
Abstract
Medulloblastoma accounts for nearly 10% of all childhood brain tumors. These tumors occur exclusively in the posterior fossa and have the potential for leptomeningeal spread. Treatment includes a combination of surgery, radiation therapy (in patients >3 years old). Patients >3 years old are stratified based on the volume of postoperative residual tumor and the presence or absence of metastases into “standard risk” and “high risk” categories with long-term survival rates of approximately 85% and 70%, respectively. Outcomes are inferior in infants and children younger than 3 years with exception of those patients with the medulloblastoma with extensive nodularity histologic subtype. Treatment for medulloblastoma is associated with significant morbidity, especially in the youngest patients. Recent molecular subclassification of medulloblastoma has potential prognostic and therapeutic implications. Future incorporation of molecular subgroups into treatment protocols will hopefully improve both survival outcomes and posttreatment quality of life.
Brief History of the Disorder
The name “medulloblastoma” was first introduced by Harvey Cushing and Percival Bailey in 1925. Drs Cushing and Bailey had initially used the term “spongioblastoma cerebelli” to describe the posterior fossa tumor seen in preadolescents. They changed the name to medulloblastoma in order to distinguish it from a distinct glial tumor contemporaneously described as a spongioblastoma by Globus and Strauss. This new nomenclature reflected medulloblastoma’s perceived derivation from 1 of the 5 pluripotent stem cells thought to populate the primitive neural tube, although it has since been recognized that there is no embryonal cell that can be identified as a medulloblast. 1 –3 Cushing, a neurosurgeon at Peter Bent Brigham Hospital, first described the defining characteristics of medulloblastoma, namely, its penchant for arising in the location of the cerebellar vermis and metastasizing to distant locations, its propensity to affect younger male patients, and its comparatively short duration of signs and symptoms prior to diagnosis. Treatment of medulloblastoma patients in Cushing’s era was fraught with immediate postoperative mortality exceeding 30%. He observed that patients who underwent more extensive operative resections had a longer duration of survival compared with those patients whose tumors were only biopsied and is credited with contributing significantly to the evolution of neurosurgical techniques in the management of medulloblastoma. Despite these advances, outcomes in medulloblastoma patients remained dismal until craniospinal irradiation was demonstrated to dramatically improve survival in a pivotal paper published by Paterson and Farr in 1953. Patients in their series received 5000 cGy to the posterior fossa and 3500 cGy to the remainder of the neuraxis and were reported to experience a 3-year survival of 65%. 4 It was subsequently recognized that this survival benefit was accompanied by significant negative impacts on younger patients in the form of neurocognitive impairment, second malignancies, and endocrine dysfunction. 5 Treatment protocols in the 1970s began to introduce adjuvant chemotherapy to surgery and radiation in an effort to improve survival outcomes, and today its use remains standard in the treatment of medulloblastoma, in some cases allowing for dose reduction or elimination of radiation. 6
In the early 1980s, based on histologic similarity between medulloblastomas and other small round blue cell tumors arising in areas outside of the posterior fossa, it was proposed that these tumors be classified together under the umbrella group of primitive neuroectodermal tumors (PNETs). 7 However, more recent studies suggest that small round blue cell tumors of the posterior fossa are molecularly distinct from those arising in the cortex or pineal regions. 8,9 This is reflected in the most recent World Health Organization (WHO) classification, which distinguishes medulloblastoma and its subtypes from other central nervous system primitive neuroectodermal tumors, pineoblastomas, and atypical teratoid/rhabdoid tumors. 10
Historically, age at diagnosis and extent of disease (as measured by the modified Chang criteria) have been most strongly associated with prognosis, with younger patients and those with more advanced disease faring more poorly than older patients and those with limited disease, respectively. 11 More recently, pretreatment prognosis of medulloblastoma has been refined by histopathologic subclassification into the following variants: large-cell medulloblastoma, anaplastic medulloblastoma, desmoplastic/nodular medulloblastoma, and medulloblastoma with extensive nodularity (MBEN). The latter 2 variants have been shown to have a significantly superior prognosis as compared to the large cell and anaplastic variants in young children. 12
The most recent insights into the biology of medulloblastomas have occurred at the molecular level, resulting in their categorization into the following molecular subgroups: wingless (Wnt), sonic hedgehog (Shh), group 3, and group 4. Each subgroup is characterized by a unique set of genetics and gene expression as well as demographic and clinical features. Although this information has not yet been used for risk stratification in clinical trials, evidence suggests that prognosis is strongly associated with subgroup affiliation. 13,14
Epidemiology
Although many sources have stated that medulloblastoma is the most common malignant brain tumor in children, the most recent data from the Central Brain Tumor Registry of the United States (CBTRUS) shows that high-grade gliomas, as a group, are slightly more prevalent. Medulloblastoma represents 9.2% of pediatric brain tumors in children aged 0 to 14 years, and approximately 338 new pediatric cases are diagnosed in the United States each year. 15 –18 Up to 30% of cases are reported in adults, generally prior to age 40 years. The incidence of medulloblastoma peaks during the first decade of life with a higher incidence noted in children between 3 and 4 years of age and between 8 and 10 years of age. Fewer than 5% of cases are associated with the hereditary cancer predisposition syndromes familial adenomatous polyposis (FAP), historically known as Turcot syndrome, or nevoid basal cell carcinoma syndrome (NBCCS), also called Gorlin syndrome. In children, medulloblastoma is slightly more common in males, with a male to female incidence rate ratio of 0.63. There is no apparent racial or ethnic predisposition. 16,19
Clinical Presentation
In concordance with its relatively rapid growth rate, patients with medulloblastoma commonly present with symptoms evolving over a period of weeks to months. A combination of signs and symptoms of cerebellar dysfunction and increased intracranial pressure are frequently encountered. Classic symptoms of increased intracranial pressure include irritability, lethargy, nausea and vomiting, morning headaches, anorexia, and behavioral changes. Signs of cerebellar involvement may differ depending on the location of the lesion. Midline cerebellar tumors are more likely to result in truncal ataxia (with impaired tandem gait and Romberg testing) as compared to cerebellar hemispheric tumors that are more commonly associated with appendicular ataxia (manifesting as difficulty with rapid alternating movements, finger-nose-finger, and heel-shin testing). Additionally, cranial nerve involvement may be present either as a result of direct involvement of these nerves or as a consequence of increased intracranial pressure. Diplopia resulting from abducens nerve dysfunction is not uncommon. In cases where disease dissemination is present, symptoms related to the location of metastatic involvement may also be observed.
