
Abstract
A retrospective cohort study was conducted to describe the relationship between gross motor function and manual ability in children with cerebral palsy and explore differences between cerebral palsy subtypes and associated comorbidities. Children with cerebral palsy born between 1999 and 2008 were included from the Registre de la Paralyse Cérébrale de Québec identifying 332 children. The overall agreement between Gross Motor Function Classification System and Manual Ability Classification Scale Levels was moderate (kappa 0.457, standard error 0.034) with a strong positive correlation (Spearman rho of 0.820, standard error 0.023). This agreement was moderate among children with spastic quadriparesis and dysketic cerebral palsy, fair in children with spastic diplegia, and poor in children with spastic hemiplegia. Children with cognitive impairment showed a higher correlation than those without cognitive impairment. The correlation between gross motor function and manual ability in children with CP varies based on neurologic subtype and cognitive level.
Cerebral palsy encompasses a group of nonprogressive disorders characterized by impairment of movement and posture, often associated with a wide range of comorbidities such as epilepsy, feeding difficulties, speech, cognitive, and musculoskeletal impairments. 1 It is the most common cause of childhood physical disability. 2
Functional outcome measures are increasingly gaining both clinical and research focus, with the recent development of reliable, valid and standardized scales to measure both gross and fine motor abilities specifically in cerebral palsy. The Gross Motor Function Classification System is a 5-level classification system that describes the gross motor function of children and youth with cerebral palsy, with well-established validity and reliability. 3 Distinctions between levels are based on functional abilities and the need for assistive technology with levels I to III being ambulant and levels IV to V being nonambulant. The Manual Ability Classification System is a newer 5-level classification system that describes the typical bimanual function for children with cerebral palsy, with established validity and reliability. 4 Distinctions between the levels are based on the child’s reported usual ability to handle objects and their need for assistance or adaptations to perform manual tasks in everyday life and situations, ranging from level I with no restriction on activities of daily living to level V where total assistance is needed for activities of daily living and there exists no discernable functional hand use.
A few studies have explored the relationship between the Gross Motor Function Classification System and Manual Ability Classification Scale Levels, with results varying from poor to good correlations or agreements. 5 –7 These studies also looked at different populations of children, from hemiplegic cerebral palsy, to all spastic types of cerebral palsy, to all neurologic subtypes. 5,6 –8 Although the pattern of Gross Motor Function Classification System and Manual Ability Classification Scale Levels were discrepant, it appears to vary with neurologic subtype of cerebral palsy. Their relationship with comorbidities has not been studied previously, and their relationship has not been explored in a North American population, where cerebral palsy subtypes are classified to distinguish between spastic diplegia and spastic quadriplegia who are classified as bilateral spastic in the European populations. The aim of our observational study was to explore the association and correlation between Gross Motor Function Classification System and Manual Ability Classification Scale levels in a population-based sample of children with cerebral palsy and explore variations based on neurologic subtype and comorbidities.
Methods
Study Population
Children with cerebral palsy were selected from the Registre de Paralysie Cerebrale du Quebec, which actively recruits children with cerebral palsy born between 1999 and 2010 living in 6 of the 17 administrative health regions of Quebec representing approximately half of the province’s annual births. Details of the registry’s methodology have been previously described and the cohort well characterized. 9 –11 The overall prevalence of cerebral palsy based on the registry’s ascertainment is 1.84 (95% confidence interval 1.60-2.08), slightly lower than the estimated overall prevalence of 2.0 per 1000 children. 12 All children who had both Gross Motor Function Classification System and Manual Ability Classification Scale scores available were selected for this study, including birth cohorts 1999 to 2008. Ethical permission for the Registry’s establishment and implementation has been obtained at the local host institution (McGill University Health Center Research Institute) and each participating pediatric rehabilitation centre and written informed consent obtained from parents or guardians.
Measures of Motor Function
The gross motor function for each child was assessed using the Gross Motor Function Classification System level recorded at 2 years of age, which was reassessed at or after 5 years of age. The appropriate Gross Motor Function Classification System classification entered in the registry was determined by the children’s treating physiotherapists. The most recent Gross Motor Function Classification System classification was used in our analysis. The Manual Ability Classification System was used to assess bi-manual ability, which became available during the follow-up period of the registry in 2007. Manual Ability Classification Scale levels are entered in the registry only when available based on the treating occupational therapists’ comprehensive assessments.
