
Abstract
This study determined the extent to which parents of adolescents with cerebral palsy seek out complementary and alternative medicine services. A regional sample of 166 adolescents (15.5 ± 2.4 years) with cerebral palsy were recruited. Parents completed a questionnaire identifying the complementary and alternative medicine services received over the past year. Most (73.2%) did not currently utilize any of the listed services; 7.3% used 2 or more services. The most commonly used services were massage (15.4%), hyperbaric oxygen (9.6%), and osteopathy (5.7%). Youth with limited hand function were more likely (P = .01) to undergo hyperbaric oxygen. Massage therapy services were more frequent in youth with greater activity limitations (P < .005). Sociodemographic factors were not predictive of use. Approximately one quarter of families sought out these services for their adolescents with cerebral palsy. Many are expensive privately funded treatments. Physicians should openly discuss these options with families, highlighting the current state of knowledge on their efficacy.
Keywords
Complementary (in addition to) and alternative (as a substitute to) medicine services are not part of current standard conventional medical or rehabilitation treatments and care. They include products or therapeutic approaches not traditionally carried out by physicians, nurses, psychologists, and occupational or physical therapists. 1 Many of these methods are becoming increasingly “conventional” in particular regions or cultures, and therefore accurately defining these services is a moving target. Generally complementary and alternative medicine treatments can include approaches for (1) “mind-body” healing such as meditation, prayer, hypnosis, or music, art, or dance, (2) biologically based methods such as vitamins or natural products that have not been scientifically shown to treat specific health conditions, (3) body manipulations such osteopathy, chiropractic manipulation, or massage, (4) alternative medical treatments such as homeopathy or acupuncture, and (5) energy or bio-magnetic therapies such as Qigong, craniosacral therapies, and magnetic fields. 1-3 The effectiveness of most of these treatments for the child’s specific health condition is not currently adequately substantiated by empirical evidence and side effects are usually unknown. 4 Nonetheless, families will seek these interventions to either complement or replace traditional medical care. When asked to rate their primary care physicians knowledge on quality and satisfaction with service, families of children with special needs rated their physicians’ knowledge about complementary and alternative medicine as low (worse than neutral). 5
Few studies have examined the prevalence of use of complementary and alternative medicine in children and youth with cerebral palsy or the factors associated with their utilization. In adults with physical disabilities, 19% used complementary and alternative medicine, which was associated with female gender, western US location, and prior use. 6 In a sample of children with chronic health conditions, 23% used complementary and alternative medicine, whereas in a sample of children (0-18 years) with cerebral palsy, 56% used complementary and alternative medicine. Lack of independent mobility, younger age, and parental use of complementary and alternative medicine were the most important predictors of use. 3
Reasons reported for using complementary and alternative medicine for individuals with physical disabilities include pain, decreasing function or severe limitations, lack of energy, and to improve sleep and relaxation. 6-8 It is likely that the decision to use these treatments is empowering to families, as this provides them with options that they can choose to pursue to optimize their child’s health and well-being.
Greater knowledge about the extent of use of complementary and alternative medicine services and the determinants of use is important for health care professionals so as to understand families’ reasons for pursuing these complementary treatment options and to counsel and support families effectively. There is a paucity of empirical data on complementary and alternative medicine use and predictors in adolescents with cerebral palsy. Therefore, the objective of this study was to determine the extent to which adolescents with cerebral palsy receive complementary and alternative medicine services and to identify factors associated with the use of these services.
Methods
This is a secondary analysis of data collected on a study whose primary purpose was to describe factors associated with the quality of life and participation in adolescents 12-19 years of age with cerebral palsy. This study was ethically approved by the Research Ethics Board of the Montreal Children’s Hospital (PED-06-043). Consent was obtained from a parent or guardian, and assent was also received by the participant (adolescent) when feasible. Adolescents recruited met the current consensus definition of cerebral palsy 9 and were examined by a neurologist to determine specific motor subtype (eg, spastic, dystonic, hypotonic) and distribution (eg, diplegia, hemiplegia, quadriplegia).
