
Abstract
Disease burden associated with tuberous sclerosis complex, a genetic disorder characterized by benign tumor growth including lesions in multiple organs, puts tremendous demands on families. This analysis examines the physical and mental health burden of tuberous sclerosis complex caregivers in the United States. An institutional review board–approved web-based survey of tuberous sclerosis complex caregivers collected information; descriptive analyses were conducted on age-based subgroups. A total of 275 caregivers of tuberous sclerosis complex patients responded. Mean patient age ≤18 years was 6.9 (±4.4) and 42.3 (±18.2) for patients >18 years of age. Caregivers reported multiple tuberous sclerosis complex manifestations and high health care utilization for patients. Caregivers spending more time on doctor visits or researching tuberous sclerosis complex had lower physical and mental health–related quality of life scores and more depressive symptoms. Tuberous sclerosis complex caregivers had significantly lower physical and mental health–related quality of life scores and more depressive symptomatology compared to US healthy adult population norms.
Keywords
Background
Tuberous sclerosis complex is a rare genetic disorder characterized by benign tumors in multiple organs. It is projected that nearly 1 million people worldwide are known to have tuberous sclerosis complex, of whom approximately 30 000 to 50 000 are in the United States. 1 -3 Diagnosis of tuberous sclerosis complex is defined by a constellation of features, and an individual is considered to have a definite diagnosis of tuberous sclerosis complex only if he or she has 2 major features of the disorder or 1 major and 2 minor features. 4 Tuberous sclerosis complex causes neurologic manifestations that include cognitive disability, 5 subependymal giant-cell astrocytoma, autism spectrum disorder, 6 behavioral problems, 7 sleep problems, 8 and severe and early-onset epilepsy, with approximately 70% to 80% of tuberous sclerosis complex patients suffering from epilepsy. 9 The complex needs of the condition signifies that nearly all tuberous sclerosis complex patients require long-term care from a caregiver.
Because of the long-term intensive nature of the condition, the majority of caring for tuberous sclerosis complex patients comes from close family members, normally the patient’s parents or siblings. Over the last few decades, there has been a considerable amount of research investigating caregiver burden in chronic conditions and illnesses. A recent study 7 investigated stress that parents of children with tuberous sclerosis complex experience. The study reported that almost half of the parents suffered from clinically significant stress levels. This stress was associated with the cognitive function of the child, frequency of epileptic seizures, and behavioral problems related to autism spectrum disorder. Caregiver burden has been shown to contribute to unmet needs in the tuberous sclerosis complex patient. 10
Rarely has this topic been addressed in prior publications. The objective of this study is to investigate well-being burden of caregivers of tuberous sclerosis complex patients in the United States. This analysis can contribute significantly to providing information about the health-related quality of life burden on caregivers of tuberous sclerosis complex patients.
Methods
Study Design
This cross-sectional, nonintervention, web-based survey study involved caregivers of persons diagnosed with tuberous sclerosis complex in the United States. Data were collected in May and June 2012. The survey and recruitment methodology were developed by the authors of this manuscript and approved by the Ethical & Independent Review Services institutional review board (Independence, MO). Survey responses were anonymous, and all participants provided online consent prior to completing the survey. Survey completion time was typically between 45 and 60 minutes. To acknowledge their effort, survey completers were eligible to receive a $25 Amazon.com gift link, or donate the $25 to either the Tuberous Sclerosis Alliance or National Organization for Rare Disorders.
Study Sample
Caregivers of persons living with tuberous sclerosis complex (ie, “tuberous sclerosis complex patients”) were recruited via e-mail and social networking web sites associated with the TS Alliance, a US-based patient advocacy organization. Eligible caregivers had to be 18 years or older, care for someone diagnosed with tuberous sclerosis complex, able to read English and participate in a web-based survey, and able and willing to provide consent. Prospective survey participants were excluded if they reported cognitive impairment or other health impairment that would interfere with completing a tuberous sclerosis complex–related online survey. Caregivers not only provided proxy report for clinical and some demographic questions but also provided self-report for the outcome measures listed below.
Survey Components
The survey included questions to assess caregiver report of tuberous sclerosis complex patient disease manifestations, clinical treatment, health care utilization, and caregiver psychosocial status and quality of life. It was designed to be comprehensive enough to illustrate the burden of tuberous sclerosis complex. Types and diagnoses of tuberous sclerosis complex manifestations were collected. Survey respondents were asked, “Which TSC [tuberous sclerosis complex] manifestation bothers your TSC patient the most?” Medical care data were collected by asking caregivers to recall tests, procedures, and treatment such as medications, surgical procedures, doctor visits, hospitalizations, and emergency room visits. Standardized self-reported outcome measures included the Short Form Health Survey 12-item version 2 and the Hamilton Depression Inventory–Short Form.