Differential Diagnosis
The radiographic differential diagnosis of a posterior fossa mass in children comprises ependymoma, atypical teratoid/rhabdoid tumor, and pilocytic astrocytoma most commonly, with additional considerations including exophytic brain stem glioma and choroid plexus papilloma as well as teratoma in infants and hemangioblastoma in patients with Von Hippel-Lindau syndrome. In adults, metastatic disease from a distant primary site is the most frequently encountered posterior fossa lesion. 20
Medulloblastomas have distinct imaging characteristics on both computed tomography (CT) and magnetic resonance imaging (MRI). Three-quarters of medulloblastomas arise from the cerebellar vermis and tend to protrude into the fourth ventricle, although the site of origin in adults is more frequently the cerebellar hemispheres rather than the vermis. In contrast to ependymomas, medulloblastomas do not typically extend into the basal cisterns. On CT, they are most commonly seen as a hyperdense mass arising from the vermis with cyst formation or necrosis more frequently observed in older patients. Effacement of the fourth ventricle and ventricular dilatation secondary to obstructive hydrocephalus are often seen. Prominent contrast enhancement is present in 90% of cases with calcification seen in 10%-20%. On MRI (see Figure 1), medulloblastomas are hypointense to grey matter on T1-weighted imaging with heterogeneous gadolinium enhancement in 90%. They are generally iso- to hyperintense to grey matter on T2-weighted imaging and commonly appear heterogeneous because of cyst formation, calcification, and necrosis. Diffusion-weighted imaging shows restricted diffusion and medulloblastomas are hyperintense to surrounding brain on fluid-attenuated inversion recovery sequences. MR spectroscopy shows elevated choline peaks and decreased creatine and N-acetyl acetate peaks, with occasional elevation in lactic acid and lipid peaks. 21,22
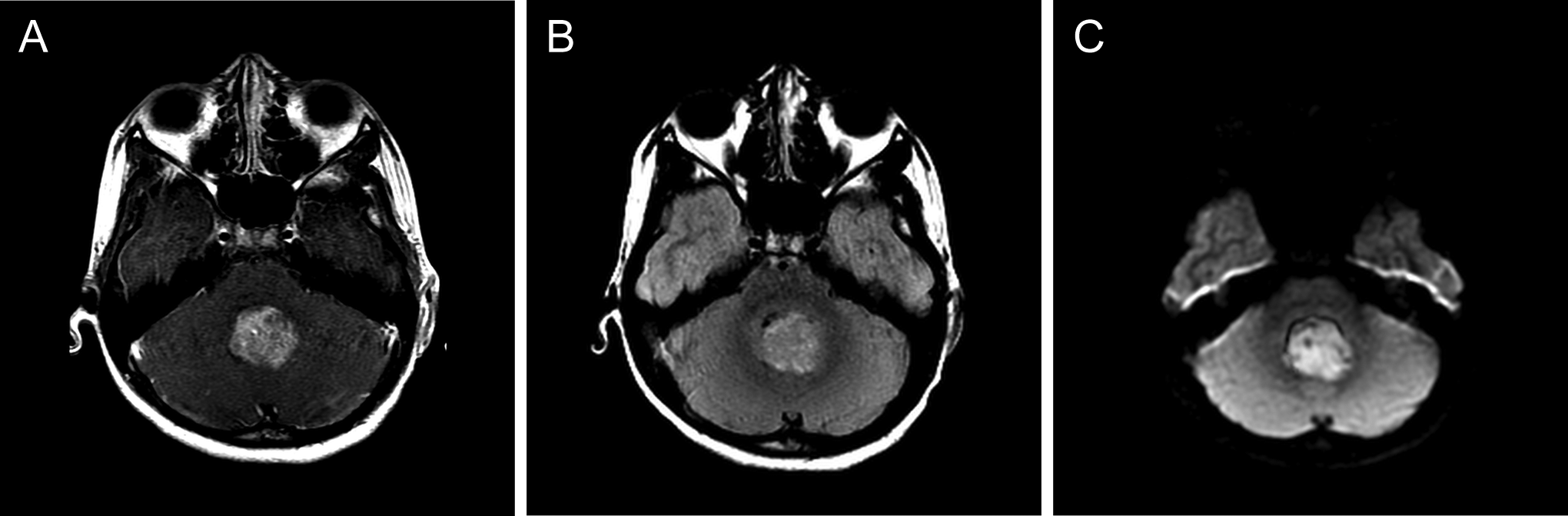
(A) Magnetic resonance imaging (MRI) T1 + gadolinium. (B) MRI fluid-attenuated inversion recovery. (C) MRI diffusion-weighted imaging.
