
Abstract
This study examined reliability and validity of the Zuk Assessment for diagnosis of motor problems and determined standardized scores in an Israeli population aged 5 to 6 years. For standardization, 156 children recruited from 13 Kindergartens of typically developing children were evaluated with the Zuk Assessment. Intrarater and interrater reliability were examined on 2 samples of 15 and 13 children, respectively. A total of 151 children referred for motor problems were examined with the Zuk and Movement Assessment Battery for Children assessment tools for validation of the Zuk Assessment. Findings showed that the Zuk total score had a normal distribution similar to that found in the literature identifying 5.1% (–2 standard deviations) and 12% (between –1 and –2 standard deviations) of children with motor-related problems. Reliability was indicated by high intraclass correlation scores both in intrarater (intraclass correlation = .89) and interrater (intraclass correlation = .95) paradigms. The Zuk assessment identified differences in subgroups, namely, typical, suspicious, and impaired, as found in the Movement Assessment Battery for Children, confirming the Zuk validity.
Motor problems are often described as performance with poor motor coordination that influences the everyday practical tasks that the child has to perform, and this, in spite of the fact that the measure of intelligence is normal and age-equivalent (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition). 1 In his work on disorders of motor development, Sigmundsson 2 stated that motor competence not only allows children to carry out tasks such as dressing, feeding, and bathing (activities of daily living) but it also affects their self-esteem and how they are viewed in the presence of their peer group. His research has shown that 6% to 10% of children will have problems with motor competence and will fall into a range below the norm.
If motor problems and clumsiness are identified in preschool children and they do not result from major motor problems such as cerebral palsy or mental retardation, this could be a sign of a risk factor for academic performance in school. Therefore, it is important to identify and assess these motor problems early, even before these children enter into the first grade, in order to intervene effectively with the motor aspect of development and its impact on function. 3
The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, defined Developmental Coordination Disorder 1 as difficulty in performing movement skills for daily activities where motor coordination in the natural environment is required. 4 Participation in typical childhood activities is part of normal, healthy living. Consequently, Developmental Coordination Disorder restricts participation in the peer group potentially rendering the child a social outcast. 5 Longitudinal studies show that the chronic aspect of this disorder has far-reaching effects on academic, social, emotional, and behavioral function. 6
The assessment tools most commonly used for identifying children with Developmental Coordination Disorder are the Assessment Battery for Children 7 and the Bruininks-Oseretsky test of motor proficiency. 8,9
As noted before that cultural differences have an effect on motor development, 10 the diverse population in Israel with its many cultural differences might not always be compatible with these tools. Children from a specific culture might be exposed to activities differently, for example, ball games, which are an integral part of the Movement Assessment Battery for Children test.
A tool for identification of the performance quality of motor problems in the preschool and first grades at school, suitable for the needs of an Israeli population would be beneficial for screening and assessing motor competence and function.
As a result, timely intervention for existing motor problems could help reduce some of the future secondary problems that might arise. The Zuk Assessment (Zuk), which examines underlying components of motor function necessary for skills used in daily activities, evolved for this population. The Zuk has been used by therapists in Israel for more than 5 years. 11,12 Before being widely used in Israel, it underwent examination of its reliability 13 and subsequently the validity was tested. 14,15
The purpose of this study is to examine reliability and validity of the Zuk Assessment for identification and diagnosis of motor problems and determine its standardized scores in an Israeli population aged 5 to 6 years.
Methods
Participants
The first step of the study was carried out in order to statistically represent the typically developing population of children in Israel. We used the approach of a hierarchical sample with reference to the following variables: urban/nonurban (rural) and secular/religious, and in this framework the representation of the socioeconomic mix of the general population was achieved. In accordance with this, 156 children aged 5 to 6 years were recruited from the normal school system. Thirteen Kindergartens were chosen to represent different social backgrounds. Ten Kindergartens, 3 of which were located in urban centers (n = 68) and 7 in rural communities (n = 58), were of a secular background. Three of the remaining 13 Kindergartens were of religious educational background (n = 30). In each of the 13 Kindergartens, all the children recruited were examined with the Zuk assessment in accordance with the directions specified in the manual. In total, 156 children aged 5 to 6 years were included in the study. In our study, the participant sample distribution of gender, domicile, and position in family, gestation, birth process, and walking age was similar to the Israeli general population. 16
One hundred fifty-one children were included in the second step of the study. Inclusion criteria were children 5 to 6 years of age referred due to gross and/or fine motor problems and grapho-motor problems. Exclusion criteria included orthopedic problems, mental retardation, cerebral palsy, and congenital abnormalities. All children were referred to Child Development Centers and were examined with the Zuk and Movement Assessment Battery for Children assessment tools in order to validate the Zuk Assessment. In steps 1 and 2, the Tel Aviv University ethics committee, the Health Ministry, and the Ministry of Education in Israel approved the research project. Written informed consent was obtained from all parents.