The Short Form Health Survey 12-item version 2 11 is a widely used generic health status measure that assesses 8 aspects of health-related functioning over the past 4 weeks. The 8 health domains are Physical Functioning, Role-Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role-Emotional, and Mental Health. Responses to the 12 items on the questionnaire can be summarized in 2 summary scores: the Mental Component Summary and Physical Component Summary scores range from 0 to 100, with higher scores indicating better functioning. 11 The Short Form Health Survey has proven to be useful in comparing general and disease-specific study samples, comparing the relative burden of diseases, differentiating the health benefits produced by a wide range of different treatments, and screening individual patients. 12 -16
Depressive symptomatology was reported using the Hamilton Depression Inventory–Short Form, a 9-item measure capturing depressive symptoms over the last 2 weeks. 17 The possible range of scores is 0 to 33, with higher scores indicating more depression symptoms. Scores of greater than 8.5 are indicative of mild to severe depression. 18 The questionnaire was scored per accepted scoring algorithms. 17
Additional questions developed specifically for this study were included related to which manifestations were most bothersome for the patient and how tuberous sclerosis complex affects a patient’s personal life and decision making. For example, caregiver respondents were asked to rate their level of agreement with statements about how tuberous sclerosis complex affected educational attainment, social life, or sleep patterns of the person with tuberous sclerosis complex for whom they are caring.
Demographic characteristics of the respondent population, including age, gender, race, and insurance status, also was collected.
Statistical Analysis
Descriptive statistics (number of respondents, mean, standard deviation, frequency) were used to characterize the sample in terms of sociodemographic and clinical characteristics, disease experience, and health care resource utilization of patients for whom caregivers are caring. Age-based subgroup analyses were conducted with caregivers of tuberous sclerosis complex patients ≤18 (pediatric group) and >18 years of age (adult group). Clinical characteristics and health care utilization was compared between those receiving medical care in tuberous sclerosis complex specialty clinics compared to those receiving regular clinical care. Regression models examined the association between the time spent by caregivers on their patients’ tuberous sclerosis complex and caregiver well-being, controlling for age group of the tuberous sclerosis complex patient.
Student t tests were used to compare mean Hamilton Depression Inventory Short Form and Short Form Health Survey scores to established population norms. 11 Short Form Health Survey data were compared to normative data for persons living with depression (n = 254) using Student t test. Hamilton Depression Inventory mean scores were compared to normative data from healthy controls and individuals with anxiety disorder using Student t test. 17 All available data from the survey were used for the analysis; no data were imputed. P < .05 was considered statistically significant. All analyses were conducted using SAS, version 9.2.
Results
Sample Description and Sociodemographic Characteristics
Of 275 caregiver survey respondents, 78.9% were female, with a mean age of 39.0 (±10.4 standard deviation, range 20-82). The caregivers of the pediatric group represented 64% of the sample and had a mean age of 36.5 (±7.2 standard deviation, range 21-58) and cared for tuberous sclerosis complex patients with a mean age of 6.9 (± 4.4, range 0-18) years of age. Caregivers of the adult tuberous sclerosis complex patient group were 43.7 (± 13.3, range 20-82) years of age and were caring for a tuberous sclerosis complex adult with an average of age of 42.3 (±18.2, range 19-83) years. The majority of caregivers of adult tuberous sclerosis complex patients reported their tuberous sclerosis complex patient as semi-independent (52.5%) or dependent (37.4%). Overall, a small percentage (4.4%) of tuberous sclerosis complex caregivers reported caring for more than 1 tuberous sclerosis complex patient. The majority of the caregivers of adult patients (79.8%) and pediatric patients (89.8%) were white. The tuberous sclerosis complex pediatric group were covered by commercial health insurance (55.7%) or had commercial and Medicaid coverage (23.9%). The tuberous sclerosis complex adult group subjects were covered by Medicaid coverage (41.4%), commercial health insurance (15.2%), both Medicaid and Medicare (17.2%), or Medicare alone (17.2%).
The majority of caregivers had some college (24.0%), a college degree (45.1%), or a postgraduate degree (20.4%). A higher proportion of the caregivers of the pediatric group had a postgraduate degree compared to caregivers of adults (23.3% vs 15.2%). Most commonly, caregivers of tuberous sclerosis complex adults reported full-time employment (63%), retired status (10%), or being a homemaker (10%). Caregivers of the tuberous sclerosis complex pediatric group most commonly reported full-time employment (48%), being a homemaker (23.9%), part-time employment (12.5%), or being unemployed (10.2%). Caregiver and tuberous sclerosis complex patient demographic data are presented in Table 1.
Caregiver Demographics.
