
Abstract
Accurate and well-targeted measurement of a child’s abilities and participation in daily activities pre- and post-intervention is essential to understanding the effects of therapies provided by pediatric practitioners. There is growing interest in identification of outcome core sets for specified client groups. This article elaborates on the concepts to consider when selecting and interpreting measures from an outcomes toolbox for children with cerebral palsy. Principles discussed include use of self-report measures to open a dialogue with the child/parent; a holistic assessment approach to identify a child’s challenges, strengths, and contextual factors that can influence functioning; links between measurement and heightened engagement of the child/family in the rehabilitation process and goals; and the need to plan the evaluation and dialogue aspects of the assessment process. If clinicians across the international rehabilitation community draw from the same toolbox, the end result could be a cohesive approach and common language to outcome measurement.
Importance of Outcome Measurement - The Concept of Core Sets and the Outcomes Toolbox
Accurate and suitably targeted quantitative measurement of a child’s abilities and health status before and after an intervention is essential to the understanding of the effects of rehabilitation, and associated surgical and medical therapies provided by pediatric practitioners. Use of a carefully planned and executed process of outcome measurement not only informs the clinician and family about the changes experienced by the child in association with an intervention, but is also critical to guide intervention planning and goal setting throughout the rehabilitation journey. 1 It is also important to carry forward the results of measures taken at the level of the individual child and family into an across-child and program-based context. This synthesis of information, in tandem with published research evidence, can influence the care system and how things are done (ie, a best practice approach to care). From an efficiency and client sensitivity standpoint, the individual child and systems measures should be well integrated, with the systems measure(s) being a subcomponent of the larger core set of measures used with the child and family. Determination of which measure(s) is selected for use across systems should be done by the clinical management team that oversees the program area in which the child’s care is based. The choice should align with the evaluation needs of the program and ideally also with a key indicator area identified by the facility.
The selection of an optimal set of outcome measures to fulfill this evaluation imperative can be a daunting task for a health practitioner given the ever-increasing number of observational and child- and parent-report measures that are available and the breadth of outcome areas that can be considered. 2 To this end, there has been growing interest in the rehabilitation world on identification of outcome measure core sets for specified adult and pediatric client groups. This core set work was done first within the context of clinical trials 3,4 but latterly has expanded to include a clinical practice perspective, 5 –7 suggesting the increasing recognition of the need for standardization in frontline care as well. These core sets typically consist of the most relevant categories (eg, sensation of pain, communicating, sleep, walking and moving, general physical endurance, fine hand use) from the International Classification of Functioning, Disability and Health 8 that should be considered when selecting outcome measures for a client group or intervention of interest. The approach taken to the derivation of the items for these core sets can range from a team-based process of determination by clinicians and researchers who work together within a local program or treatment network 9 to formal development by means of a systematic review (eg, Schiariti et al 6 ) and international clinical/research expert consensus exercise (eg, Verschuren et al, 5 Schiariti et al 10 ).
When applied to clinical practice, an outcome core set can be thought of as a toolbox 11 that contains the tools (the measures that reflect the core set items, such as those referred to in the preceding paragraph) that the clinician can choose as appropriate for the evaluation task that is at hand. When selecting the most suitable tools from this toolbox, the clinician needs to think about the purpose of their use (as described later) as well as the International Classification of Functioning, Disability and Health areas that are relevant to the intervention, to the child’s and the parents’ goals, and to the assessment circumstances. These considerations allow a clinically supported narrowing of the entire group of measures within the toolbox to the ones that meet the particular needs of that child or intervention or service. This decision process supports the integrity of the outcomes core set concept and standardized measurement while also streamlining the approach for the individual client/intervention/service. If clinicians from across the international rehabilitation community (from acute care to rehabilitation to community settings) draw from the same toolbox, the end result is expected to be a cohesive approach and common language to outcome measurement.
