
Abstract
In South Africa, and worldwide, rheumatic fever represents a public health problem. Improved diagnosis and management of Sydenham chorea, a major manifestation of acute rheumatic fever is key to prevention of rheumatic heart disease. This article reviews Sydenham chorea from its original description to current opinions. Recommendations are founded on expert opinion as class 1 data is lacking. This South African perspective is relevant to resource-poor settings globally insofar as it provides diagnosis and management recommendations for primary- and secondary-level healthcare professionals who care for patients in such environments. Four basic tenets of care are recommended, namely, elimination of the streptococcal infection, symptomatic treatment, immunological treatment, and nonpharmacologic interventions. A user-friendly outcome measurement tool, viable for use in low-resource settings is presented. Introduction of this tool may lead to increased awareness of the neuropsychiatric manifestations of poststreptococcal movement disorders in Africa, where reports are limited.
Introduction
Sydenham chorea was first described by Thomas Sydenham in 1686 and has received ongoing attention since then. Nevertheless, it remains an enigmatic condition, and clinicians continue to seek more reliable diagnostic procedures and efficacious interventions. This paper combines the first author’s (KW’s) clinical experience through working in a dedicated rheumatic fever clinic, prospective studies from the center focused on diagnostic scales, prognostic markers, and the published evidence base of clinical trials. In addition, the article highlights the need for awareness of the neuropsychiatric manifestations of movement disorders in Africa, where reports are limited.
Sydenham chorea is a major manifestation of acute rheumatic fever. 1 Although the incidence of acute rheumatic fever has declined significantly in high-income countries, it remains a problem in low-income countries. 2 –4 A minimum of 15.6 million people worldwide are estimated to have established rheumatic heart disease and close to 300 000 new cases are identified each year, with 233 000 directly attributable deaths. 5 The prevalence of rheumatic heart disease in children aged 5 to 14 years (as of 2005) is highest in sub-Saharan Africa (5-7 per 1000), the Pacific, and indigenous populations of Australia and New Zealand (3-5 per 1000) and South-Central Asia (2.2 per 1000). Prevalence is lowest in high-income countries (0.5 per 1000). 5 Global prevalence data for Sydenham chorea are lacking. 6
In contrast, other neuropsychiatric movement disorders such as Tourette’s disorder report prevalence rates of 1% in the worldwide community. No prevalence data on Sydenham chorea, PANDAS (pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection), or Tourette’s disorder are recorded in sub-Saharan Africa. 7 This raises the question whether such neuropsychiatric conditions are rare in Africa or whether they are merely underdiagnosed? If the former is true this would have important genetic and environmental implications. If the latter is correct, strategies are required to increase awareness, knowledge, and tools to improve identification and treatment.
Sydenham chorea is the most common form of acquired chorea in children and may be the presenting feature of acute rheumatic fever. 8,9 The last 2 decades have seen a re-emergence of Sydenham chorea in North America. The condition should always be considered when evaluating new-onset movement disorders in childhood. 10 There being no specific laboratory marker for Sydenham chorea, the diagnosis relies on a careful clinical history, examination, and laboratory assessment to exclude alternative causes of chorea. 8,11,12
Previously, Sydenham chorea was thought of as an isolated movement disorder with management consisting of symptomatic treatment of the involuntary choreiform movements. 13,14 In 1894, Osler was the first to describe the behavioral component of Sydenham chorea, which he referred to as “perseverativeness of behaviour.” Since the 1990s, several comprehensive reviews have described the psychiatric component. 15 –18 It is now accepted that Sydenham chorea is a neuropsychiatric movement disorder and that treatment should include assessment for and treatment of the comorbid psychopathologies. 9,14,19,20
Diagnosis
Dr T. Duckett Jones proposed the original criteria for the diagnosis of acute rheumatic fever in 1944. Referred to as the Jones criteria, these criteria have been modified 4 times with the most recently revised criteria published in 1992. 21 Jones criteria remain a guideline for diagnosis. 1,21 In the presence of other major Jones criteria, the diagnosis of Sydenham chorea is straightforward. The 1992 modified Jones criteria stated that the presence of Sydenham chorea alone (pure chorea) was sufficient to make a diagnosis of acute rheumatic fever. 21
Interestingly, the prevalence of chorea in patients with acute rheumatic fever varies widely. The proportion of patients with chorea in all cases of acute rheumatic fever from selected published studies shows a percentage variation from 1 to 52 percent. 22 The apparent predilection of certain populations to chorea may offer clues to the pathogenesis. Furthermore, this variance in prevalence may relate to characteristics of the group A streptococci that cause acute rheumatic fever. 22
Sydenham chorea is characterized by significant variability in clinical presentations. 8,9,19 Patients may have severe chorea and few psychiatric symptoms or they may present with severe psychiatric symptoms and a mild neurologic component. 19 Abnormal movements may include tics and ballistic movements in addition to classical chorea. 8,23 –25 When tics are present rather than classical chorea, and no other major manifestations of acute rheumatic fever are present, the diagnosis becomes more difficult.
A number of psychiatric movement disorders following streptococcal infection are described. 23,24,26 The term PANDAS was coined to describe a subset of children with sudden-onset infection-related obsessive-compulsive disorder or tic disorders that meet specific criteria. 27,28 Swedo stated that “PANDAS is not equivalent to a mild case of Sydenham chorea, as the presence of chorea, rheumatic carditis or any of the other major manifestations of rheumatic fever is an exclusionary criterion for PANDAS.” 28 The entity of PANDAS remains controversial, and an in-depth discussion is beyond the scope of this article.
