
Abstract
The goal of this project was to promote bicycle helmet use via an inpatient educational program. We hypothesized that this program would increase bicycle helmet use. One hundred twenty inpatients with history of regular (>1 time per week) bicycle riding (mean age 10.0 ± 3.6 years; 67 males, 53 females; 57 whites, 59 blacks, 4 other) were randomized to treatment (n = 58) or control (n = 62) groups. All participants received a bicycle helmet. At 1 month, 50 (92.6%) of the intervention group and 48 (82.8%) of the control group wore a helmet every bike ride (P < .07). At 3 months, 50 (96.2%) of the intervention group and 44 (80%) of the controls wore a helmet with every bike ride (P < .03). The study proved feasible, requiring trained personnel to deliver the intervention. Providing a helmet without the intervention was effective in 80% to 83% of cases with respect to parental report of helmet wearing compliance.
Keywords
Epidemiologic studies report that 70% to 80% of bicycle casualty deaths are caused by traumatic brain injury. 1 There were 4924 bicycle-related deaths in children in the United States from 2000 to 2005. 2 Bicycle injury prevention studies conducted outside of hospital settings have mostly used helmet-wearing rates as outcomes; however, recent studies have measured injuries as outcomes of interventions. 3 There is evidence that education about helmet wearing produces modest gains in the rate of bicycle-helmet use but this is not sustained over time. Current rates of helmet use in the southeastern United States are very low, for example, 1% to 2%. 3
The inpatient setting creates opportunities to address some of the barriers to helmet use, including lack of injury prevention counseling, poor role modeling by parents, and negative parental pressure. 4 Families of children admitted to the hospital and the children/teenagers themselves may be especially accepting of information about an injury prevention program that would decrease chances of readmission for life-threatening traumatic injury. Parents who receive counseling from their health care provider have been shown to be more likely to report that their child always wears a helmet. 5
To date, there are no studies that have evaluated the efficacy of head injury prevention with the education of hospitalized children and their caregivers. It is thought that continuous access to children and that direct involvement of primary caregivers over 2 or more days would increase target safety awareness and child and caregiver commitment to bicycle helmet use. The overarching goal of this project is to reduce traumatic brain injury in children and adolescents, which is a leading cause of death and disability. The hypothesis was that the implementation of a Safe Kids East Central brain injury prevention program targeting children and caregivers admitted to the Georgia Health Sciences University Children’s Medical Center is feasible and that short-term treatment effects of injury prevention education on the child or adolescent and the caregiver will increase bicycle helmet use.
Methods
Subject Characteristics
One hundred twenty subjects were recruited and consented, 58 for the intervention group and 62 for the control group. Children between the ages of 5 and 18 were screened for eligibility. Inclusion criteria were as follows: (1) hospitalized in-patients in the Children’s Medical Center, (2) projected length of stay >24 hours, (3) mentally and physically fit to complete the educational program, and (4) history of regular (>1 time per week) bicycle riding. The recruitment site was the Children’s Medical Center. All gender and racial/ethnic groups were eligible for the study.
Study Protocol
This was a prospective trial conducted between September 2010 and August 2011. The subject pool was chosen from the Children’s Medical Center list of 1150 patients. Seven hundred forty-five were eliminated because of inclusion/exclusion criteria, leaving 405 subjects. Of these, 120 subjects volunteered to be in the program and were randomly assigned to intervention or control groups (see Figure 1). The Safe Kids East Central injury prevention educational program was customized for hospitalized subjects and their caregivers. Educational training sessions were conducted for the intervention-delivering personnel. The research assistant delivering the intervention had an MPH and an MBBS and was considered competent to deliver health education to patients in the clinical setting. Collection of data was through survey responses from the subject and/or his or her parents at the Children’s Medical Center and from parental interview telephone surveys following the intervention. No medical records were used in this study. Determination of eligibility was from an initial survey. The patients were not in-patients as the result of trauma. In addition to informed consent/assent, signed by the child and parent, a release form for bike helmet giveaway, approved by the Children’s Medical Center, was signed by the mother, father, or legal guardian to release the Georgia Health Sciences University from liability for any injuries or damages from the helmet use. There was no financial reimbursement for participation in the study. Study participants (both intervention and control) received bicycle safety educational materials and a bicycle helmet. Subjects were randomly assigned by flip of a coin prior to the consent process. The intervention was provided individually in privacy of the patient’s hospital room. Interaction between the control and intervention group was minimized because patients were separated by distance (separate rooms) and time (different times and days), and none of the patients to our knowledge knew each other.