Comorbidities
Six different comorbidities were documented for each child. Cortical visual impairment was defined as determined by an ophthalmologist. A sensorineural auditory impairment was defined as severe if there was bilateral hearing loss of 70 dB or greater on audiometric testing. Communication impairment was further classified as verbal, verbal and nonverbal, nonverbal, or unable to communicate. Nonverbal was defined as absence of specific words or recognizable vocabulary in the child’s maternal language regardless of whether evident concurrent cognitive limitations were present. Enteral feeding status referred to use of a temporary or permanent artificial tube to provide nourishment to the child. Coexisting epilepsy was defined as occurrence of afebrile seizures in the 12 months preceding Registry inscription. The presence of cognitive impairment was defined as mild, moderate, or severe as assessed by standardized neuropsychological testing when available at 5 years of age or later. A lack of consistent access to psychiatric information deterred from the accurate ascertainment of possible concurrent behavioral disorders.
Statistical Analyses
Statistical analyses were performed with SPSS version 20.0 (IBM) with P values less than .05 considered as statistically significant. Descriptive statistics were used to characterize the study population. Correlations between Gross Motor Function Classification System and Manual Ability Classification Scale levels were performed with the Spearman correlation test. The overall agreement between the Gross Motor Function Classification System and Manual Ability Classification Scale levels were analyzed using nonweighted Kappa statistics. Interpretation of a kappa value is suggested to be as follows: <0.20 as poor agreement, 0.21 to 0.40 as fair agreement, 0.41 to 0.60 as moderate agreement, 0.61 to 0.80 as good agreement, and >0.80 as very good agreement.