The Purpose of This Paper
This paper elaborates on the concepts that should be considered in selecting and interpreting outcome measures with respect to use with children with cerebral palsy. The intent is to provide readers with suggestions of the compartments that might be considered for the toolbox, and of how the measures from these compartments could be prioritized and employed. Although examples are provided of candidate toolbox measures within key International Classification of Functioning, Disability and Health categories, our goal was not to identify the core sets or final group of measures that belong in the toolbox. This extensive International Classification of Functioning, Disability and Health–based core set development work for use with children with cerebral palsy is being done by others through use of formal international consensus methods, 10 and has been completed in the specific area of exercise tolerance measurement in children with cerebral palsy. 5 We propose however that the concepts and processes discussed below can be applied in the meantime by clinicians to sets of measures that they are familiar with using now, or to published core sets such as the one by Verschuren et al. 5
The Scope of Outcome Measurement
The consensus definition of cerebral palsy elucidates that this is not only a disorder of movement and posture but is also associated with activity limitations across domains such as daily living skills, communication, socialization, and mobility and is often associated with impaired sensation, perception, cognition, language, and behavior. 12 As such, outcome measurement for children with cerebral palsy should consider all aspects of functioning and health to include impairments, activity limitations, and participation restrictions. These components of functioning align with the World Health Organization’s International Classification of Functioning, Disability and Health–Child and Youth version (ICF-CY; http://apps.who.int/classifications/icfbrowser/Default.aspx, accessed December 3, 2013) and are comprehensively described in another manuscript in this issue by Vargus-Adams and Majnemer. As part of this international classification scheme, contextual factors are also considered, as these personal (eg, sociodemographic factors, lifestyle preferences, personality traits) and environmental (eg, family functioning, access to services, physical barriers) factors can either positively or negatively influence functioning. In addition, there is recent interest in characterizing the child’s perceived quality of life to better appreciate the extent to which the individual has adapted to their impairments and limitations and is able to participate in meaningful activities of their choosing that make them happy. 11,13 Therefore, outcome measurement for children with cerebral palsy should adopt a holistic view of the child in the context of their environment, so as to identify strengths as well as problems and challenges. A more comprehensive picture of the child enables the interdisciplinary team of rehabilitation specialists to minimize deficits, promote independence, and optimize participation in relevant and meaningful activities. 14
The actual selection of outcome measures from the toolbox by a health practitioner is largely dependent on the purpose of measurement. The clinician needs to reflect on why it might be important to measure a particular domain(s) of interest. Measurement of certain areas that are discipline-specific can inform the treatment plan and the areas in which to intervene. Indeed, outcome measurement should inform clinical decisions that help to define the goals of interventions; these goals should not be predetermined on the basis of the diagnosis of the child. Assessments can include patient-reported outcome measures and, as such, identifies the main priorities and needs of the child and family. Measurement processes may also need to be imposed, at least in part, by administrators or managers who require standardization of particular outcome measurement for quality assurance purposes and program evaluation.
The purpose of measurement is strongly influenced by the clinician’s role. For example, if the rehabilitation specialist works in an acute care hospital setting, their role is primarily diagnostic and the evaluation process is focused on describing the extent and nature of impairments and activity limitations. If assessment is being carried out as part of the provision of an intensive treatment intervention, that is, within a rehabilitation center, outpatient, school, or home setting, the measurement tools that are selected need to be sensitive to changes over time when used pre- and post-intervention as well as at any other progress evaluation time points. For rehabilitation specialists providing consultative services (typically within a community setting), the focus is more likely to be on adaptation and integration/inclusion, and therefore measures should capture whether or not the recommended adaptations or activities have made a difference in optimizing the child’s participation in life roles.
Family and Child Perspectives and the Fit of Outcome Measurement With Family-Centered Care
One of the driving forces behind decisions on what belongs in the outcomes toolbox needs to be family-centered care, a central tenet of pediatric rehabilitation. There are several ways in which the composition of the outcomes toolbox can support the emphasis on family-centered care. The first way is through the inclusion of self-report measures, that is, report by the child or by parent proxy for younger children or those who cannot self-report because of cognitive and language impairments about what actually happens in real life and how they feel about it. These child- and parent-report measures are reflective of “performance” in the context of real life. In other words, they take into account the influence of environmental and personal factors (parent and child) on what the child actually does and experiences. 15 –17 These questionnaires, also known as patient-reported outcomes, provide the clinician with the individual’s perspectives on symptoms, functional status, participation, health perception, quality of life, environmental factors, or satisfaction with services. 18 A user’s guide for implementing patient-reported outcome assessment in clinical practice 19 is available on the International Society for Quality of Life Research website (http://www.isoqol.org/UserFiles/file/UsersGuide11-11.pdf). There is strong evidence that a well-designed questionnaire-style measure, regardless of measurement domain, can be highly reliable, valid, and capable of detecting change in abilities (responsiveness). 20 –22 Examples of these recommended measures for the cerebral palsy outcomes toolbox are shown in Tables 1 to 5.
Examples of Mental Functions Measures That Could Be in the Toolbox for Children With Cerebral Palsy.
