
Abstract
The aim of this study was to investigate the effects of valproate and carbamazepine, on renal glomerular and tubular functions. The patient group comprised 54 children with new-onset epilepsy treated with valproate (n = 30) and carbamazepine (n = 24). Twenty-six healthy children were in the control group. The serum creatinine and cystatin C levels and urinary excretion of N-acetyl-β-
Epilepsy is one the most prevalent chronic neurologic disorder, affecting 0.5% to 1.0% of children 1,2 ; it requires continued medication for at least 2 years or more and occasionally lifelong management. It is well known that administration of antiepileptic drugs may have unwanted effects on many organs such as hepatic and thyroid functions; however, limited data exist for their influence on renal functions in children.
Valproate and carbamazepine are effective and widely used antiepileptic drugs for the treatment of many types of epilepsy in children.
3
A few studies have demonstrated their nephrotoxicity, particularly on renal tubular functions.
4,5
Among many urinary enzymes studied in children either with epilepsy or other disorders, N-acetyl-β-
Glomerular filtration rate (GFR) measurement is a reliable marker of glomerular function in children. Estimations with 24-hour creatinine clearance and practical formulas based on the serum creatinine level are widely used to determine the glomerular filtration rate. However, serum creatinine levels are influenced by several factors, such as age, gender, and muscle mass of the patients. In recent years, plasma cystatin C has been proposed as a better marker to show the variations in glomerular filtration rate than serum creatinine. Thus, practical formulas based on cystatin C for glomerular filtration rate measurements have also been developed. 9 –11
In this study, we evaluated the effect of valproate and carbamazepine on renal glomerular and tubular functions of children with epilepsy.
Methods
A total of 54 idiopathic epileptic children between the ages of 4 to 16 years were enrolled in the study. Twenty-six healthy age- and sex-matched (mean age 8.7 ± 2.6 years) children without any history of neurologic, nephrologic, or other diseases such as diabetes mellitus that could affect renal functions were chosen as the control group.
Duration of antiepileptic drug treatment of the patients was between 3 and 24 months, 30 of 54 patients (55.6%) were receiving valproate, and 24 of 54 (44.4%) were receiving carbamazepine monotherapy. Of the 54 patients, 26 (48%) had generalized seizure and generalized epileptic activity on electroencephalography (EEG); 28 (52%) had partial, complex partial seizure and focal epileptic activity on EEG. All patients were seizure free. Mean age was 10.4 ± 3.5 years and 10.7 ± 3.7 years in valproate and carbamazepine groups, respectively. Patients who had used any other antiepileptic drug previously; received any drug within the past 3 months that could affect renal function, such as aminoglycosides and steroids; any nephrologic disease, including glomerulonephritis, nephritic syndrome, or recurrent urinary tract infections; any chronic disease such as cardiovascular thyroid disease or diabetes mellitus; and those with refractory seizures were excluded from the study. The number of patients in both drug groups decreased at 6 months of the study. The valproate and carbamazepine groups had 24 and 18 patients, respectively. The study was approved by the local ethics committee, and written informed consent was obtained from the parents.
Blood and urine samples from all patients were taken at the beginning of the study and after 6 months. They were taken for only once at the beginning of the study from the control group. Plasma concentrations of valproate and carbamazepine were measured in all patients taking these drugs. Blood levels of cystatin C and serum creatinine and urine creatinine (UCr) levels were measured on the same day with the nephelometric and Jaffe methods, respectively. Urine samples obtained for N-acetyl-β-
GFR Estimation Formulas.