Results
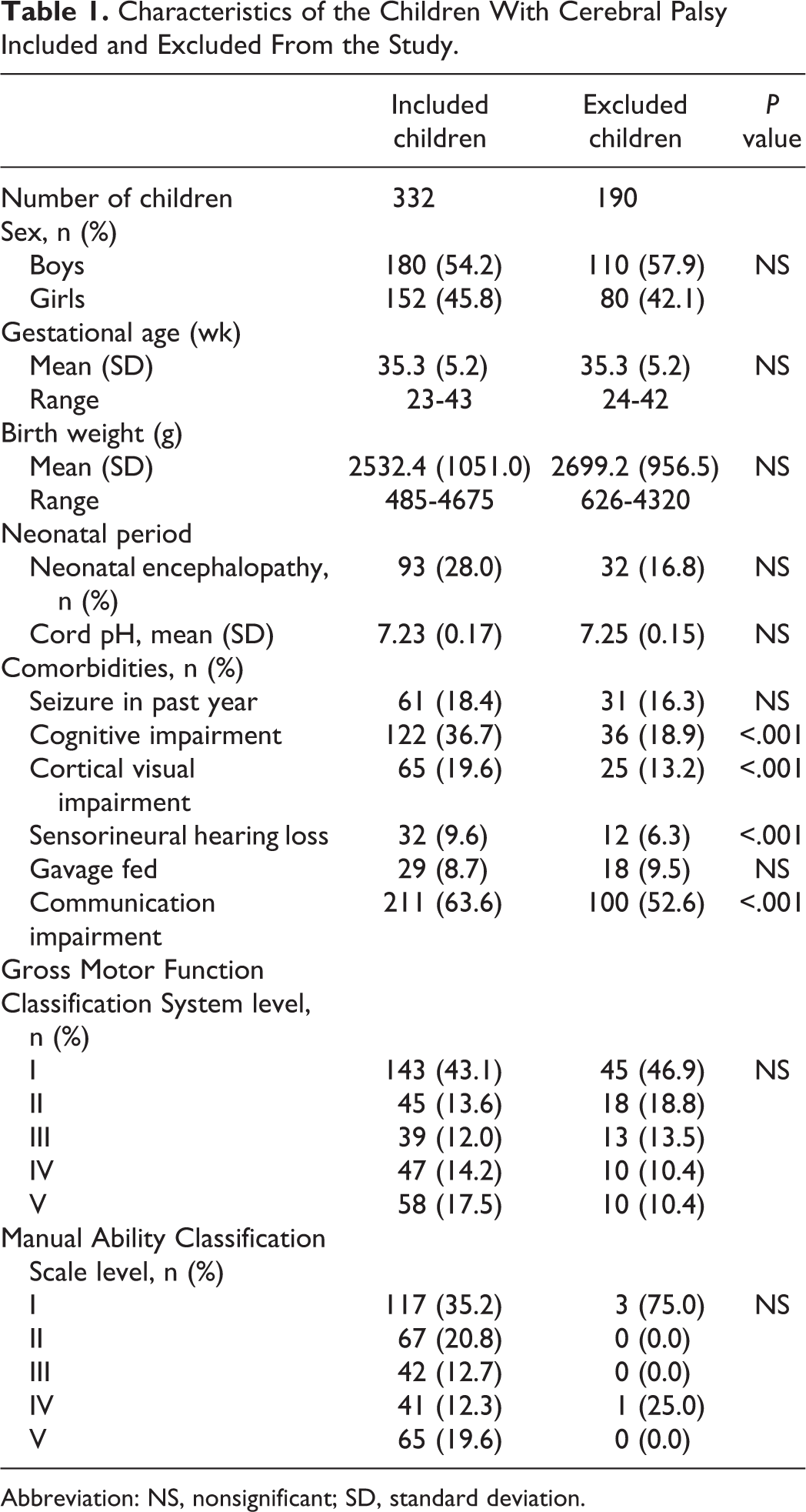
A total of 614 children with cerebral palsy were identified through the Registre de la Paralyse Cérébrale de Québec, of which 522 participated in the registry’s ascertainment and inscription protocol. From these, 332 children with cerebral palsy had both Gross Motor Function Classification System and Manual Ability Classification Scale levels available and were selected as our study population. Many children were registered prior to the availability of the Manual Ability Classification Scale and therefore only had Gross Motor Function Classification System levels. The details of our sample selection are outlined in Figure 1. The characteristics of the children participating in the registry are outlined in Table 1. Children included in our study differed significantly from children excluded in terms of their 5-minute Apgar score, and the number of comorbidities reported (cognitive impairment, cortical visual impairment, sensorineural hearing loss, and communication impairment). All other characteristics at birth including sex, gestational age, birth weight, presence of neonatal encephalopathy, and cord pH values did not differ between the 2 groups. Their Gross Motor Function Classification System and Manual Ability Classification Scale levels were also equally distributed between included and excluded children, although not many children in the excluded group had Manual Ability Classification Scale available.
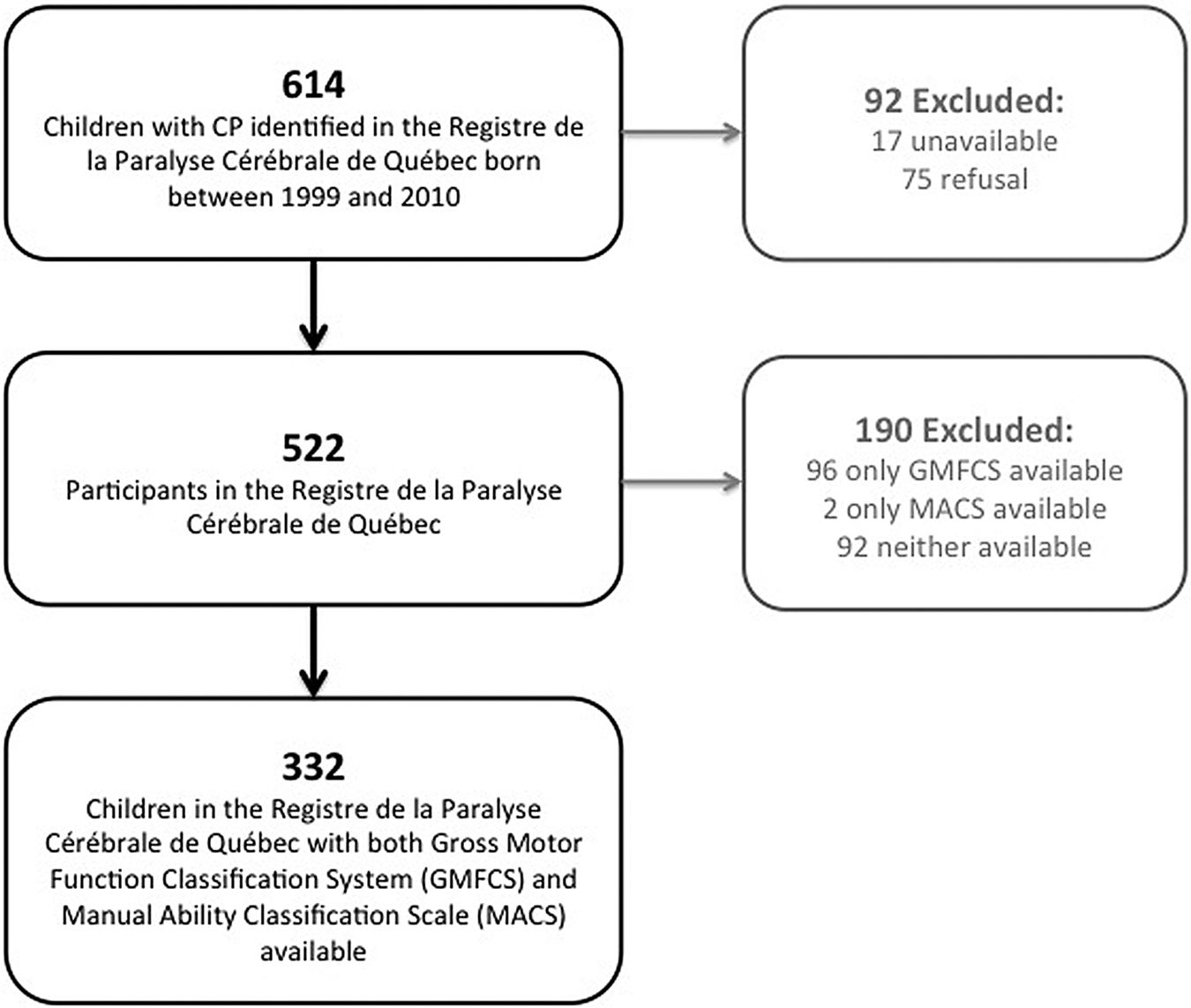
Sample selection
Characteristics of the Children With Cerebral Palsy Included and Excluded From the Study
Abbreviation: NS, nonsignificant; SD, standard deviation.