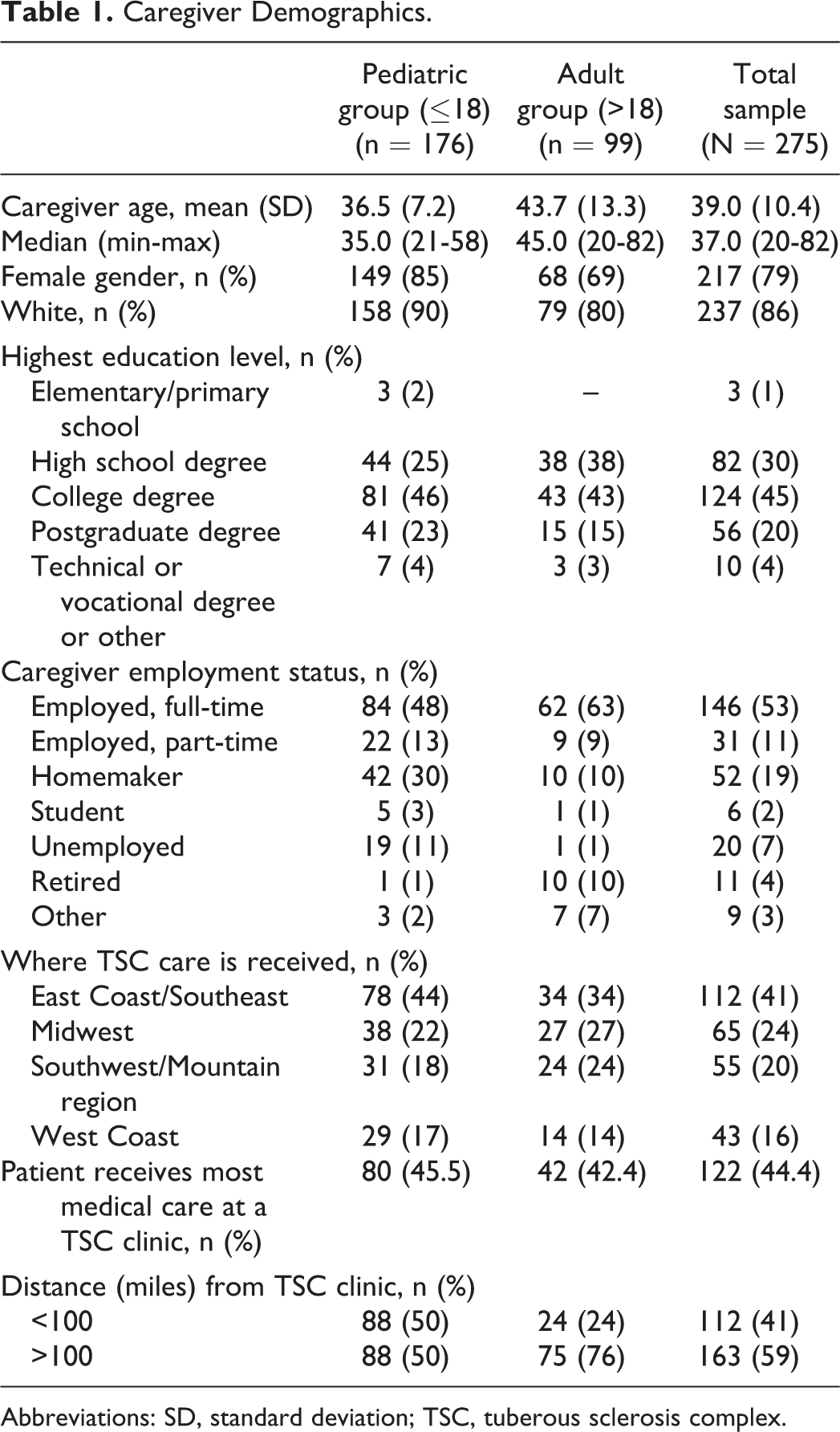
Abbreviations: SD, standard deviation; TSC, tuberous sclerosis complex.