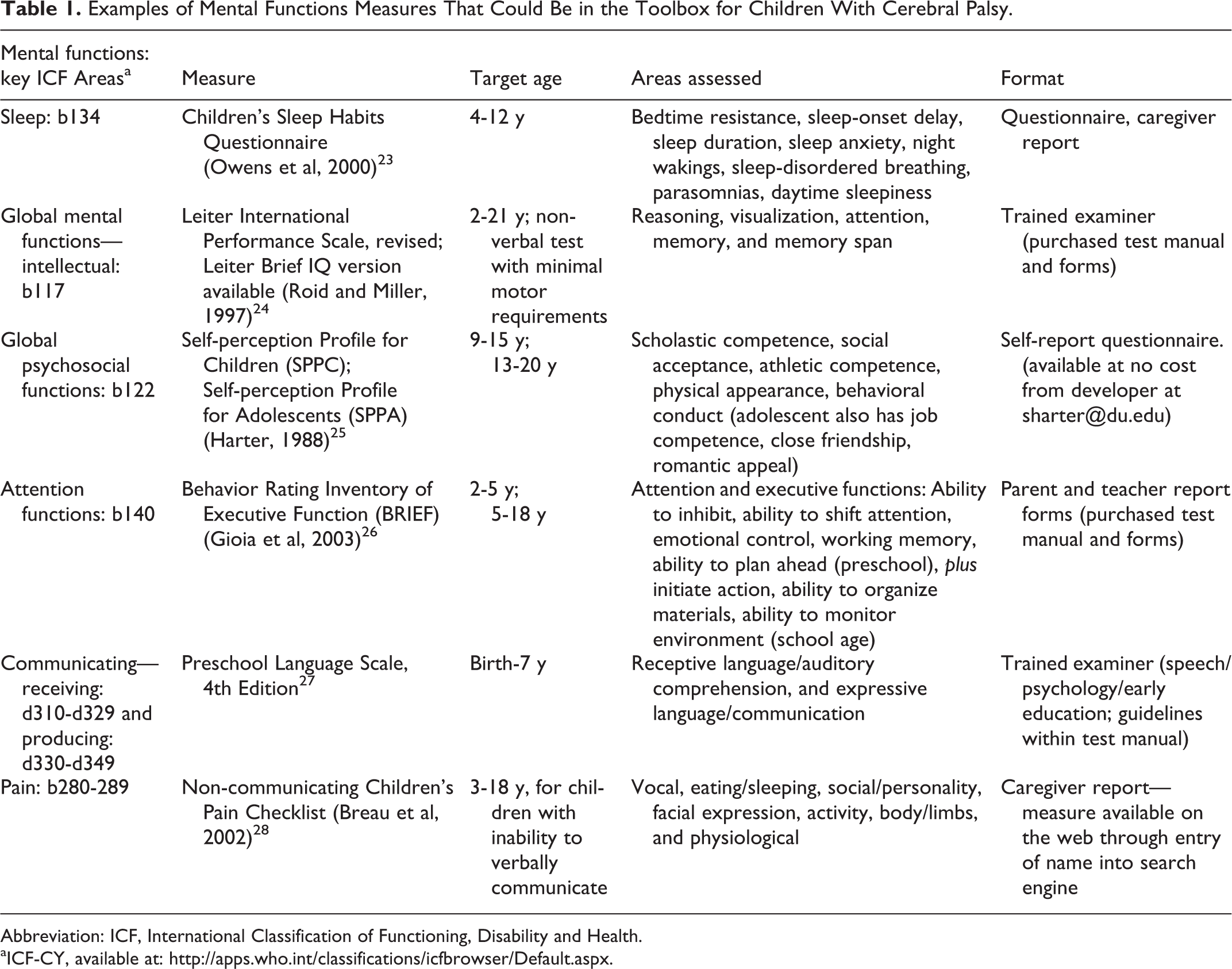
Abbreviation: ICF, International Classification of Functioning, Disability and Health.
aICF-CY, available at: http://apps.who.int/classifications/icfbrowser/Default.aspx.
Examples of Motor Functions Measures That Could Be in the Toolbox for Children With Cerebral Palsy.
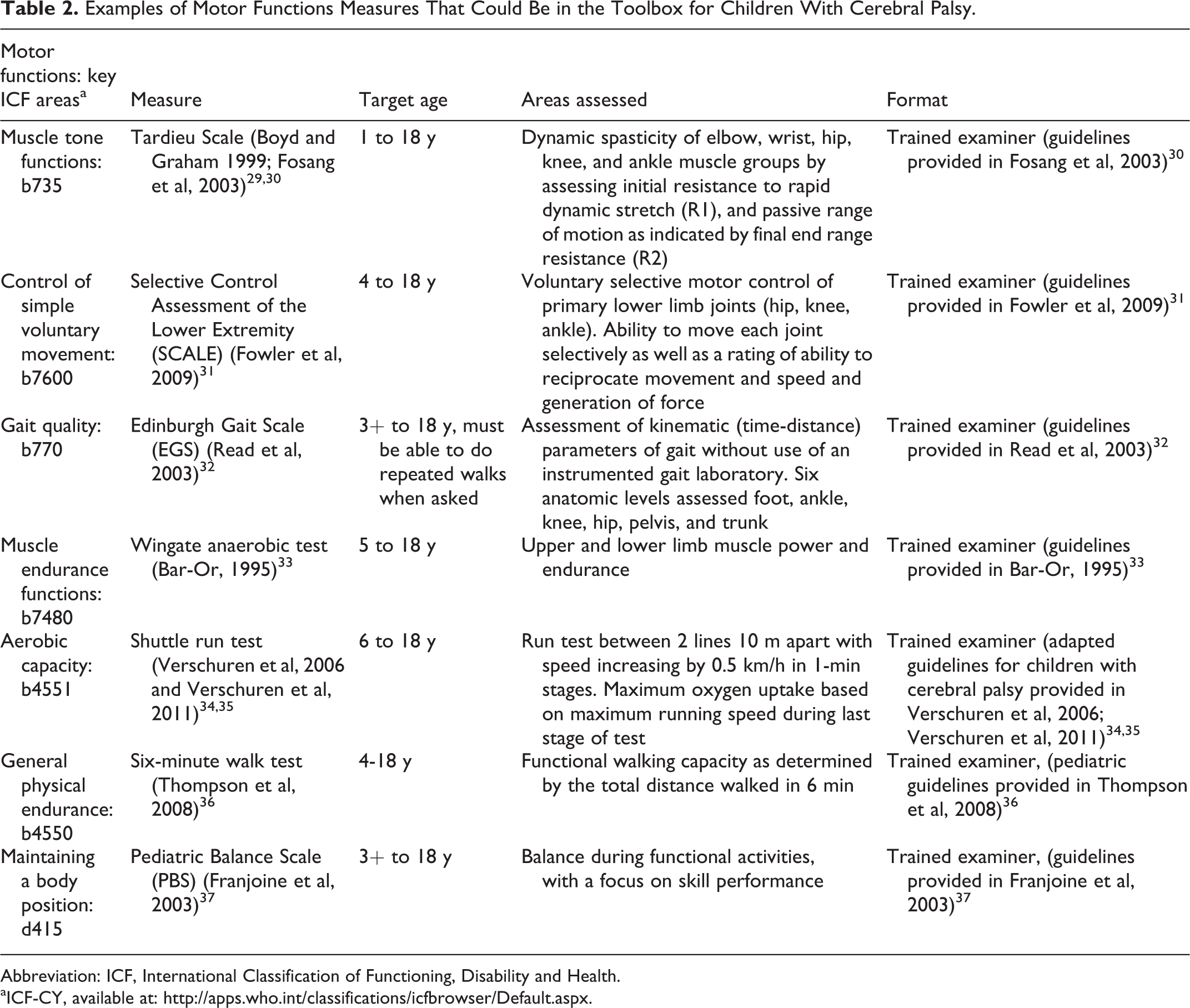
Abbreviation: ICF, International Classification of Functioning, Disability and Health.