Instrument
The Zuk assessment tool is organized into 10 categories that include 38 subtest items (Table 1) and examines the underlying motor components in 3 areas of competence, gross motor, fine motor, and graphic motor function. The 10 categories were selected and developed for the assessment by a pediatric physical therapist who is a senior lecturer in pediatrics in the medical faculty at the Tel Aviv University (LZ). Content validity of the Zuk Assessment tool was examined by 3 expert pediatric physical therapists, all of whom had 15 to 20 years of experience in the field of assessment and treatment of children with motor problems. They validated the inclusion of all the subtest items. Table 1 shows the 10 categories and the subtest items of the Zuk. It includes standing and walking (6 items); static balance (2 items) and dynamic balance (3 items); changing posture (4 items); head and shoulder control and strength (2 items); sitting (8 items); graphic motor development (4 items); fine motor development (5 items); ability of the eyes to focus and follow (1 item); preferred eye and hand development (2 items), and finally joint hyperlaxity (1 item). The scoring method is simple and easy to use. Scores are calculated according to the successful achievement of the subtest item being examined. The total score is the sum of the scores of the subtest items examined in the 10 categories. Table 1 presents the score of each subtest item in each category. According to the items examined, children can score between 0 and 1, 0 and 2, 0 and 4, and 0 and 8. Each category has a different total maximal score that varies between 1 and 20.
Categories and Subcategories of Scored Subtest Items.
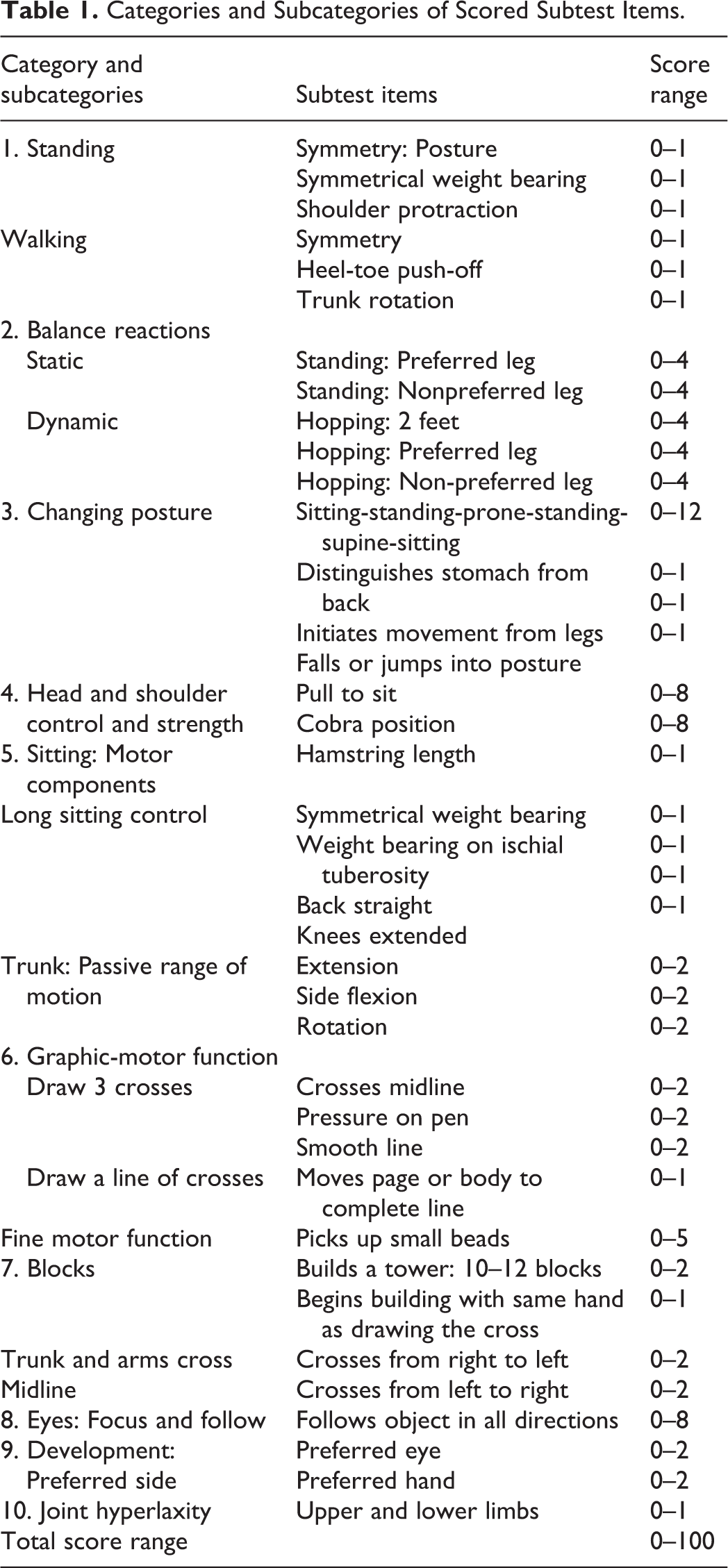
Finally the total score shows the level of function and motor performance of the child being examined. The higher score represents better performance. In 8 of the 10 categories examined, subtest items have identical evaluation scores for performance for ages 4 to 8 years inclusive. However, in the category of static and dynamic balance and tower building, the scores are age related and noted accordingly. Therefore, all age groups examined reflect the scores of the assessment tool.
The manual of the test gives precise instructions on how to present, execute, and score each of the subtest items. The length of time taken to score the subtest item is not taken into consideration. Three trials are given for execution of each subtest item and the 2 most similar (best or worst) results record the score. Subtest items are presented verbally with the understanding, on the part of the examiner, that the child grasps the meaning of the instructions; if this is not so, then an interpreter needs to be present (this with regard to the diverse population in Israel). No practice runs of the subtests are given. Scoring of the results reflects the automatic level of motor function of the child being examined. Administration of the test is user-friendly, takes 35 to 45 minutes to execute, and requires a minimum of equipment.