Pediatric acute-onset neuropsychiatric syndrome (PANS) is a more recent term used to describe acute onset of neuropsychiatric conditions with a range of potential etiologies. 28,29 A key diagnostic feature of pediatric acute-onset neuropsychiatric syndrome is the acute dramatic onset of an obsessive-compulsive disorder or severely restricted food intake. There are also a range of other accompanying neuropsychiatric symptoms. It can be associated with or without an environmental trigger but “the symptoms must not be better explained by a known neurological or medical disorder.” The associated neuropsychiatric symptoms comprise anxiety, emotional lability and depression, aggression and oppositional behavior, behavioral regression, sudden deterioration in school performance, sensory and motor abnormalities, and somatic signs and symptoms. These proposed criteria require further validation. 28
Sydenham chorea and PANDAS exhibit many clinical and laboratory similarities as outlined in Table 1. 23,24,26,30 –34 They are proposed to be antineuronal, antibody-mediated neuropsychiatric movement disorders. Antibodies that arise in response to group A beta-hemolytic streptococcus infection are proposed to cross-react with epitopes on neurons within the basal ganglia, frontal cortex, and other regions. Studies support that children with Sydenham chorea have elevated serum antineuronal antibody titers and antibodies to surface dopamine-2 receptors. 28,29,34 –39
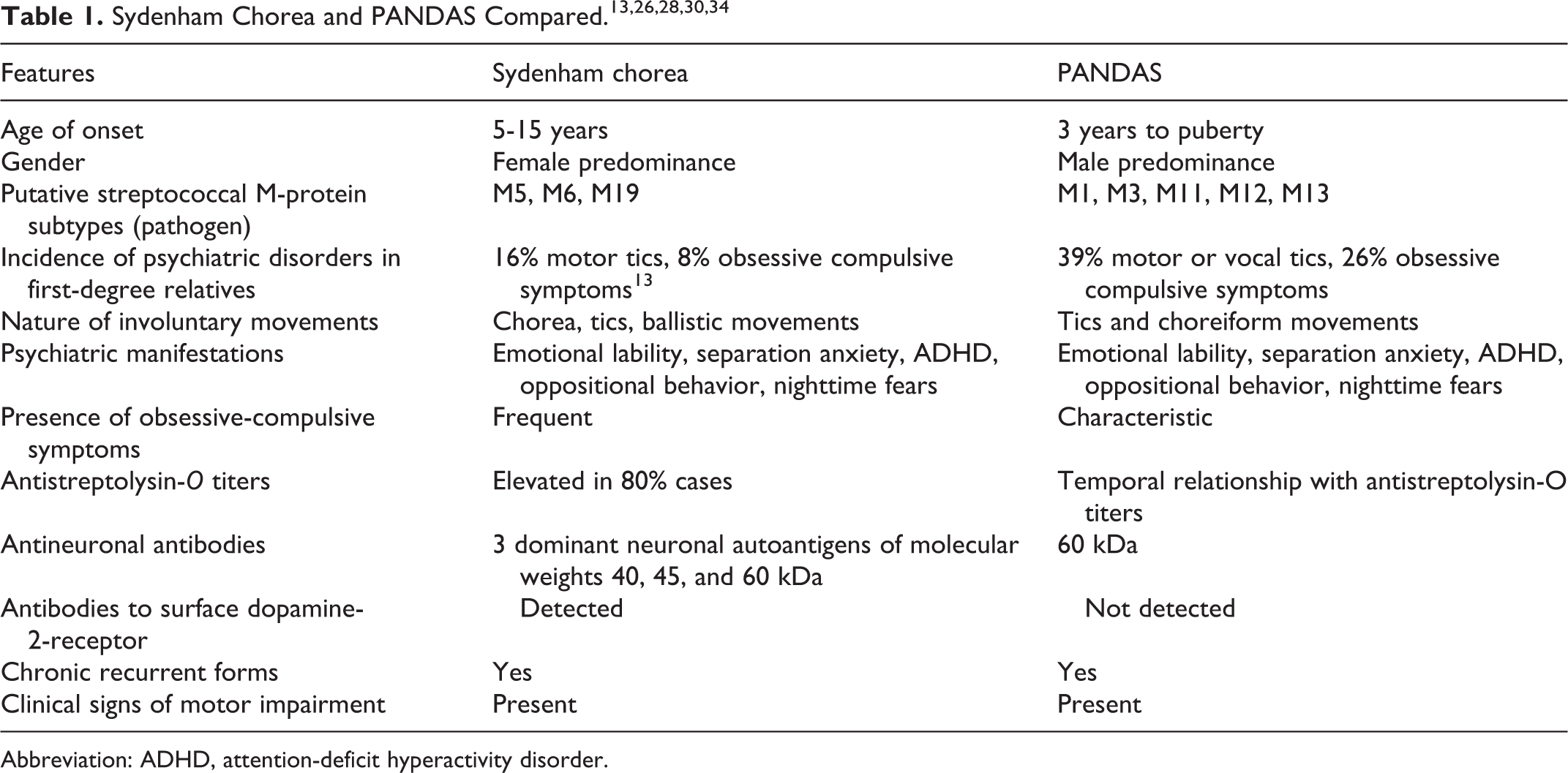
Abbreviation: ADHD, attention-deficit hyperactivity disorder.