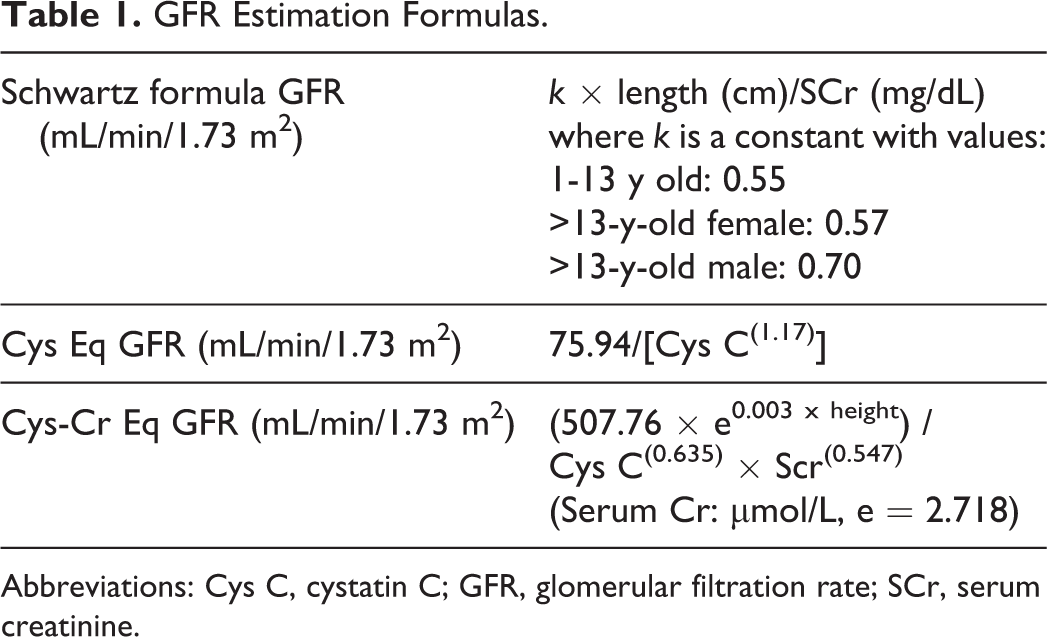
Abbreviations: Cys C, cystatin C; GFR, glomerular filtration rate; SCr, serum creatinine.
According to the Schwartz et al equations, 12 the glomerular filtration rate was calculated on the basis of serum creatinine levels. Glomerular filtration rate values were also calculated by 2 new Filler Formula that were introduced by Zapitelli et al. 13 One of them uses cystatin C level for glomerular filtration rate calculations, and the other uses both cystatin C and serum creatinine levels. Reference values for glomerular filtration rate were derived from inulin clearance investigations in healthy children older than 2 years of age. The normal level of inulin clearance in the literature is 127 mL/s/1.73 m2 (range: 89-165). 14,15
Our patients were divided into 2 different groups: patients having the drugs and the control groups. Data were also analyzed longitudinally between measurements at baseline and at month 6 in each drug group. The results of descriptive analyses were reported as a mean + standard error for the group. Conformity for normal distribution of quantitative data was performed with the Shapiro-Wilks test. For statistical analysis, nonparametric tests were applied. For evaluations of categorical data, independent groups, and dependent groups, χ2 test, Mann-Whitney U test, Kruskall-Wallis H test, and Wilcoxon test were used respectively. All tests were classified as significant if the P value was <.05. The Statistical Package for the Social Sciences (version 16.0, SPSS Inc, Chicago, Illinois) was used for all statistical analysis.
Results
The clinical characteristics of the patient and control groups were similar in regard to male-to-female ratio, mean age, body weight, height, and duration of treatment (Table 2). The concentrations of serum creatinine, serum cystatin C, and glomerular filtration rate values that were calculated by the 3 formulas at the beginning and at the sixth month of the study were denoted (Table 3). They were all normal according to the range of the laboratory. Mean serum creatinine and serum cystatin C concentrations were all similar in the patient and control group. Glomerular filtration rate cystatin C, glomerular filtration rate cystatin C–creatinine, Schwartz, and urine N-acetyl-β-
Baseline Characteristics of Study Groups.