Procedure
In both the first and second steps of the study, each child was examined individually in a quiet, private room that was similarly set up for the assessment. Each room contained a free walking space of at least 5 to 6 m for testing the walking and balance subtest items, and a small table and chair for fine and grapho-motor examination. All equipment used for both the Movement Assessment Battery for Children and the Zuk Assessment was easily accessible to the examiner.
Reliability
Step 1 of the study: In the population sample of 156 typically developing children, 28 (∼20%) were randomly selected from the sample in order to undergo repeated measures.
Intrarater reliability: From this group of 28 children, 15 children were randomly selected and examined and assessed at 2 different points in time (10-14 days’ interval) by 1 of the authors to record the intrarater reliability. 13
Interrater reliability agreement was examined between one of the authors 13 and a second physical therapist who was experienced in the use of the Zuk Assessment, on the remaining 13 of the 28 randomly chosen children simultaneously observing and noting their findings.
Validity
To ensure that the subtest items represented all aspects of motor function included in the tool, the face and content validity were examined by 3 pediatric physical therapists with 15 to 20 years of experience and who were skilled in the use of motor assessments. Construct validity was assessed by examining the distribution of the scores in the total sample with the assumption that 5% to 10% would be identified with motor problems, and that a larger number of males would be identified.
In the second step of the study, 151 children with suspected gross and/or fine motor problems who had been referred to child development centers, were examined with the Zuk and Movement Assessment Battery for Children assessment tools for validation of the Zuk Assessment. Each child was assessed with both the tools, 1 week apart in time and with a random choice of initial assessment (Movement Assessment Battery for Children or Zuk).
Statistical Analysis
Normal distribution of the scores in the categories and the total score were evaluated with the Kolmogorov-Smirnov test (step 1). The t test was applied to compare scores between the subgroup of 13 and 15 participants that were chosen for intrarater and interrater reliability and the remaining group. Reliability for continuous scores was evaluated with intraclass correlation. For categorical variables, the Kappa and percentage agreement were used.