A recent publication by Perreault et al reported a statistically significant relationship between medulloblastoma molecular subgroups and both enhancement pattern and tumor location on MRI. In their cohort of 47 patients, tumors located along the cerebellar peduncle/cerebellopontine angle cistern were found to exclusively represent Wingless pathway tumors (Wnt), with 3 of 4 Wnt pathway tumors occurring in this location while one was located in the midline vermis/fourth ventricle. More than half of the 13 sonic hedgehog (Shh) tumors were located within the cerebellar hemispheres, with the remainder found in the midline vermis/fourth ventricle. Shh was the only molecular subgroup whose tumors were found in hemispheric locations. All 30 group 3 and group 4 tumors were encountered in the midline vermis/fourth ventricle. Group 3 tumors were more likely to demonstrate ill-defined tumor margins, whereas group 4 tumors were generally characterized by minimal or absent contrast enhancement. The presence of cysts, hemorrhage/mineralization, edema, and necrosis were not specifically associated with any molecular subgroup. 23 In a series of 130 patients from the Hospital for Sick Children in Toronto, the presence of hydrocephalus necessitating cerebrospinal fluid diversion surgery was approximately 30% in patients with Shh, group 3, and group 4 tumors. None of the 15 Wnt medulloblastoma patients in this cohort required endoscopic third ventriculostomy or ventriculoperitoneal shunt placement. This finding was thought to be a result of clinical features associated with this molecular subgroup, namely, older age and lack of metastatic disease at diagnosis. 24 The presence of hydrocephalus on MRI would therefore argue in favor of Shh, group 3, or group 4 molecular subgroups over Wnt.
Workup
Imaging of the entire neuraxis is indicated because of medulloblastoma’s predilection for spread along the cerebrospinal fluid pathways with resultant drop metastases and leptomeningeal disease, present in approximately one-third of patients at time of diagnosis. In a stable patient, it is considered preferable to obtain this imaging prior to surgical intervention in order to avoid potentially confounding postoperative artifact. Lumbar puncture for cerebrospinal fluid cytology is performed to provide additional information regarding microscopic leptomeningeal disease dissemination, although evaluation of the cerebrospinal fluid may be negative in patients with nodular spinal cord disease. Lumbar puncture may be performed prior to surgery once hydrocephalus and increased intracranial pressure have been ruled out via imaging studies. As patients with posterior fossa tumors often present with symptomatic hydrocephalus, it is not uncommon for lumbar puncture to be deemed unsafe at the time of presentation. When deferred until the postoperative setting, lumbar puncture should be delayed by 10 to 14 days in order to avoid false-positive evaluations due to surgical tumor debris. 25 –27 The combination of brain/spine imaging and lumbar cerebrospinal fluid cytology is more sensitive than either test alone; therefore, both are recommended as part of the extent of disease evaluation. 28 Extraneural spread of disease to bone and bone marrow has also rarely been reported in medulloblastoma patients. A bone scan may be indicated in symptomatic patients, and bone marrow evaluation, though not routinely performed, is considered in any patient with unexplained abnormal peripheral blood counts and occasionally in those medulloblastoma patients younger than 3 years because of their increased risk of disease dissemination outside of the central nervous system. 26 –28
The staging criteria proposed by Chang et al in 1969 categorizes medulloblastomas by degree of metastasis. M0 disease is defined as lacking any evidence of metastatic disease by MRI of brain and spine as well as analysis of cerebrospinal fluid cytology. M1 disease is characterized by positive cerebrospinal fluid cytology without gross leptomeningeal tumor deposits visible on imaging of the neuraxis. M2 and M3 disease are both characterized by the presence of gross nodular seeding either within the third or lateral ventricles or the cerebellar/cerebral subarachnoid space (M2) or within the spinal subarachnoid space (M3). Finally, M4 medulloblastomas are those rare cases that present with disease dissemination outside of the central nervous system. 11 The Chang staging system also classified medulloblastomas by the size and extent of the primary tumor. This has not been shown to have prognostic significance, in contrast to the residual postoperative tumor bulk and the presence or absence of disease dissemination. 29