In our study group of 332 children with cerebral palsy, 54.2% were boys, with a mean gestational age of 35.3 weeks and a mean birth weight of 2532.4 g. The distribution of cerebral palsy subtype was as follows: 105 had a spastic hemiparesis, 117 had a spastic quadriparesis, 86 had a spastic diplegia, 19 had a dyskinetic cerebral palsy, and 5 had other types (ataxic cerebral palsy, hypotonic cerebral palsy).
Seizures in the year prior to enrollment in the registry were reported in 18.4% of the children, cortical visual impairment was reported in 19.6%, and 8.7% of the Registry participants were fed by gavage feeding. A large proportion of children were reported as having a cognitive impairment (36.7%). Of these, information on the severity of cognitive impairment was available on 100 children: 26 had a mild impairment, 20 had a moderate impairment, and 54 had at least a severe impairment as evaluated by standardized psychometric testing. More than half of children in our study had a degree of communication impairment (211 children, 63.6%). Information on their communication ability was available on 209 children: 88 used verbal communication, 49 used both verbal and nonverbal communication, 41 used nonverbal communication, and 31 were not able to communicate using words or signs.
In all children included in the study, there was a strong positive correlation between the Gross Motor Function Classification System and Manual Ability Classification Scale, with Spearman rho of 0.820, standard error 0.023 (P < .001). The agreement between the 2 motor scales is moderate, with a kappa of 0.457, standard error 0.034 (P < .001). Table 2 shows the distribution of Gross Motor Function Classification System level by Manual Ability Classification Scale level for all children in the study. The Manual Ability Classification Scale level was 2 levels higher (ie, worse functioning) than the Gross Motor Function Classification System level in 17 children, 1 level higher than the Gross Motor Function Classification System level in 65 children, and they were equal in 196 children. The Gross Motor Function Classification System level was 1 level higher (ie, worse) than the Manual Ability Classification Scale level in 47 children and 2 levels higher in 7 children. Overall, 92.8% of children showed a Gross Motor Function Classification System and Manual Ability Classification Scale level that were within 1 ordinal of each other.
Distribution of Gross Motor Function Classification System and Manual Ability Classification Scale Scores for the Study Population
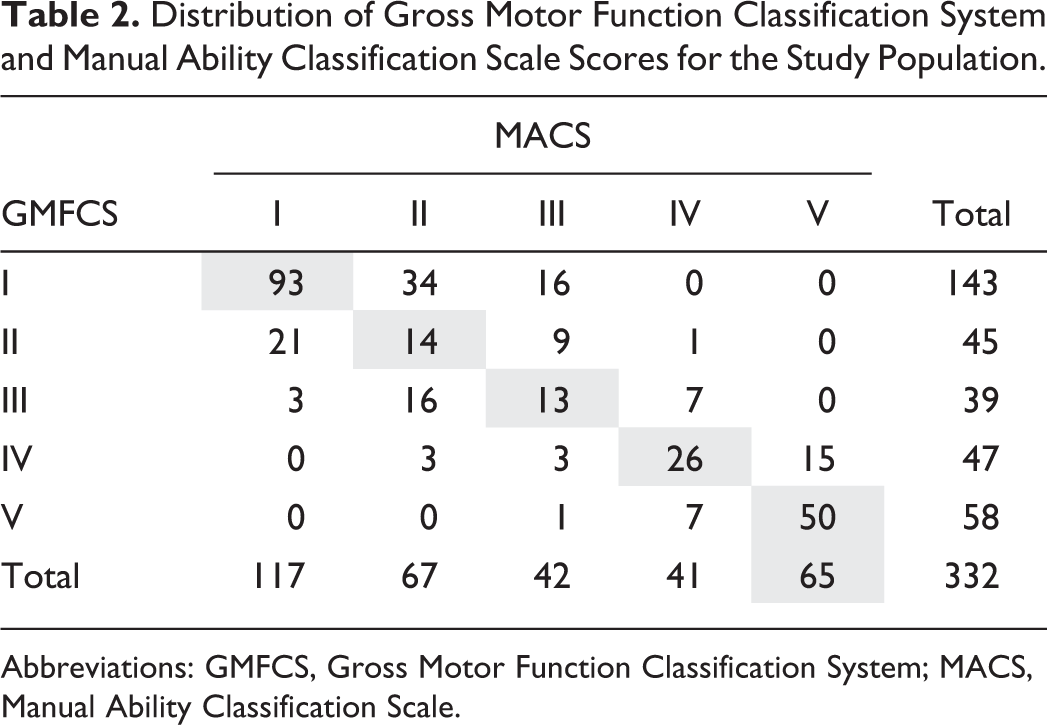
Abbreviations: GMFCS, Gross Motor Function Classification System; MACS, Manual Ability Classification Scale.