As part of data collection for this study, parents completed a formal questionnaire on sociodemographic factors and current services, which included the following question on complementary and alternative medical services: “In the
As part of this questionnaire, categorical information was also collected on maternal education (ranging from high school or less to university degree) and total family income (5 categories ranging from <$20,000 to >$80,000).
Participants were evaluated by an occupational or physical therapist and psychologist. Adolescents were classified in terms of the severity of motor function using the Gross Motor Function Classification System 10 and the Manual Ability Classification System. 11 Intellectual ability was measured using the Leiter Brief IQ. 12 Internalizing and externalizing behavior problems were measured by parental report using the Strengths and Difficulties Questionnaire. 13 In addition, activity limitations across domains were ascertained by semistructured interview using the Vineland Adaptive Behavior Scale–2nd edition. 14 Family context was evaluated by parent report using the Family Environment Scale. 15 These measures all have acceptable psychometric properties, are age appropriate, and may be used on adolescents with cerebral palsy.
Statistical Approach
Descriptive statistics were applied to characterize the sample and provide a profile of use of complementary and alternative medicine interventions. Factors considered that could be associated with a greater use of complementary and alternative medicine were sociodemographic factors (maternal education, total household income, age, gender), cognitive impairments (Leiter Brief IQ), behavior problems (Strengths and Difficulties Questionnaire), activity limitations (Vineland Adaptive Behavior Scale–2nd edition), and family environment (Family Environment Scale). Simple logistic regressions were applied with the dependent variable being use of complementary and alternative medicine (yes/no). The 2 most commonly utilized complementary and alternative medicine services were also considered as dependent variables (yes/no for hyperbaric oxygen and massage) in separate models.
Results
Group Characteristics
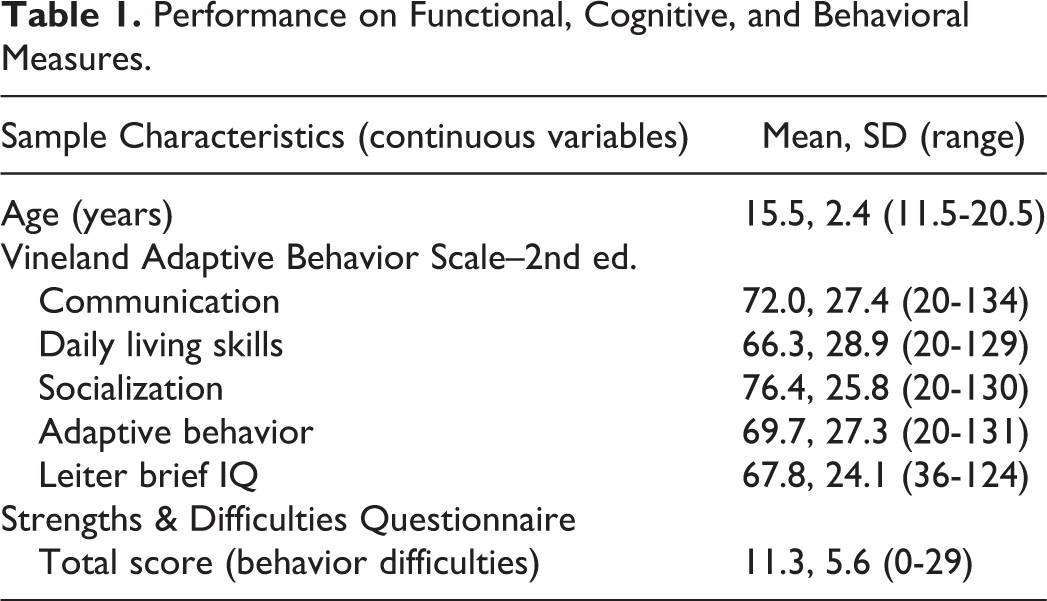
A regional sample of 166 adolescents (58.8% male) with cerebral palsy participated in this study. Mean age at testing was 15.5 years, (SD = 2.4, range 11.5-20.5). As expected based on local population-based registry data, 16 most adolescents were self-ambulatory but may have required aids or adaptations (Gross Motor Function Classification System I: 31.4%, II-III: 35.2%, IV-V: 33.3%). Most adolescents were able to handle objects to perform daily activities, although many may have required some adaptation or assistance (Manual Ability Classification System I: 28.9%, II-III: 44.0%, IV-V: 27.0%). Performance ratings on cognitive (Leiter Brief IQ), behavioral (Strengths and Difficulties Questionnaire), and functional (Vineland Adaptive Behavior Scale–2nd edition) measures appear in Table 1. Mothers had either high school education or lower (32.5%), junior college (32.5%), or undergraduate/graduate degrees (35.0%). Total household income was under $40,000 for 30.6%, $40,000-$80,000 for 26.7%, and >$80,000 for 42.7%.