Validation of the Zuk with the Movement Assessment Battery for Children: According to the cut-off of the Zuk Assessment, a 1-way analysis of variance model was applied to assess the differences in the Movement Assessment Battery for Children Assessment score; P ≤ .05 was considered statistically significant. All statistical analyses were performed using SPSS v. 17 software packages.
Results
Step 1
Birth order was diverse in the sample, 145 children were born after a normal pregnancy and 11 after bed rest (mean gestational age [weeks] = 39.63 ± 2.00); 129 were born without any complications, 22 with caesarean intervention, 4 with vacuum birth, and 1 with forceps. Sixty-four children walked before 1 year of age. Mean age at entry into the study was 5.47 ± .37 years. Gender was found to be split 78 boys and 78 girls. The ratio of boys to girls with motor problems was found to be 3:2. Joint hyperlaxity was present in 31 children.
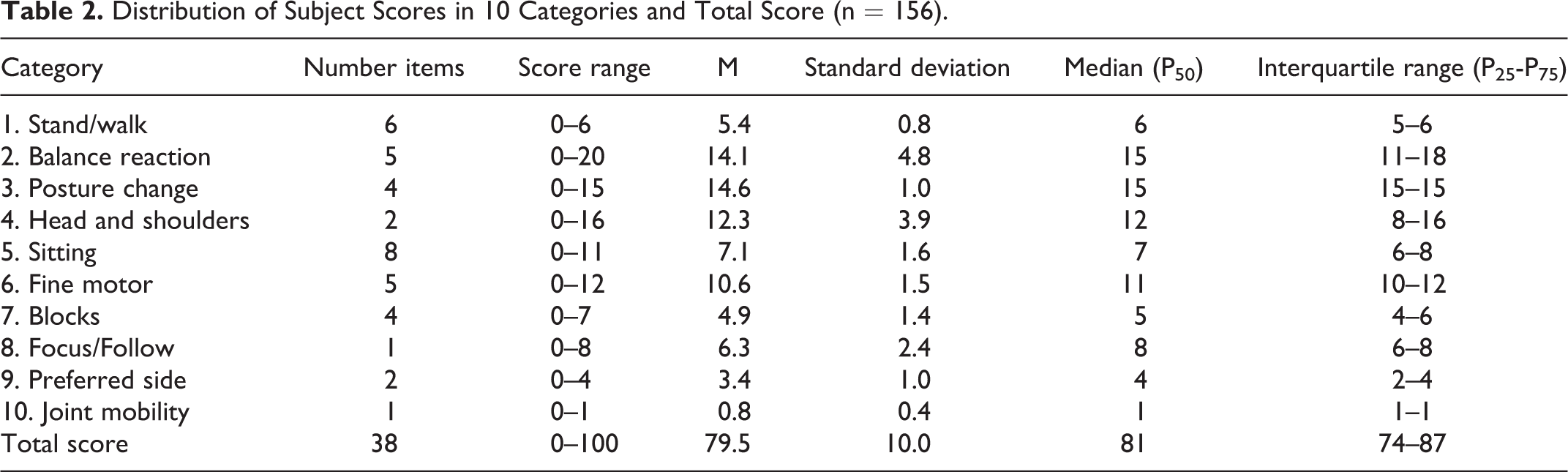
Subject score distribution in 10 categories and total score are presented in Table 2. Total score and category scores: The total average score was 79.5 (standard deviation = 10) close to the median of 81 (Q1-Q3 = 74-87). In the categories of standing/walking, changing posture, fine motor function, and preferred side, a ceiling effect could be seen as expected in a typically developing population.
Distribution of Subject Scores in 10 Categories and Total Score (n = 156).
Intrarater Reliability
No difference in the total score was found between this group (n = 15) and the remaining subjects (n = 141; t test, P = .2243). Results of the intrarater reliability included intraclass correlation values for each category and final score (Table 3). A high reliability score was found for the final score (intraclass correlation = .89, P < .001). Out of 10 category items, only 5 items appeared to be less reliable (P > .05). The intraclass correlation for the specific categories ranged from .20 to .89 as follows: high values (intraclass correlation >.70) for balance reactions, head control, shoulder muscle strength, focus and follow with eyes. Low values (intraclass correlation <. 40) were found for changing posture, sitting motor components, and tower building.