The distribution of comorbidities, correlation, and agreement among Manual Ability Classification Scale and Gross Motor Function Classification System levels were explored for the 4 most common cerebral palsy subtype groups (Table 3). The correlation between Gross Motor Function Classification System and Manual Ability Classification Scale levels were highest among children with spastic quadriparesis and dyskinetic cerebral palsy, although these still showed a positive correlation for the other cerebral palsy subtypes. The agreement between the scored levels showed a similar pattern, with a moderate agreement in children with spastic quadriparesis and dyskinetic cerebral palsy, fair agreement in children with spastic diplegia, and poor agreement in children with spastic hemiparesis. As expected, in children with a spastic hemiparesis, most children showed equal Gross Motor Function Classification System and Manual Ability Classification Scale levels (55.2%) or a Manual Ability Classification Scale level higher (lower functioning) than their Gross Motor Function Classification System level (41.9%). In children with a spastic quadriparesis, most had equal Gross Motor Function Classification System and Manual Ability Classification Scale levels (65.8%), without a significant difference in smaller groups having a higher (lower functioning) Manual Ability Classification Scale level (19.7%) or a higher (lower functioning) Gross Motor Function Classification System level (14.5%). As expected, in children with spastic diplegia, most either had equal Gross Motor Function Classification System and Manual Ability Classification Scale levels (53.5%) or a Gross Motor Function Classification System level higher (lower functioning) than their Manual Ability Classification Scale level (37.2%). The 8 children with a Manual Ability Classification Scale levels higher (lower functioning) than their Gross Motor Function Classification System level in this group all had a Gross Motor Function Classification System level of 1, with 7 having a Manual Ability Classification Scale level of 2 and 1 having a Manual Ability Classification Scale level of 3. In children with dyskinetic cerebral palsy, the majority had equal Gross Motor Function Classification System and Manual Ability Classification Scale levels (63.1%), with 31.6% showing a higher (lower functioning) Manual Ability Classification Scale level than Gross Motor Function Classification System level.