Performance on Functional, Cognitive, and Behavioral Measures.
Use of Complementary and Alternative Medicine
Of 183 recruited, 166 families (91%) completed the survey on complementary and alternative medicine services. Findings indicate that 73.2% did not currently (ie, within the past year) use any of the complementary and alternative medicine services listed; 26.8% used at least 1 service; 7.3% used 2 or more services. The most common complementary and alternative medicine services used were massage therapy (15.4%), hyperbaric oxygen (9.6%), and osteopathy (5.7%). Less than 5% claimed use of a special diet (4.1%), herbal/naturopathic remedies (3.6%), chiropractic manipulations (2.4%), homeopathy (1.6%), or acupuncture (0.8%). Treatments listed in the “other” category included conductive education, Alexander technique, amino acids, hippotherapy, and faith.
Factors Associated With Use of Complementary and Alternative Medicine
Youth with more limited gross motor function (higher Gross Motor Function Classification System, P = .001, β = .09, r2 = .13) and manual ability (higher Manual Ability Classification System, P < .001, β = .11, r2 = .07), greater activity limitations across domains (communication: P = .003, β = –.005, r2 = .06; daily living skills: P = .007, β = –.004 r2 = .05; socialization: P = .017, β = –.004 r2 = .07), and lower IQ (P = .035, β = –.006 r2 = .003) were more likely to use complementary and alternative medicine services. Family’s intellectual/cultural orientation (Family Environment Scale) was modestly associated (P = .057, β = .007, r2 = .02) with the greater use of complementary and alternative medicine. These relationships were statistically significant but weak associations overall (strongest being the severity of motor dysfunction), suggesting that other factors mediate decisions regarding the use of complementary and alternative medicine. Sociodemographic factors (age, gender, maternal education, family income) were not predictive of complementary and alternative medicine.
Factors Associated With Use of Massage Therapy
Motor function levels were associated with massage treatment such that youth with more limited manual ability (P < .001, β = –.10, r2 = .14, 67% Manual Ability Classification System IV-V) and gross motor function (P < .001, β = –.09, r2 = .15, >70% Gross Motor Function Classification System IV-V) was more likely to use massage therapy. Indeed, activity limitations across domains was associated with massage therapy use (Vineland Adaptive Behavior Scale–2nd edition daily living skills: P < .001, β = –.004 r2 = .10, communication: P < .001, β = –.004, r2 = .10, socialization: P = .006, β = –.004, r2 = .06, adaptive behavior: P < .001, β = –.005, r2 = .10). Lower IQ had a modest association with use of massage treatment (P = .02, β = –.003, r2 = .06).
Factors Associated With Use of Hyperbaric Oxygen
Overall, activity limitations were not an important determinant of use of hyperbaric oxygen with the exception of limited manual ability (> half IV-V) which was only weakly associated with greater use of this service (P = .039, β = .03, r2 = .03). There was a trend for Family Expressiveness (P = .07) and Family Conflict (P = .08) to be associated with the use of complementary and alternative medicine, although this did not reach significance.