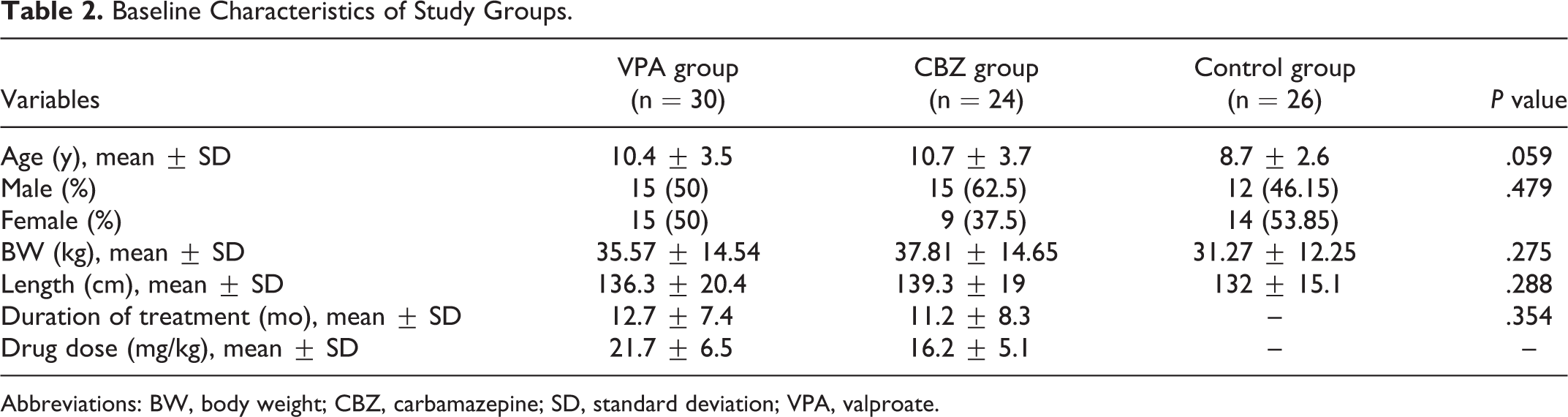
Abbreviations: BW, body weight; CBZ, carbamazepine; SD, standard deviation; VPA, valproate.
Baseline Serum Cr, Cys C, GFR, Drug, UNAG/Cr Levels in Patients and Controls.a
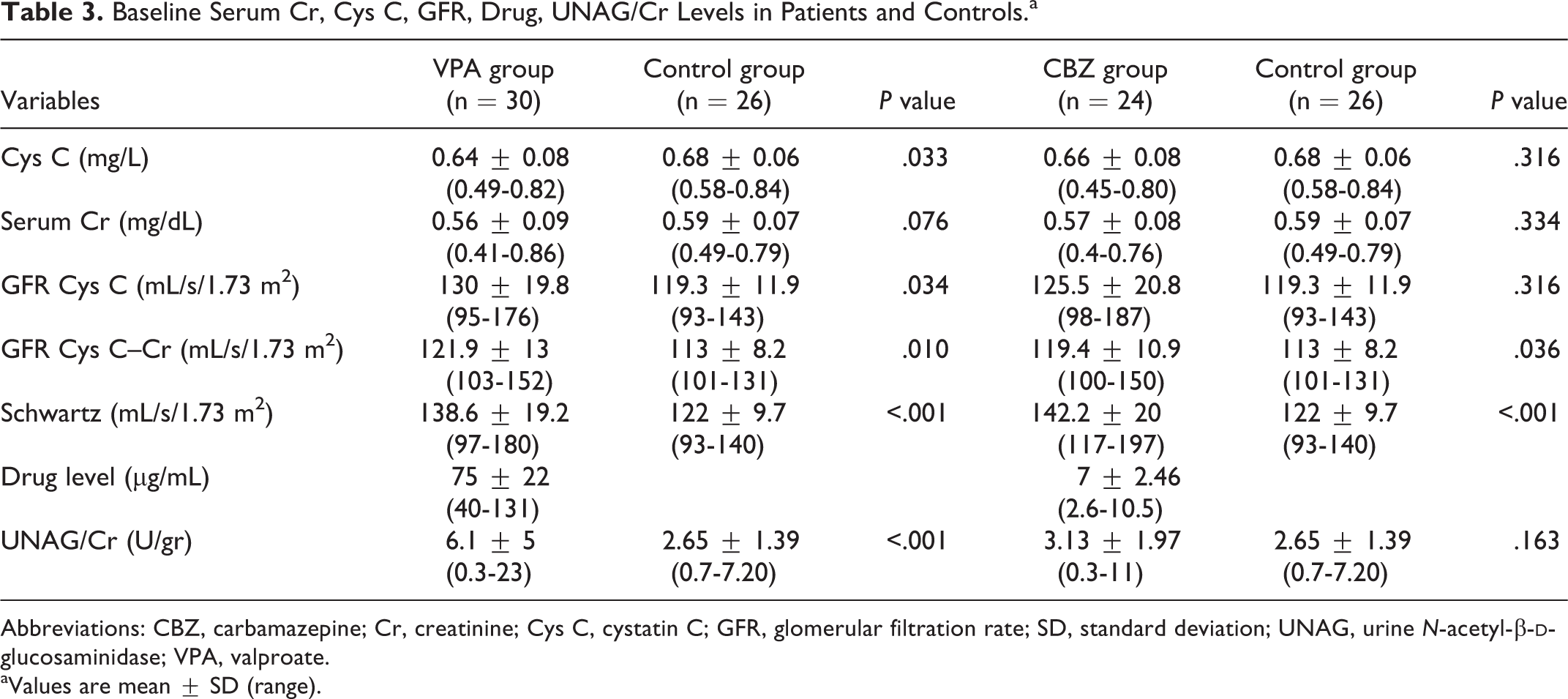
Abbreviations: CBZ, carbamazepine; Cr, creatinine; Cys C, cystatin C; GFR, glomerular filtration rate; SD, standard deviation; UNAG, urine N-acetyl-β-
aValues are mean ± SD (range).