aICF-CY, available at: http://apps.who.int/classifications/icfbrowser/Default.aspx.
Examples of Mobility Measures That Could Be in the Toolbox for Children With Cerebral Palsy.
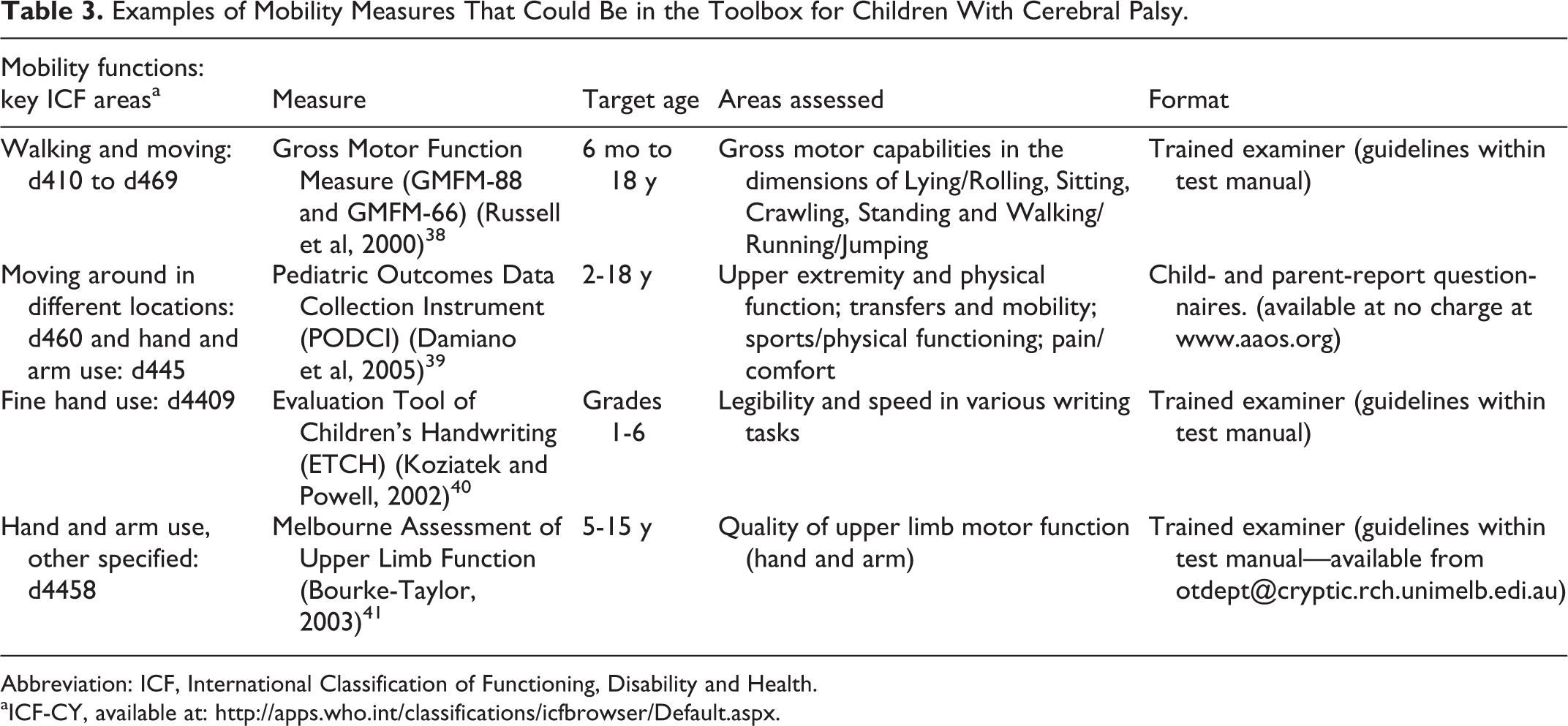
Abbreviation: ICF, International Classification of Functioning, Disability and Health.
aICF-CY, available at: http://apps.who.int/classifications/icfbrowser/Default.aspx.