In contrast to Sydenham chorea these dopamine-2 receptor antibodies were not detected in PANDAS. 34 Studies by Swedo and colleagues at the National Institute of Mental Health (NIMH) have shown that some cross-reactive “anti-brain” antibodies do not produce full-blown Sydenham chorea, but instead cause obsessive-compulsive behavior, tics, and the other neuropsychiatric symptoms of PANDAS hypothesized as being a forme fruste or unusual form rather than a mild form of Sydenham chorea. 28 PANDAS has also been suggested to be neurologically specific (no cardiac involvement) whereas Sydenham chorea is part of a multiorgan disease. 23,40 In the author’s center, a retrospective study of 42 children with Sydenham chorea found that 6 children diagnosed with Sydenham chorea were subsequently diagnosed with PANDAS and of these, 5 children had cardiac involvement. 13 Because access to echocardiogram screening has become more routinely available, functional and morphologic valve changes are reported in increasing numbers of patients with PANDAS. 41 –44 This is contrary to the original PANDAS hypothesis as established by Swedo et al. Differences between Sydenham chorea and PANDAS are highlighted in Table 1. 13,19,23,24,26,30,34,37,39,45,46 A difference not addressed in this table is whether Sydenham chorea patients require penicillin prophylaxis to protect the heart and patients with PANDAS do not. Penicillin may be beneficial in PANDAS as 2 separate trials on patients with PANDAS demonstrated that prevention of group A beta-hemolytic streptococcus infections was associated with decreased numbers of neuropsychiatric symptom exacerbations and overall improvement in symptom severity. 47 –49 These were small observational studies. There are anecdotal reports suggesting rapid symptom alleviation after antibiotic prescription (by elimination of the streptococcal infection) in PANDAS. 34 In the South African context, it is recommended that penicillin be prescribed for all poststreptococcal neuropsychiatric conditions. We recommend that the diagnosis and monitoring of these 2 conditions not be differentiated at primary health care levels. Given the high prevalence of rheumatic heart disease, an approach that includes Sydenham chorea and PANDAS as being on the same spectrum, under the umbrella of poststreptococcal neuropsychiatric movement disorders, may provide a safety net that avoids missed diagnoses following group A beta-hemolytic streptococcus infection. Health care workers based at the primary level receive basic training in neurology and psychiatry during their training and may not be in a position to distinguish between the subtle semantics of abnormal movements. It is important that they recognize poststreptococcal neuropsychiatric movement disorders and refer appropriately. Notably, South Africa has 1.9 pediatricians per 100 000 population, 1.2 psychiatrists per 100 000 population, and there are 30 child neurologists. 50
As the diagnosis of Sydenham chorea is essentially a clinical diagnosis, history and examination are paramount. The B-cell antigen D8/17 is not considered helpful. 8,12 In the absence of other Jones Criteria, the diagnosis is then by exclusion of other causes of chorea that are summarized in Table 2. 9 Thorough screening for recent evidence of streptococcus infection is recommended as well as screening for cardiac involvement by echocardiogram. 41,42,51 Clinical examination to identify both the neurologic and psychiatric phenotypes and the impact on activities of daily living is essential. Markers for these are summarized in Tables 3 and 4.
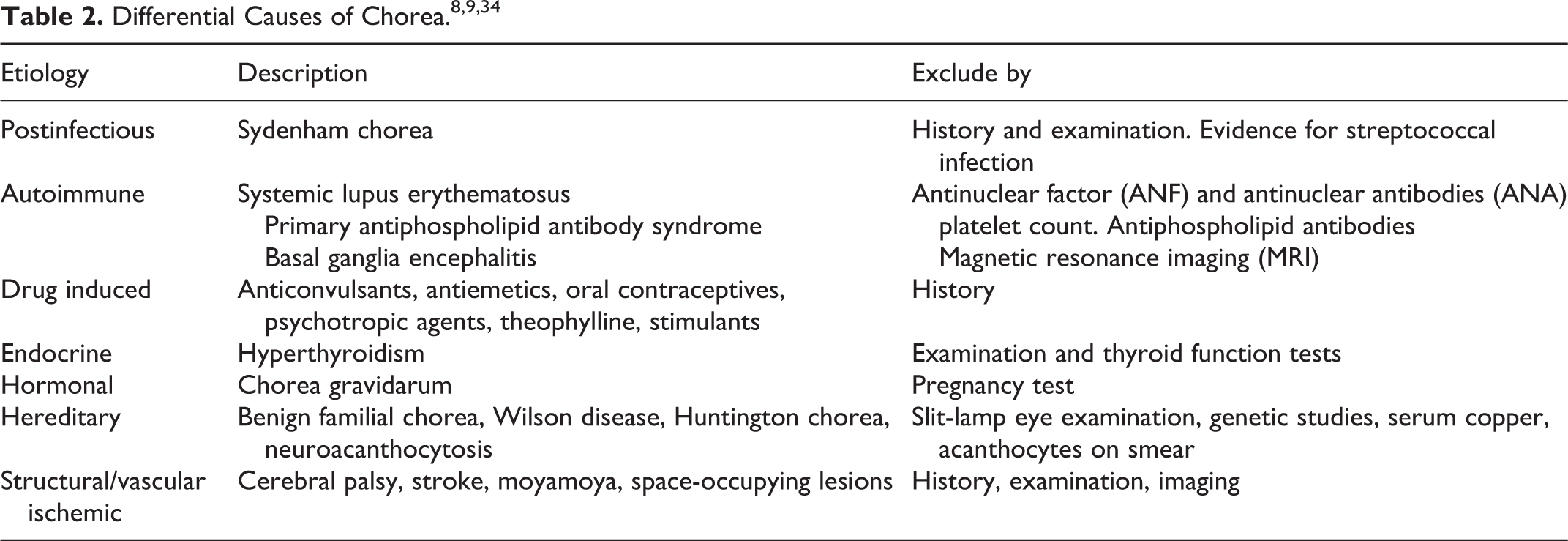
Causes of Chorea 8,9
Table 2 lists disorders that cause chorea in children. These causes may be postinfectious, drug induced, endocrine, hormonal, hereditary, structural, or vascular. 52 The more common causes and diagnostic tools are listed. A positive throat culture and a positive anti-streptolysin-O titer are not essential to make a diagnosis of Sydenham chorea as the condition may occur up to 9 months following streptococcal infection. 28 A rising titer is a more reliable diagnostic tool than a single antibody level. A comprehensive history and examination remain seminal to making a diagnosis and to permit focused testing from the list for conditions suspected or not otherwise excluded.