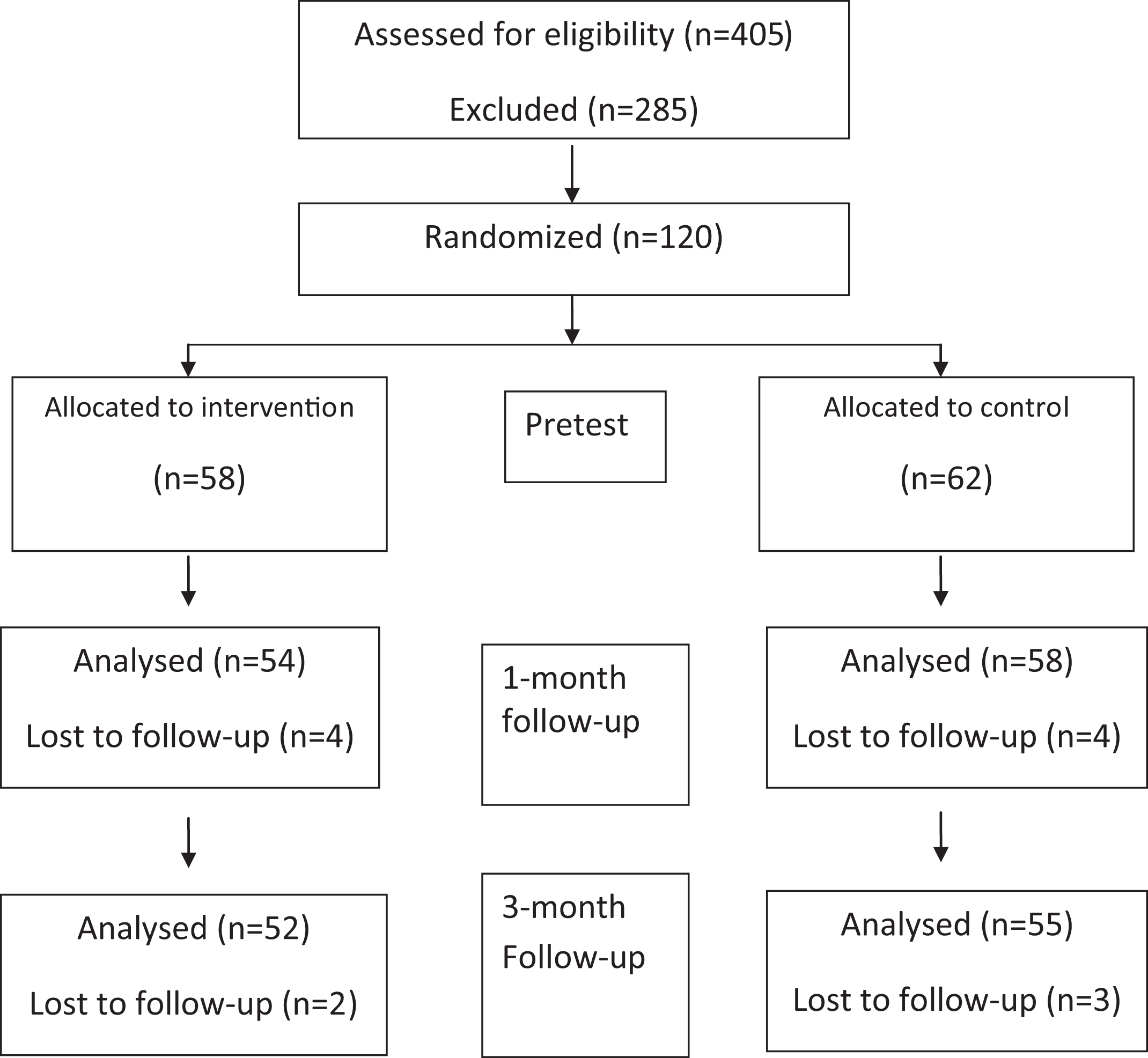
Flow of study recruitment.
Brain Injury Prevention Education Intervention
The educational intervention included case scenarios as well as education about the benefits of bicycle helmet use. The intervention was designed to be sensitive to the age and educational level of the study participant and his or her parents. Educational materials were chosen to provide use of the 5 senses to enhance the learning experience. The intervention took place in the privacy of the patient’s hospital room. The study was designed so as not to interfere with the hospital standard of care.