In longitudinal analyses, average serum cystatin C and creatinine concentrations, and glomerular filtration rate cystatin C, glomerular filtration rate cystatin C–creatinine, Schwartz, and urine N-acetyl-β-
Serum Cr, Cys C, GFR, drug, UNAG/Cr Levels at Baseline and at Month 6 in Patients Receiving Valproate.a
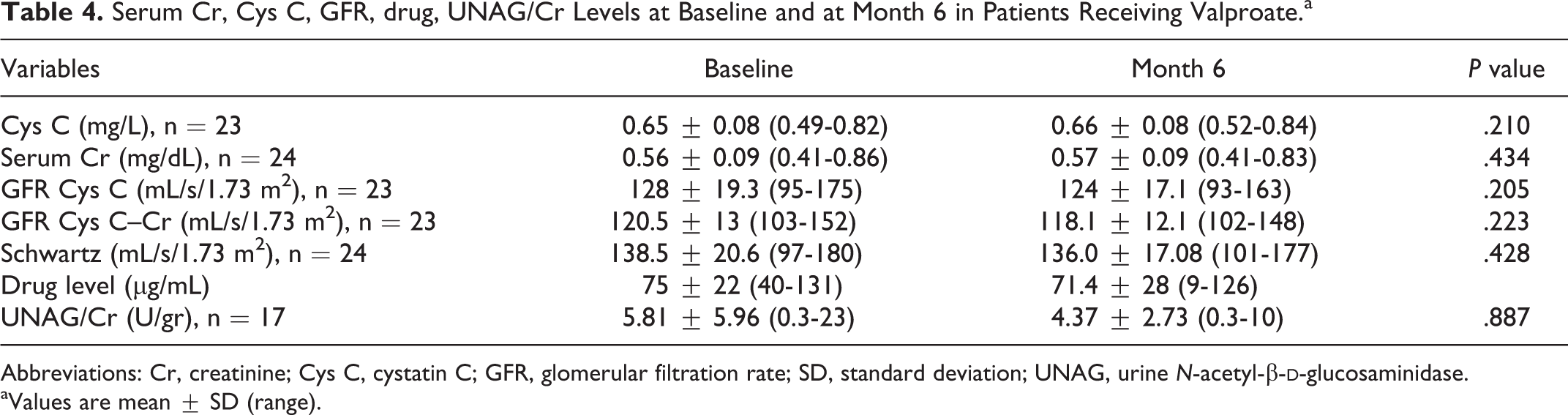
Abbreviations: Cr, creatinine; Cys C, cystatin C; GFR, glomerular filtration rate; SD, standard deviation; UNAG, urine N-acetyl-β-
aValues are mean ± SD (range).