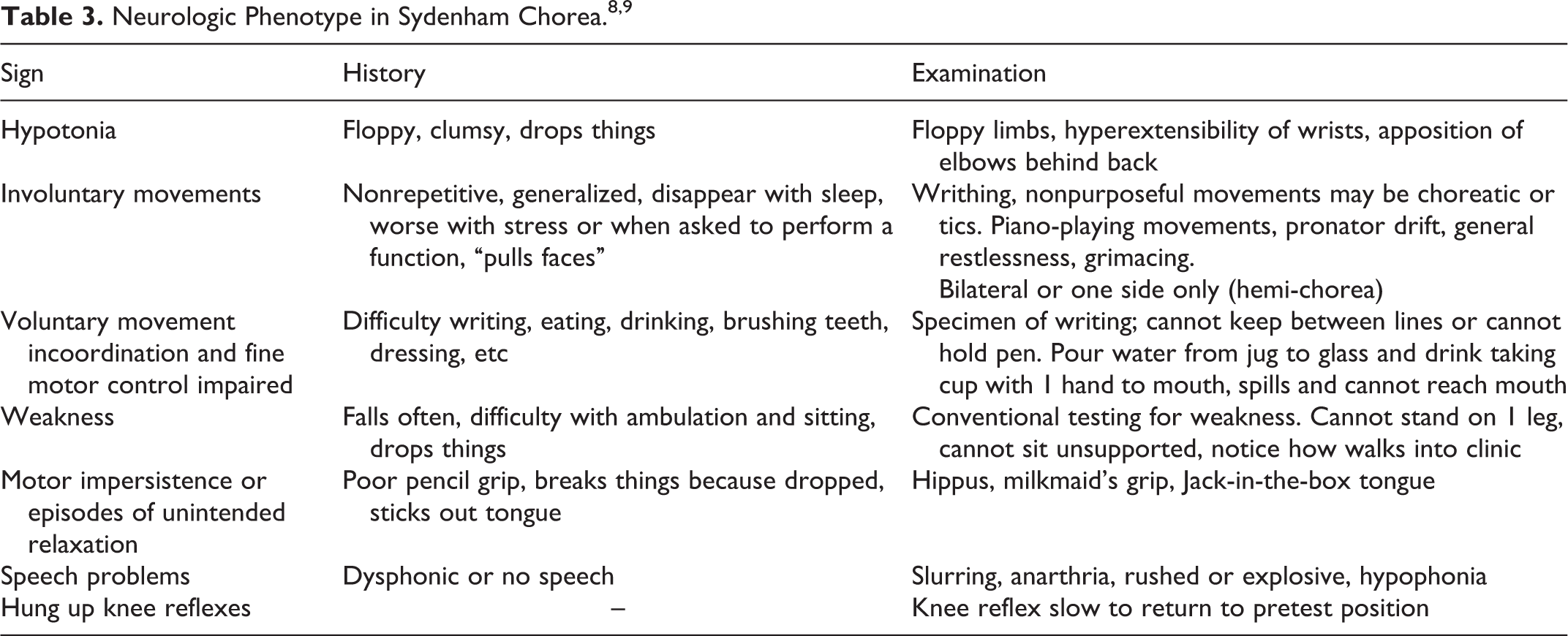
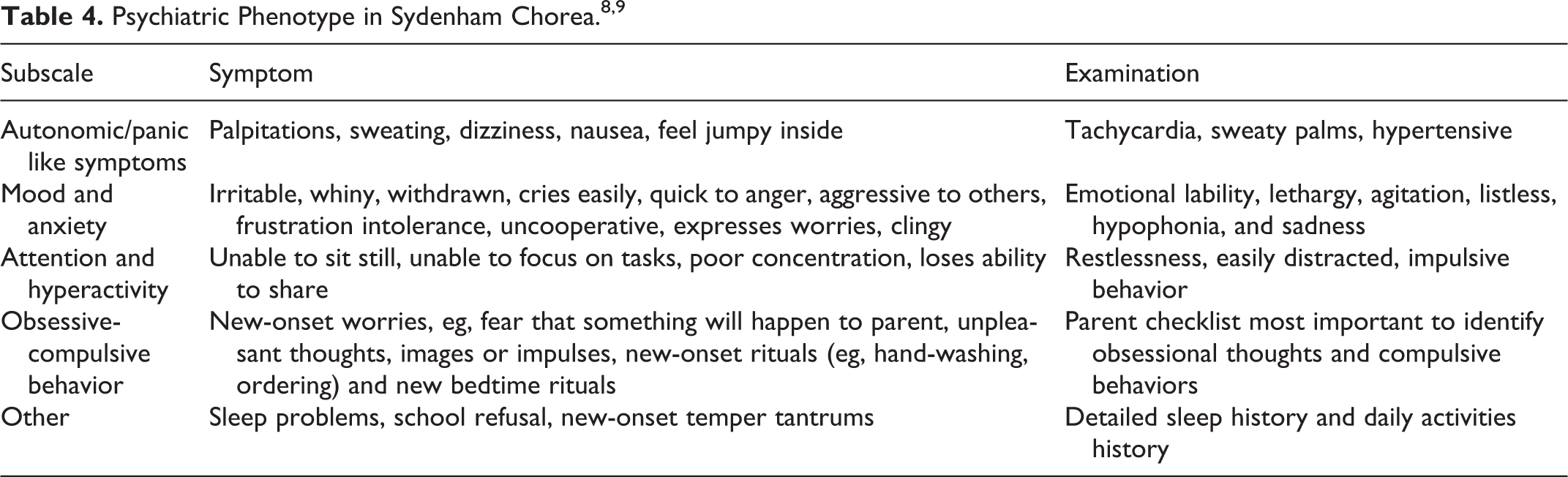
Clinical Features (Tables 3 and 4)
The clinical features include both neurologic abnormalities and psychiatric manifestations. The former comprise involuntary movements—chorea, tics, or ballistic movements, voluntary movement incoordination, muscular weakness, and hypotonia. 8,9,14 Psychiatric features include emotional lability, hyperactivity, distractibility, obsessions, and compulsions. 9,15,16,18,53
A combination of these symptoms results in difficulties in the execution of activities of daily living, thus impacting negatively on the quality of life of affected children. Movements disappear with sleep and rest. Voluntary movements make the chorea/tics worse. 