
Abstract
Neurocysticercosis is a common parasitic infection of the central nervous system. Intraparenchymal giant cysticercosis has been described in literature, but this is a rare report of a thalamic giant cysticercosis in a young child where the diagnosis could be made on follow-up. A 1½-year-old male child presented with seizures, hemiparesis, and features of raised intracranial pressure. Initial neuroimaging findings of thalamic swelling with minimal edema and contrast enhancement with choline peak on magnetic resonance spectroscopy were attributed to thalamic glioma. Subsequent imaging revealed a ring enhancing lesion with an eccentric nodule suggestive of neurocysticercosis. It later resolved with residual gliosis. The presence of a pathognomic scolex and the resolution of size and symptoms without definitive treatment helped in making the diagnosis. This report reinforces the importance of considering cysticercosis in diagnosis of acute presentations of large cerebral masses in infants, particularly in prevalent regions, and emphasizes the follow-up of these patients.
Cysticercosis is a common parasitosis with tropism for the central nervous system causing neurocysticercosis. 1 The diagnosis of neurocysticercosis is suspected by clinical presentation and confirmed with radiological features. Giant neurocysticercosis is a rare finding when it measures more than 4 or 5 cm in its largest dimension. 2 The authors report a rare case of a thalamic giant neurocysticercosis in a young child presenting as seizures and hemiparesis where the diagnosis was established at the second visit.
Case Summary
A 1½-year-old male child with normal premorbid development presented at another center with sudden onset of generalized seizures and vomiting followed by left-sided hemiparesis over 3 to 4 days. On examination, the child was lethargic and had a head circumference of 49 cm, with no dysmorphism or neurocutaneous markers, but he had left hemiparesis. There were no cranial nerve palsies, nystagmus, or meningeal signs.
Contrast-enhanced computed tomography (CT) of the head showed a hypodense lesion, 4.3 × 4.5 cm in size, causing diffuse enlargement of the right thalamus with the eccentric scolex in the inferior cyst wall, with minimal peripheral enhancement and moderate perilesional edema. It was causing mass effect in the ipsilateral lateral ventricle and gangliocapsular region (Figure 1A). Subsequently, contrast-enhanced magnetic resonance imaging (MRI) of the brain with spectroscopy was done, which confirmed the CT findings (Figure 1, B and C). Single-voxel magnetic resonance spectroscopy revealed increased choline peak and decreased N-acetyl aspartate, suggestive of a neoplastic origin. Electroencephalography (EEG) was normal. The seizures were controlled initially with injectable and later oral phenytoin sodium. Mannitol was administered along with conservative measures to reduce intracranial pressure. The parents were counseled at that center regarding the need for biopsy, possible surgery, radiation therapy, and adjuvant chemotherapy. However, they agreed only on administration of oral phenytoin and refused any other intervention. The hemiparesis improved gradually. The child was discharged from the hospital.