Serum Cr, Cys C, GFR, drug, UNAG/Cr Levels at Baseline and at Month 6 in Patients Receiving Carbamazepine.a
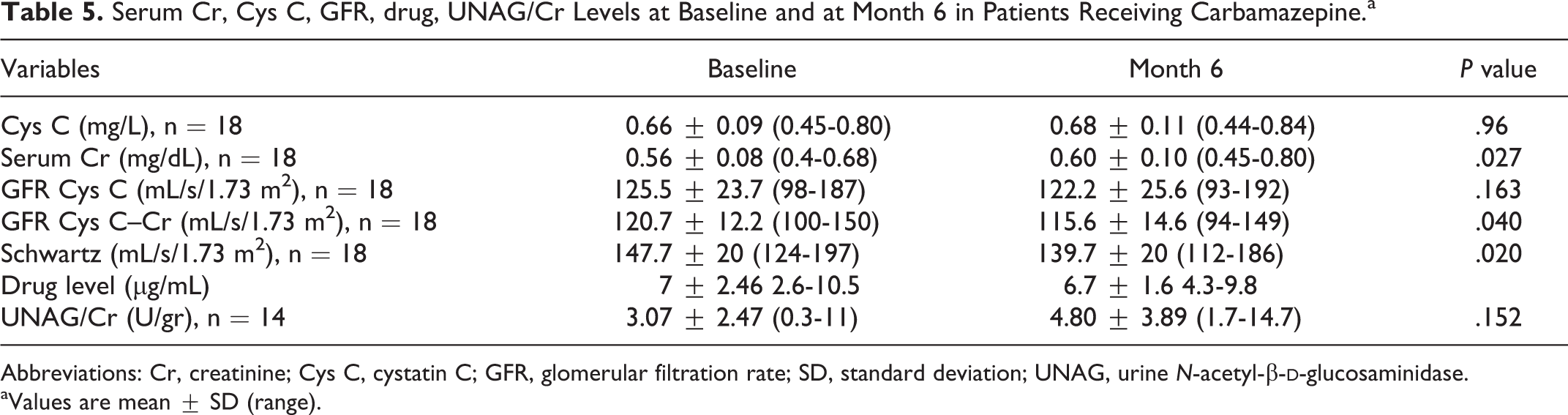
Abbreviations: Cr, creatinine; Cys C, cystatin C; GFR, glomerular filtration rate; SD, standard deviation; UNAG, urine N-acetyl-β-
aValues are mean ± SD (range).
Discussion
Consistent with previous studies, the present prospective study showed an increased excretion of tubular N-acetyl-β-
In our study, there was no correlation between the urinary N-acetyl-β-
In another study, Verrotti et al
17
showed an increased level of N-acetyl-β-
All studies in the literature have emphasized an increased risk of tubular functional impairment in patients receiving valproate and carbamazepine therapies, and they all have suggested screening of tubular functions in these patients even if the renal function tests were normal.