Reliability of Zuk Assessment by Intraclass Correlation Coefficients and Confidence Intervals.
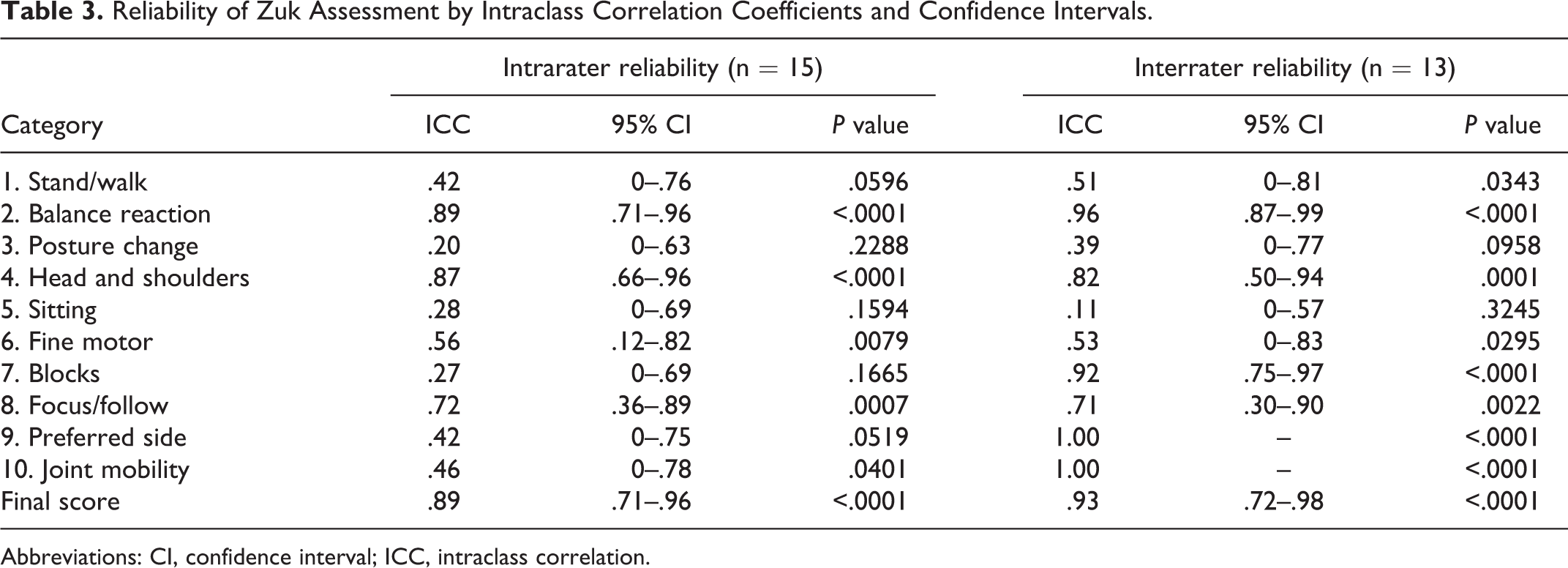
Abbreviations: CI, confidence interval; ICC, intraclass correlation.
Interrater Reliability
There was no difference in the total score between this group (n = 13) and the remaining group (n = 143; t test, P = .8909). Results of the interrater reliability are shown in Table 3. A high reliability score was found for the final score (intraclass correlation = .93, P < .001). The intraclass correlation for the specific categories ranged from .11 to 1. High values (intraclass correlation > .70) were calculated for balance reactions, head control, shoulder muscle strength, focus and follow, tower building, preferred side and joint hyperlaxity, whereas low values (intraclass correlation < .40) were found for changing posture and sitting motor components. Disagreement between the raters' results was indicated by a intraclass correlation of <.40). Percentage of agreement was as follows: changing posture (77%), preferred side (100%), and hyperlaxity (100%).