Histology
The 2007 WHO classification system recognizes several histopathologic variants of medulloblastoma, all of which are categorized as grade IV neoplasms within the broader grouping of embryonal neuroepithelial tumors. In addition to classic medulloblastoma, other variants include desmoplastic/nodular medulloblastoma, medulloblastoma with extensive nodularity, anaplastic medulloblastoma, and large cell medulloblastoma. 10 The classic variant is the most frequently encountered and is characterized by both high cellularity and elevated proliferative indices. Classic medulloblastoma cells typically have small to medium-sized, round to oval-shaped hyperchromatic nuclei, and minimal cytoplasm. Homer-Wright rosettes are sometimes intermingled and their presence can be associated with high mitotic activity and increased nuclear pleomorphism. Although desmoplasia may occur focally in many medulloblastomas, widespread desmoplasia is characteristic of the desmoplastic/nodular variant, which is also distinguished from the classic variant by the presence of nodular, reticulin-poor “pale islands” of neurocytic differentiation surrounded by densely packed, mitotically active cells. Compared with desmoplastic/nodular medulloblastoma, the related medulloblastoma with extensive nodularity variant has an expanded lobular architecture with more prominent reticulin-free zones that are more elongated and rich in neutropil-like tissue. Both the desmoplastic/nodular and medulloblastoma with extensive nodularity variants are associated with an improved prognosis as compared to classic medulloblastomas. 12,30 –32 In contrast, large cell and anaplastic medulloblastomas have a distinctly poor prognosis when compared to the classic variant. Both large cell and anaplastic variants comprise cells with large, round, vesicular nuclei and prominent nucleoli, from which the large cell variant derives its name. Like desmoplastic/nodular and medulloblastoma with extensive nodularity variants, large cell and anaplastic medulloblastomas have a significant degree of cytologic overlap and are differentiated only by the degree of anaplasia, characterized by marked nuclear pleomorphism and nuclear molding as well as atypical mitotic forms and abundant apoptotic bodies. 33,34 Significantly inferior outcomes have been observed in patients with increasing degrees of anaplasia. 35,36 Two additional histologic patterns have been recognized but are not considered distinct variants. Medullomyoblastomas contain rhabdomyoblastic cells that may be encountered in distinct groups or intermingled with the neuroepithelial cells of one of the aforementioned medulloblastoma variants. 37 The most rarely reported pattern is that of melanotic medulloblastoma, characterized by the accumulation of melanin in the cytoplasm of the neuroepithelial medulloblastoma cells. 38
Molecular Pathology
In 2010, an international group of medulloblastoma experts convened in Boston to come to a consensus on the molecular subgrouping of medulloblastomas. Four distinct subgroups were identified based on transcriptional profiling studies; wingless (Wnt), sonic hedgehog (Shh), group 3, and group 4 (see Figure 2). Each subgroup was characterized by a unique set of demographic and clinical features, genetics, and gene expression. 14 Identification of molecular subgroup more accurately predicts outcome and clinical behavior than does histopathology or clinical staging. It is hypothesized that these different medulloblastoma subgroups arise from distinct cells of origin. This is in part supported by the observation that medulloblastoma maintains its subgroup affiliation at the time of both recurrence and metastasis, a finding that differentiates medulloblastoma from other cancers that demonstrate a change in molecular subclass at recurrence or metastasis. 39 –41 These molecular subgroups are distinct from the histologic subtypes, although there are some areas of substantial overlap as demonstrated by an international meta-analysis of data from 7 studies with a total of 550 medulloblastoma patients. In this meta-analysis, 97% of 58 Wnt pathway tumors were classic medulloblastoma subtype by histology, and 89% of 44 desmoplastic/nodular medulloblastomas in infants belonged to the Shh molecular subgroup. 42
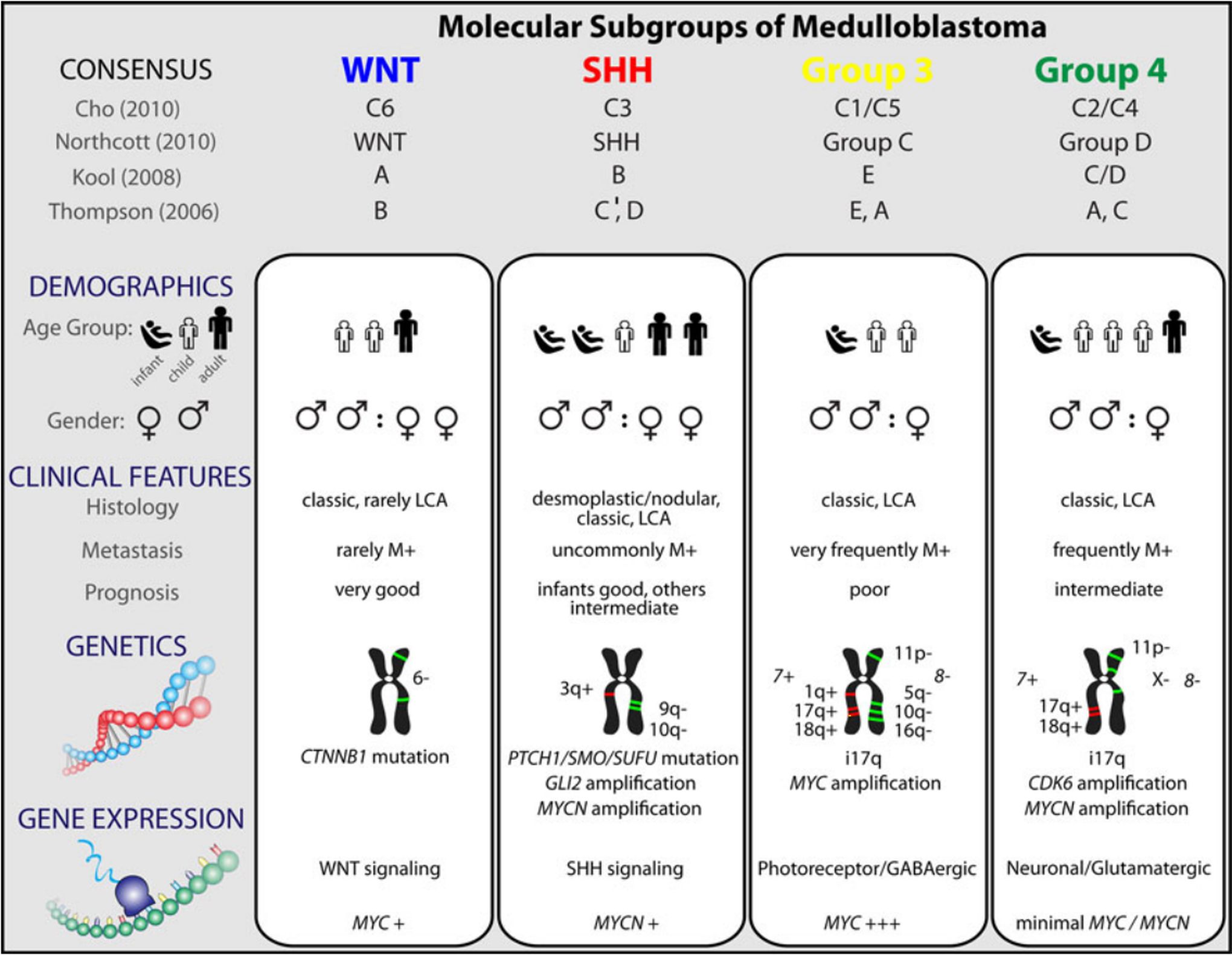
Comparison of the various subgroups of medulloblastoma including their affiliations with previously published papers on medulloblastoma molecular subgrouping. Source: Taylor MD et al. “Molecular subgroups of medulloblastoma: the current consensus.” Acta Neuropathol. 2012;123(4):465-472.