Examples of Activities and Participation (General) Measures That Could Be in the Toolbox for Children With Cerebral Palsy.
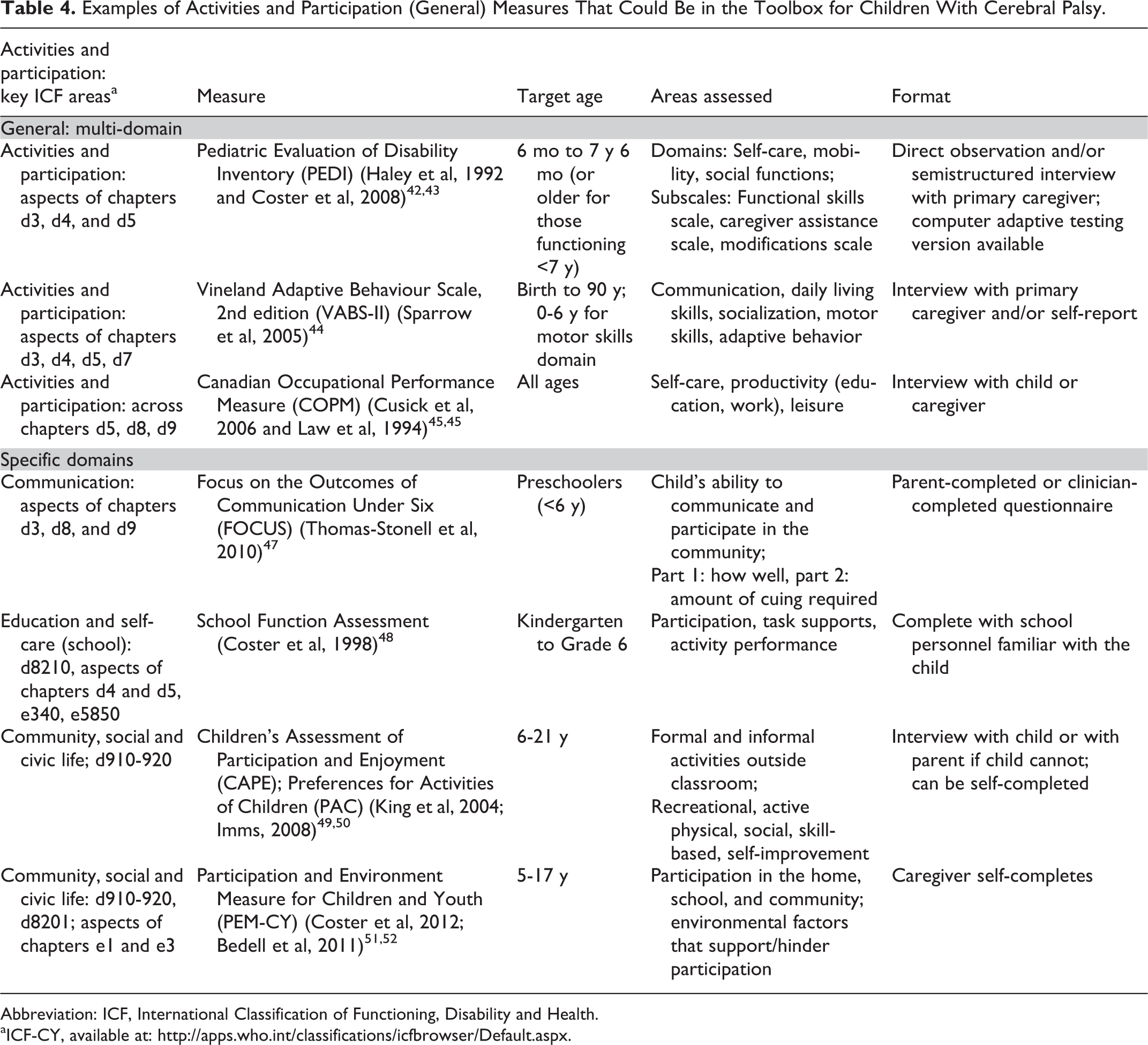
Abbreviation: ICF, International Classification of Functioning, Disability and Health.
aICF-CY, available at: http://apps.who.int/classifications/icfbrowser/Default.aspx.
Examples of Contextual Factors Measures That Could Be in the Toolbox for Children With Cerebral Palsy.
