
Abstract
Abusive head trauma has a robust and interesting scientific history. Recently, the American Academy of Pediatrics has endorsed a change in terminology to a term that is more general in describing the vast array of abusive mechanisms that can result in pediatric head injury. Simply defined, abusive head trauma is “child physical abuse that results in injury to the head or brain.” Abusive head trauma is a relatively common cause of childhood neurotrauma, with an estimated incidence of 16 to 33 cases per 100 000 children per year in the first 2 years of life. Clinical findings are variable; AHT should be considered in all children with neurologic signs and symptoms, especially if no or only mild trauma is described. Subdural and retinal hemorrhages are the most common findings. The current best evidence-based literature has identified some features—apnea and severe retinal hemorrhages—that reliably discriminate abusive from accidental injury. Longitudinal studies of outcomes in abusive head trauma patients demonstrate that approximately one-third of the children are severely disabled, one third of them are moderately disabled, and one third have no or only mild symptoms. Abusive head trauma cases are complex cases that require a rigorous, multidisciplinary team approach. The clinician can establish this diagnosis with confidence if he/she maintains a high index of suspicion for the diagnosis, has knowledge of the signs, symptoms, and risk factors of abusive head trauma, and reasonably excludes other etiologies on the differential diagnosis.
Keywords
Since its inception, abusive head trauma has been known by many different names—“whiplash shaken infant syndrome,” 1 “inflicted childhood neurotrauma,” 2 “nonaccidental head injury,” 3 “shaken baby syndrome,” and most recently, “abusive head trauma.” 4 This most recent shift in terminology reflects an attempt by the American Academy of Pediatrics to encourage physicians to utilize more general terms in describing the vast array of abusive mechanisms that can result in pediatric head injury. 4 As there are many mechanisms for inflicting pediatric head injury (blunt force trauma, acceleration/deceleration [inertial] forces, penetrating trauma, and asphyxiation), the use of more general terminology is, ironically, more diagnostically precise, as the exact abusive mechanism may not be immediately determinable.
Probably unbeknownst to many physicians, abusive head trauma/shaken baby syndrome has engendered some controversy in the public media 5 and legal literature. 6 As a consequence, physicians have increasingly been, and may continue to be, questioned about the validity of the diagnosis. This review will examine the historical context of the diagnosis, the current medical evidence base for the diagnosis, and areas of ongoing and future research. Finally, we will emphasize the subspecialist’s role, in particular the child neurologist, in the diagnosis and management of abusive head trauma.
Historical Context
Some of the strongest diagnostic roots of abusive head trauma can be traced back to the early 1900s. Prior to that time, physicians were highly influenced by the prevalent “germ theory” for medical diseases. Consequently, the medical community presumed that subdural hemorrhages were caused by infection and inflammation, terming it “pachymeningitis hemorrhagic interna.” Frustrated by that term, a prominent British neurosurgeon, Sir Wilfred Trotter, identified trauma as the primary etiology of subdural hemorrhages. 3 Trotter stated, “[Subdural hemorrhages] [are] almost if not quite invariably a true traumatic haemorrhage coming from veins torn in their course between the brain and a dural sinus.” 3 Trotter’s work paved the way for other physicians to reexamine the pathophysiology of subdural hemorrhages. As a consequence, multiple case reports by well-reputed physicians began to question other previously well-recognized causes—syphilis, 3,7 hydrocephalus, 3,8 and nutritional (scurvy) 3,9 —as the primary etiology for subdural hemorrhages.
Thereafter, physicians began publishing reports of various traumatic injuries, for which no presumable correlation could be found. In 1946, Dr John Caffey, widely recognized as the father of pediatric radiology, published a case series of 6 infants with subdural hemorrhages and long bone fractures. 10 In none of the 6 cases was there a historical report of trauma or of systemic disease. Nevertheless, after systematically ruling out all other causes, Caffey concluded that trauma was the most logical etiology for these radiologic findings. Caffey even associated the retinal hemorrhages in several of these cases to trauma. Caffey, however, was reluctant to conclude inflicted injury in these cases. In the 2 decades that followed Caffey’s historic article, multiple articles, from national and international authors, confirmed the association of subdural hemorrhages with trauma. 3,11
However, it was only in 1962 that the work of an eminent pediatrician, C. Henry Kempe, and his colleagues brought the issue of child abuse to the medical and national forefront. In their landmark article, “The Battered-Child Syndrome,” 12 Kempe et al carefully and thoughtfully described a syndrome of various injuries, including subdural hemorrhages, that resulted from trauma. However, unlike the vast majority of physicians that preceded them, Kempe et al concluded that these injuries resulted from the intentional acts of parents or other caregivers. Kempe et al stated that abuse “should be considered in any child exhibiting evidence of fracture of any bone, subdural hematoma, failure to thrive, soft tissue swellings or skin bruising, in any child who dies suddenly, or where the degree and type of injury is at variance with the history given regarding the occurrence of trauma.”
As a consequence of Kempe and colleagues’ historic work, and the general medical community’s increasing acceptance of child abuse as a viable medical entity, case reports continued to publish the presence of concurrent subdural hemorrhages, retinal hemorrhages, and bony lesions in infants, often without external signs of trauma. Finally, in the early 1970s, based on the work of Wilfred Trotter, numerous case reports, and the experimental biomechanical evidence of Ommaya and colleagues, 13,14 a British Neurosurgeon, A. Norman Guthkelch, and the Father of Pediatric Radiology, John Caffey, proposed shaking or whiplash injury as the cause of infantile subdural hemorrhages. 1,15 In theorizing that multiple acceleration and deceleration events caused by head shaking caused the intracranial injuries, Guthkelch stated that “the relatively large head and puny neck muscles of the infant must render it particularly vulnerable to whiplash injury.” That syndrome has evolved into what is known as abusive head trauma today.
Epidemiology
For various reasons, the precise incidence of abusive head trauma has proven elusive. Although definitional variance has been an issue, physician underdiagnosis 16 and underreporting have probably been the most pervasive and persistent reasons for imprecise data. Population-based studies 17,18 have estimated the incidence of abusive head trauma in the first 2 years of life to be 16 to 33 per 100 000 infants per year. Data (eg, anonymous parental surveys 19 ), however, suggest this to be an underestimate. Placed into perspective with other childhood maladies, abusive head trauma is as prevalent as neonatal meningitis (25-32 per 100 000 live births) and lymphatic leukemia (28.7-36.6 per 100 000 children <1 year old). 20 Yet, clinicians are still uncomfortable with the diagnosis and, more concerning, are still reluctant to even consider it on the differential in a child with head injury.