Interestingly, a recent study by Perreault et al demonstrated that molecular subgroup could be correctly predicted by neuroimaging in 65% of 99 retrospectively reviewed medulloblastoma cases based on tumor location and enhancement pattern. In terms of location, Wnt pathway tumors were most likely to arise in the cerebellopontine angle cistern or cerebellar peduncle, whereas Shh pathways tumors were found in the cerebellar hemispheres. Group 3 and group 4 tumors were the primary subgroups encountered in the midline fourth ventricle, and group 4 tumors were characterized by absent or minimal contrast enhancement. 23
Wingless Pathway Tumors
The Wnt/β-catenin pathway is composed of secreted glycoproteins that act through signal transduction to control various aspects of embryonic development. Unregulated activation of Wnt pathway signaling leads to the accumulation of β-catenin, encoded by the CTNNB1 gene, and results in aberrant upregulation of transcription and subsequent oncogenesis. Wnt pathway tumors are the least common of the 4 molecular subgroups, representing approximately 10% of sporadic medulloblastomas. They are characterized genetically by the presence of monosomy 6, CTNNB1 mutations, and nuclear β-catenin positivity by immunohistochemistry. Demographically, Wnt subgroup medulloblastomas are more common in children and adults than in infants, and the slight male predominance generally seen in medulloblastomas has not been demonstrated in tumors of this subgroup. Fewer than 10% of Wnt subgroup tumors present with metastatic disease at the time of diagnosis, and outcomes for these medulloblastomas are excellent, with 5-year overall survival of 95% in children and 100% in adults. TP53 mutations are found almost exclusively in Wnt and Shh subgroup medulloblastomas. In contrast to Shh subgroup tumors, the presence of mutant TP53 in Wnt subgroup tumors does not impact prognosis. 43
The association between primary central nervous system tumors and colorectal polyposis, historically known as Turcot syndrome, is well studied in patients with familial adenomatous polyposis (FAP). Patients with FAP have a loss of functional adenomatous polyposis coli (APC) protein as a result of an inactivating germline mutation of the APC gene. The APC protein forms part of a “destruction complex” that serves to degrade β-catenin, and its loss results in the accumulation of β-catenin in the cytoplasm and nucleus. This specific disruption in the Wnt signaling pathway leads to an increased risk of medulloblastoma in FAP patients as compared to the general population. 44,45
Sonic Hedgehog Pathway Tumors
The Shh medulloblastoma subgroup is also associated with a genetic predisposition syndrome characterized by germline mutations in the patched-1 gene (PTCH1) or the suppressor of fused gene (SUFU). Individuals with Gorlin syndrome, also known as nevoid basal cell carcinoma syndrome, suffer from the early onset of multiple nevoid basal cell carcinomas and medulloblastomas as well as developmental abnormalities. Loss of function PTCH1 and SUFU mutations result in truncation of their associated protein products, leading to failure of their tumor suppressor effects and activation of Shh signaling with subsequent tumorigenesis. Germline PTCH1 mutations have been associated with a risk of medulloblastoma of less than 2%, whereas the risk is substantially higher in those Gorlin syndrome patients with germline SUFU mutations, as illustrated in a small study of 9 patients in which in one-third developed childhood medulloblastoma. 46 Germline Shh pathway mutations comprise only a small proportion of medulloblastomas. Somatic mutations in PTCH1 and SUFU are also associated with sporadic medulloblastomas characterized by activation of the Shh pathway, along with PTCH2, SMO, GLI1, and GLI2 mutations. As a whole, Shh subgroup tumors represent approximately 30% of medulloblastomas overall and demonstrate a bimodal distribution, being much more common in patients younger than 3 years and older than 16 years than in children between 3 and 16 years of age. Similar to Wnt pathway medulloblastomas, Shh pathway tumors are equally distributed between both genders. They are more likely to metastasize than Wnt subgroup tumors in infants and children, but less likely than group 3 or group 4 tumors to present with disseminated disease. Survival for Shh subgroup medulloblastomas is intermediate between that of Wnt and group 3 medulloblastomas and varies significantly according to age and histologic subtype. Infants with desmoplastic/nodular tumors have the best prognosis among Shh subgroup tumors, with 10-year overall survival of 84%. The increased prevalence of desmoplastic/nodular histology in infants likely accounts for their increased overall survival at 10 years of 77% as compared to children and adults, whose 10-year overall survivals are 51% and 34%, respectively. Notably, TP53 mutations are associated with significantly inferior outcomes in Shh subgroup medulloblastomas, in contrast to Wnt pathway tumors, and occur most often in patients between 5 and 18 years of age, generally representing the least frequently encountered age group in Shh subgroup tumors. 42,43
Non-Wnt/Shh Tumors
The non-Wnt/Shh tumor subgroups comprise group 3 and group 4, in which the underlying genetic driver mutations have not yet been established. In contrast to the Wnt and Shh subgroups, both group 3 and group 4 are characterized by a male predominance of approximately 2:1 and are associated with a higher frequency of disease dissemination, with metastases detected in approximately 30% of patients at time of diagnosis. Despite these similarities, group 3 and group 4 subgroup medulloblastomas have distinctive clinical and genomic features. Group 3 tumors, representing approximately 30% of medulloblastomas, are more likely to have high-level expression and amplification of MYC, occur more often in infants and children, and are associated with the least favorable outcomes across all molecular subgroups, with 10-year overall survival of 39% in infants and 50% in children. Group 4 tumors form the largest molecular subgroup of medulloblastomas, comprising about 35% of medulloblastomas overall. Similar to Shh subgroup tumors, group 4 tumors have a prognosis that is intermediate between those of Wnt and group 3 subgroup tumors. The peak incidence for this subgroup is in late childhood and early adolescence. Within group 4 medulloblastomas, significantly inferior outcomes have been observed in patients with metastatic disease or MYCN amplifications. 42
Treatment—General Principles
