
Abstract
Posttraumatic headache is one of the most common and disabling symptoms after traumatic brain injury. However, evidence for treating posttraumatic headache is sparse, especially in the pediatric literature. This retrospective chart review evaluated the use of occipital nerve blocks in adolescents treated for posttraumatic headache following mild traumatic brain injury, presenting to the Complex Concussion and Traumatic Brain Injury clinic. Fifteen patients (mean age 15.47; range: 13-17) received occipital nerve block for posttraumatic headache. Follow-up was obtained in 14 patients at 5.57 (standard deviation = 3.52) months postinjury. The headache burden was high, with all except one having headaches 15 or more days per month (median 30, range 10-30). Sixty-four percent reported long-term response to the occipital nerve blocks, with associated improved quality of life and decreased postconcussion symptom scores (P < .05). One patient reported transient allopecia. Occipital nerve blocks are well tolerated and can be helpful in posttraumatic headache.
Mild traumatic brain injury is a common and disabling occurrence, with children and adolescents being the highest risk age group. 1 Epidemiologic studies have highlighted the frequency of these injuries: the reported yearly incidence of traumatic brain injury in the pediatric age group is between 0.1% and 1.75%, with 55% to 95% of these injuries categorized as mild traumatic brain injury.2 –6 Traumatic brain injury causes significant lasting disability among children and adolescents, 7 with one study reporting a 4% to 10% rate of new disability 12 months postinjury in mild traumatic brain injury patients. 8
Postconcussion syndrome is a constellation of symptoms that persist after the initial mild traumatic brain injury. Symptoms fall into four categories: somatic (dizziness, headache, nausea, photophobia, phonophobia), cognitive (impaired memory, impaired concentration), behavioral (depression, irritability), as well as sleep-related disturbances. Studies in the pediatric age group have found that 9% to 35% of children with mild traumatic brain injury had symptoms of postconcussion syndrome 3 months after the initial injury.9 –11
Posttraumatic headaches are a common feature of postconcussion syndrome and can also occur in isolation after mild traumatic brain injury. The International Classification of Headache Disorders, 3rd edition (ICHD-III), classifies posttraumatic headaches according to time course and mechanism of injury. 12 Criteria for persistent headache attributed to traumatic injury to the head require the onset of the headaches to be within 7 days of the initial injury. The headache disorder is acute if it resolves within 3 months and chronic if it persists beyond 3 months. 12 A recent pediatric cohort study at our institution found that 7.8% of children with mild traumatic brain injury go on to develop posttraumatic headaches 3 months postinjury, 13 with a similar cohort in another study of mostly mild traumatic brain injury participants developing chronic posttraumatic headaches in 6.8% of subjects. When compared to children with arm fractures, mild traumatic brain injury was associated with a higher risk of headache for more than 3 months postinjury (relative risk = 1.7, 95% confidence interval = 1.2-2.3) when controlling for age, gender, race, insurance, and parental education. 14
Despite the relatively common and disabling nature of posttraumatic headaches, there is little evidence to guide clinicians in their management, especially in children. Our recent case series found that 64% of children with posttraumatic headaches do respond to therapies commonly used when treating pediatric headache disorders. 13 Occipital nerve blocks are used to treat occipital neuralgia, headaches associated with tenderness over the occipital nerves, occiput, and/or in the evaluation of cervicogenic headache. The aim of this study was to evaluate the use of occipital nerve blocks in adolescents treated for posttraumatic headaches following mild traumatic brain injury seen in a tertiary care brain injury clinic.
Methods
Study Design
A retrospective chart review of a case series consisting of occipital nerve block injection and follow-up.
Study Sample
Participants were identified from a sample of patients referred to the Complex Concussion and Traumatic Brain Injury clinic at the Alberta Children’s Hospital between 2011 and 2013. Any child, aged 6 to 18 years, with mild traumatic brain injury and posttraumatic headaches treated with occipital nerve block were included in the study. Occipital nerve block is routinely performed for occipital neuralgia, predominant occipital cephalgias with or without occipital tenderness, and/or in the evaluation of cervicogenic headaches. Some children with these criteria are not treated with occipital nerve block because of needle phobia or refusal of the procedure.