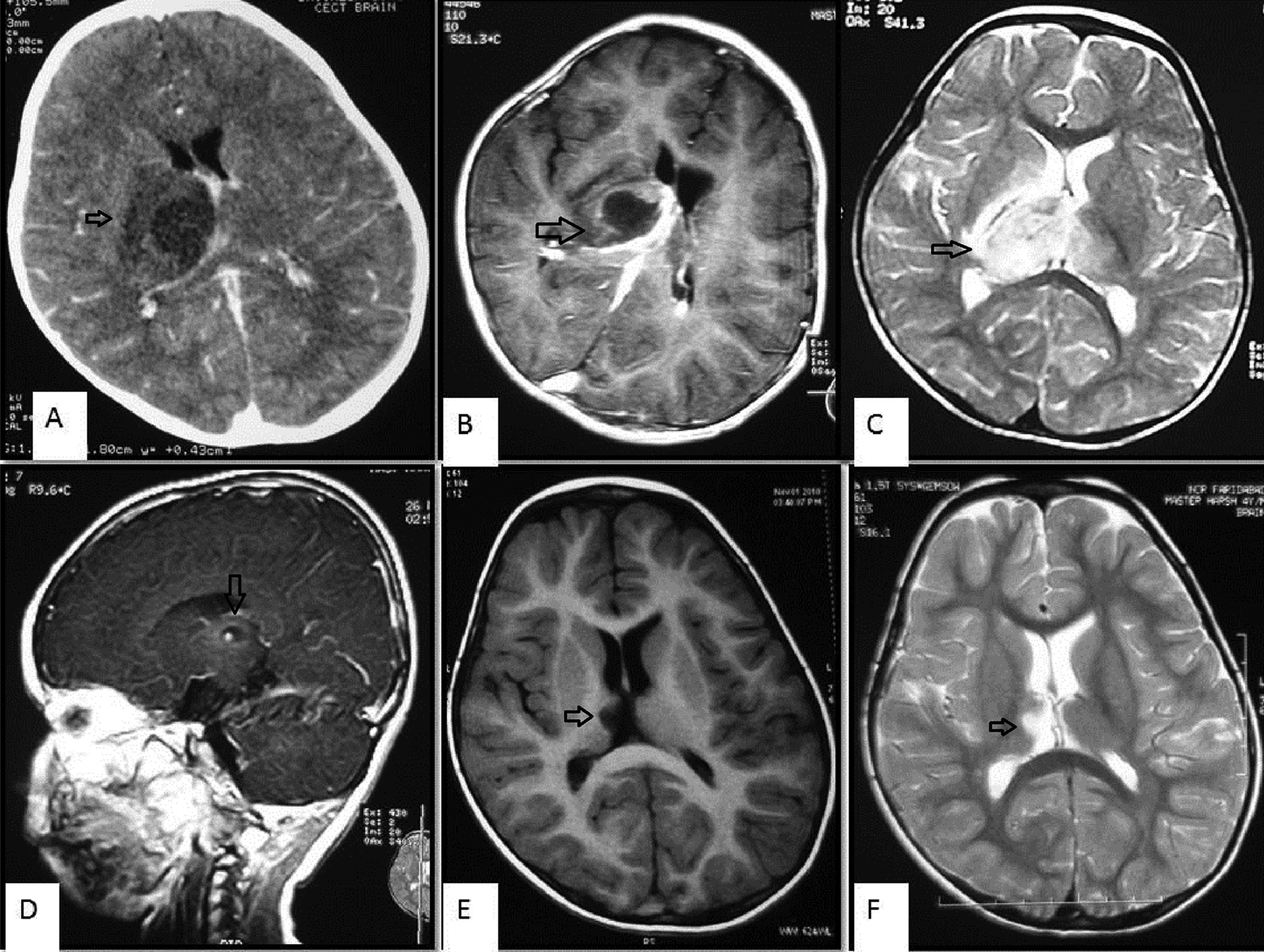
(A) Axial contrast-enhanced computed tomography (CT) scan showing a hypodense lesion in the right thalamus with the eccentric scolex in the inferior cyst wall, mild peripheral enhancement, and moderate perilesional edema with compression of the ipsilateral lateral ventricle. (B) Axial contrast-enhanced T1-weighted magnetic resonance image (MRI) showing a hypointense lesion in the right thalamus with mild peripheral enhancement. (C) Axial T2-weighted MRI showing a heterogeneously hyperintense lesion with moderate perilesional edema and mass effect in the lateral ventricles. (D) Sagittal T1 contrast-enhanced MRI showing a cystic lesion with the scolex in the right thalamus. (E, F) Axial T1- and T2-weighted MRIs showing a residual gliotic focus in the right thalamus.