Several factors have been associated with an increased risk for abusive head trauma in a child (Table 1). Factors that have not been associated with an increased risk of abusive head trauma are race and ethnicity. Additionally, a triggering event, such as crying, has been linked with creating an environment conducive to, but not necessarily causative of, abusive head trauma. 26 As such, educating caregivers on the appropriate response to infant crying has been the subject of many abusive head trauma prevention programs.
Factors Have Been Associated With an Increased Risk for Abusive Head Trauma in a Child.
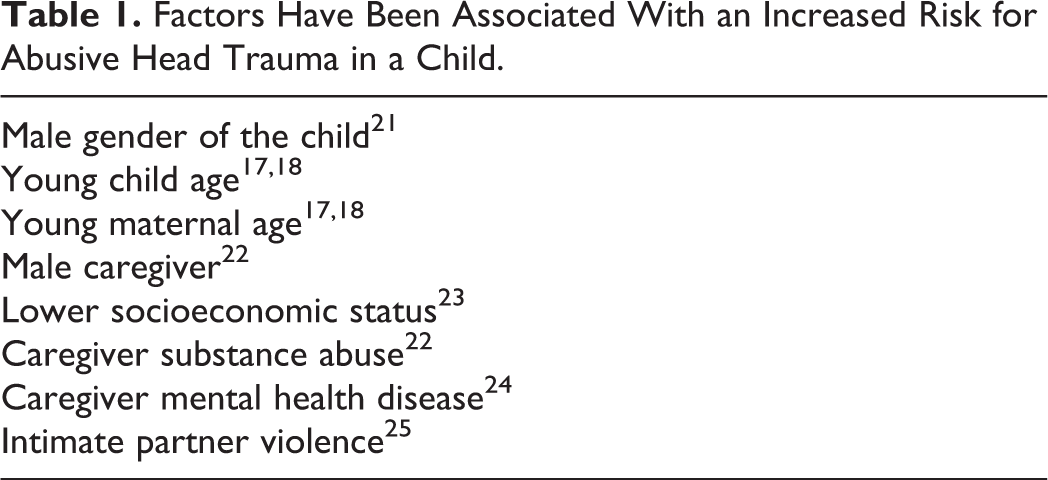
Although these risk factors are interesting and instructive, they should be implemented with caution. They are not to be utilized in creating a template or “patient profile” of abuse (ie, “a 2 month old male infant being cared for by mom’s boyfriend = abuse”). Using these factors in such a fashion will generate heuristics that invariably will result in cognitive diagnostic errors. Jenny et al 16 clearly demonstrated the disastrous consequences (missing 4 of 5 deaths resulting from abusive head trauma) that occur when physicians anchor upon certain risk factors and base diagnostic decisions upon erroneous patient profiles. These factors provide a backdrop. In cases concerning for abuse, they will “set the stage.” They will portray an environment of an already stressed caregiver, with an inadequate social support network, confronted with an additionally stressful event.
Diagnosis
Abusive head trauma is simply “child physical abuse that results in injury to the head or brain.” 27 However, determining whether abuse has occurred is itself not a simple process. Increasingly, physicians are recognizing that the best determinations in these difficult cases are made via a multidisciplinary team approach. 28 The typical composition of a multidisciplinary child protection team includes a child abuse pediatrician (now with subspecialty board certification available since 2009), a social worker, and relevant medical/surgical subspecialists (such as pediatric radiology, pediatric ophthalmology, and pediatric neurosurgery). The multidisciplinary child protection team confers with child protection workers and, occasionally, other investigative personnel to review all information related to a particular case, and renders diagnostic impressions.
Infants and children with abusive head trauma present with a wide range of symptoms—from nonspecific symptoms such as irritability, poor feeding, vomiting (15%), or delayed development (12%) to life-threatening symptoms such as lethargy (77%), respiratory compromise, seizures (43%-50%) or apnea. 20 The clinical presentation will depend on the severity of the inflicted trauma and, consequently, the severity of the resulting brain injury. Abusive head trauma can also result in a variety of physical findings: scalp injury, skull fractures, intracranial hemorrhage, diffuse axonal injury, cerebral edema, cervical spine fractures, cervical spinal cord injury/hemorrhage, retinal hemorrhages, rib fractures, and long bone fractures. As seizures or developmental delay are not uncommon presentations of abusive head trauma, the child neurologist will often be consulted in the diagnostic process.