Occipital Nerve Block Procedure
Parent consent and participant assent was obtained. Under sterile technique, the participants were draped and the occipital area was sterilized with a chlorhexidine solution. The area of the greater occipital nerve was landmarked as 2 cm lateral from the external occipital protuberance and 2 cm inferior to that location, using palpation to determine the area of greatest point tenderness and subsequent point of injection. Later, 2.5 mL of 2% lidocaine (50 mg) was injected subcutaneously in the territory of the greater occipital nerves. Unilateral injections were used only in the setting of unilateral occipital neuralgia. The occipital area was then assessed for numbness to ensure blockade. Subsequently, 0.5 mL of methylprednisolone acetate (20 mg) or 2.5 mL of triamcinolone (25 mg) was injected into the same region. The routine standard follow-up is composed of a telephone follow-up at 2 to 4 weeks and a clinic appointment 2 to 3 months after the procedure. All participants were instructed to contact the clinic with any concerns.
Primary Outcome
“Full” response was defined as the percentage of participants with a 50% or greater reduction in headache frequency. A “partial” response was defined as significant improvement but less than a 50% reduction in headache frequency. Secondary outcome measures included a measure of postconcussion symptoms using the Rivermead Post-Concussion Symptoms Questionnaire (RPSQ) 14 and quality of life using the Pediatric Quality of Life Inventory, Version 4 (PedsQL). 15 These were collected at the time of injection and at the next clinic follow-up.
Statistical tests were performed in SPSS 19 (released 2010, IBM Corp, Armonk, NY) using a paired samples t test. This study obtained approval from the University of Calgary Conjoint Health Research Ethics Board.
Results
Fifteen participants (10 females, 5 males) received occipital nerve block for posttraumatic headaches. The mean age was 15.47 years (range: 13-17). All participants met criteria for posttraumatic headaches, 11 had chronic posttraumatic headaches, and 4 had subacute posttraumatic headaches. The characteristics of the headaches are shown in Table 1. Six participants met ICHD-III 12 criteria for occipital neuralgia, and 8 had mixed headache disorder. Eight participants had occipital tenderness, 