The brain injury prevention education included the following elements: (1) Discussion of basic brain function. The project coordinator or educator asked the children and parents what the brain does and coached them through the following basic brain functions: thinking and making decisions; sending signals to muscles for movement; balancing; using the 5 senses; and sending chemical messages for body functions, through hormones secreted by the brain. (2) Discussion of basic brain anatomy (using the brain/skull model): skull or cranium, brain, and cerebral spinal fluid. (3) Demonstration of how the brain is similar to an egg. The educator showed an egg in a sealed zip-top bag and explained that the shell is similar to the skull; the brain is similar to yolk; and the cerebral spinal fluid is equivalent to the egg white, and explained how the egg white and the shell help to protect the yolk and that the brain is protected by the skull and cerebral spinal fluid in much the same way. The educator asked, “Do you know why eggs are in special boxes and are not loose like cereal in a box?” The educator asked, “Do you use anything special to protect your brain when riding a bike, scooter, skateboard or inline skates?” The educator asked, “What could happen if a person does not use a helmet to protect the head and has a crash and hits his or her head?” The educator then dropped the egg while it is still in the sealed zip-top bag.
(4) Demonstration of gelatin brain made from a mold. The educator then asked, “What does the brain look and feel like?” (The educator demonstrated a gelatin brain made from a mold.) He or she explained that the gelatin brain is not a real brain, although there are some differences and some similarities to a real brain. The gelatin brain is much colder than a real brain and the gelatin brain smells much better than a real brain. They were asked if they could identify the peach scent of the mold. The gelatin brain, however, is very much like what a real brain looks and feels like.
(5) Simulation of a brain injury. The educator provided the participant with a blank sheet of paper and a marker. Holding up a mirror, the participant was instructed to look only in the mirror while drawing a picture, such as a clock face. Afterwards, the educator discussed the difficulty of the task and the difficulty of doing everything after a brain injury. (6) The proper way to fit the bicycle helmet was demonstrated.
The intervention was delivered by a trained research assistant. Approximately 30 to 45 minutes were required to provide the intervention depending on the age of the child, with older children needing less time. After receiving the education intervention, the subjects were certified as “helmet ready,” and subjects and caregivers were invited to sign a compliance contract. All subjects received a bicycle helmet and educational materials, including those in the control group. There was a preintervention assessment, and follow-up phone assessments at 1 and 3 months post hospitalization.
Data Analysis
The a priori power calculation modeled the projected sample size with the intentions of a significance level of alpha = .05. It indicated that a sample size of 60 in each arm of the trial would provide an effect size such that the intervention would improve reported compliance by at least 20% from baseline, based on findings from a previous study. 6 Analysis of variance was used to determine if the intervention and control samples differed at baseline with respect to demographic characteristics at baseline. Because there were a number of dependent variables, a multivariate analysis of variance was used to compare changes in groups by treatment. Effects that were significant were retained, and a series of mixed model univariate analyses were used to determine group differences across the follow-ups on helmet wearing.
Results
Random assignment to groups produced a slightly older intervention group with significant differences in age and grade at baseline (see Table 1, both Ps < .03). Subjects in both groups resided in urban, suburban, or rural locations in Richmond and Columbia counties in Georgia or in other parts of Georgia or South Carolina. Groups were similar at baseline in numbers that owned a bicycle helmet, wore their helmet, and reported having a bike. About one-third (33.3%) of the total sample owned a helmet at baseline, which did not fit in 47.6% of cases. One-fourth (24.4%) of the total sample, 13.9% more in the intervention group than controls, rode their bikes daily, whereas 8.4% more controls rode once/week and 54.5% rode every 2 weeks. Ninety-six subjects (80%) indicated that they do not ride alongside an adult. Thirty-two (26.7%) reported their yard as the main bike riding location and 23 (39.7%) in the intervention group and 39 (62.9%) controls rode their bike in the street. Those that did ride with an adult claimed that, of those adults, only 8 (6.6%) always wore a helmet while riding. 18.3% reported that their helmet did not fit. Forty-five percent of the total group had been involved in some type of bicycle-related accident; 2 of those subjects had required hospitalization as a result of their accidents (all unrelated to the present hospitalization). Only 1 in the intervention group did not think it was a good idea to wear a helmet, and 9 in the intervention group and 3 controls thought helmets should not be required.