Characteristics by Cerebral Palsy Subtype
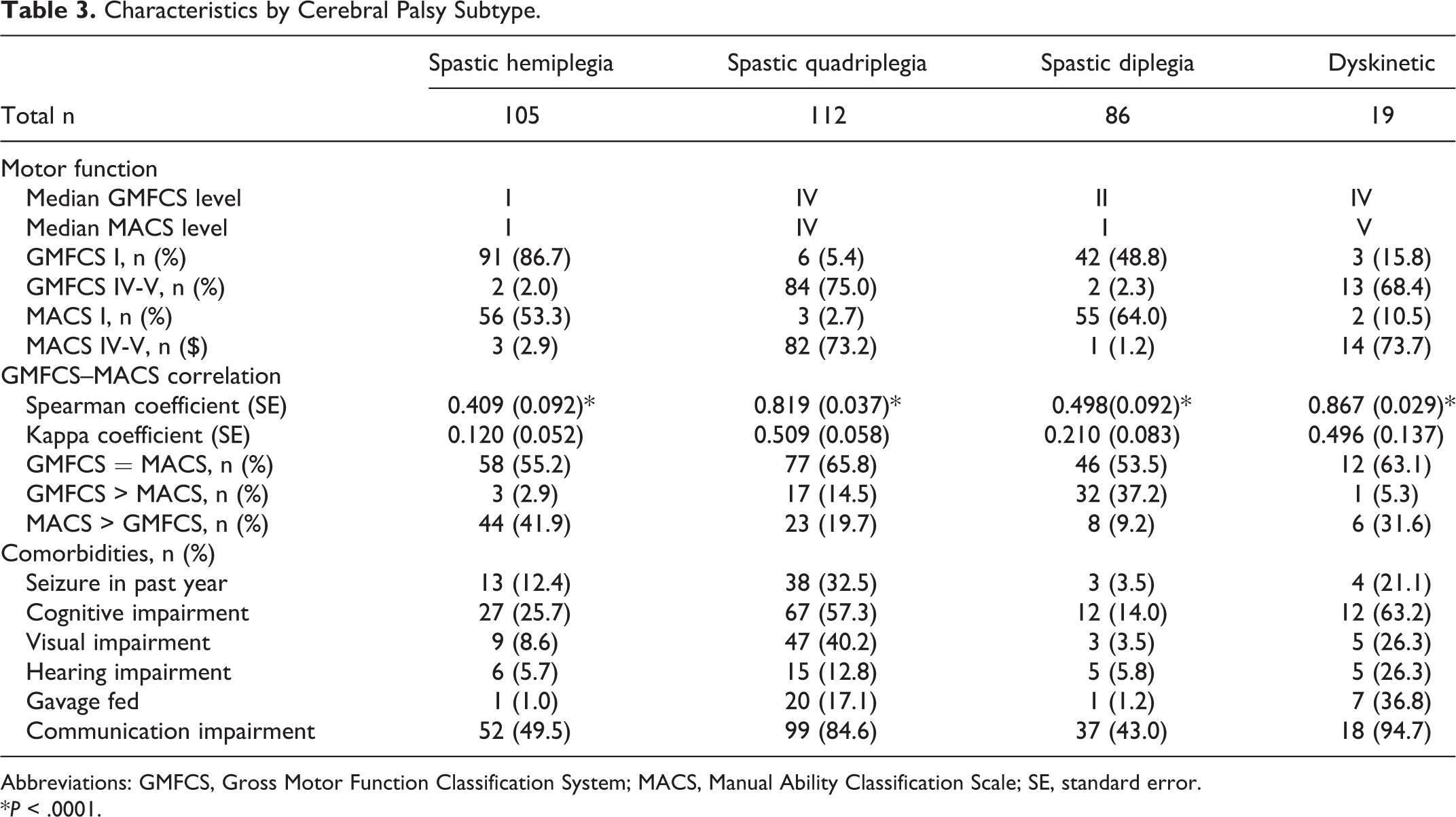
Abbreviations: GMFCS, Gross Motor Function Classification System; MACS, Manual Ability Classification Scale; SE, standard error.
*P < .0001.
The median Gross Motor Function Classification System level was IV in children with spastic quadriparesis and dyskinetic cerebral palsy, with 75.0% and 68.4%, respectively, having a Gross Motor Function Classification System level IV to V corresponding to nonindependent ambulation or nonambulation. The median Gross Motor Function Classification System levels were lower for children with spastic hemiparesis and spastic diplegia (I and II respectively), with 2.0% and 2.3% respectively having a Gross Motor Function Classification System level IV to V (nonambulant).
A separate analysis in children with and without cognitive impairment was performed, showing important differences between the 2 groups (Table 4). Children with cognitive impairment had worse gross and fine motor ability levels (median Gross Motor Function Classification System level IV, median Manual Ability Classification Scale level IV) compared to children without cognitive impairment (Median Gross Motor Function Classification System level I, median Manual Ability Classification Scale level I). The agreement and correlation between the Gross Motor Function Classification System and Manual Ability Classification Scale Levels were also higher in children with cognitive impairment although most children had equal Gross Motor Function Classification System and Manual Ability Classification Scale levels. In children without cognitive impairment, the distribution of children with a higher Gross Motor Function Classification System or higher Manual Ability Classification Scale level (lower functioning) was comparable (20.6% and 21.9%, respectively). However, in children with cognitive impairment, a greater proportion had a higher Manual Ability Classification Scale level (lower functioning) than Gross Motor Function Classification System level.