As mentioned above, medulloblastoma therapy has evolved to include surgery, radiation therapy, and adjuvant chemotherapy. It is recommended that all medulloblastoma patients undergo maximal safe surgical resection. There is not a role for biopsy if the medulloblastoma diagnosis is supported by radiographic evidence. Postoperatively radiated patients in whom a gross total or near total resection is achieved have been shown to have superior overall survival as compared to patients who undergo biopsy alone. 47,48 Beyond surgical resection, current standards of radiation therapy and medical management vary by extent of disease and age of the patient, based on the risks of recurrence and of neurocognitive effects of radiation therapy, respectively. As it has been demonstrated to significantly improve outcomes, adjuvant chemotherapy is recommended for all patients. 6 Patients who are 3 years of age or older are stratified as either “average-risk” or “high-risk” based on the volume of postoperative residual tumor and the presence or absence of disseminated disease. Average-risk children are defined as having <1.5 cm2 of tumor present after surgical resection and both negative cerebrospinal fluid cytology and no evidence of disease dissemination on MRI of both brain and spine. In contrast, high-risk children are those with ≥1.5 cm2 of residual postoperative tumor and/or disease dissemination. A third group of patients, those younger than 3 years, are treated without upfront radiation therapy because of the unacceptably high risk of severe neurocognitive impairment. Outcomes in the youngest patients are often poor. The Children’s Cancer Group study CCG-9921 reported 5-year event-free survival ranging from 25% in infants with metastatic disease at diagnosis to 41% in nonmetastatic patients with minimum postoperative residual tumor. 49 In addition to younger age, larger residual tumor volume after surgery, and the presence of metastatic disease at diagnosis, inferior prognosis has also been associated with MYC amplification, anaplastic or large cell histology, and tumors molecularly categorized as either group 3 or sonic hedgehog pathway with TP53 mutations.
Treatment and Prognosis: Average-Risk Patients ≥3 Years of Age
In the postoperative setting, average-risk patients were previously treated with 36 Gy craniospinal irradiation and a boost to the posterior fossa for a total dose of 54 Gy. The latter is indicated because of the high rate of relapse within the posterior fossa. Studies conducted by the International Society of Pediatric Oncology (SIOP) and the Children’s Oncology Group, among others, have supported a reduction in the craniospinal irradiation dose to 23.4-24 Gy with the addition of adjuvant chemotherapy. 50,51 ACNS0331, a COG study of further craniospinal irradiation dose-reduction to 18 Gy in young children (aged 3 to 7 years) is currently underway. Similarly, several studies have demonstrated that the posterior fossa radiation volume may be safely reduced through conformal treatment to the tumor bed, allowing for sparing of normal structures, including the temporal lobes, hypothalamus, and cochleae, although this is not a universally accepted practice. 51 –53 Similarly, the use of IMRT or proton beam therapy can reduce exposure to the heart and liver during craniospinal irradiation. 54 –57 Vincristine is generally given weekly during radiation therapy. Current recommendations for postradiation chemotherapy in average-risk patients include approximately 1 year of therapy consisting of 8 cycles at 6-week intervals of cisplatin, lomustine (CCNU), and vincristine. This regimen, first described by Packer et al in 1988, is associated with a 5-year event-free survival of approximately 80%. 58 A similar regimen substituting cyclophosphamide for lomustine has been associated with statistically equivalent outcomes. 27,59 The St Jude Medulloblastoma-96 trial found a similar event-free survival of 83% utilizing an alkylator-based, dose-intensive chemotherapy regimen consisting of four 4-week cycles of cyclophosphamide, cisplatin, and vincristine with autologous stem cell rescue following each cycle. 50 Delays in the initiation of radiation therapy have been associated with inferior outcomes, including those delays related to the use of neoadjuvant chemotherapy prior to irradiation. 60 –62
Treatment and Prognosis: High-Risk Patients ≥3 Years of Age
The postoperative treatment of high-risk medulloblastoma in children 3 years and older typically involves the administration of “standard dose” radiation therapy (36 Gy craniospinal irradiation with a boost to both the posterior fossa and focal sites of metastatic disease to 55.8 Gy) as well as adjuvant chemotherapy, although the ideal chemotherapeutic regimen has not been identified to date. A phase II trial of a regimen utilizing radiation therapy with concurrent vincristine followed by maintenance chemotherapy with lomustine, vincristine, and cisplatin showed a progression-free survival of 67%, with the caveat that patients with M1 disease were analyzed together with patients with M2 or M3 disease. 63 A larger subsequent trial from the German Society of Pediatric Hematology and Oncology of an identical regimen found 3-year progression-free survival in M2/M3 patients to be only 30%, and the Children’s Cancer Group (CCG) showed a similar outcome with 5-year progression-free survival of 40% using an adjuvant chemotherapy regimen of radiation therapy with concurrent vincristine followed by lomustine, prednisone, and vincristine. 29,62 Neoadjuvant chemotherapy, including the CCG’s “8-in-1” regimen (8 drugs in 1 day, comprising vincristine, methylprednisolone, lomustine, hydroxyurea, procarbazine, cisplatin, cyclophosphamide, and cytarabine), the PNET-3 regimen tested by the International Society of Pediatric Oncology/United Kingdom Children’s Cancer Study Group (etoposide, carboplatin, cyclophosphamide, and vincristine), and the German HIT 91 trial’s “sandwich therapy” (consisting of 2 ifosfamide, etoposide, cisplatin, cytarabine, and high-dose methotrexate cycles prior to radiation therapy), has shown similarly poor outcomes for high-risk patients. 29,62,64 The current COG protocol, ACNS0332, was designed to address 2 specific endpoints: whether the addition of carboplatin to vincristine as a radiosensitizer during radiation therapy or concurrent retinoid therapy during maintenance chemotherapy and for 6 months thereafter results in improved survival. The retinoid-containing arms of this trial were recently closed after futility analysis suggested that isotretinoin therapy will not lead to a significant event-free survival advantage. The adjuvant chemotherapy used in this protocol consists of six 4-week cycles of cisplatin, cyclophosphamide, and vincristine. A previous COG phase I/II trial of post–radiation therapy vincristine and cyclophosphamide with or without cisplatin and with the addition of carboplatin during radiation therapy showed 5-year overall and progression-free survival of 78% and 71%, respectively. 