Given the variability in presentation, clinicians should maintain a high index of suspicion for abusive head trauma. Abusive head trauma should be on the differential of all children less than 2 years with neurotrauma, and infants who present with a variety of nonneurologic presentations, such as increasing head circumference, vomiting, excessive crying, and developmental delay. In a recent systematic review by Maguire et al, the only reliably discriminating symptom between abusive and accidental head trauma was apnea, having a positive predictive value of 93% and odds ratio (OR) of 17 for inflicted brain injury. 29
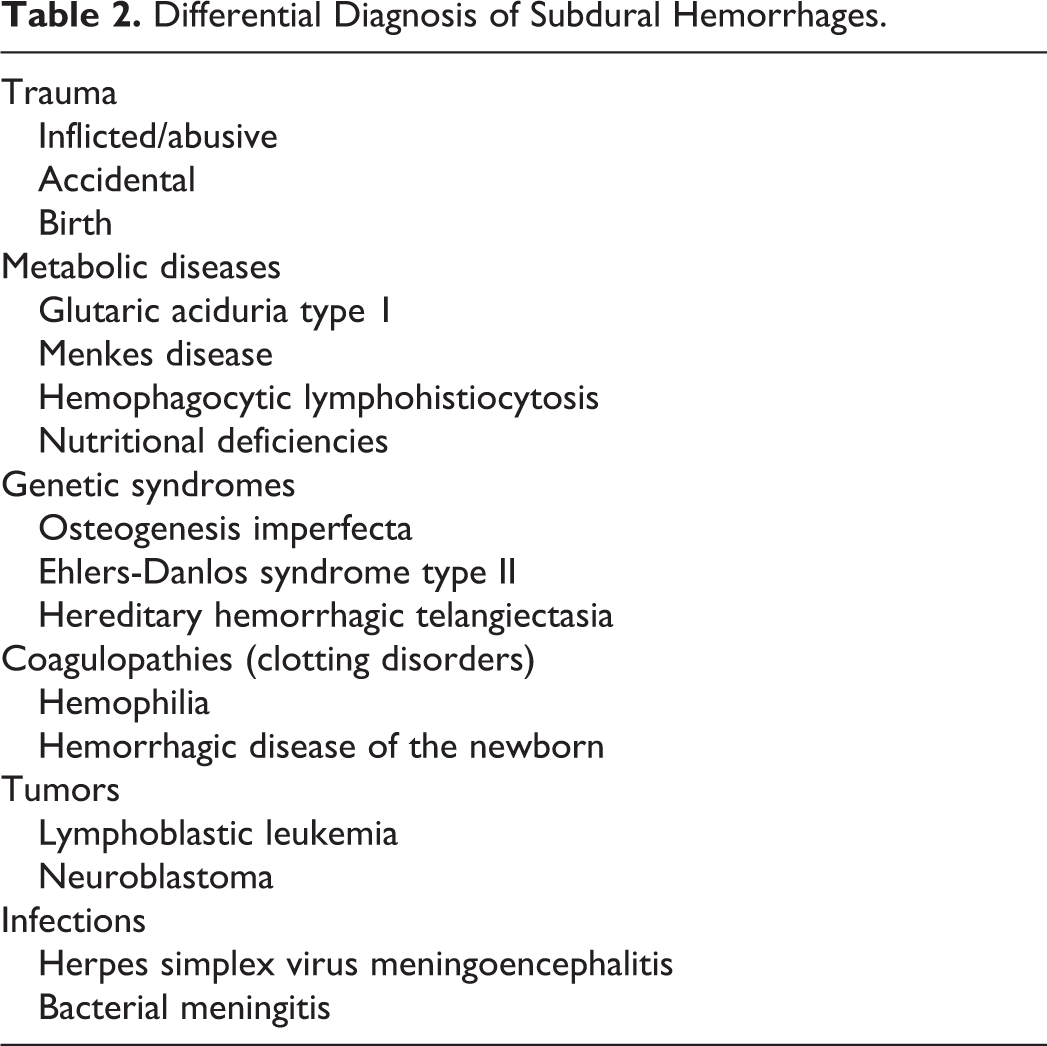
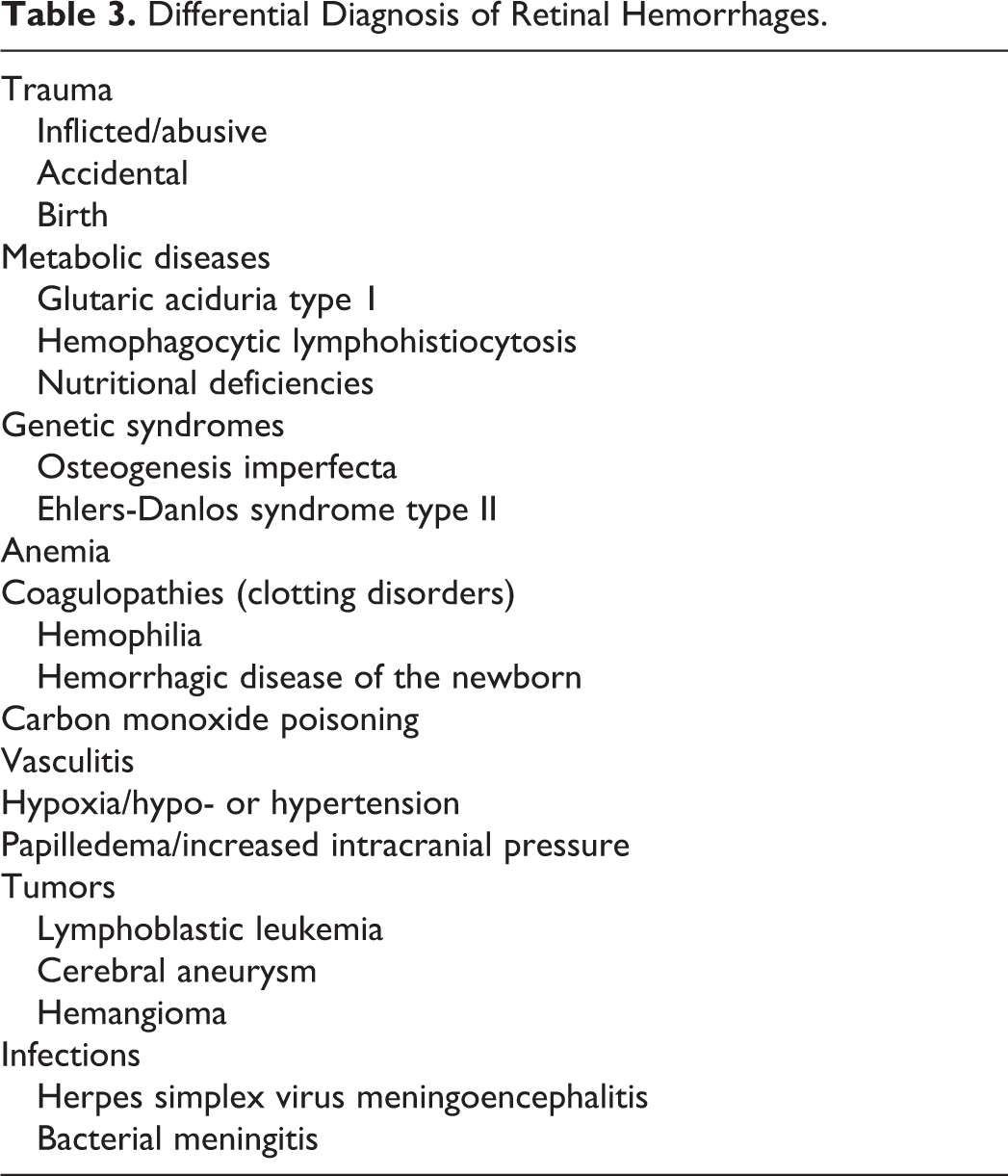
The most common findings, however, are subdural hemorrhages and retinal hemorrhages. Subdural hemorrhages have been reported in 77% to 90% of patients with abusive head trauma, and retinal hemorrhages have been described in approximately 74% to 82% of abusive head trauma cases. 20 Although subdural and retinal hemorrhages are the more common features of abusive head trauma, they have an extensive differential diagnosis (see Tables 2 and 3). Radiographically, certain characteristics of subdural hemorrhages demonstrate a greater association with abusive head trauma. In their systematic review of neuroradiologic features in abusive and nonabusive head trauma, Kemp et al 30 reported that multiple subdural hemorrhages and subdural hemorrhages in certain locations (ie, within the interhemispheric fissure or over the convexities) were significantly statistically associated with abusive head trauma.