Discussion
Individuals typically will seek complementary and alternative medicine services to augment the repertoire of treatments available for their child and to provide greater control and hope. 1 In the general population, complementary and alternative medicine therapy such as chiropractic manipulations, massage, herbal and other dietary therapies, and spiritual healing are increasingly used, especially in children and adults with chronic health conditions. 8 To our knowledge, only 1 study surveyed the use of different complementary and alternative medicine treatments in a sample exclusively of children with cerebral palsy and identified factors that are associated with use. 3 Overall, studies on children with developmental disabilities suggest that a wide range of treatment options may be utilized to include mind-body interventions, body-based manipulation methods, and energy therapies. 2 Nonetheless, studies to support the actual effectiveness of these treatments on a relevant outcome in this population of interest are lacking. In Liptak’s review, 17 complementary and alternative medicine techniques such as patterning, craniosacral, and other touch therapies have been shown not to be more effective than placebo. Interpretation of studies on other complementary and alternative medicine approaches such as conductive education is inconclusive, based on the existing evidence. Unfortunately, several of these treatment options are largely supported by anecdotal reports and not by scientific evidence. 4 On the other hand, recent systematic reviews have shown that hippotherapy is effective at the impairment level (muscle symmetry) and in improving gross motor function. 18
In our sample, 26.8% of adolescents were using 1 of the complementary and alternative medicine services identified in our survey. Reports of prevalence in other samples of children with special needs are wide-ranging. For example, 23% of 194 children with chronic medical conditions in Ontario, Canada claimed use of complementary and alternative medicine in 1 survey although prevalence was 35% in the subset of children with cerebral palsy. 8 In another sample of 376 children with special health care needs (18% with cerebral palsy) in Arizona, 64% reported using complementary and alternative medicine, with spiritual healing noted as most popular. 19 In a comparison study in the United Kingdom, children with chronic health conditions (cerebral palsy, inflammatory bowel disease, cancer) were more likely to use complementary and alternative medicine than healthy peers (40% as compared to 12%; 56% in the cerebral palsy group). 20 In the study by Hurvitz et al 3 on a sample of 213 children 0 to 18 years of age with cerebral palsy in Michigan, USA, prevalence of use was 56%. Differences across samples likely relate to sample characteristics (age, severity, socioeconomic factors) and environmental factors (local availability of services, geographic variation, insurance coverage). Furthermore, the type of complementary and alternative medicine services specified in the survey may also influence prevalence reports. 19
Our findings on the popularity of massage therapy as a complementary treatment further substantiates findings by Glew et al 7 on massage use in 104 children with cerebral palsy (17 months to 21 years; United States). In this study, 51% (compared to 15.4% in our sample of adolescents) were currently receiving massage, although only 23% from a trained professional. In another study 3 on children with cerebral palsy, 25% used massage therapy. A greater severity of disability was also found to be a predictor of massage therapy use in these other studies. 3,7 Massage therapy may be administered by a massage therapist, physical therapist, or other individual.
Hyperbaric oxygen was used in close to 10% of adolescents in our regional sample, in spite of objective evidence from a randomized trial that demonstrated no advantage above placebo of this costly treatment. 21 Local availability and strong endorsement by family groups likely influenced the popularity of this treatment method. Prevalence of use in the study by Hurvitz and colleagues 3 was 6%. The scientific rationale for this costly treatment has been repeatedly challenged in terms of the likelihood of pressurized oxygen to activate dormant cells in the areas of tissue necrosis in the brain. 4,22
Adolescents more likely to use complementary and alternative medicine treatments in our sample were those with greater activity limitations in motor function, confirming findings by others, 3,8 but also those with limitations in all other activity domains. This relationship appears to be primarily for use of massage therapy. Sociodemographic factors such as family income were not significantly associated with the use of complementary and alternative medicine, which is generally supported by most studies. In the study by Hurvitz et al, 3 higher maternal education was only weakly associated. Younger age, in samples that included younger children, was found to be associated with greater complementary and alternative medicine use. 3 The actual number of adolescents using complementary and alternative medicine in our sample was small, which may have limited our ability to identify predictor variables. Previous studies suggest that parental use of complementary and alternative medicine is an important determinant of concurrent use in their child. 3,19 In our study, there was a modest relationship between family relationship dimensions (expression of feelings, expression of anger/conflict) and the use of hyperbaric oxygen. Families with a greater interest in cultural and intellectual activities were more likely to use complementary and alternative medicine. These relationships would need validation, but suggest that family environmental factors (cultural beliefs, family coping) can exert influences on complementary and alternative medicine use.