9 Hypotonia and weakness range from mild to severe. The severe form is termed chorea mollis, or chorea paralytica, and may be confused with the clinical appearance of a stroke. 2,8,54 A change in behavior may precede the abnormal movements. For instance, the child may cry easily, show unusual aggression, make faces, or exhibit sudden onset of obsessions and compulsions that manifest as unusual behaviors for that child. 9,28,40 History taking is important to elicit behavior changes. Tables 3 and 4 provide a diagnostic checklist of the neurologic and psychiatric phenotypes and Table 5 is a behavior checklist for parents adapted for use in clinical settings. 30,49
Red X Behavior Check List for Parentsa (Recent Onset). 49
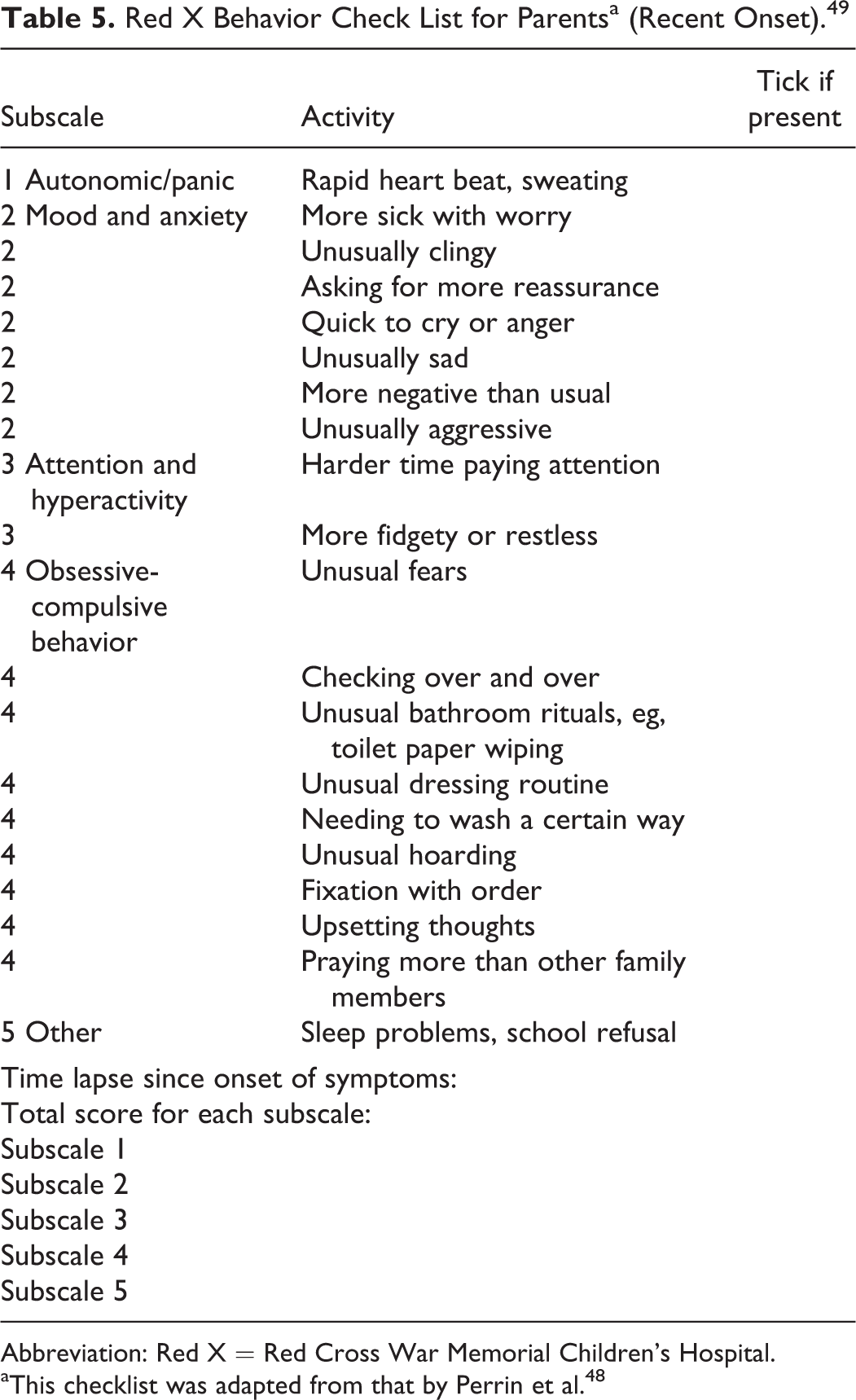
Abbreviation: Red X = Red Cross War Memorial Children’s Hospital.