Differential Diagnosis of Subdural Hemorrhages.
Differential Diagnosis of Retinal Hemorrhages.
It is important for the clinician to understand that not all retinal hemorrhages are the same. Hemorrhages can occur on the surface of the retina (preretinal), under the retina (subretinal), or within the retinal layers (intraretinal). Hemorrhages can have a certain appearance and size (eg, “flame,” “splinter,” or “dot-blot”) and can be confined to the posterior pole or extend to the ora serrata (the edges of the retina). 31 Mild retinal hemorrhages are generally understood to be a few, dot/blot or flame/splinter-shaped, in the intraretinal or preretinal layers, and confined to the posterior pole (see Figure 1).
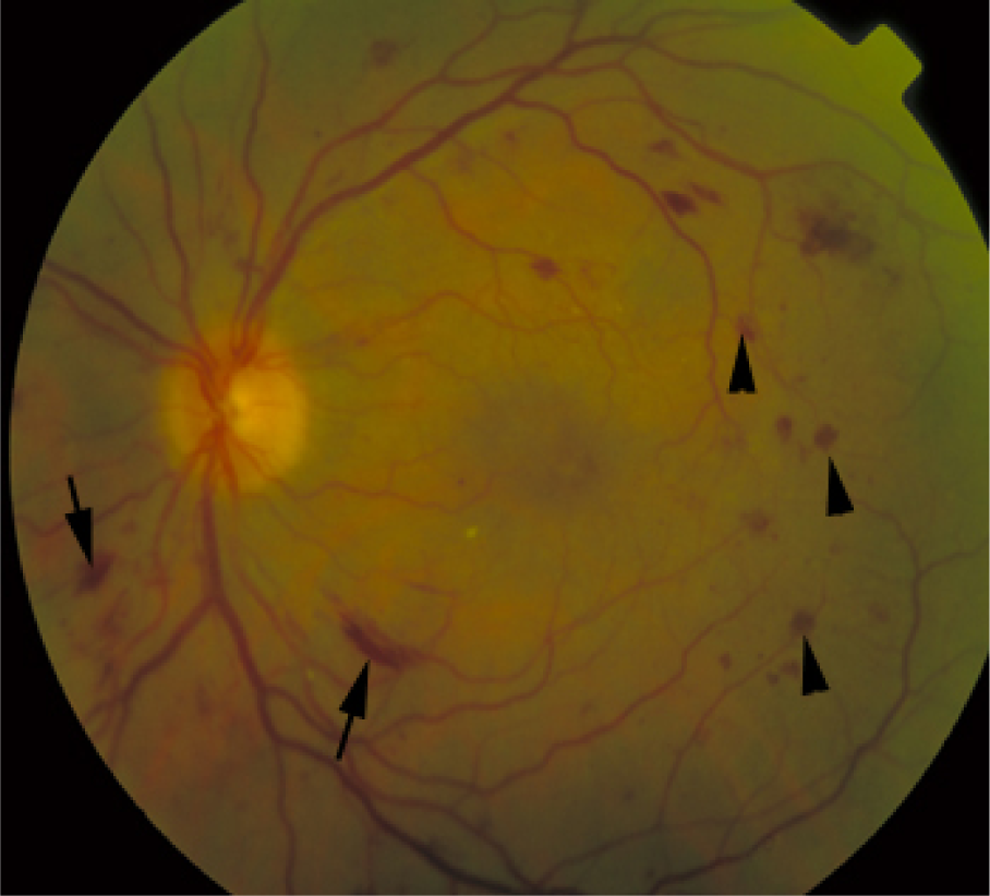
Mild nonspecific retinal hemorrhage confined to the posterior pole. Arrows show superficial flame hemorrhages. Arrowheads indicate dot/blot intraretinal hemorrhage.
Severe retinal hemorrhages are generally understood to be diffuse, too numerous to count hemorrhages, extending to the periphery of the retina (not confined to the posterior pole), usually involving multiple layers of the retina (intraretinal, preretinal, or subretinal), and sometimes accompanied by retinoschisis with or without folds (see Figures 2 and 3). 32 Given the importance of the description of the retinal hemorrhages, clinicians are exploring the development of a standardized tool for reporting ophthalmic findings. 33
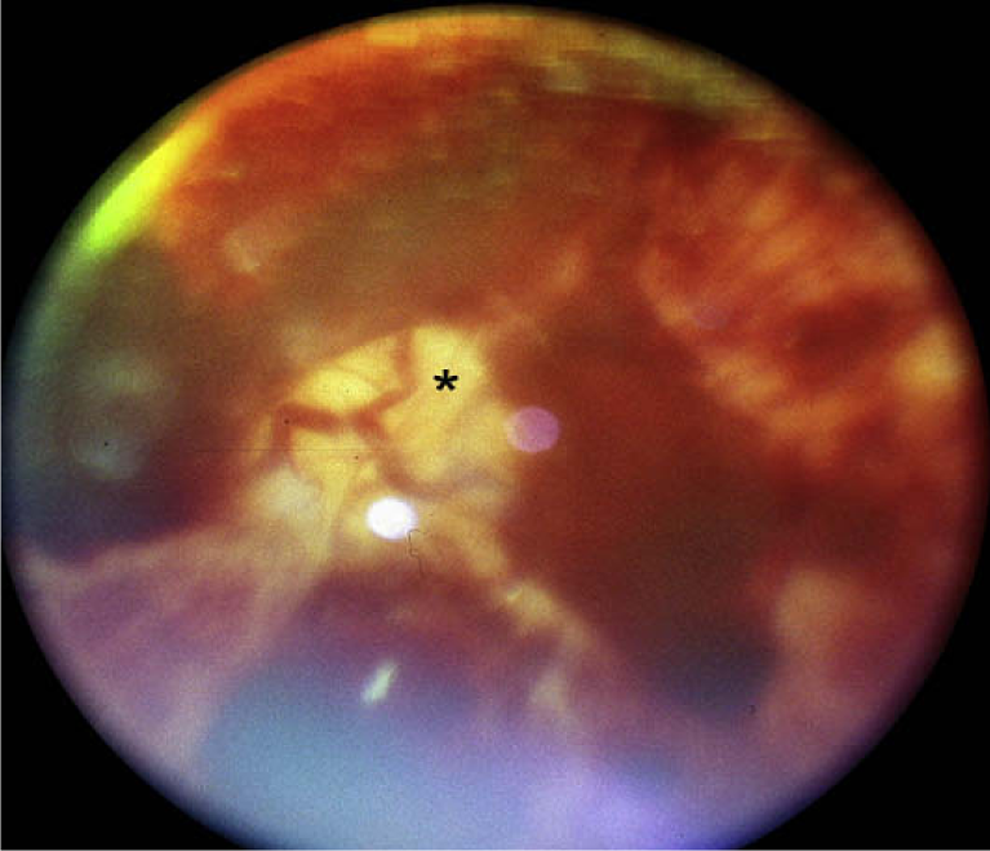
Severe retinal hemorrhages, too numerous to count, surrounding the optic nerve (*). Virtually no normal retina is visible due to the severity of the hemorrhages.