65 Comparable outcomes have been achieved by groups utilizing high-dose chemotherapy with autologous stem cell rescue. The St Jude Medulloblastoma-96 trial demonstrated a 5-year overall and progression-free survival of 70% in high-risk patients with the same cyclophosphamide-based, dose-intensive chemotherapy regimen utilized in average-risk patients as described above, with a percentage of patients also receiving preradiotherapy topotecan. There were no treatment-related mortalities observed. 50 Researchers from the Samsung Medical Center in Seoul investigated the use of high-dose chemotherapy with autologous stem cell rescue with reduced-dose radiotherapy in 20 patients, finding a 5-year event-free survival of 70% using a regimen consisting of induction chemotherapy for 2 cycles followed by radiation therapy and 4 additional cycles of induction chemotherapy prior to tandem autologous transplant. Induction chemotherapy consisted of cisplatin, etoposide, vincristine, and either cyclophosphamide or ifosfamide. Craniospinal irradiation was initially given at a dose of 23.4 Gy but this was increased during the study period to 30.6 Gy in patients older than 6 years because of spinal cord relapse or progression in 3 of 9 patients with metastatic disease. Focal boosts were given to the sites of primary and nodular metastatic disease at total doses of 54 and 45 Gy, respectively. The first tandem transplant used a regimen of carboplatin, thiotepa, and etoposide, whereas the second comprised cyclophosphamide and melphalan. Treatment-related mortality in this study was 10%. 66 Another group has attempted to modulate radiotherapy-induced side effects through the use of hyperfractionated accelerated radiotherapy (HART). Thirty-three patients in their study received 2 months of postoperative induction chemotherapy with etoposide, methotrexate, cyclophosphamide, and carboplatin. Hyperfractionated accelerated radiotherapy was subsequently administered with a craniospinal irradiation dose of 31.2 Gy and a posterior fossa boost to 59.7 Gy in patients younger than 10 years of age, and a craniospinal irradiation dose of 39 Gy with a posterior fossa boost to 60 Gy in those older than 10 years. An additional 9 Gy was given to sites of nodular metastatic disease. Patients in complete remission after hyperfractionated accelerated radiotherapy received maintenance chemotherapy for 1 year with vincristine and lomustine, whereas those without complete remission received tandem high-dose thiotepa-based autologous transplant. Five-year event-free survival rates in this study were 70%. 67
Treatment and Prognosis: Infants and Children <3 Years of Age
The neurocognitive outcomes in children younger than 3 years who receive craniospinal irradiation are very poor. For this reason, investigations have focused on delaying or omitting radiotherapy in this population. There is evidence that regimens consisting of surgery and chemotherapy without radiation therapy can be successful in specific subsets of medulloblastoma patients, namely M0 patients in whom a gross total surgical resection has been achieved and in patients with either desmoplastic/nodular medulloblastoma or medulloblastoma with extensive nodularity histologic subtypes. The former was investigated in medulloblastoma patients younger than 5 years of age without metastases or postoperative residual disease who were enrolled in a French Society of Paediatric Oncology (SFOP) trial. These patients had 5-year progression-free survival of 41% as compared to 0% in those in whom only a subtotal resection was performed using postoperative multiagent chemotherapy (carboplatin, vincristine, procarbazine, etoposide, and cisplatin) without radiotherapy. 68 Two chemotherapy regimens (vincristine and etoposide with either cisplatin and cyclophosphamide or carboplatin and ifosfamide) were investigated in a CCG trial that included 92 medulloblastoma patients younger than 36 months of age. Five-year event-free and overall survival for these patients were 32% and 43% with some suggestion of improved early tumor control, but not survival benefit, with the cisplatin and cyclophosphamide-containing regimen. Radiotherapy was withheld until disease progression and approximately one-quarter of M0 patients in whom a gross total resection was achieved were alive and without evidence of disease progression at the 5-year mark without the use of radiation therapy. 49 Improved survival was demonstrated in several trials with the use of systemic and intraventricular methotrexate in addition to a postoperative systemic chemotherapy regimen of cyclophosphamide, carboplatin, etoposide, and vincristine. Progression-free and overall survival with this regimen in 48 patients younger than 4 years without disseminated disease were 57% and 80%, respectively. 69,70 Another multi-institutional trial using the same agents resulted in progression-free and overall survival of 58% and 66% in 43 medulloblastoma patients age 3 years or younger with or without disseminated disease. Again, in this trial, the benefit of localized disease and gross total resection was appreciated, with 5-year progression-free survival and overall survival rates up to 82% and 92%, respectively, in patients without postoperative residual tumor or evidence of metastatic disease. Unfortunately, the use intraventricular methotrexate was shown in this study to be associated with significantly lower age-matched IQ scores, although they remained significantly superior to those of children treated with radiotherapy and systemic chemotherapy. 71 The use of high-dose chemotherapy with autologous stem cell rescue, investigated in the multi-institutional “Head Start” I and II trials, demonstrated 5-year progression-free and overall survival rates of 52% and 70% in 21 M0 patients. There was no significant impact on intellectual functioning in the 71% of surviving patients who were not treated with radiotherapy. Of note, there were 4 treatment-related deaths in these 2 trials. 72 The current COG trial, ACNS0334, is designed to investigate whether the addition of systemic methotrexate to a postoperative induction regimen of etoposide, cyclophosphamide, cisplatin, and vincristine followed by high-dose thiotepa and carboplatin with autologous stem cell rescue will improve survival in medulloblastoma patients younger than 3 years with disseminated disease.