aThis checklist was adapted from that by Perrin et al. 48
Neuroimaging in Sydenham Chorea
The main use of neuroimaging in Sydenham chorea is to exclude other acquired causes of chorea, notably vascular and structural etiologies. 8 Magnetic resonance imaging (MRI) showing enlargement of basal ganglia in the acute phase, with resolution correlating with decreased antineuronal antibodies is described. 55 However studies are limited and the numbers are small. Functional imaging such as single photon emission computed tomography (SPECT) is a useful tool for evaluation in research. It reveals changes in perfusion seen as hyper- or hypoperfusion. SPECT has indicated that the basal ganglia and frontostriatal regions are both commonly affected. 56 –58 In addition, recent SPECT studies show persistent changes after Sydenham chorea suggesting that perfusion abnormalities in the basal ganglia may persist in a select number of patients. 59
Clinical Rating of Severity
It is important to quantify the severity of symptoms in order to monitor treatment. In 1965 Aron devised a clinical classification which referred to “mild” in the presence of minimal movements, “moderate” in the presence of movements of obvious inconvenience to the patient but which did not interfere with self-care, and “severe” if there were movements sufficiently incapacitating for the patient to require assistance for the activities of daily living. 60 The scale of Teixeira et al, The Universidade Federal de Minas Gerais (UFMG) Sydenham’s Chorea Rating Scale (USCRS), assesses behavior, motor function, and functionality as reflected by the ability to perform activities of daily living. 61,62 This scale was tested at a Motor Disorders Clinic by specialists who were trained and experienced in the management of Sydenham chorea and not by primary-level medical practitioners who form the main point of contact for patients in areas where acute rheumatic fever is endemic.
The WWW (Walker, Wilmshurst, Wendy) Clinical Rating Scale for Sydenham chorea is a scale designed to be “user-friendly” for primary health care workers. This scale includes neurologic and psychiatric signs and symptoms, and like the Universidade Federal de Minas Gerais scale it assesses behavior, functionality and motor function but at a lower level of specificity than the Universidade Federal de Minas Gerais scale. This scale was devised in 2002 for use as an outcomes measurement tool for a randomized controlled treatment trial in Sydenham chorea. 56
Since completion of the trial, the scale was modified to improve its use by primary health care physicians. The psychiatric and neuro-motor components plus the effect of these on activities of daily living are clearly itemized in a table. The clinician notes the presence or absence of a clinical sign and calculates a total score. Scores range from 0 to 30 and provide the clinician with an objective measure of clinical progress. This Red X (Red Cross) Clinical Rating Scale for Sydenham chorea is shown in Figure 1. Further research is needed to investigate the psychometric properties of this scale.
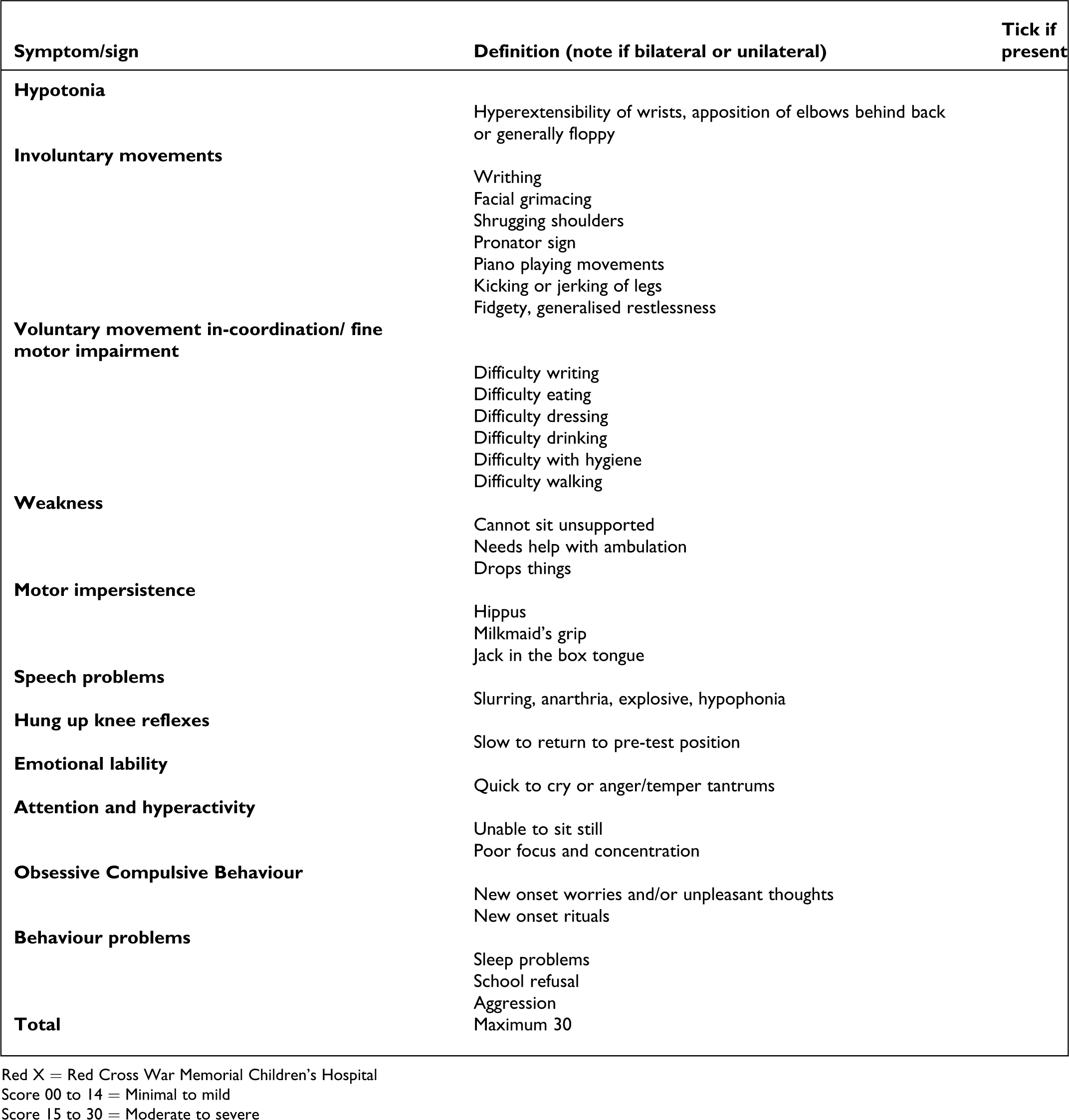
Red X Clinical Rating Scale for Sydenham Chorea. Score 00 to 14 = minimal to mild; score 15 to 30 = moderate to severe. Abbreviation: Red X = Red Cross War Memorial Children’s Hospital.