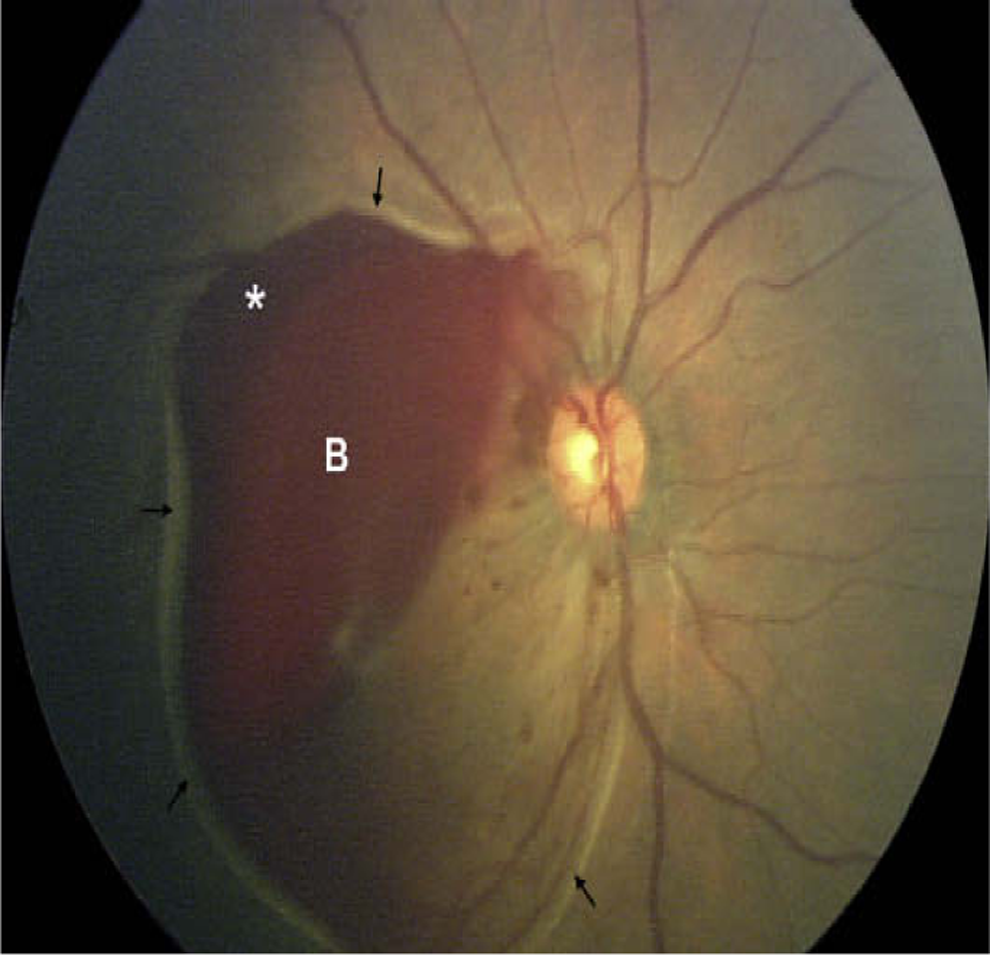
Macular traumatic retinoschisis. Blood (B) within the schisis cavity. Arrows indicate surrounding hypopigmented (pale appearance) retinal fold at the edge of the schisis cavity.
Although advances in our understanding have educated us that retinal hemorrhages are not pathognomonic for abusive head trauma, severe hemorrhagic retinopathy does hold high specificity and positive predictive value for abusive head injury. In a systematic review examining the characteristics of retinal findings that distinguish abusive from accidental trauma, Maguire et al 32 found that retinal hemorrhages were “rare in accidental trauma and, when present, are predominantly unilateral, few in number and in the posterior pole.” The authors went on to conclude that “certain patterns of RH [retinal hemorrhages] were far commoner in AHT [abusive head trauma], namely large numbers of RH in both the eyes, present in all layers of the retina, and extension into the periphery.” Similar results were reported by Vinchon et al 34 in their comparative study of witnessed accidents and confessed abuse cases (see Figure 4 below).