3 had cervical pain, and 6 had migrainous features. Eight participants had repetitive mild traumatic brain injury ranging from 2 to 5 previous injuries. Daily headaches (30 days per month) occurred in 13 of the 15 participants, and cases 14 and 15 had 10 and 15 headache days per month, respectively. Initial occipital nerve blocks were performed 5.57 (± 3.5) months postinjury. Nine participants received a single treatment with occipital nerve block, 4 had a second occipital nerve block, and 1 received a total of 5 occipital nerve blocks.
Demographic, Injury, and Headache Data of Patients Receiving Occipital Nerve Block.a
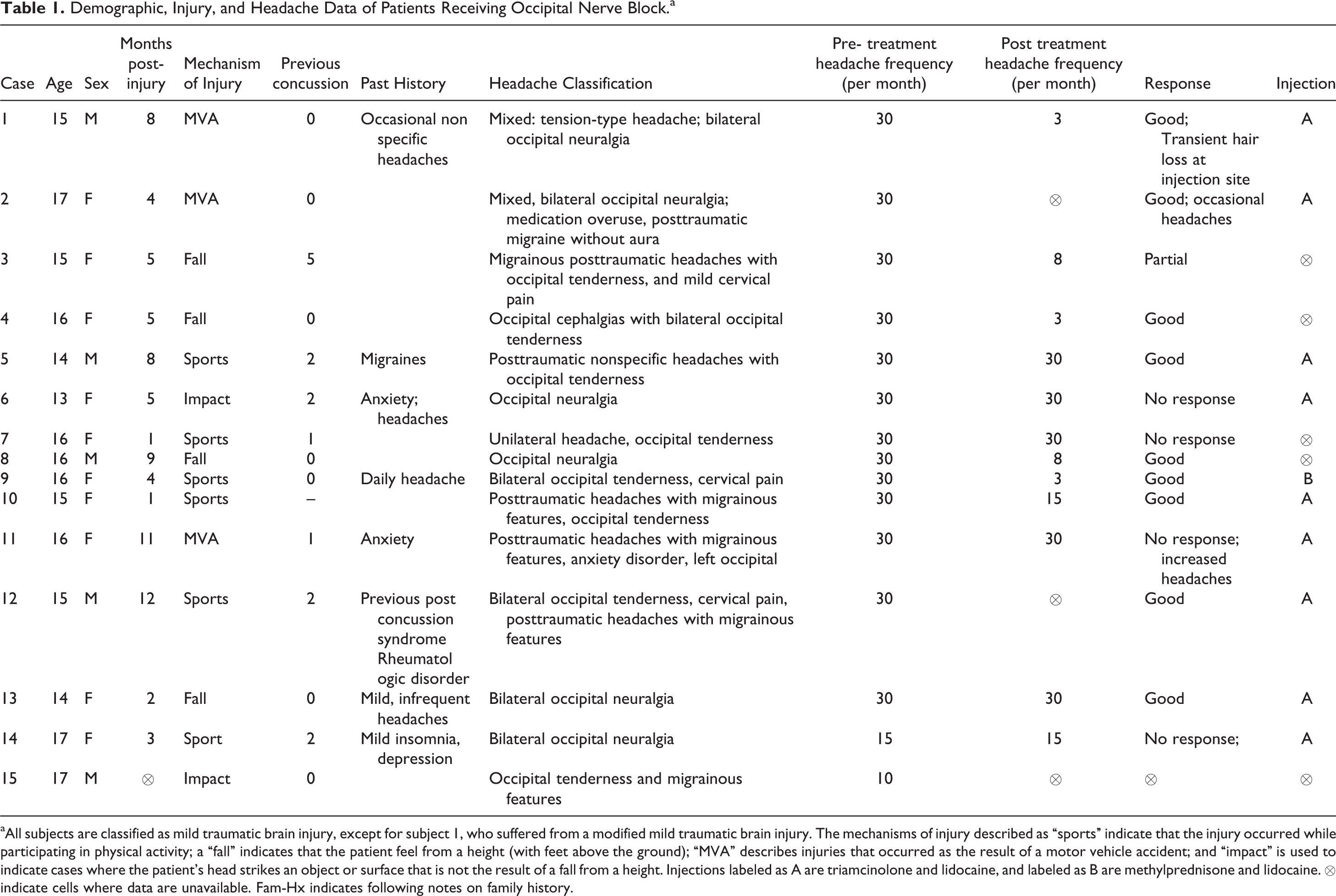
aAll subjects are classified as mild traumatic brain injury, except for subject 1, who suffered from a modified mild traumatic brain injury. The mechanisms of injury described as “sports” indicate that the injury occurred while participating in physical activity; a “fall” indicates that the patient feel from a height (with feet above the ground); “MVA” describes injuries that occurred as the result of a motor vehicle accident; and “impact” is used to indicate cases where the patient’s head strikes an object or surface that is not the result of a fall from a height. Injections labeled as A are triamcinolone and lidocaine, and labeled as B are methylprednisone and lidocaine. ⊗ indicate cells where data are unavailable. Fam-Hx indicates following notes on family history.
Outcome
Clinic follow-up was obtained on 14 participants at a mean of 5.57 months (±3.52) after the procedure. Nine participants had a full response to treatment, and 1 had a partial response. Four participants had no improvement in their posttraumatic headaches. Three nonresponders had occipital neuralgia and 1 had occipital cephalgias associated with occipital tenderness. Preinjection mean headache frequency was 26.25±7.11 days per month, and postinjection mean headache frequency was 17.50 ± 11.62, t(11) = 2.91, P = .014.
RPSQ scores pretreatment were 33.67 ± 13.47 (range: 20-57) and posttreatment were 24.33 ± 18.54 (range: 10-61); t(5) = 3.04, P = .029. The mean improvement on the RPCSQ with treatment was 9.33 ± 7.53. This was associated with an improvement in the PedsQL scores from 52.04 ± 21.36 (range: 37.24-66.84) to 68.75 ± 27.50 (range: 49.69-87.81), t(7) = –2.62, P = .035.