Our recommendation is that patients be assessed (using 1 of these tools) at regular intervals. It is important to emphasize that these are symptom rating scales and not diagnostic tools.
Treatment Strategies for Sydenham Chorea
In South Africa, there is increasing surveillance with the intent to prevent rheumatic fever and rheumatic heart disease. Every child with Sydenham chorea should be notified and should undergo echocardiography. 63,64
Treatment of Sydenham chorea is multidisciplinary and has 4 main tenets: elimination of the streptococcus, pharmacologic symptomatic treatment of the involuntary movements and psychiatric symptoms, treatment of the immune and inflammatory response, and nonpharmacologic treatment strategies that aim to support the patient and family. 7,14
Primary Treatment: Elimination of Streptococcus
When Sydenham chorea is diagnosed, penicillin 500 mg twice daily for 10 days is recommended. 42,65,66 Rest is advised as movements disappear with sleep and are aggravated by voluntary movements. Prophylaxis with long-term penicillin is primarily given to protect the heart. The South African updated Guideline recommends intramuscular penicillin every 21 days. 42,67 To date, the Rheumatic Fever Clinic at the Red Cross War Memorial Children’s Hospital has adhered to the Australian guideline of administering intramuscular benzyl penicillin every 28 days (1.2 million units if patient weighs 30 kg or more and 600 000 units if weight is less than 30 kg) or oral penicillin VK 250 mg twice daily as secondary prevention of rheumatic heart disease. 65 Intramuscular penicillin is the preferred route but where children find the injection too traumatic we work on the principle that “any form of treatment course of penicillin is better than no penicillin.” 67 The decision to use this guideline is governed by convenience factors for the patient and caregiver thereby enhancing adherence.
Painful injections can be minimized by diluting penicillin with 1% lidocaine instead of sterile water. 68 Australian guidelines recommend secondary penicillin prophylaxis until 21 years old in the presence of a normal heart and until 35 to 40 years where rheumatic heart disease exists.
Patients must be advised to seek primary treatment for future streptococcal sore throats.
Symptomatic Treatment
Despite more than 3 centuries of experience, no expert consensus guideline has been established using current methods of guideline formulation. Treatments have ranged from bleeding, purging, hyperthermia, anti-inflammatory agents, sedation, and currently, a variety of oral pharmacotherapy is prescribed. The use of sedation was based on the observation that excitement and stress aggravates symptoms and sleep diminishes them. In the 1960s, barbiturates, bromides, and chloral hydrate were used for sedation.
Currently, agents that affect the neurotransmitters dopamine and γ-aminobutyric acid (GABA) are used as symptomatic treatment. 14 Dopamine D2 receptor antagonists include haloperidol, pimozide, and risperidone. Sodium valproate increases GABA in the brain. 29 These agents are used as symptomatic medications, and slow titration is recommended to reach maximum effect with minimal toxic manifestations.
There is limited evidence base for the use of these agents. 8 Studies pertaining to pharmacotherapy are uncommon, control groups are rare, and objective outcome measures are not always used. 14 Recommendations for the use of these agents remain “off label” and no guidelines exist that indicate when treatment should be stopped. 8
The experience at our clinic has primarily been with antipsychotics such as haloperidol. However, others have advocated the atypical antipsychotics, which may have the advantage of being associated with fewer extrapyramidal side effects, but it must be emphasized that side effects are more common in all groups in the presence of Sydenham chorea. 7,8 Systematic studies of these agents are needed.
In South Africa, haloperidol is currently a first-line therapy as it is inexpensive and readily available. Use of haloperidol is based on a regimen of “start low and go slow”; 0.025 mg/kg/d in divided doses going up to a maximum of 0.05 mg/kg/d in divided doses but the total daily dose should not exceed 2 mg. 7,14 This dose is less than that given for psychotic disorders. Smaller doses are sufficient and higher doses more likely to cause side effects in the presence of chorea. 7,28 As the atypical antipsychotics become cheaper and more readily available, they increasingly become a consideration.