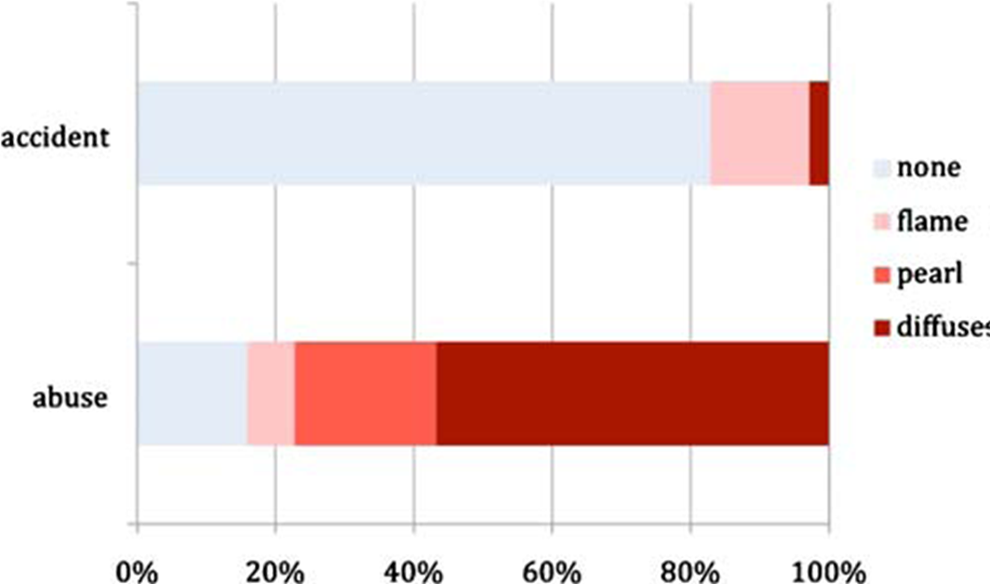
Retinal hemorrhage in the accidental trauma and inflicted head injury groups. Although most cases of abuse were associated with severe hemorrhage, 7 had no hemorrhage, and 3 had only mild hemorrhages. Conversely, no or mild retinal hemorrhages were found in 34 cases of accidental trauma, and only 1 had severe hemorrhage caused by direct facial impact.
Cervical spine injury has been an underreported and underappreciated clinical aspect of abusive head trauma. However, it is an area that has generated increasing clinical and radiographic interest in recent years. Initial studies indicated low detection rates of c-spine injury in children with abusive head trauma. 35 But more recent case series have found increased detection of cervical spine injuries in up to 44% of children with confirmed inflicted trauma. 36 Most commonly, cervical spine injury radiographic manifestations include ligamentous injury, spinal extra-axial hemorrhage, and vertebral body subluxations or fractures. 37 Less common, but still described, manifestations include spinal cord injury and spinal cord injury without radiologic abnormality. 38 Currently, dedicated c-spine computed tomography (CT) or magnetic resonance magnetic resonance imaging (MRI) is not a routine part of the abusive head trauma evaluation. 39 Although larger-scale studies are needed to determine the utility of c-spine CT or MRI as a routine course in abusive head trauma evaluations, physicians should consider those modalities in cases where historical or clinical signs and symptoms warrant further investigation.
Laboratory evaluation in suspected abusive head trauma is variable and injury specific. Initial laboratory evaluation should include a comprehensive metabolic panel, a complete blood count, and a basic coagulation panel (prothrombin time and partial thromboplastin time). Additional bleeding studies (such as platelet function tests, fibrinogen levels, D-dimer, specific factor levels, or von Willebrand factor panels) may be ordered, in consultation with a pediatric hematologist, especially if the initial screen is abnormal. Physicians should remember that patients who suffer a traumatic brain injury can have a transient coagulopathy that does not reflect an underlying congenital disorder. Additional metabolic (serum amino acids, urine organic acids, and serum acylcarnitine profile) and bone health (phosphorous, intact parathyroid hormone, and vitamin D 25-OH levels) studies may also be ordered, in consultation with a child abuse pediatrician, in the presence of particular injuries. Dilated indirect ophthalmoscopy by a pediatric ophthalmologist is the method of choice for evaluating the retinas of children suspected of having suffered abusive head trauma.
Radiographic skeletal survey is the primary imaging modality in any child younger than 2 years with suspicious injuries. “Babygrams” or limited skeletal surveys are inadequate modalities for properly assessing suspected abuse. The American College of Radiology has provided specific, evidence-based guidelines for the skeletal and neuroradiologic evaluation of suspected abuse. 39 Despite advances in MRI, CT of the head remains the imaging modality of choice in the initial evaluation of pediatric head trauma. MRI is an important adjunct in the evaluation of abusive head trauma, often used to further clarify CT findings. CT and MRI can be useful in providing general age ranges of intracranial hemorrhages. 40 The absence of a validated model predicting the evolution of blood signal in head-injured infants and the differential mixing and settling of blood components are just a couple of reasons that precise dating of intracranial hemorrhage in infants should be avoided.
Arriving at the diagnosis of abusive head trauma is no different than arriving at any other clinical medical diagnosis: it starts with a detailed history and physical examination. For abuse cases, a particular emphasis is placed upon a detailed history of the events surrounding the presenting symptom(s), a trauma history, and a comprehensive psychosocial history. It is important to note that a trauma history often is missing in a child with abusive head trauma, or a minor trauma history is given (a fall from a sofa or bed, for example). Corroborating what common sense and clinical experience already mandate, Hettler and Greenes found that an absent or evolving trauma history had a 97% specificity and 92% positive predictive value for abusive head trauma. 41 Many of the potential disorders on the differential can be eliminated through a detailed history, physical examination, and initial laboratory and radiologic information. Ultimately, in the vast majority of cases, the common denominator for subdural and retinal hemorrhages will be trauma.
Differential Diagnosis
As mentioned above, an extensive list of medical conditions with features of intracranial hemorrhage and/or retinal hemorrhage can be confused with abusive head trauma. A review of all these conditions is beyond the scope of this article. The most common conditions that could present with findings concerning for abusive head trauma—accidental trauma, birth trauma, bleeding disorders, metabolic disease, and anatomic conditions—will be briefly discussed here. The vast majority of these conditions can be distinguished from child abuse with a detailed history, careful physical examination, and radiologic or laboratory studies.
Accidental Trauma
Children fall frequently, and falls are one of the most commonly offered explanations provided to explain a child’s serious head injury. In Fujiwara and colleagues’ review of 28 abusive head trauma cases and 232 nonabusive head injuries, fall was the history presented in at least 17.9% and 62.9% of the cases, respectively. 42 Authors in pediatric literature have defined short falls as heights varying from less than 15 feet, to 10 feet, to less than 1.5 meters (5 feet). Although there exists no standardized definition of a “short fall,” more recently consensus has shifted toward recognizing a “short fall” as a fall of less than 1.5 m (5 feet).