One of our goals in this study was also to see the effect of antiepileptic drugs on the glomerular filtration rate of the patients. Inulin clearance and iohexol clearance are both considered as gold standards for glomerular filtration rate measuring. 18 The most practical common marker used to estimate glomerular filtration rate is serum creatinine concentration. However, tubular creatinine secretion, muscle mass, age, gender, regular diet, and hepatic function of the patients all affect serum creatinine concentration. Creatinine clearance is a much more sensitive method for the detection of renal dysfunction, but it requires very precise urine collection for 24 hours. Therefore, a recent research has been directed toward the identification of a more specific, reliable, and practical serum marker of glomerular filtration rate. 19 Serum cystatin C has been proposed as a new endogenous marker of glomerular filtration rate. 20 Several studies have shown that cystatin C correlated better with inulin or chromium ethylenediaminetetraacetic acid clearance than serum creatinine in patients with mild to moderately impaired renal function. 21–23
In our study, we evaluated both cystatin C and serum creatinine levels. Moreover glomerular filtration rate was estimated by using recent formula with cystatin C, serum creatinine, and cystatin C + serum creatinine . The values of the glomerular filtration rate calculated with all 3 formulas were within the normal reference values. 14,15 Although the glomerular filtration rate values calculated with all 3 different formulas of valproate and carbamazepine groups were within the normal reference ranges, they were significantly higher than the values of the control group. (However, the patients’ glomerular filtration rate values calculated using cystatin C levels in the carbamazepine group were higher than the values of the control group, though statistically insignificant. Because the glomerular filtration rate, cystatin C–creatinine formula was more predictive than the glomerular filtration rate cystatin C formula, this discrepancy is not considered important). Because the patients and control groups were similar in terms of age, height, body mass index, and body weight, this high value may suggest subclinical hyperfiltration of early glomerular toxicity, which is also seen in some other chronic disorders such as diabetes mellitus and sickle cell anemia. 24 –26 Studies in experimental animals indicate that dilatation of the afferent (precapillary) glomerular arteriole plays an important role in the hyperfiltration response, by raising both the intraglomerular pressure and renal blood flow. 24 Why these hemodynamic changes occur is not well understood in diabetes mellitus, but factors that may contribute to afferent arteriole dilation include insulin-like growth factor I, atrial natriuretic peptide, sex hormones, intracellular sorbitol, early glycation products, and enhanced tubular sodium reabsorption in the proximal tubule. 27 –32 Otherwise, glomerular ischemia appears to promote increased renal blood flow and glomerular filtration rate in sickle cell anemia. Studies in mice suggest that increased glomerular nitric oxide synthesis also could contribute to the glomerular hyperfiltration. 33,34 It could be speculated that antiepileptic drugs and their metabolites can cause glomerular arteriolar dilation and increased blood flow and glomerular hyperfiltration. When the antiepileptic drug usage is continued for a longer period of time as stated above, the glomerular filtration rate may be reduced in time because of the effect of the antiepileptic drugs rather than the disease itself. Patients who use these drugs for a certain amount of time should be reevaluated for glomerular filtration rate. Csáthy et al 8 and Unay et al 4 found normal urea and creatinine concentrations in patients receiving antiepileptic therapy. In addition, Altunbaşak et al 35 did not find impaired creatinine clearance in children receiving valproate. Because there is no other study in the literature using cystatin C level and serum creatinine for the estimation of glomerular filtration rate in the patients having antiepileptic drug, our results can be used as reference values.
The major limitations of this study can be stated as follows: we have no values of N-acetyl-β-
In conclusion, our data suggest that valproate and carbamazepine have varying degrees of adverse effects on renal tubular functions in children with epilepsy. Whether these drugs affect glomerular function and what is the mechanism involved is not clearly known and has not been widely investigated. Therefore, renal tubular and glomerular function in children receiving carbamazepine and valproate should be kept in mind.
Footnotes
Acknowledgment
This study was conducted at the Gazi University Faculty of Medicine, Ankara, Turkey.
Author Contributions
CH, KG, and NB designed the study. UY, EG, OG, ED, and AS collected and analyzed patient data and drafted this article. All authors have contributed and agreed to the content of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study received ethical approval from the Ministry of Health of Turkey General Directorate of Pharmaceuticals and Pharmacy Ethics Committee. Ethics Committee approval number: 45484.