Clinical Characteristics of Tuberous Sclerosis Complex Patient
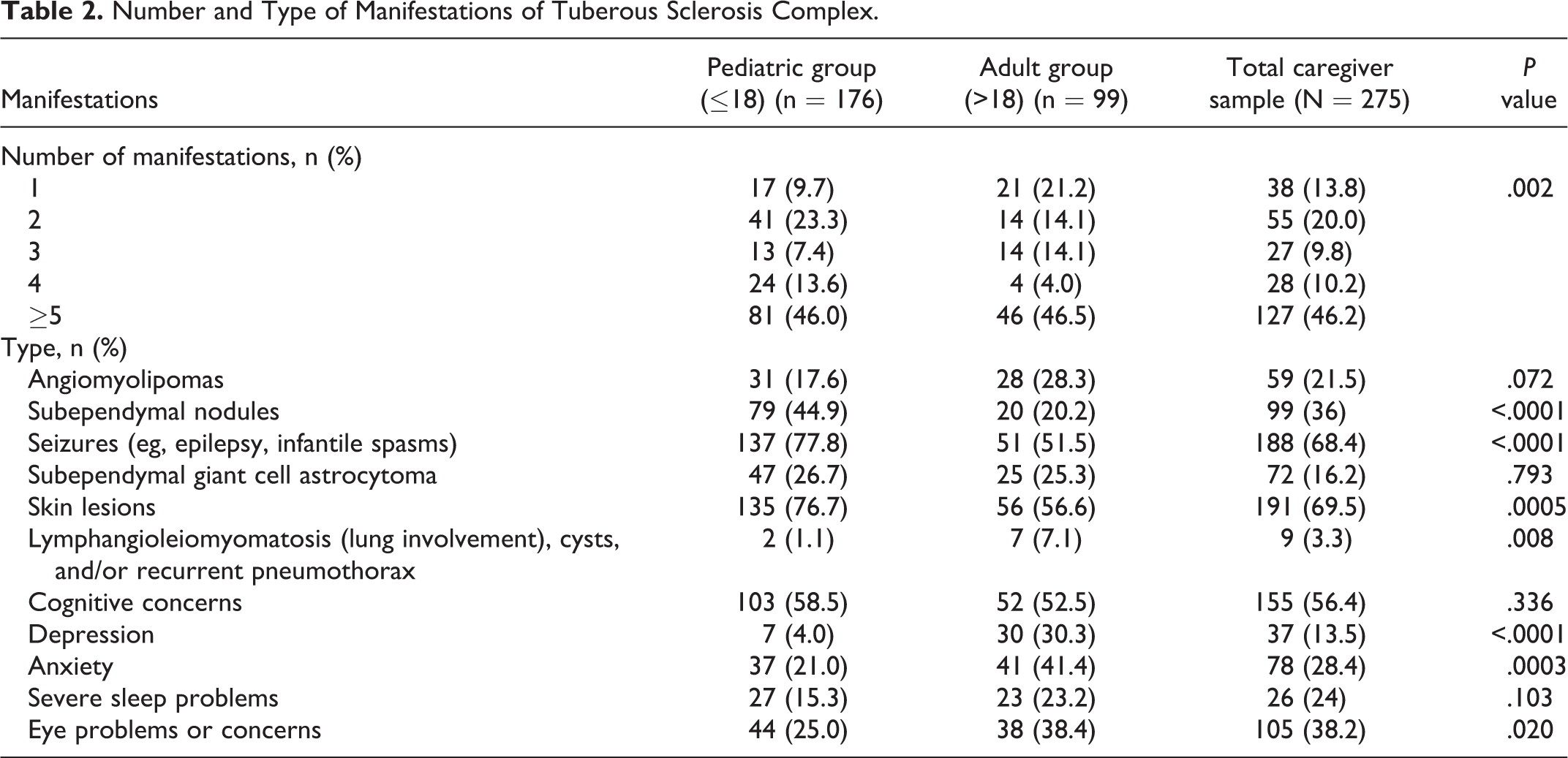
Of those pediatric patients not diagnosed in utero (93%), their caregivers reported that their tuberous sclerosis complex diagnosis was received at a mean age of 2.0 (±2.6 standard deviation, range 0-16) years, with 84% receiving a tuberous sclerosis complex diagnosis before 6 years of age, and 92.0% before the age of 13. Approximately 7% of the pediatric tuberous sclerosis complex pediatric group was diagnosed with tuberous sclerosis complex while in utero. Caregivers of the adult tuberous sclerosis complex group reported that the mean age of the tuberous sclerosis complex diagnosis for those not diagnosed in utero was 20.9 (±21.9 standard deviation, range 0-73) years, with 58% of tuberous sclerosis complex adults diagnosed before 18 years of age. Caregivers reported a significantly different number of manifestations between the pediatric and adult age groups (P = .002), with more pediatric patients compared to adults reporting 2 to 4 manifestations (44.3% vs 32.2%), but similar proportions of the tuberous sclerosis complex pediatric and adults patients having 5 or more tuberous sclerosis complex manifestations (46% vs 46.5%) (Table 2). The majority of tuberous sclerosis complex adults experienced skin lesions (56.6%), seizures (51.5%), and angiomyolipomas (28.3%). The tuberous sclerosis complex pediatric group most commonly experienced seizures (77.8%), skin lesions (76.7%), and subendymal tumors (44.9%). Caregivers also reported cognitive concerns in more than half of the pediatric (58.5%) and adult (52.5%) patient groups. Between the pediatric and adult groups, significant differences were reported in the percentage of subependymal nodules (44.9% vs 20.2%, P < .0001), seizures (77.8% vs 51.5%, P < .0001), skin lesions (76.6% vs 56.6%, P = .005), and lymphangioleiomyomatosis (1.1% vs 7.1%, P = .008). Likewise, significant differences were seen between pediatric and adult patients for depression (4.0% vs 30.3%, P < .0001), anxiety (21.0% vs 41.4%, P < .0003), and eye problems (25.0% vs 38.43%, P = .020). Table 2 describes the type of manifestations reported over the past year.
Number and Type of Manifestations of Tuberous Sclerosis Complex.