Serious and fatal injuries following accidental falls can occur, but very, very rarely, and usually involve complex falls involving stairs or infant walkers. 43,44 The knowledge base for such a conclusion stems from various well-conducted studies in various lines of research. Household falls most often result in no injury. Injuries that are seen are primarily focal, contact injuries such as a scalp laceration or contusion. 45 Witnessed falls in objective settings such as hospitals or day cares have rarely resulted in significant injury. 46 In 2010, the Centers for Disease Control and Prevention data on fatal injuries shows there were 37 fatal falls in a population of more than 20 million children ages 0 to 4 years—a rate of 0.18 per 100 000 children. 47 Furthermore, retinal hemorrhages, as a result of accidental falls, motor vehicle collisions, or other accidental trauma, are an uncommon occurrence and present as few in number, intraretinal, and located in the posterior pole of the retina. 48
Birth Trauma
Both subdural hemorrhages and retinal hemorrhages have been described as a result of the birth process. However, important differences exist between the hemorrhages observed in birth trauma and those associated with abusive head trauma. Intracranial hemorrhages from birth are usually asymptomatic, located in the posterior fossa, and resolve by 2 to 3 months of age. 49 Historical features associated with subdural hemorrhage from birth are those born prematurely, operative vaginal delivery, or with disorders of coagulation in mothers or babies. Retinal hemorrhages frequently occur from birth. A recent large series of 3573 infants by Li et al 50 found the incidence of retinal hemorrhage to be about 22% within 1 week of birth. Vacuum-assisted delivery is more likely to be associated with birth-related retinal hemorrhages. But the vast majority of birth-related retinal hemorrhages are intraretinal, located in the posterior pole, and resolve by 2 to 4 weeks of life. 51
Bleeding Disorders
Bleeding disorders may be congenital (inherent to the genetic makeup of an individual) or acquired. Several coagulopathies are of consideration in cases of abusive head trauma—von Willebrand disease, mild platelet disorders, vitamin K deficiency, and factor XIII deficiency. It is important for the clinician to remember that most bleeding disorders are rare; the more common bleeding disorders typically are mild; and intracranial hemorrhage resulting from bleeding disorders is a rare complication of the more severe diseases. 52 Furthermore, intracranial hemorrhage, as the initial presentation of an underlying coagulopathy, is an extremely rare event.
Of the major inherited bleeding disorders, von Willebrand disease is the most common congenital bleeding disorder. Current estimates indicate that low von Willebrand factor levels may occur in up to 1% of the US population. It most commonly presents with mild to moderate bleeding from the nose or mouth, bruising, or heavy bleeding during a woman’s menstrual period. It is generally classified in terms of von Willebrand factor levels and the type of functional defect affecting the von Willebrand factor protein. Type 1 disease results from an absolute decrease in the von Willebrand factor protein and is the most common. Type 3 is characterized by nearly absent levels of von Willebrand factor as well as low factor 8 and is the most severe version of von Willebrand disease. In nearly all cases where von Willebrand disease is mild, it often does not cause any symptoms until a hemostatic challenge, like the removal of teeth. Intracranial hemorrhage as the presenting finding of severe von Willebrand disease is extremely rare (upper limit of probability of 1 per 7.5 million people). 53
Mild congenital platelet disorders include Quebec platelet disorder, the MYH9-related disorders, Scott syndrome, Hermansky-Pudlak syndrome, Chediak-Higashi syndrome, and Wiskott-Aldrich syndrome. Most bleeding with these disorders is mild and manifests as excessive bruising or menorrhagia (heavy menstrual periods). The probability of mild platelet disorders causing intracranial hemorrhage is also unknown but is likely very low given the typical clinical manifestations.
Vitamin K is a fat-soluble vitamin necessary for synthesis of 4 clotting factors (II, VII, IX, and X), as well as the anticoagulation proteins C and S. Early onset vitamin K deficiency bleeding presents within 24 hours of birth and is usually seen in infants of mothers taking drugs that inhibit vitamin K such as anticonvulsants, antituberculosis drugs, and cephalosporins. Early-onset presentation is often with severe scalp, intracranial, and intra-abdominal hemorrhage. Classical vitamin K deficiency bleeding occurs between 24 hours and 7 days of life and typically involves gastrointestinal, umbilical, and circumcision site bleeding. 54 Late-onset vitamin K deficiency presents between 2 and 12 weeks and is associated with exclusive breast-feeding. Significant intracranial hemorrhage can be present, resulting in vomiting, bulging fontanelles, and seizures. 55 Retinal hemorrhages are rarely reported as a clinical finding in infants with vitamin K deficiency bleeding, but there have been reports nevertheless. 56
Factor XIII deficiency, a rare autosomal recessive coagulopathy, is the last enzyme in the coagulation/thrombosis cascade and is essential in forming and stabilizing clots by cross-linking fibrin and preventing degradation of the fibrin clot. The most common and classic presentation of factor XIII deficiency is delayed or prolonged umbilical cord bleeding. Other presentations include soft tissue bruising, intramuscular hemorrhage, and rarely, intracranial hemorrhage. 57 Importantly, routine coagulation studies such as prothrombin time, activated partial thromboplastin time, and platelet function tests are normal in congenital factor XIII deficiency. Specific factor XIII assays must be used to identify factor XIII deficiency.
Metabolic Diseases
Two metabolic diseases, glutaric aciduria type I and Menkes disease, are of particular consideration in cases of suspected child abuse. Glutaric aciduria type I is caused by a deficiency of glutaryl-CoA dehydrogenase, an enzyme involved in the metabolism of amino acids lysine, hydroxylysine, and tryptophan. The enzyme deficiency eventually results in severe dystonia caused by basal ganglia neuronal loss. Initial clinical manifestations, however, can be very subtle and nonspecific, presenting as hypotonia, feeding difficulties, irritability, and an enlarging head circumference. The undiagnosed, untreated infant can then present with encephalopathy triggered by, or in conjunction with, a mild illness.
Glutaric aciduria type 1 can be associated with acute subdural hemorrhage, chronic subdural collections, and retinal hemorrhages and can be mistaken for abusive head trauma. 58,59 However, glutaric aciduria does not predispose patients to fractures. Neuroimaging features can include frontotemporal atrophy, subdural fluid collections, and characteristic widened sylvian fissures. 60 All states in the United States presently include glutaric aciduria type 1 on the routine newborn screen. Urine organic acid analysis is diagnostic with increased 3-hydroxyglutaric acid and/or increased glutaric acid. If urine organic acids do not confirm the diagnosis and clinical suspicion remains high, other testing such as enzyme assays and molecular analysis of the glutaryl-CoA dehydrogenase gene can be performed.
