepsy, and Heyman et al 16 used lacosamide in 5 patients with focal and generalized seizures, 2 of them with Lennox Gastaut syndrome. We have successfully used lacosamide on 23 patients with symptomatic or cryptogenic generalized epilepsy. In our study, 42.5% of children with partial-onset epilepsy had an improvement with lacosamide compared with 57.5% of children with generalized epilepsy, although this difference did not reach statistical significance. One of our patients with refractory juvenile myoclonic epilepsy averaging several generalized tonic-clonic seizures per day has not had a single seizure for over a year after the introduction of lacosamide. This is the largest group of pediatric patients with refractory generalized epilepsy in the literature, showing that lacosamide can also be effective in this type of epilepsy.
Heyman et al, 16 as indicated above, reported the use of lacosamide monotherapy in 4 children, with a 25% response rate. We also successfully used lacosamide as monotherapy in 4 children, but with a 100% response rate, 3 patients becoming seizure free and 1 achieving 80% decrease in seizure frequency.
We found that there was no significant association between dosing and seizure reduction. Patients who were started on lacosamide generally responded soon after treatment initiation and they did not necessarily improve after upward titration. The nonresponders in our study averaged a higher daily dose than the patients achieving seizure freedom.
Those patients who had tried more than 6 antiepileptic drugs in the past were less likely to respond to lacosamide. This finding is consistent with prior studies showing that there is an increased chance of developing resistance with each successive attempted antiepileptic drug. 19
Adverse events in other studies have been reported to be dose dependent and included a variety of symptoms previously described in the summary of the pediatric studies. 14 –17 Side effects tended to happen early in our cohort of patients, which may have limited the upward titration of lacosamide in order to treat the seizures. Side effects are hypothesized to occur more frequently when lacosamide is used in conjunction with other antiepileptic drugs that act on the sodium channel (ie, carbamazepine, oxcarbazepine, lamotrigine, phenytoin, and topiramate). Our data show that there was no significant association between side effects and the use of a specific concomitant antiepileptic drug with lacosamide. Gavatha et al 14 also found a lack of association between lacosamide side effects and other antiepileptic drugs acting on the sodium channels.
It was the goal of this study to review the medical records of our pediatric epilepsy patients and summarize the effectiveness and tolerability of lacosamide in a pediatric population. Our data are consistent with the currently available adult and pediatric studies and provides the largest collection of patients on the use of lacosamide in children. We conclude that lacosamide is effective as adjunctive therapy in children with refractory epilepsy, both partial and generalized, and is well tolerated. The overall efficacy in patients with severe refractory epilepsy and the good response in patients with monotherapy suggest that lacosamide may be more effective as a first choice for antiepileptic treatment than other antiepileptic drugs, and theoretically could have the potential of reducing the risk of progressing to refractory epilepsy. 9 Its availability as an intravenous formulation makes it also a good choice to treat status epilepticus, particularly refractory status, both in adults and children. 20,21 There is a need for studies with larger populations of pediatric patients to better define the role of lacosamide in the therapeutic armamentarium of pediatric epilepsy.
Footnotes
Acknowledgments
These data were presented at the Annual American Academy of Neurology meeting on April 14, 2011, in Honolulu, Hawaii.
Author Contributions
WRY drafted the original manuscript and performed the data collection and analysis. AL and IV contributed to the statistical analysis, writing, and revision of the final manuscript. DK, KC, and HH contributed to the drafting and editing of the manuscript and provided clinical information.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board of St. Christopher’s Hospital for Children, Drexel University College of Medicine.