Adverse effects
The procedure was well tolerated in all cases. A small area of alopecia 1.5 × 1.5 cm developed in 1 participant treated with 2% lidocaine and triamcinolone. This resolved completely over 6 months.
Discussion
Between 7.8% and 43% of children with traumatic brain injury develop frequent headaches after traumatic brain injury. 16 Despite this high prevalence, evidence is lacking regarding the treatment of these patients, especially in the pediatric literature. Observational studies in adults have reported some improvement in posttraumatic headaches with a variety of pharmacologic agents (including amitriptyline, 17 botulinum toxin, 18 intravenous chlorpromazine, 19 intravenous dihydroergotamine with metoclopramide, 20 divalproex, 21 topical ketoprofen, 22 propranolol, 18 and subcutaneous sumatriptan 23 ). Indomethacin has been used successfully in adult patients who meet criteria for posttraumatic hemicrania continua 24 and chronic paroxysmal hemicrania. 25
Targeted injections have been used with success in a variety of headache disorders in adults, including the trigeminal autonomic cephalalgias, 26 occipital neuralgia, 27 –29 trigeminal neuralgia, 27 cervicogenic headache,28,30,31 and migraine.30,32,33 The response of posttraumatic headaches in adults to occipital nerve block is variable.23,34 –36 In a retrospective review, 63 of 87 adult patients with post-traumatic headaches had significant improvement in their headaches up to six months after occipital nerve block with xylocaine and methylprednisolone. 23 In contrast, another small case series of 11 patients reported only brief relief of posttraumatic headaches associated with occipital tenderness when treated with occipital nerve block: although 91% of the participants had a response in the first week, only 9% sustained that response beyond 1 week. 34
This study adds significantly to the small body of existing literature regarding the treatment of posttraumatic headaches. One recent case series supports our finding that occipital nerve block is a worthwhile consideration in the management of posttraumatic headaches in children. Dubrovsky et al performed a retrospective chart review of 28 children with posttraumatic headaches associated with tenderness over the greater occipital nerve and examined the response to scalp injections (using 2% lidocaine with epinephrine). Following occipital and supraorbital nerve block, 26% of 28 patients had some headache relief for 24 hours or more postinjection or requested an additional injection. Improvement or resolution of headaches was sustained in the “weeks” following the injection in 61% of patients. 37
We found that 64% of children with posttraumatic headaches associated with occipital tenderness or neuralgia who had been symptomatic for almost 6 months following their injury responded favorably to the injections. This was associated with improvement in the severity of postconcussion symptoms and quality of life. Most of these children were experiencing headache every day before treatment with a marked reduction in the frequency of these headaches posttreatment. It is highly unlikely that this is due to the natural history of the headache disorder, especially in those with chronic posttraumatic headaches.9,13 Further, the ONB procedure was well tolerated, with only 1 patient reporting a mild adverse event.
This study has several limitations. It is susceptible to bias due to the retrospective design, small size, and the lack of a control group. The indications, procedures, and use of standard outcome measures are routinely collected prospectively in the Complex Concussion and Traumatic Brain Injury Clinic. Although a headache diary would have helped to decrease recall bias, it is standard practice for patients to prospectively monitor their PCS symptoms using a PCS symptom questionnaire. The placebo effect here could be considerable, as it is significant in headache disorders, especially in the pediatric population. 38 Further, it is higher in studies using injections for headache therapy. 39 The use of 2 different types of steroids is unlikely to have significantly affected the results. 40 Lastly, the results of this study cannot be generalized to all children with posttraumatic headaches as this procedure is currently performed for posttraumatic headaches in the presence of occipital neuralgia, occipital tenderness, and/or neck pain.
In summary, occipital nerve block can be an effective treatment for posttraumatic headaches in children when associated with occipital tenderness. Future well-designed trials to evaluate the use of occipital nerve blocks in posttraumatic headache disorders with and without occipital or neck tenderness in children are warranted.
Footnotes
Acknowledgments
Alberta Children’s Hospital Foundation
Author Contribution
All authors contributed to data collection and manuscript preparation. TAS, SO, and KMB analyzed the data. SO performed literature review. KMB was the principal investigator who designed the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the University of Calgary Research Ethics Board; REB number-24168.