Resource Utilization of Tuberous Sclerosis Complex Patient
Nearly all of the caregivers reported that their adult patients (98%) or pediatric patients (98.9%) visited a physician in the past year. A slightly higher proportion of caregivers reported that their pediatric patients underwent procedures or tests compared to adult patients (97.7% and 90.9%). A similar median number of procedures or tests 6.0 (±8.0) and physician visits 16.0 (±19.0) per year were reported for both patient age groups. Likewise, a similar proportion of the pediatric and adult patients (37.5% vs 35.4%, respectively) were hospitalized in the past year.
Three-quarters of the adult group and 50% of the pediatric group reported living more than 100 miles from a tuberous sclerosis complex specialty clinic, and similar proportions of patients within the pediatric and adult age group (45.5% vs 42.4%) received most of their care from a tuberous sclerosis complex clinic. There was no consistent trend in differences between those who received most of their medical care at tuberous sclerosis complex clinics versus those who do not with regards to number and type of tuberous sclerosis complex manifestations, medical procedures, and health care utilization. However, in the pediatric group, a greater percentage of patients who received most of their medical care at tuberous sclerosis complex clinics had seizures (86% vs 71%, P = .015), and a smaller percentage reported skin lesions (67.5% vs 83.9%, P = .012) compared to those not receiving most of their medical care at tuberous sclerosis complex clinics. In the adult group, a greater percentage of patients receiving most of their medical care at tuberous sclerosis complex clinics reported lymphangioleiomyomatosis (14.3% vs 1.9%, P = .038), and a smaller percentage reported cognitive concerns (42.9% vs 64.2%, P = .022). Pediatric age patients who received most of their medical care at tuberous sclerosis complex clinics had more emergency room visits in the past year (41.3% vs 21.5%, P = .005) compared to pediatric patients who do not receive care at tuberous sclerosis complex clinics. Adult patients who received most of their medical care at tuberous sclerosis complex clinics reported more physician visits (mean 31.9 ± 33.1 vs 19.4 ± 17.4, P = .021) and more procedures or tests (12.4 ± 11.9 vs 7.8 ± 7.0, P = .024) in the past year compared to adults not receiving most of their medical care in a tuberous sclerosis complex clinic.
Caregivers of the pediatric group spent a median of 15.0 (±29.0) hours over the past 12 months traveling to and from doctor’s appointments for tuberous sclerosis complex care for their pediatric patient, whereas caregivers of the adult group spent 20.0 (±18.0) hours. Caregivers of the pediatric and adult groups spent a median of 8.0 (±21.5) and 9.0 (± 20.0) hours, respectively, over the past month researching tuberous sclerosis complex, finding appropriate doctors, and scheduling visits. Compared to adult patients not receiving most medical care in tuberous sclerosis complex clinics, caregivers of adult patients who do receive most medical care in tuberous sclerosis complex clinics reported spending more time traveling to and from doctor’s offices for tuberous sclerosis complex care (median hours 24.5 ± 25.0 vs 15.0 ± 16.0, P = .005) and more median total hours in a doctor’s office in the past 6 months (35.0 ± 41.0 vs 15.0 ± 34.0, P = .027). There was no difference in the number of medications taken within each patient group whether receiving medical care at tuberous sclerosis complex clinics or not.
The caregivers of pediatric patients reported that their patients most commonly had surgery due to epilepsy (15.9%), laser surgery to remove skin lesions (13.1%), or brain surgery for subependymal giant cell astrocytoma (7.4%). The most common surgeries reported by caregivers for their adult patients were laser surgery to remove skin lesions (15.2%), brain surgery for epilepsy (12.1%), brain surgery for subependymal giant cell astrocytoma (10.1%), or nephrectomy (7.1%).
Caregivers reported that their tuberous sclerosis complex patients had a number of diagnostic tests and procedures over the previous year. In the past year, pediatric patients most often received a magnetic resonance imaging (MRI; 67%), underwent blood work (56.8%), had an ultrasound (45.5%), an electroencephalogram (EEG; 56.3%), or a tuberous sclerosis complex–related eye examination (40.3%). Over a third of the pediatric tuberous sclerosis complex patients also had an electrocardiogram (32.4%) and a computed tomographic (CT) scan (38.1%). Among the adult patients, the most frequent test was blood work (56.6%), followed by CT scan (43.4%), MRI (38.4%), and ultrasound (34.3%). More than a third of the adult tuberous sclerosis complex patients also had an x-ray (33.3%) and a tuberous sclerosis complex–related eye exam (31.3%). Other treatments were more commonly used by the pediatric group, of whom 56.8% received speech therapy, occupational therapy (47.2%), physical therapy (41.5%), or behavioral management (31.3%) in the past year. More than one third (33.3%) of the adult patient group reported receiving no other treatments in the past year.