Menkes disease, also known as Menkes kinky hair syndrome, is an X-linked recessive neurodegenerative disorder caused by a mutation in the copper transport gene, causing copper deficiency, decreasing the activity of copper-dependent enzymes. Typical clinical features include early, severe neurologic deterioration, characteristic thin, brittle, and hypopigmented hair that twists upon itself, and connective tissue disorders. Menkes disease can be confirmed with a low serum ceruloplasmin level. Other findings described in Menkes disease are subdural hemorrhage and metaphyseal changes mimicking classic metaphyseal lesions. Retinal hemorrhages, however, are not a commonly described feature of Menkes disease. 61
Benign Extra-axial Fluid of Infancy/Benign External Hydrocephalus
Infants with an isolated large or rapidly increasing head circumference may be referred to pediatric neurologists for evaluation. Benign extra-axial fluid of infancy/benign external hydrocephalus is a self-limiting condition commonly defined as a large or rapidly growing head circumference in infants, combined with enlarged subarachnoid spaces and no or only moderate ventricular enlargement. 62 Additionally, there is an absence of clinicoradiologic features of increased intracranial pressure. The most common pathophysiological theory for this disorder is that immature arachnoid villi are not able to absorb the cerebrospinal fluid that is produced continuously. Other reported symptoms of this condition include developmental delay, hypotonia, irritability, and seizures. An increased risk of subdural hemorrhage with minor trauma may exist in these children. 63 The enlarged frontal spaces can be confused for chronic subdural hematomas, particularly on CT imaging, but should be readily distinguishable on MRI.
Although benign external hydrocephalus is a consideration in certain cases of suspected abuse, there are features that distinguish this disorder from many cases of abuse. First, unlike many cases of abuse (as will be discussed further below), this is a benign, self-limited condition that spontaneously resolves in early childhood. Second, there have been no literature reports of an associated finding of severe hemorrhagic retinopathy. Finally, there have been no reports of fractures associated with this disorder.
Special Considerations for Child Neurologists
Because seizures are a frequent finding associated with head trauma, child neurologists are often asked whether seizures cause subdural and/or retinal hemorrhages. Seizure activity, in-and-of itself, has not been reported to cause subdural hemorrhages. However, seizures that may result in falls or other trauma have the potential to result in subdural hemorrhages, as a consequence of the related trauma. Curcoy et al 64 prospectively studied the incidence of retinal hemorrhages in children under the age of 2 who were admitted to their institution with “first convulsions.” Of 189 children examined with direct ophthalmoscopy by an ophthalmologist, none were found to have retinal hemorrhages. Similar findings have been reported by Mei-Zahav et al 65 and Sandramouli et al. 66 Thus, to date, no well-designed study has found retinal hemorrhages, especially severe retinal hemorrhages, to have been associated with seizures.
Another consideration recently raised in legal circles is the theory of hypoxia-related subdural hemorrhages. In summary, multiple lines of research (eg, research in drowning victims, 67 research in cardiopulmonary resuscitation victims 68 ) have failed to identify an association of subdural hemorrhages with hypoxic injury. When observed, the intracranial hemorrhage presentation most consistent with hypoxic-ischemic injury is intraparenchymal hemorrhage. Finally, multiple studies have conclusively demonstrated that hypoxia is not a putative factor in causing severe retinal hemorrhages. 69 Additionally, other proffered theories, such as coughing (pertussis), 70 vaccinations, or increased abdominal pressure from vomiting 71 have been studied and have also failed to demonstrate either the subdural or severe retinal hemorrhages commonly seen in abusive head trauma.
Management and Outcomes
Infants and young children with abusive head injury are generally treated in the pediatric intensive care unit for airway stabilization, ventilator support, and management of intracranial pressure to mitigate secondary insults from hypoxia, mass effect, cerebral edema, and seizures. Seizures are common and early posttraumatic seizure prophylaxis is recommended. Surgical strategies to decrease intracranial pressure include decompressive craniectomy, subduroperitoneal shunt, or subduroexternal drainage.
Well-designed comparative studies have demonstrated a statistically significant worse outcome (for both physical and cognitive functioning) for abusive head trauma patients over accidental trauma patients. Morbidity and mortality rates for abusive head trauma are extraordinarily high. Approximately 15% to 23% of all recognized cases of abusive head trauma die before or shortly after presentation for medical care. 20 In a Swiss Abusive head trauma follow up study, Fanconi and Lips documented that only 36% of Abusive head trauma patients had a “good outcome,” and 64% were either moderately or severely disabled. 72 Similar results were reported by Duhaime et al. 73
Future Research
Within the last 2 decades, tremendous strides have been made in abusive head trauma research. In the realm of biomechanics, improvements in the biofidelity of anthropomorphic test devices have refined biomechanical data on head and neck injury in infants. Finite element modeling has been utilized to investigate parameters of physical forces surrounding fractures. 74 Although biomechanical research has yet to provide a definitive answer to several biomechanical questions surrounding abusive head trauma (such as whether shaking can or cannot cause subdural hemorrhages, and whether neck injury is necessary in cases of violent shaking), the biomechanical literature, in spite of its flaws, is useful and informative. Additionally, exciting research has emerged into the use of serum or cerebral spinal fluid biomarkers to aid in the diagnosis of abusive head trauma. Over the past decade or so, biomarkers, such as neuron-specific enolase and myelin basic protein, were identified by Berger et al 75 to be potentially useful as screening tools to identify brain injury in infants with nonspecific symptoms. Currently, large prospective case-control studies are continuing to investigate the utility of specific biomarkers in diagnosing, monitoring or prognosticating patients with traumatic brain injury or other pediatric neurocritical care conditions. 76 Finally, large, multicenter collaboratives, such as the Pediatric Brain Injury Research Network (PediBIRN) and Examining Siblings to Recognize Abuse (ExSTRA), have been created with the aim of conducting rigorous, evidence-based clinical research on various aspects of pediatric trauma.
Conclusion
Abusive head trauma remains a common pediatric diagnosis. Unfortunately, for various reasons, physicians continue to underrecognize and underdiagnose it. The proper diagnosis of this complex disease requires clinicians to maintain a high index of suspicion, to utilize a multidisciplinary team approach, and to rigorously exclude other etiologies on the differential. Certain symptoms and findings, such as apnea and severe retinal hemorrhages, hold a high specificity and positive predictive value for abusive head trauma. When confronted with these findings in light of an inadequate, evolving or absent trauma history, physicians can diagnose abusive head trauma with a high degree of confidence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.