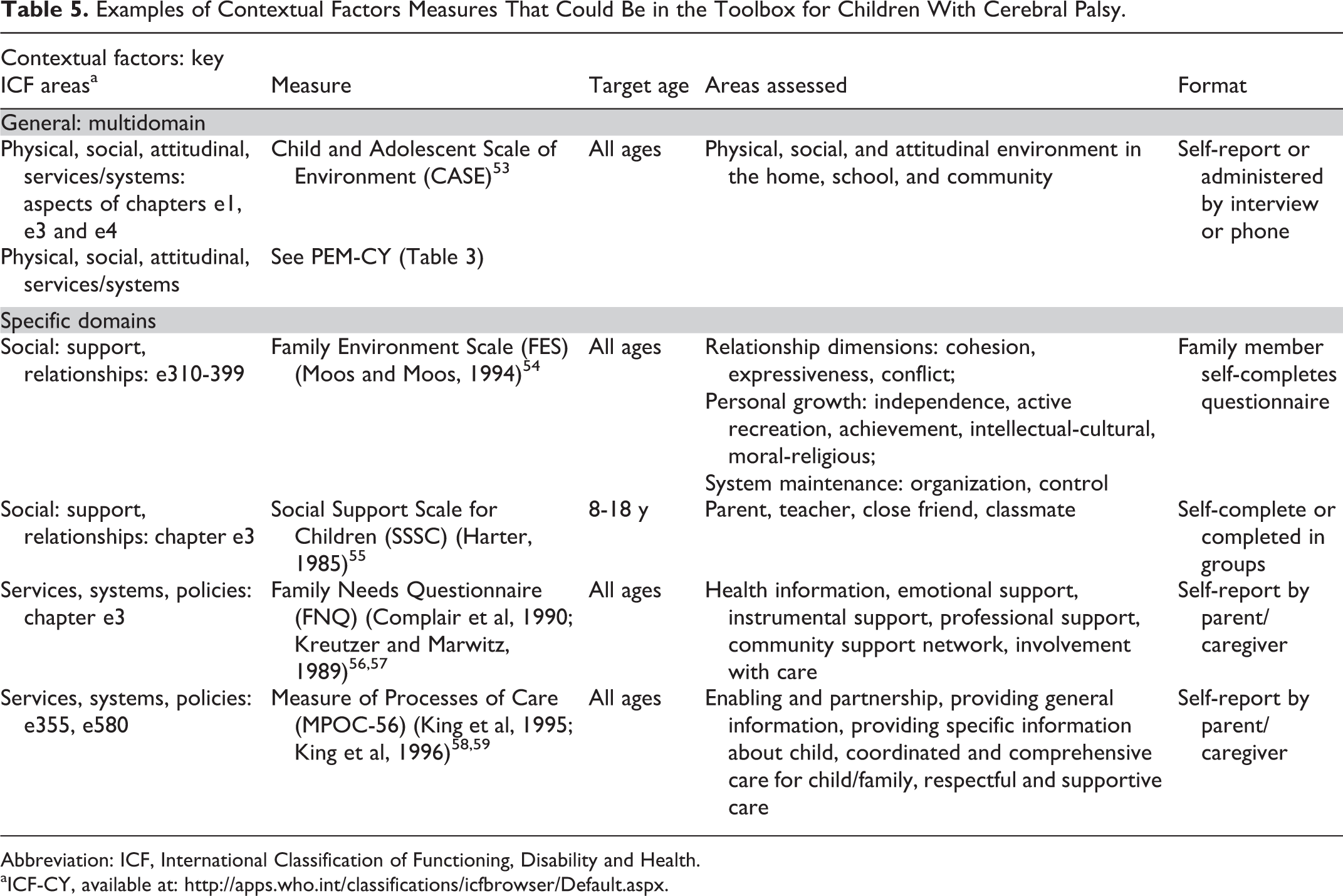
Abbreviation: ICF, International Classification of Functioning, Disability and Health.
aICF-CY, available at: http://apps.who.int/classifications/icfbrowser/Default.aspx.
Second, it is also important to consider “real life performance” jointly with a child’s capabilities (ie, what he/she is able to do in a clinical environment and test scenario). When the underlying composite skills are directly observable, it is recommended that performance-reflective (self-report) questionnaires be used in conjunction with objective observational measures from the toolbox that capture a child’s capability in a similar area(s). The clinician can then move from performance areas that are viewed as a priority to the child and/or parent to set goals that work to close the gap between capability (can do in the test environment) and performance (does do in real life). As noted earlier, this may involve interventions focused on “changing” the child or might instead also focus on changing the task or environment to support the child’s performance (participation). 60
Third, the addition of individualized outcome measures such as the Canadian Occupational Performance Measure and Goal Attainment Scaling to the outcomes toolbox has strong merit. These measures require the collaboration between the clinician and the child/parent and are based on identifying their priorities and setting goals and evaluating outcomes directly related to the priority goals. The Canadian Occupational Performance Measure and/or Goal Attainment Scaling can be applied regardless of goal area, intervention focus, age or diagnosis of the child. 61,62 Furthermore, they are highly responsive to change and therefore useful in the determination of the effectiveness of a particular intervention. This use of individualized goals is fully aligned with the model of family-centered care 1 as well as considerations of the developing autonomy of the child or youth. Although the goals are specific to the child and hence have strong meaning in their particular evaluation, both Goal Attainment Scaling and Canadian Occupational Performance Measure outcome scores can be rolled up across children to the program level to provide information both on the types of goals/International Classification of Functioning, Disability and Health areas worked on for a particular client group or intervention program 61 and also the extent of accomplishment (program effectiveness). 45,62
Fourth, the use of parent or child self-report measures can open a dialogue with families, and in a sense become an added part of the intervention. The reflective process that a child or parent needs to go through to complete a functional ability or participation questionnaire for example, may bring a new consciousness or awareness of not only the child’s strengths and challenges but also the circumstances in the surrounding environment (caregivers and other people, structures, systems) that may need to change to allow the child to move to the desired level of performance. 63 Although it may seem expedient and time-efficient to give a child or parent a questionnaire to complete on their own and then score at a later point in time for purposes of documentation and measurement of change, it is the follow-up session with the child/parent shortly after questionnaire completion that leads to the performance dialogue that supports both goal-setting and intervention planning.