Use of multiple medications was common among tuberous sclerosis complex patients, with 64% of pediatric and 75% of adult patients taking 2 or more medications for tuberous sclerosis complex symptoms or manifestations. The most prescribed classes of medications for adult patients were antidepressants/antianxiety/antipsychotics (41%), antiepileptic (36%), and sleep medication (23%). For the pediatric group, antiepileptics (77%) were reported as most common, followed by sleep medications (28%).
Caregivers were asked to evaluate which manifestation was most bothersome to their tuberous sclerosis complex patient. The most bothersome manifestations for the tuberous sclerosis complex adult group were seizures (20.2%), anxiety (12.1%), and kidney complications (9.1%). Caregivers of the tuberous sclerosis complex pediatric group reported that the most bothersome manifestations for their patients were seizures (33%), cognitive concerns (25%), and skin lesions (13.1%). Caregivers were also asked to evaluate their level of agreement with statements about effects of tuberous sclerosis complex on patients’ everyday life. Caregivers of the pediatric group showed the most agreement (ie, “very much agree”) with statements about patients’ sleeping difficulties, such as having trouble breathing during sleep, unusual sleeping episodes (nightmares, sleepwalking/talking), and waking in the middle of the night and not being able to get back to sleep. Caregivers of adult patients reported they “very much agree” with statements about their patient having trouble breathing while sleeping, unusual sleeping episodes, and worries that the tuberous sclerosis complex patient would pass on tuberous sclerosis complex to future offspring.
Psychosocial Burden/Health-Related Quality of Life of Tuberous Sclerosis Complex Caregivers
Caregiver health-related quality of life and depressive symptomatology was compared by tuberous sclerosis complex patient group. Caregivers of adult patients reported significantly lower (worse) mean physical health-related quality of life scores (Physical Component Summary score: 46.5 vs 51.0, P < .0001) compared to caregivers of tuberous sclerosis complex pediatric patients. Mental health–related quality of life scores did not differ between caregivers of tuberous sclerosis complex patient groups.
Compared to US-based norms for healthy adults, tuberous sclerosis complex caregivers overall had significantly lower mean physical (Physical Component Summary score: 49.4 vs 54.3, P < .0001) and mental health–related quality of life scores (Mental Component Summary score: 43.4 vs 52.9, P < .0001) and statistically lower Short Form Health Survey scores for all 8 subdomains: Physical Functioning, Role Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role Emotional, and Mental Health. However, tuberous sclerosis complex caregivers showed statistically significantly better scores for physical (49.4 vs 45.4, P < .0001) and mental health–related quality of life (43.4 vs 37.4, P < .0001) and across the 8 subdomains compared to US-based norms for adults with clinical depression (Table 3).
Health-Related Quality of Life Burden: Tuberous Sclerosis Complex Caregiver Versus US Based Population Norms.
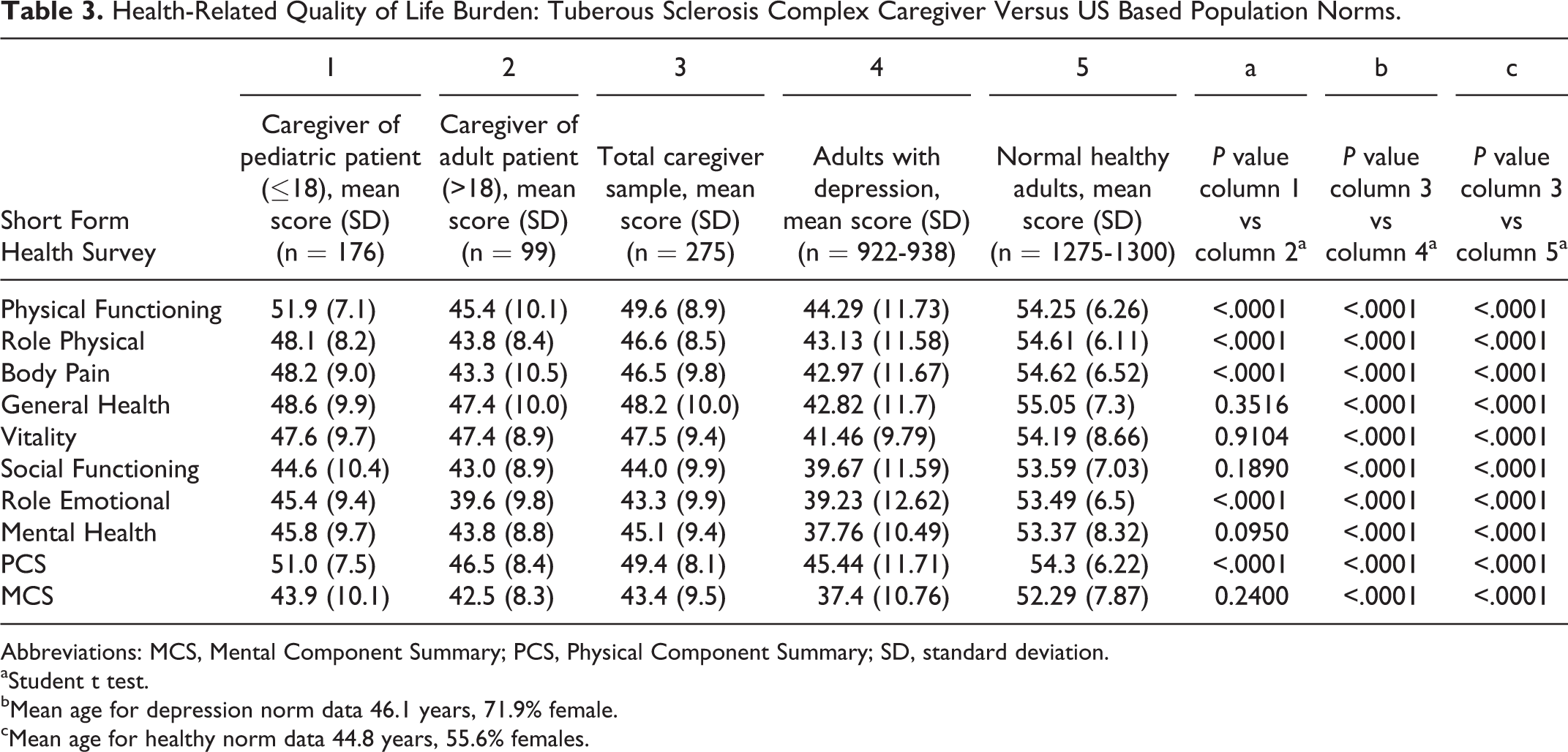
Abbreviations: MCS, Mental Component Summary; PCS, Physical Component Summary; SD, standard deviation.
aStudent t test.
bMean age for depression norm data 46.1 years, 71.9% female.
cMean age for healthy norm data 44.8 years, 55.6% females.