Functional Motor Levels in Children With and Without Cognitive Impairment
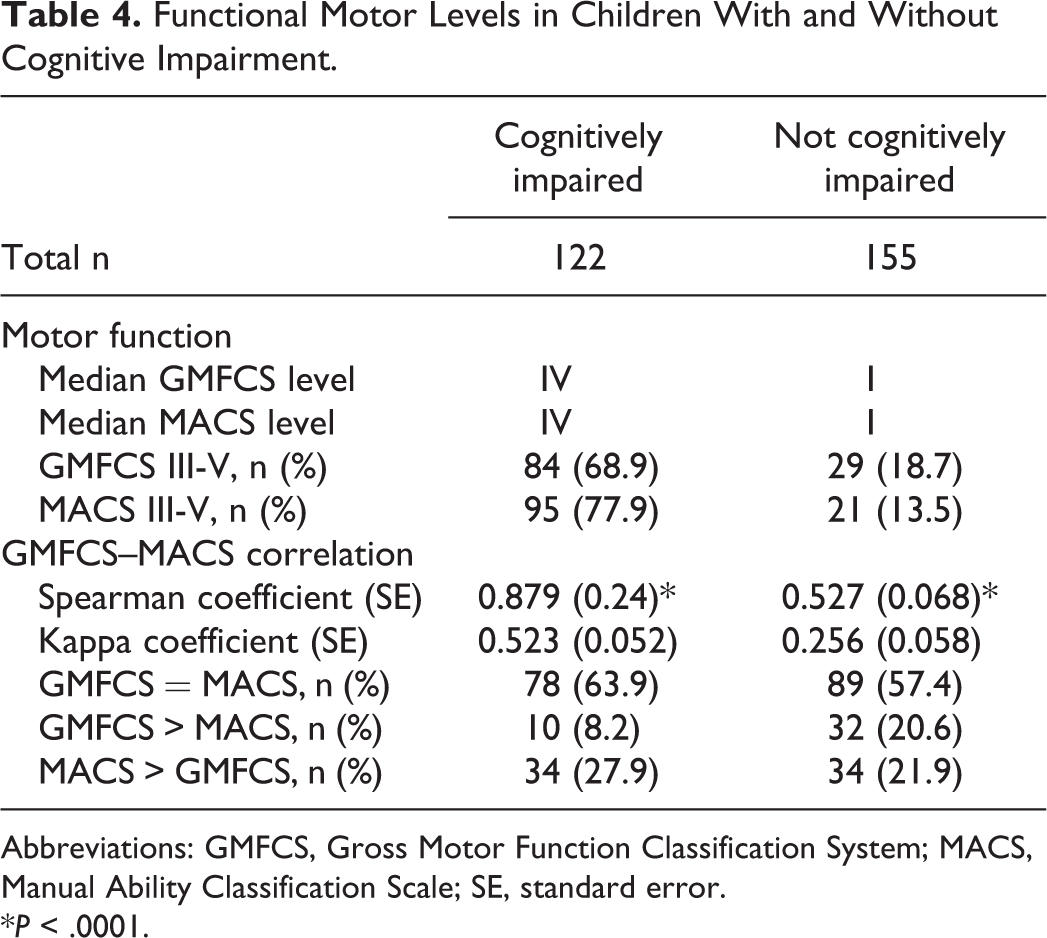
Abbreviations: GMFCS, Gross Motor Function Classification System; MACS, Manual Ability Classification Scale; SE, standard error.
*P < .0001.
Discussion
This study shows the agreement and correlation between gross motor function and bimanual ability in children with cerebral palsy as measured by the Gross Motor Function Classification System and Manual Ability Classification Scale Levels in a population-based sample of children with cerebral palsy. Only 1 previous study had explored a similar question published 5 years ago in Sweden. 5 In their cohort born between 1992 and 2001, the agreement between Gross Motor Function Classification System and Manual Ability Classification Scale Levels was found to be poor as measured by kappa, and no further correlation studies were performed. The authors highlighted a pattern of lower manual ability level than gross motor function in children with spastic hemiplegia and the reverse association in children with spastic diplegia, with no differences in children with dyskinetic cerebral palsy. Only 17 of the 359 children had bilateral spastic tetraplegia and all were found to have Gross Motor Function Classification System level V. Our study highlights similar patterns; however, we have a larger group of children with spastic quadriparesis cerebral palsy, which showed a similar distribution to the dyskinetic group. This suggests a potential difference in neurologic subtyping between the 2 registries. In a separate study on children with spastic cerebral palsy from a hospital-based convenience sample in Turkey, a good overall correlation was found between Gross Motor Function Classification System and Manual Ability Classification Scale levels, although agreement using kappa was not specifically explored. 6 They highlighted their limitation of not being able to explore the effect of cognitive level on both scales. A recently published study from North America using a case series of children with cerebral palsy showed a strong correlation between Gross Motor Function Classification System and Manual Ability Classification Scale levels. This relationship was also found to be strongest in children with spastic quadriplegia, moderate in children with spastic hemiparesis and weaker in children with spastic diplegia. The authors acknowledge that it is not a population-based sample, and they indeed have fewer children with high functioning Gross Motor Function Classification System level I than our sample. The study also was based on parent assessments of each classification system, and parent–professional agreement on Manual Ability Classification Scale levels is not well established. 7 A population-based study in Australia on children with hemiplegic cerebral palsy found only Gross Motor Function Classification System levels I to II, with Manual Ability Classification Scale levels I to III, describing a moderate agreement without kappa scores provided. 8
There is some disagreement over the classification of bilateral spastic cerebral palsy, some suggesting abandoning the distinction between spastic quadriplegia and spastic diplegia while others highlight the clinical importance of maintaining this distinction. 13,14 Children with spastic quadriplegia cerebral palsy have lower gross motor function and a higher incidence of comorbidities compared to children with spastic diplegic cerebral palsy, thus representing 2 distinct clinical phenotypes. 14 In our cohort, children with spastic quadriplegia had a higher Gross Motor Function Classification System levels, with the majority being nonindependent for ambulation or simply not ambulatory, with corresponding higher Manual Ability Classification Scale levels. In contrast, children with spastic diplegia had much lower Gross Motor Function Classification System and Manual Ability Classification Scale levels, with only a minority being nonindependent for ambulation. The correlation and agreement between the gross and fine motor functional levels also differed significantly between the 2 groups, with a higher association seen in children with spastic quadriparesis. This contributes to the evidence in favor of keeping the distinction between diplegia and quadriplegia as it carries important clinical differences.