Demographic Characteristics, Bicycle Riding, and Helmet Wearing Behavior at Baseline.
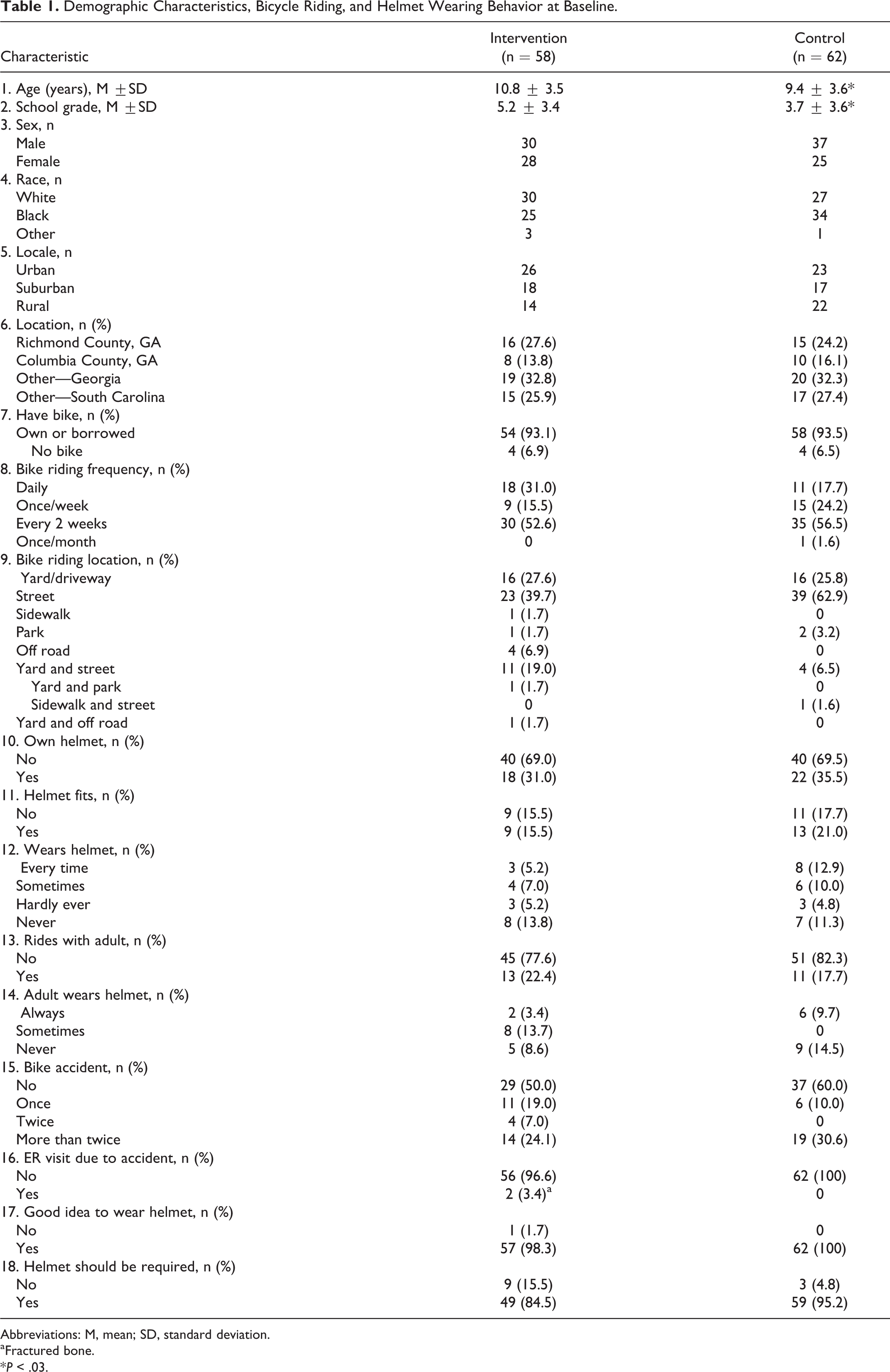
Abbreviations: M, mean; SD, standard deviation.
aFractured bone.
*P < .03.