Although 42% of caregivers’ scores on the Hamilton Depression Inventory–Short Form did exceed the 8.5 point cut-off indicative of the presence of mild to severe depressive symptoms, the group’s mean score did not: 8.2 points for caregivers of tuberous sclerosis complex adult patients and 6.9 points for caregivers of tuberous sclerosis complex pediatric patients. A total of 19.3% of caregivers reported that they were taking psychotropic or antidepressant medication, which is more than two-thirds higher than the national average of 11.1%. 19 Compared to nonpsychiatric community-dwelling healthy controls (2.05 ± 1.92) and individuals with anxiety disorders (7.19 ± 4.4), caregivers of tuberous sclerosis complex adult patients experience significantly higher depressive symptoms (7.36 ± 4.64; P < .0001 for both comparisons), respectively (data not shown).
The median time spent researching tuberous sclerosis complex, finding, and arranging doctor’s visits in past month is significantly related to caregiver’s health-related quality of life. Caregivers of tuberous sclerosis complex patients for both patient age groups who spent more total hours researching tuberous sclerosis complex, finding appropriate doctors, and scheduling doctors visits had lower (worse) physical (t = –3.12, P = .0025) and mental health–related quality of life scores (t = –1.96, P = .0534) and higher (worse) depressive symptom scores (t = 4.05, P = .0001) (data not shown).
Discussion/Conclusion
Our analysis is among the first to examine the burden of caregiving for tuberous sclerosis complex patients and the potential driving forces of burden on health-related quality of life. These data suggest that tuberous sclerosis complex caregivers have important unmet psychosocial, health-related quality of life and humanistic needs. Caregivers are taking care of day-to-day needs of tuberous sclerosis complex patients throughout a patient’s lifetime, resulting in considerable physical and psychosocial burden over the caregiver life course. Compared to healthy adults in the US population, tuberous sclerosis complex caregivers have significantly worse physical and mental health and more depressive symptomatology.
As evidenced by this study, tuberous sclerosis complex patients have a number of physical and mental health manifestations that span across a wide age range and result in varying levels of patient disability. A recent systematic review of burden in tuberous sclerosis complex and its neurologic manifestations concluded that morbidity and treatment burden in tuberous sclerosis complex is significant. 20 Tuberous sclerosis complex patients are utilizing a wide array of health care services annually, but fewer than half are accessing health care services and treatment at tuberous sclerosis complex clinics with multidisciplinary services. A recent study has shown that disabling seizures in epilepsy significantly lowers the quality of life of tuberous sclerosis complex patients, but successful treatment of epilepsy can improve quality of life. 21 The number and severity of tuberous sclerosis complex manifestations that a patient might have signifies frequent physician visits to many different specialists. The number of different tests and procedures reported in the past year for this study sample demonstrates that tuberous sclerosis complex is associated with significant health care resource utilization and burden on the caregiver to navigate health care resources and aid the tuberous sclerosis complex patient in seeking health care. Our study data seem to indicate that the physical and mental health burden on the caregiver may compound as tuberous sclerosis complex patients age.