Finally, when thinking about measurement in a family-centered care context, the importance (the “so what”) factor of measurement needs to be clear. What we as clinicians measure and then what we plan to do with the results need to be explicitly conveyed through the clinician’s/team’s discussions with the family at the outset of a care cycle. This will help to position measurement as an essential part of the care process and getting to know the child and family and their priorities rather than just something that is a system requirement. It takes time to measure attributes well and share the results, and the clinician needs to consciously plan when the evaluations will take place and when the dialogue will occur so that these aspects do not become an afterthought or add-on. Outcome measurement with family involvement deserves to be an integral part of the care process. However, it will only be experienced in this way if the health practitioner works from the start with a well-targeted selection of measures from the toolbox and encourages open dialogue through the measurement process, and if the child/parent and clinician are fully engaged with the prioritized goals throughout the intervention and are given meaningful feedback of the outcome results by the clinician in conjunction with discussion of next steps.
Developmental Considerations
When selecting outcome measures, whether in a clinical or research context, it is essential that the measure(s) is age appropriate and contextually relevant. 64,65 Child development is a dynamic, evolving background. Although cerebral palsy, and indeed most developmental disabilities, is a static nonprogressive condition, the child is constantly changing over time. They may be making gains in developmental milestone acquisition, but possibly regressing or worsening with respect to some symptoms, impairments, or activities (ie, cycle of deconditioning) as they transition through adolescence into adulthood. 66 The age and stage of the child’s development therefore guides the focus of evaluation in terms of emphasis on particular age-appropriate activities and life roles. Thus, assessment should focus not only on the preoccupation of the clinician on domains relevant to their discipline, but must also center on the activities most relevant to the child at that point in their development. There is a tendency to provide a comprehensive evaluation only in the early stages of development, soon after diagnosis; however, as the child transitions to different stages of development, the child is faced with new challenges and life roles. Therefore, comprehensive outcome measurement should occur periodically, to overlap with these important transition points so that new challenges can be addressed by intermittent, well-timed injections of rehabilitation service provision. 64
Rehabilitation interventions are gradually evolving beyond a “fix it” model to include strength-based, solutions-oriented therapy that may be context-focused. 60 The emphasis of these intervention approaches is on promoting meaningful participation in spite of disability and modifying the task and the environment instead of the child (http://www.acywr.org/wp-content/uploads/2011/09/SBA-Backgrounder.pdf, accessed December 5, 2013). These approaches rely on the ability to capitalize on particular strengths (eg, social skills, communication, mastery motivation, peer supports, physical accessibility, adapted technologies) that are age-specific and contextually relevant. Assessment at a particular stage of development provided a key opportunity to identify the child’s developmental assets or specific strengths or abilities, not only their challenges or difficulties. This process of discovery could include unique capabilities in particular domains or activities, but could also include environmental resources and supports to include the family.
Motivate to Change
A positive by-product of a well-targeted and finely tuned outcome measurement process can be the heightened engagement of the child and family in the intervention itself, and associated enhanced motivation to work toward the desired areas of change. 67 As noted above, use of a parent- or child-report questionnaire has the potential to spark this motivation to change when the content of the measure fits the child and the intervention possibilities, and is used in a facilitating manner by the health practitioner. For observational measures, it is important to elicit the child’s maximum ability in a way that their strengths can be fully recognized and then capitalized upon within the goal-setting process that follows the evaluation. The sense, during the assessment process, of being able to demonstrate skills accomplished may in itself set the tone for a client’s enhanced self-belief (self-efficacy) in their ability to succeed in the goals that are set for the intervention. It also suggests the need for clinicians to reframe their assessment approach with the child for the functional and participation-based measures to be one that is strengths-based and discovery focused (to aid goal-setting) rather than the more usual focus on deficits and remediation that can so easily invade a testing milieu. What this requires within the assessment process is selection of measures from the toolbox that fit the child’s abilities as closely as possible while still leaving some challenge (room) at the upper end of the measurement scale to allow for evaluation of change. 63,68
Outcome Versus Determinants
Children with cerebral palsy are highly heterogeneous in terms of comorbidities (sensory, cognitive/perceptual, speech and language, behavioral, and musculoskeletal impairments) that collectively can influence functional outcomes. Furthermore, contextual factors such as age, gender, socioeconomic status, mastery motivation, lifestyle preferences (ie, personal factors) and also family functioning, resources, social supports, societal attitudes, and physical barriers (ie, environmental factors) can greatly influence the outcomes of these children. 69 –72 Therefore, when selecting measures from the toolbox, it is important to also consider additional measures of factors or “determinants” that may influence the outcomes of interest. Determinants that enhance functioning (eg, family environment, peer support, motivation, and lifestyle preferences) should be facilitated and supported, whereas factors that hinder the outcomes of interest (eg, fear of failure, family stress, physical barriers, access to aids, and adaptations) need to be addressed so as to optimize the health and functioning of the child. The most relevant determinants for the child/family situation should be considered and measured in research studies and as part of clinical interventions, bearing in mind when selecting the tools they need to keep this additional measurement activity feasible as far as administration time and respondent burden. Most of these contextual (personal and environmental) measures are child or parent report and therefore do not necessarily require additional time for the clinician to administer. However, once completed, they need to be scored and interpreted, and the findings should inform goal-setting discussions and practice decisions. For example, the child or parent can complete the Dimensions of Mastery Questionnaire 73,74 to measure mastery motivation of the child with cerebral palsy. If results indicate that the child demonstrates a high persistence in social tasks but low persistence in motor activities, then this information should guide adjustments in therapeutic interventions. Specifically, social activities with peers might be used to increase motivation and adherence to treatment, whereas task avoidance and lack of confidence in performing motor activities might need to be tackled as an important focus of intervention.