One-Month Follow-Up
At 1 month post intervention, 50 (92.6%) of the intervention group and 48 (82.8%) of the control group reported wearing a helmet every bike ride (see Table 2, P < .07). None in the intervention group and 3 in the control group reported not wearing their helmet. Reasons given for not wearing their helmet were “helmet does not fit” and “not riding in the street” in the intervention group and “could not find helmet,” “not riding in the street” and “refused” in the control group. A total of 84.8% of the subjects were reported riding their bikes more than twice in the past month. Four subjects in the intervention group and 3 in the control group reported having a bike accident. These did not require a hospital visit. In addition, 87.5% of the parents had talked to their child about wearing a helmet.
Bicycle Riding and Helmet Wearing Behavior at 1 and 3 Months.
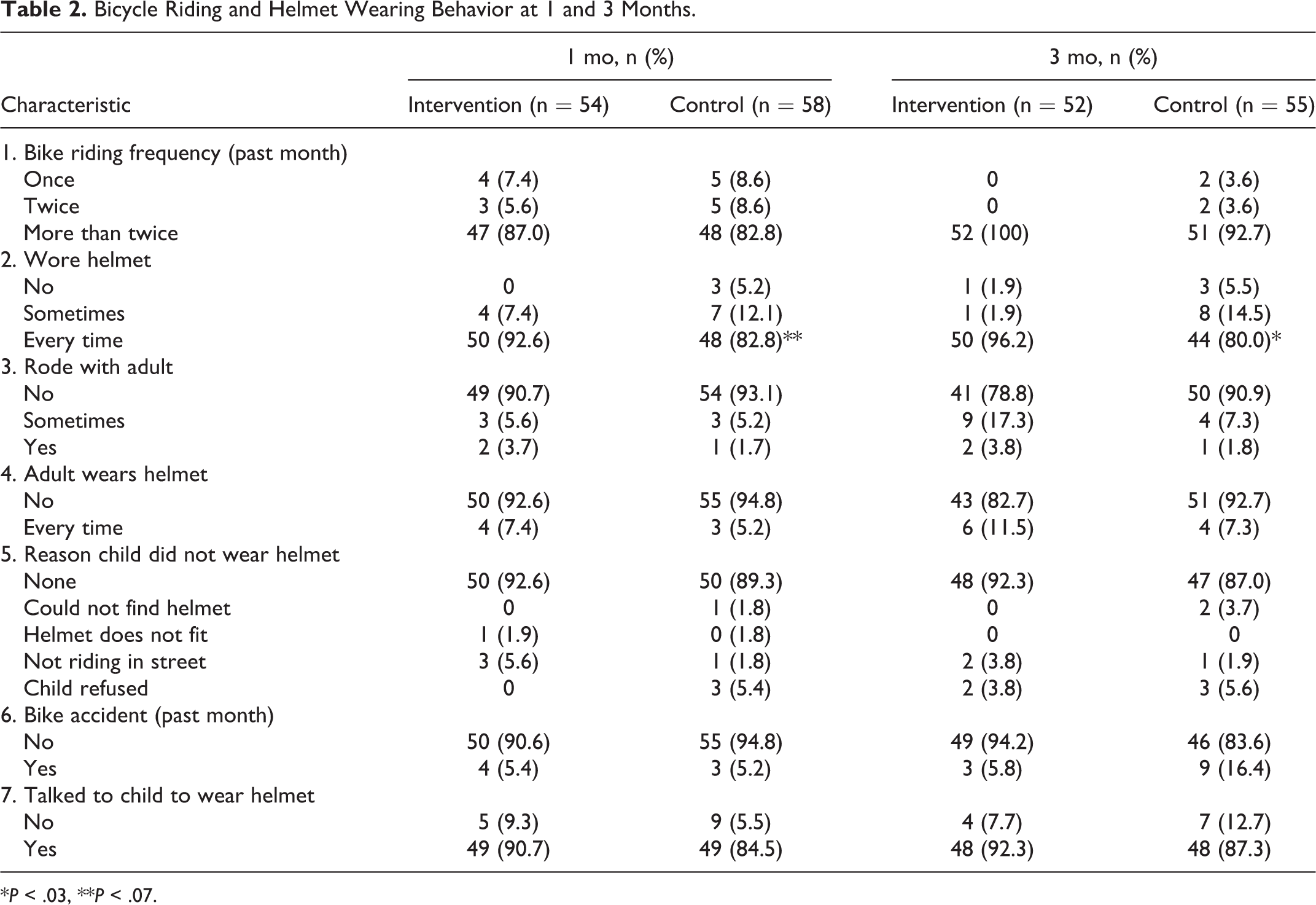
*P < .03, **P < .07.