The distance to tuberous sclerosis complex specialty clinics reported in our sample may represent a call for an increase in the number of tuberous sclerosis complex Centers of Excellence. Similar to other rare diseases, it is often necessary to travel long distances to obtain care from health care providers experienced in treating tuberous sclerosis complex conditions. Another challenge with rare diseases is simply identifying health care professionals who have experience treating the condition. Lack of access to experienced tuberous sclerosis complex health care professionals and the multifactorial nature of tuberous sclerosis complex are likely reasons caregivers spend so much time coordinating their patient’s care. This time spent on coordinating care is related to lower health-related quality of life scores. The relationship between increased caregiver time spent on care coordination and lower physical and mental health–related quality of life and increased depressive symptoms may indicate caregivers’ lack of time to engage in more positive activities for self or family.
A recent study in Italy has qualitatively investigated the parents’ experience of caring for a tuberous sclerosis complex child. 22 The study reported that the illness lowers quality of life for the tuberous sclerosis complex patient and for the patient’s family. The main themes expressed by caregivers were the feeling of being “out of control” as a result of the increasing unsustainability of the disease and the need to cope with the disease. Caregivers described caring for someone with tuberous sclerosis complex as a “complex process” with family routines that centered on the needs of the patient. The authors also discussed caregivers’ unmet needs, with 50% of the sample having few emotional or pragmatic resources to cope with tuberous sclerosis complex.
Survey studies have been carried out researching the functional ability and quality of life of children and adolescents with tuberous sclerosis complex in the United States and the United Kingdom. 7,23 Results from the UK survey demonstrated that many tuberous sclerosis complex patients cannot perform independent activities of daily living, 23 showing that 75% of the sample needed supervision or total care with toileting and 64% of males in the sample needed help with washing and bathing.
The increased burden over time and aging of caregivers may explain our results of worse physical health–related quality of life for caregivers of adults compared to caregivers of pediatric tuberous sclerosis complex patients. The finding that tuberous sclerosis complex caregivers have worse health-related quality of life and higher depressive symptomatology compared to healthy controls is not surprising given the intensity of caregiving required by patients with a severe health condition like tuberous sclerosis complex. Tuberous sclerosis complex is associated with a significant caregiver health-related quality of life burden in both physical and mental health domains compared to healthy adults. Caring for tuberous sclerosis complex patients with certain types of tuberous sclerosis complex manifestations may also present a differential impact on the health-related quality of life among caregivers and is an area needing further study.
Our sample represents a cross section of caregiver respondents who were recruited via social networking websites associated with the Tuberous Sclerosis Alliance. Only those who have Internet access and received our alert on a few patient advocacy websites were included. Although care was taken to conduct the survey in a scientifically rigorous manner, anonymous web-based data collection processes prevent clinician verification of diagnoses and other clinical data. The generalizability of our results may be limited because of the convenience sampling. Caregiver participants self-selected into the study. There may be differences between caregivers who responded to the survey and those who did not.
The results of this analysis on the diverse, wide-ranging, and considerable health-related quality of life burden experienced by caregivers of tuberous sclerosis complex patients should help inform clinicians and health care providers on their interactions with patients and family caregivers and the need for providing interventions for caregivers. Additional research tracking patients and caregivers longitudinally, combined with chart review and/or clinician input, would add to the knowledge base in this area. Additionally, future studies should examine the economic burden of tuberous sclerosis complex on families over time.
Footnotes
Acknowledgments
The authors thank Kelly McDaniel, Katherine Kim, and Zaneta Balantec for their assistance with data collection, Owen Cooper for his assistance with a literature review, and Ren Yu for data analysis. Authors gratefully acknowledge the support of the Tuberous Sclerosis Alliance and the patients and caregivers who participated in this survey.
Author Contributions
AMR, AMS, and CLP made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; have been involved in drafting the manuscript and revising it critically for important intellectual content; and have provided final approval of the version to be published. ZL and MM made substantial contributions to conception and design, interpretation of data; have been involved in revising the manuscript critically for important intellectual content; and have provided final approval of the version to be published. MM, DWD, MDF, JAN, JP, and JWW have been involved in revising the manuscript for important intellectual content and have provided final approval of the version to be published.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.R. and A.S. are employed by Evidera, which provides consulting and other research services to pharmaceutical, device, government, and nongovernment organizations. As Evidera employees, they work with a variety of companies and organizations and are expressly prohibited from receiving any payment or honoraria directly from these organizations for services rendered. C.Pa. was employed by United BioSource Corporation (UBC) at the time of this study. UBC provides consulting and other research services to pharmaceutical, device, government and non-government organizations. As a UBC employee, he worked with a variety of companies and organizations and was expressly prohibited from receiving any payment or honoraria directly from these organizations for services rendered.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from Novartis Oncology, East Hanover, NJ.
Ethical Approval
Institutional review board approval was granted by Ethical & Independent Review Services, Independence, MO. E&I IRB approval number is: 12055 – 01X.