Sodium valproate is a simple branched-chain fatty acid with a complex mechanism of action, including the inhibition of catabolism of GABA. When used to treat Sydenham chorea, recommended doses of sodium valproate vary between 15 and 20 mg/kg/d in 2 or 3 divided doses. 25,69,70
There are detailed descriptions of the psychiatric manifestations in Sydenham chorea but no randomized controlled trials of treatments specifically targeting these symptoms. Sodium valproate may benefit hyperactivity, impulsivity, irritability, and aggression in bipolar disorder and Sydenham chorea. 69 A randomized controlled trial of sodium valproate in Sydenham chorea would assist clarification of the potential efficacy of the agent. Selective serotonin reuptake inhibitors are used to treat obsessive-compulsive behaviors but have not been rigorously studied in the context of Sydenham chorea. 29
Therapeutic Interventions: Immunological Treatments
The serum of patients with Sydenham chorea indicates that the condition is a humorally mediated autoimmune condition. 36 Immunomodulatory therapies are described using corticosteroids, intravenous immunoglobulins, and plasma exchange. 56 Prednisone and methylprednisolone have been used in the presence of carditis or with chorea refractory to symptomatic agents or where unacceptable side effects occur. 8,71 –73 Treatment with steroids show a trend to better outcomes. 13,71 –73 However, a limitation to the use of steroids in South Africa is the high prevalence of tuberculosis in our communities where acute rheumatic fever occurs. Small studies using intravenous immunoglobulins show promising results but the intervention is expensive and beyond the capacity of resource-poor settings. 56
Plasma exchange was tried by Garvey and colleagues in the United States. The numbers are small and this intervention is not readily available in low- and middle-income countries.
Studies show that the disease process of Sydenham chorea can damage or sensitize the brain. 59 Immunomodulatory treatments by suppressing the inflammatory response may in essence be “curative.” Controlled studies are needed to definitively clarify the efficacy of these interventions. In the South African context, the use of steroids and/or intravenous immunoglobulins should only be implemented with specialist supervision.
Nonpharmacologic Treatment Strategies
Management should aim at the optimal treatment of the child as a whole. The patient, family, and educators must become partners in the treatment process of neuropsychiatric conditions. 7,74 Holistic management is multidisciplinary. In addition to medical interventions, psychoeducation and appropriate psychotherapies may be beneficial. 7
Psychoeducation may include the use of a behavior checklist, providing information regarding symptoms and the implications thereof and supportive reassurance. Other supportive strategies include offering and gaining informed consent to write to the teacher. Teachers are often the first to notice symptoms, and including these professionals in the treatment plan may be beneficial. Evidence-based psychotherapies such as cognitive-behavioral therapy for obsessive-compulsive behaviors should be considered. It goes without saying that active listening to the patients’ and families’ descriptions of difficulties experienced is basic good clinical practice and should not be forgotten.
Conclusion
Sydenham chorea is a poststreptococcal, autoimmune, neuropsychiatric movement disorder with an acute or subacute onset and a varied clinical presentation. It is not always a benign self-limiting condition. 13,59 It is the most common form of acquired chorea as supported by case series of chorea from Tunisia, Iran, and Turkey. 75,76
Documentation of movement disorders in Africa is scant and the few reports to date suggest a lower prevalence in Africa compared to other continents. 6 This raises the question of whether Sydenham chorea in Africa is underrecognized and thus underreported or whether the prevalence is in fact lower. This question is particularly important in light of the high prevalence of rheumatic heart disease in Africa.
Up to 60% of patients who present with Sydenham chorea develop rheumatic heart disease. 22 Rheumatic fever is the major cause of acquired heart disease in children. 42 Hence, when Sydenham chorea is diagnosed, treatment strategies include prevention of rheumatic heart disease.
A clearer picture of the prevalence of Sydenham chorea in Africa is needed. This article presents practicable diagnostic, monitoring, and management tools for use in resource-poor settings. The development of a registry for patients with Sydenham chorea may assist in establishing the prevalence in Africa. 77 Multicenter trials in resource-poor settings together with validation of the rating scale tool would go some way to alleviating the burden of disease by identifying patients at risk of developing rheumatic heart disease and psychiatric complications. Introduction of this tool may lead to increased awareness of the neuropsychiatric manifestations of poststreptococcal movement disorders in Africa. This South African perspective may be relevant to resource-poor settings globally.
Primary prevention remains the ultimate challenge. This would encompass eradication of poverty and poor living conditions. Until this millennium developmental goal is achieved, strategies to optimize management of Sydenham chorea are needed to reduce the burden of disease for such children.
Footnotes
Author Note
This article was based on a presentation delivered at the 6th World Congress of Pediatric Cardiology & Cardiac Surgery 2013 by the first author KW.
Acknowledgement
Dr Pauline Samia (MBChB, MPhil), pediatric neurologist at Aga Khan University, Departments of Pediatrics and Child Health, Nairobi, Kenya proof read the article. During her tenure as a fellow in Pediatric Neurology at Red Cross War Memorial Children’s Hospital she assisted in the management of patients with Sydenham chorea. Prof. Stein is supported by the Medical Research Council of South Africa.
Author Contributions
KW devised the WWW and Red X rating scales and wrote all the drafts of the article.PdV assisted in the formulation of the behavior checklist and critically appraised the article for intellectual content. DJS assisted in the psychiatric diagnosis of Sydenham chorea and critically appraised the article for intellectual content.JW supported KW in writing the proposals for the studies mentioned. She critically appraised all drafts. Together with KW, she devised the WWW clinical rating scale. All authors approved the final version prepared for submission
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.