Normal and Abnormal Groups
The distribution of the total Zuk assessment score is presented in Table 2. The distribution can assumed to be normal with a mean of 79.5 (standard deviation = 1.0) (Kolmgorov-Smirnov P = .22). The total score was categorized to 3 levels, normal (score > 70), suspected (score 70-61), and abnormal (score ≤ 60). The cutoff point of 70 was chosen based on the mean –1 standard deviation, and 60 based on the mean –2 standard deviation, indicating the distribution of the typically developed children from the first step of the study sample: (1) normal motor performance: a score of 71 or more (129/156 = 82.7%); (2) suspected motor problems: a score of 61 to 70 (19/156 = 12.2%); (3) motor problems: a score of 60 or less (8/156 = 5.1%).
Reliability in Normal and Abnormal Groups
Agreement between the results of this dichotomous categorization scores was evaluated on subjects who underwent intrarater evaluation (n = 15) with findings of Kappa = .70 (P = .0067) and for those subjects (n = 13) who were observed by 2 experts (interrater) with findings of Kappa = .58 (P = .0211).
Step 2
Validity between Zuk Assessment and Movement Assessment Battery for Children assessment
According to the cutoff of the Zuk Assessment, significant differences were noted in Movement Assessment Battery for Children scores (F 2, 148 = 23.6, P < .001). The mean Movement Assessment Battery for Children scores in the motor problem subgroup in the Zuk were 5.93. Figure 1 shows mean and 95% confidence interval of Movement Assessment Battery for Children scores in Zuk subgroups.
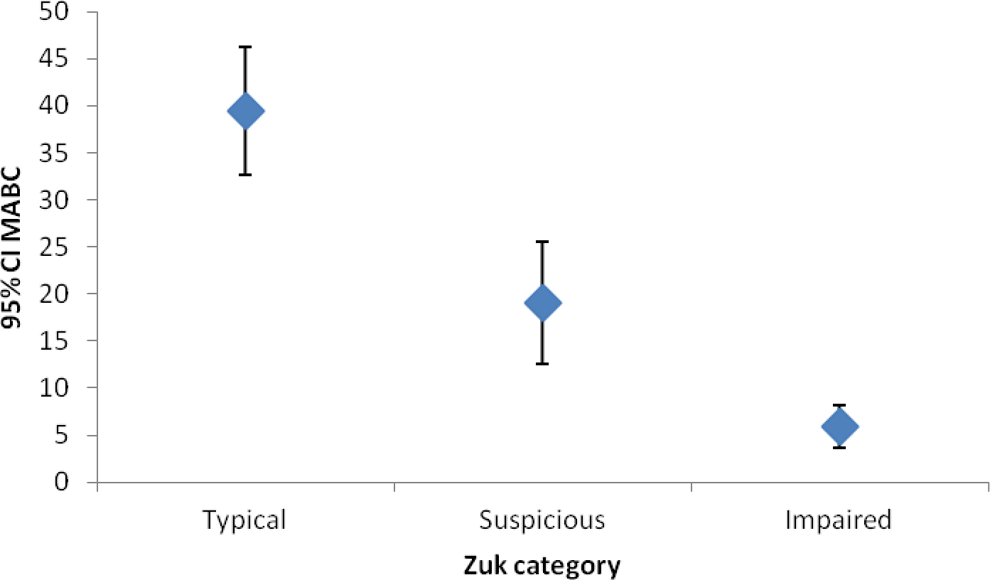
Mean and 95% confidence interval of Movement Assessment Battery for Children score by Zuk subscores.
Discussion
This study examined reliability and validity of the Zuk assessment for typically developing children with a birth history similar to that of the general Israeli population. 17 The tool was developed for identification of children with motor problems in preschool and first and second grades. Although Kindergarten is not a part of the school system in Israel, all children aged 5 to 6 years are compelled to attend Kindergarten, early identification of motor problems (5-6 years) would enable intervention before entering into the first grade.