Three-Month Follow-Up
At the 3-month follow-up, 50 (96.2%) of the intervention group and 44 (80%) of the control group reported wearing a helmet with every bike ride (P < .03). Reasons given for not wearing a helmet were “not riding in the street” and “refused” in the intervention group and “could not find helmet,” “not riding in the street” and “child refused” in the controls. Moreover, 96.3% of the parents reported their child rode their bikes more than twice in the past month. Eighty-five percent rode without an adult. One adult in the intervention group and 4 adults in the control group wore their helmets. Three in the intervention group and 9 controls reported having had an accident in the past month. Majority (89.7%) of the parents reported talking to the child about wearing a helmet. No adverse events were reported.
Discussion
The study proved feasible, requiring trained personnel to deliver the intervention and requiring costs for the helmets. Providing a helmet without the intervention was effective in 80% to 83% of cases with respect to helmet-wearing compliance. Determination of the best times to deliver the intervention was the main challenge for the study. The findings revealed a statistically significant 16.2% improvement over controls in helmet wearing at follow-up, attributable to the educational intervention.
The findings compare favorably with a helmet distribution study in an emergency department with children to improve bicycle helmet use. This study had a follow-up rate of 67% and a compliance rate with helmet wearing of 66% at 1 month. 7 In the current study, the follow-up rate was 89% and helmet-wearing compliance rate was 92.6% at 1 month; however, the study findings may not be generalizable to all medical centers. Eleven percent of the parents could not be reached by telephone after 3 attempts at different times of day. Baseline helmet ownership did not differ at baseline between groups suggesting success of the randomization procedure. The research assistant who delivered the intervention was well qualified to deliver health education but was not blinded to the study outcome. One likely threat to validity to study results is over-reporting of helmet use at follow-up by parents. One study reported that parents exaggerated helmet use by 50%; 8 however, no differences in reporting validity were found between intervention and control group families in another home safety study. 9 In the current study, parents were poor role models for their children, with only 5% to 6% of the parents wearing a helmet every time at the follow-ups. It appears the intervention had little impact on the parents and needs to target the parent as well as the child to improve effectiveness.
The findings imply that direct education on helmets to child and caretakers in a hospital setting works. What this suggests is that health establishments have a significant role in promoting helmet use. This should include at a minimum, provision for a helmet or subsidy for a helmet at the time of contact. The current findings suggest that in addition to providing a helmet, providing reasoning to the child in the hospital setting regarding the importance of wearing a helmet has been shown to be of greater benefit long-term to their usage behavior. This study provides a model for how this intervention might work in other health settings. The implementation cost for helmets and staff time needed for intervention are minimal compared to the benefit in terms of traumatic brain injury prevention.
This project extended the reach of Safe Kids East Central led by Georgia Health Sciences University’s Children’s Medical Center that promotes bicycle helmet use in our community. This project provides the scientific community and the medical field with a new translational tool that could be used in the hospital to help reduce traumatic brain injury in adolescents and youth and thereby contribute to public health.
Footnotes
Acknowledgments
This study was conducted at the Children’s Medical Center, Augusta, Georgia. The findings were presented to the Society of Behavioral Medicine 33rd Annual Meeting and Scientific Sessions in New Orleans, Louisiana, April 2012. We gratefully acknowledge Kiet Nguyen, who assisted with intervention development and power analysis; V. Pradeep Shenbagarajan, MBBS, MPH, who delivered the intervention, collected the data, and enrolled and assigned patients to groups; Harry Davis, for consultation on the data analysis; Gwen Bulluck, who assisted with the follow-up; and Catherine L. Davis, PhD, for editing assistance. We thank the staff of the Children’s Medical Center for their cooperation in making this study possible.
Author Contributions
VB designed the study, designed the data collection instruments, coordinated and supervised data collection, and drafted the initial manuscript. BM conceptualized and secured funding for the study. ALC facilitated recruitment, and reviewed and revised the manuscript. IH provided the training for the intervention delivery and reviewed and revised the manuscript. All authors approved the article as submitted.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Georgia Health Sciences Foundation GHSF11085. The authors have no financial relationships relevant to this article to disclose.
Ethical Approval
Ethics approval was obtained by the Georgia Health Sciences University Institutional Review Board.