The child presented 4 months later at the authors’ center with a breakthrough seizure. Repeat brain MRI at this time revealed a ring enhancing lesion with eccentric nodule in the right thalamus suggestive of neurocysticercosis granuloma (Figure 1D). The patient was prescribed albendazole under cover of steroids, but treatment was refused by the parents as they had opted for indigenous traditional practices. The child was lost to follow-up. Four years later, he again presented to the authors’ center with another seizure with status epilepticus. However, brain MRI at this time revealed only a small gliotic focus in right thalamic region (Figure 1, E and F).
Discussion
The present case describes a giant thalamic neurocysticercosis that was mistaken for a glioma at initial presentation at another center. However, the sudden onset of the typical neurological picture of neurocysticercosis supported by neuroimaging findings and rapid improvement with conservative management make a malignant tumor very unlikely. Cerebral cysticercosis is rare in patients under 2 years of age. 3 But a few previous reports have documented neurocysticercosis in children less than 18 months of age. 4 -7 Furthermore, cysticercosis is endemic to India. 8 An elevated choline peak in magnetic resonance spectroscopy can be seen in both tumors and neurocysticercosis 9,10 but was wrongly attributed to a tumor.
The clinical manifestations of neurocysticercosis are pleomorphic and depend on the number and location of cysts as well as the host immune response to the parasite. Patients commonly present with seizures, headache, and vomiting. Less common presentations include encephalopathy, ataxia, sensory deficits, involuntary movements, stroke-like symptoms, isolated focal myokymia, and Millard-Gubler syndrome. 11,12 The neuroimaging findings of neurocysticerci vary with the stages of degeneration: namely, vesicular stage, colloidal vesicular stage, granular nodular stage, and nodular calcified stage.
In the present case, at the time of initial presentation, the cysticercus appeared to be in an early degenerating stage because of perilesional edema and mild enhancement of its capsule. The typical size of cysticercus ranges between 4 and 20 mm. However, this was an unusually large cyst. The presence of a pathognomic scolex within the cystic lesion seen in the present case is an absolute criterion for making the diagnosis of neurocysticercosis. 13 This produces the so-called “hole-with-dot” imaging.
The commonly used serum enzyme-linked immunosorbent assay for anticysticercal antibodies or cysticercal antigens cross-reacts with other cestode infections like Hymenolepis nana and Echinococcus granulosus. 14 Enzyme-linked immunosorbent assay of the cerebrospinal fluid has more sensitivity and specificity. However, lumbar puncture is not recommended only for performing enzyme-linked immunosorbent assay because of associated pain and invasiveness. The enzyme-linked immunoelectrotransfer blot assay using purified extract of Taenia solium is reported to have a sensitivity of 98% and specificity of 100%. 15 However, its sensitivity in case of a single enhancing or calcified lesion is much lower, 16 and its availability is limited. Enzyme-linked immunoelectrotransfer blot assay is one of the stipulated major criteria whereas enzyme-linked immunosorbent assay is one of the minor criteria and is recommended when absolute criteria are not being fulfilled.
Thalamic gliomas can present with motor weakness or with features of severe intracranial hypertension. On neuroimaging, the histological subtypes have characteristic appearances; pilocytic astrocytomas appear as solid, cystic, or mixed, well-defined masses with strong contrast enhancement of the solid portion and no edema. In contrast, oligodendrogliomas present as diffuse swelling of the entire thalamus generally without contrast enhancement, with or without edema. 17 This picture is incompatible with the present case.
A hydatid cyst was also ruled out because it is more spherical and does not show either a scolex or spontaneous resolution.
This report highlights how a giant neurocysticercosis was mistaken for a thalamic glioma, which has different treatment and prognostic implications. Undue importance should not be accorded to magnetic resonance spectroscopy findings, and one should have a high index of suspicion for cerebral cysticercosis in a thalamic cystic lesion in an endemic country.
Footnotes
Acknowledgments
The authors are grateful to parents of the child who agreed to share his medical information.
Author Contributions
AM provided clinical care to the patient under the supervision of RS and KCA. BS and AK provided radiological input. AM prepared the first draft of the manuscript, which was edited and approved by all the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Written informed consent was taken from the parents of the child.