The International Classification of Functioning, Disability and Health (ICF) model 18 characterizes differences at the levels of body structure, whole body movements or activities, and participation in life situations. Applying this model, the Developmental Coordination Disorder child will have problems of body structure presenting among others as poor coordination, 3 poor balance reactions, 19 and poor postural control. 20 These activity limitations interfere with participation and a child’s acceptance with his or her peer group, and manifest as difficulties in most physical activities and both organized and free play. 21 Therefore, the earlier the identification and therapeutic intervention of Developmental Coordination Disorder, the greater the possibility of reducing these problems of generalized poor self-efficacy toward physical activity 21 and overall participation in the home, community, and school. 22
Research has shown that early identification of the motor problem and timely treatment would be helpful in preventing the development of the secondary problems of Developmental Coordination Disorder, for example, academic, emotional and social problems. 22,23 Skinner and Piek showed how crucial motor coordination is in psychosocial development, and support early intervention for those children with motor problems and Developmental Coordination Disorder in order to assist them in improving their self-image and self-worth. 24
The choice of 4 years as the lower age limit of the Zuk was based on developmental considerations. Ruff and colleagues found that indexes of attention increased from 30 to 54 months of age. 25 The typically developing child aged 4 years and more becomes more adept at responding to higher-level demands of function with sustained attention. 26 Except for balance reactions and tower building, all the included items have been achieved among typically developing children up to the age of 4 years. The validation was carried out on a sample of children aged 5 to 6 years.
A high and significant correlation was found for the total score in the intrarater reliability (intraclass correlation = .89) and even higher in the interrater reliability (intraclass correlation = .93). These results indicate that the Zuk assessment is stable and consistent between professional examiners. The intrarater reliability of the Zuk is also maintained when the categorization of normal and abnormal is applied. Some items in the intrarater assessment had a lower reliability for the group of children identified with motor problems (abnormal group) when compared to the group of children with normal motor function. The literature supports this finding and emphasizes that Developmental Coordination Disorder children show large variability of performance when faced with motor tasks and function in test situations. 27 Difficulties in motor learning 28 weak musculature and poor coordination between body parts 29 contribute to their problems.
In the present study, a larger number of males compared to females were identified with motor problems (3:1). This finding is well supported by the literature. Crawford and colleagues 30 found in their study that the ratio of males to females was 1.5:1. A study assessing the movement skill problems of 7- and 9-year-old children who used a motor competence checklist found the ratio to be 2 and 3:1. 31 In a clinic-referred group of Developmental Coordination Disorder children with motor problems, the male-female ratio was 7:1. 32
The cutoff score of 70 or lower identified the motor problems (possible Developmental Coordination Disorder) and indicated the need for intervention. Two abnormal groups were identified: scores from 70 to 61 showed a moderate degree of motor problems, whereas scores below 61 were indicative of severe motor problems. This division into 2 subgroups could play an important role in the treatment approach, namely, group treatment versus individual treatment. 33 Our cut-off point of 71 identified 33% of the distribution (in a normal distribution) and relates to a large group of possible motor problems.
The Zuk Assessment scores were found to be significantly valid when compared to the Movement Assessment Battery for Children scores. The literature reports that cultural differences affect motor development; therefore, the assessment tool should meet with the demands of the population being examined, as found with respect to the Zuk. 10 Children in religious Kindergartens in Israel are an integral part of a cross section of the population. However, their cultural and physical environment differs from the general population and adhere to a much stricter code of behavior.
The Zuk differentiates between gross motor, fine motor, and graphic motor domains of development, allowing the examiner to relate to and address not only the total score of the assessment but in addition to the score of the subdomains as the interrater reliability of the subdomains was found to be significant. The results of these scores are important and help guide the examiner toward the type of intervention program that should be applied.
Conclusion
The goals of the Zuk Assessment were to identify children with motor problems from within a typically developing population. It was found that the Zuk Assessment tool was reliable and valid in terms of its total score and the diagnosis obtained. The tool, therefore, could be applied to the general Israeli population with its diverse cultural backgrounds. This assessment tool proved to be valid. Subtest items in the tool reflected the tested subject matter found in the professional literature. The tool is user friendly and easy to administer and requires little equipment.
Footnotes
Author Contributions
All authors of this article have directly participated in the research design, acquisition, analysis, and/or interpretation of the data. LZ contributed to the research design, interpretation, and writing of the first draft and the final draft of the manuscript. HT contributed to the acquisition of the data, had complete access to the study data, and contributed to the analysis of the data. MK-L analyzed and interpreted the data and assisted in the writing of the final draft of the manuscript. CP analyzed and interpreted the data. EC assisted in the study design and had complete access to the study data that support this publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Step 1 and step 2 of this study was approved by the ethical committee of the University of Tel Aviv, and by the Health Ministry and the Ministry of Education in Israel (2007015; 2007017; 2008012).