Other treatments (eg, osteopathy, chiropractic, herbal/naturopathic, special diet, homeopathy, acupuncture, conductive education, meditation/prayer, hippotherapy) were less often used. It is likely that the popularity of particular complementary and alternative medicine treatments are influenced by local contextual factors related to availability and knowledge by the particular community about options for children with cerebral palsy. In the other study 3 focusing on children with cerebral palsy, most common complementary and alternative medicine interventions used were 40% prayer, 25% massage therapy, 25% aquatherapy, 18% hippotherapy, 12% chiropractic manipulation, 10% conductive education, 8% craniosacral therapy, 6% Adeli Suit, 6% special diet, 6% hyperbaric oxygen. Some of these treatments such as hippotherapy have demonstrated increasing scientific evidence to support their efficacy, and will likely gain popularity with time.
The strengths of this particular study are the application of standardized measures to ascertain activity limitations and family environmental factors and the distribution of severity of cerebral palsy that is comparable to a population-based cerebral palsy registry sample. 16 Furthermore, this study focuses specifically on adolescents with cerebral palsy, a stage of transitional development when the individual is likely to make individual increasingly autonomous personal choices about treatment use. A limitation is that parent report is the source of determination of complementary and alternative medicine use, which may not be entirely accurate. Furthermore, sample size for those using complementary and alternative medicine treatments limits the determination of predictor variables that may have a modest effect on service utilization.
Complementary and alternative medicine such as massage, chiropractic, meditation, and spiritual healing, yoga, and natural products are increasingly pursued as a treatment for a variety of conditions and health concerns by the public at large. In most cases, families are using these treatments as an adjunct to traditional medical approaches. 8 It is conceivable that the core belief in complementary and alternative medicine therapies have a powerful placebo (Hawthorne) effect. Physicians need to be aware of the current trends in use of these complementary treatments, the evidence either supporting or discrediting the effectiveness of these interventions. 4 Physicians should openly discuss and respond to questions about complementary and alternative medicine options with families of children with cerebral palsy and with the adolescents themselves, highlighting the current state of knowledge on their efficacy, potential risks, and side effects. 1,17
Footnotes
Acknowledgements
Many thanks to the adolescents and families that participated in this study. We wish to thank Anna Radzioch, our research coordinator, for her efforts on this project. We would also like to acknowledge the contributions of the evaluators who assessed participants in the study: occupational therapists—Noemi Dahan-Oliel, Rena Birnbaum, and Claudia de Luca; physiotherapists—Melissa Turner and Shannon McShane; psychologists—Lisa Steinbach, Mafalda Porporino, Chantal Martel, Catherine Zygmuntowicz, and Sarah-Jane Renaud; neurologists—Dr Shevell, Dr Poulin, Dr Moore, Dr Rosenblatt, Dr Srour, Dr Tremblay, and Dr Oskoui. This article was presented at the Child Neurology Society meeting, October 2012.
Author Contributions
AM conducted the analyses and wrote the manuscript. KST, MIS, CP, LL, NS, and ML contributed to the conceptualization of the research proposal and the interpretation of the findings and provided feedback before submission. The QUALA Group includes the following collaborators: Michele Gardiner, Danielle Guimond, Celine Lepage, France Martineau, Kathleen Montpetit, and Sylvie Thibault. These individuals assisted with the recruitment of participants and were asked to provide feedback on the research proposal and the manuscript submitted for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is a secondary analysis of a study on participation and quality of life of adolescents with cerebral palsy. This study was funded by REPAR and the Canadian Institutes of Health Research MOP-84261 with Annette Majnemer as principal investigator. In addition, we benefited from research infrastructure provided by the Montreal Children’s Hospital Research Institute and the Centre de Recherche Interdisciplinaire en Réadaptation du Montréal Métropolitain (CRIR), both funded by the Fonds de la Recherche en Santé du Québec (FRSQ). KS was supported by doctoral fellowship awards provided by the Canadian Child Health Clinician Scientist Program, NeuroDevNet, and the Montreal Children’s Hospital Research Institute/Foundation of Stars.
Ethical Approval
This study was approved by the Research Ethics Board of the Montreal Children’s Hospital. Parents provided written consent, and, when feasible, adolescent participants provided written assent.