Children with cognitive impairment also showed important differences in their motor function, with more severe gross and fine motor functional abilities. A greater proportion of these children had more severe fine motor than gross motor functional impairment compared to children without cognitive impairment. This may suggest a more significant cerebral insult, resulting in cognitive impairment, or a difference in Manual Ability Classification Scale level obtained based on cognitive level. The Manual Ability Classification Scale describes the child’s typical bimanual fine motor abilities and not their best ability, which may be dependent on cognitive level. In contrast, the Gross Motor Function Classification System level highlights the child’s best ambulation ability, which is typically independent of cognitive level.
Our study shows important strengths. It is population based, with clear and uniformly applied diagnostic criteria and definition of variables with near complete capture of the whole population of interest. It is also the first population-based North American study exploring this association to our knowledge, and the first study to explore the association to several comorbidities. Our study also has some limitations. As the Manual Ability Classification Scale was introduced after many of the children were registered and reassessed at 5 years, it was not available on all children in our cohort. Children who had not yet been reassessed at 5 years and did not have a Manual Ability Classification Scale level assigned were preferentially excluded. This may contribute to the greater number of comorbidities reported in the included group as these are often noted over time and not at the time of first assessment at 2 years of age. Although the baseline characteristics between included and excluded children were similar other than their number of comorbidities, a bias cannot be excluded if the included children had significantly different Manual Ability Classification Scale levels or were more impaired than the excluded group.
In the present study, we demonstrate a moderate agreement between Gross Motor Function Classification System and Manual Ability Classification Scale levels and a strong positive correlation. Important differences were observed between neurologic subtypes, with a stronger correlation in children with spastic or dyskinetic cerebral palsy compared to other subtypes who also had higher median Gross Motor Function Classification System and Manual Ability Classification Scale levels. Children with cognitive impairment showed a stronger correlation than children without cognitive impairment, with a higher proportion having a more severe Manual Ability Classification Scale level than Gross Motor Function Classification System level. These 2 motor function classification scales provide complementary information which may help guide planning of early intervention therapies.
Footnotes
Author Contributions
MO conducted all the statistical analyses for this study and wrote the first draft of this manuscript. MO, LD, and MS participated in data acquisition, and MO and MS were responsible for data analysis. All authors participated in concept design and interpretation of data and critically revised the manuscript and gave final approval before submission.
Acknowledgment
The Registre de la Paralyse Cérébrale de Québec consortium includes the following collaborators: Jean Mathieu, MD, Claude Desjardins, MD, Nicole Pigeon, MD, Louise, Koclas, MD, Céline Lamarre, MD, Carol Richards, PhD, Francine Malouin, PhD, Diane Munz, MD, Josée Fortier, MD, Marie-Danielle Boucher, MD, and Michel Sylvain, MD.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Registre de la Paralyse Cérébrale de Québec has been funded by the Réseau de recherche sur le développement, la santé et le bien-être de l'enfant des Fonds de Recherche en Santé du Québec and NeuroDevNet National Centre of Excellence. No funding sources were involved in the design, analysis, or manuscript preparation of this study.
Ethical Approval
Ethical permission for the Registry’s establishment and implementation has been obtained at the local host institution (McGill University Health Center Research Institute) and each participating pediatric rehabilitation centre.