Future Directions
The work by Schiariti et al, 10 now underway, will result in outcome core sets spanning the International Classification of Functioning, Disability and Health that are linked to the age and stage of development for children and youth with cerebral palsy. We likely can expect to see the publication of various versions of International Classification of Functioning, Disability and Health–based outcome core sets over the next decade as this concept takes hold. Some, like the work by Schiariti et al, 10 will encompass the breadth of the International Classification of Functioning, Disability and Health, whereas other core sets may focus on categories within the International Classification of Functioning, Disability and Health (such as exercise tolerance as Verschuren et al 5 have done). The set of toolbox measures that we have provided in the tables are examples of possible measures that may be considered within the selected International Classification of Functioning, Disability and Health components. One of the challenges will be to keep these toolboxes current with respect to newly validated measures coming onto the scene or in response to changes in the understanding of the strengths and merits of currently recommended tools. Further, in addition to the accepted tools within the main compartments of the toolbox, the clinician might want an extra compartment that contains emerging tools (ie, ones that are in early validation stages) that could be added by a clinician to their selection of main compartment tools to round out or fill a gap in the established measures for a particular client/client group. 9 Finally, as with all tools, outcome measures are very dependent on the skills of the user, both as far as selection of the right tool and ensuring its optimal application. Access to a more complete toolbox carries with it the inherent possibility of encountering measures that are unfamiliar to the clinician. Thus, the use of a toolbox needs to be accompanied by a caveat about the need to familiarize oneself with the requirements for using the measure before applying it within clinical practice.
Measures that are accepted into a toolbox are expected to have demonstrated strong reliability and validity when used with children with cerebral palsy. In addition, to fulfill the requirement of indicating change (outcome), these measures also should have established sensitivity to change or responsiveness. In reality, most measures used in practice and in research do not as yet have psychometric validation of their responsiveness to change. Responsiveness is often evaluated through statistical approaches such as standardized response means, and while valuable, these statistics are devoid of any link with clinical meaning of the change magnitudes. 75 Validation work with extensively used pediatric measures such as the Gross Motor Function Measure–66 76 have estimates of clinically important change from parent ratings of change that are considered in relation to minimum detectable change (as derived from test-retest reliability work). However, clinically important change is complex to establish from a methodologic standpoint as it is likely specific to the intervention in terms of factors such as intensity, cost, and risk and also to the child’s starting ability level and preintervention expectations. 77,78 Thus, the concept of a “one size fits all” clinically important change score magnitude for a particular measure is unlikely, and points to the need for extensive work in the future with different interventions and groups of children to establish a range of target change score magnitudes.
Over the past decade, a plethora of outcome measures have been developed across the spectrum of the International Classification of Functioning, Disability and Health framework that may be used for children with developmental disabilities. 14 These advances in measurement development have been prompted by the need to accurately document small but clinically important changes in functioning following rehabilitation interventions. It is likely that we will continue to see growth and development in the toolboxes themselves with respect to what we measure and how we go about it. Although it is expected that many of the measures that make the grade for current toolboxes will stand the test of time as permanent members of the toolbox, clinicians need to keep an eye on the changing landscape and watch for new measures that are created in response to identified measurement gaps as well as for validated next versions of existing toolbox measures. Better measures in specific areas of body function will likely continue to evolve to address content and psychometric shortcomings of current tools, and there is a need to expand the toolbox in some of the domains of activities and participation to enhance relevance across different age groups and severity of disability. Because there is increasing interest in modifying the task or environment to enhance autonomy, measures of aspects of the environment need further advancement as well. Participation measures and measures of the environment typically require cultural and linguistic validation, particularly in low- and middle-income countries, to ensure transferability and relevance.
Finally, creation of toolboxes that contain measures that are acceptable across cultures will support the vision of a cohesive International Classification of Functioning, Disability and Health–based outcome measurement approach that ultimately achieves international acceptance as the common language of outcome measurement for children with cerebral palsy. This would greatly enhance sharing of intervention-based outcomes knowledge across the pediatric rehabilitation community and assist in the creation of best-practice care standards to optimize the outcomes experienced by children with cerebral palsy and their parents.
Footnotes
Acknowledgments
FVW holds the Holland Bloorview Kids Rehabilitation Hospital Foundation Chair in Pediatric Rehabilitation. The Chair supported the assistance provided by Elizabeth Luff, RA, in formatting this paper.
Author Contributions
FVW and AM both participated fully in all aspects of the writing of this paper, from inception of the idea to completion of the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.