Several studies have demonstrated the prognostic implications of tumor histology in this age group. The HIT-SKK’92 trial showed 5-year progression-free and overall survival of 85% and 95% in patients with desmoplastic/nodular histology. 69 A confirmatory trial performed by the same organization showed 5-year progression-free and overall survival of 90% and 100% in desmoplastic/nodular and medulloblastoma with extensive nodularity patients with M0 disease. Outcomes were significantly inferior in patients with other histologic variants. 70
Treatment and Prognosis – Patients with Relapsed Disease
Outcomes in patients with relapsed disease are generally poor, with reported 5-year survival rates of approximately 25%. 73,74 Multiple treatment strategies have been investigated, including repeat surgical resection, reirradiation, stereotactic radiosurgery, high-dose chemotherapy with autologous stem cell rescue, low-dose oral etoposide, the use of biologically targeted agents, or some combination of the above modalities. Treatment of patients with localized recurrence is more successful in general than treatment of patients with disseminated recurrence. 74 –84 The current COG trial ACNS0821 for patients with recurrent medulloblastoma compares temozolomide and irinotecan therapy to the same regimen with concurrent bevacizumab.
In young children whose initial treatment did not include radiotherapy, craniospinal irradiation as part of multimodality salvage therapy has been demonstrated to be successful in small numbers of patients. 82 –85
Complications of Treatment
Posterior fossa syndrome, also known as cerebellar mutism syndrome, is a well-known complication of surgical resection in medulloblastoma and other posterior fossa surgical interventions. It occurs in approximately one-quarter of medulloblastoma patients who undergo surgical resection, and symptoms begin to manifest within 1 to 2 days of posterior fossa surgery. The syndrome is characterized by progressively diminished speech leading to full mutism, ataxia, emotional lability, and axial hypotonia. It appears to be associated with more aggressive surgical resections and brain stem infiltration by tumor. 86 –89 Midline location of tumor and younger age have also shown some association with the development of posterior fossa syndrome and there is a suggestion that left-handed children may be at higher risk. 88,90 Recovery is incomplete in a significant number of affected patients, with persistence of any combination of neurocognitive deficits, speech/language impairment, and ataxia at 1 year following diagnosis. 89 More severely affected patients are more likely to have persistent deficits. In spite of more than 2 decades of research, the precise etiology of cerebellar mutism syndrome remains unclear. Relationships to postoperative edema, vasospasm-induced ischemia, or disruption of the dentatothalamocortical tracts have been proposed, and studies investigating the exact mechanism of the development of posterior fossa syndrome are ongoing. 90 –93
The long-term sequelae of radiation therapy and chemotherapy are well described. Endocrinopathies as well as neurocognitive and neurosensory impairment can occur as a result of craniospinal irradiation, with their frequency and severity modulated by patient age and radiation dose. 94,95 Cerebrovascular disease, including late-occurring stroke, steno-occlusive disease, vascular malformations, and strokelike migraine variants, is also known to occur with increased frequency in cancer survivors with a history of cranial irradiation. Data from the Childhood Cancer Survivor Study demonstrated that the rate of late-occurring stroke is elevated in all brain tumor survivors irrespective of radiation exposure (267.6 per 100,000 person-years); however, brain tumor survivors who had been treated with cranial radiation had a significantly higher rate of stroke (339.5 per 100,000 person-years). The risk of stroke increases in a radiation dose-dependent fashion as well as with age, with an incidence of 1.3% at 10 years from diagnosis growing to 14.2% at 30 years from diagnosis in survivors of central nervous system tumors who were treated with ≥50 Gy of cranial radiation. 96,97 Additionally, there is an increased risk of second malignancies in the radiation field. Chemotherapy drugs, particularly alkylating agents, are also associated with the development of treatment-related cancers. A 2013 review of 379 patients with nondisseminated medulloblastoma who were enrolled on the COG A9961 trial showed a cumulative incidence of secondary malignancies of 4.2% at 10 years, somewhat higher than the estimated risk of 1% to 2%. 98
Vincristine is known to cause various types of neurotoxicity, including autonomic neuropathy manifesting as constipation, isolated cranial nerve involvement (most commonly the oculomotor nerve), distal paresthesias, and loss of deep tendon reflexes. These symptoms manifest with increased severity in patients with preexisting neurologic diseases, the best described of them being Charcot-Marie-Tooth. 99 Neuropathies caused by vincristine are generally not permanent, with the exception of loss of ankle reflexes in some patients. The time to full recovery may be protracted and symptoms may continue to progress for a number of months before resolving, although children generally recover more quickly than adults. 100 Similarly, the use of cisplatin is also associated with neurotoxicity, specifically peripheral neuropathy and ototoxicity. Cisplatin-associated peripheral neuropathies are generally seen after a total cumulative dose of 300 mg/m2 and may manifest with paresthesias that begin distally and spread proximally along with loss of ankle deep tendon reflexes. Autonomic symptoms are uncommon. As with vincristine-associated neuropathies, symptoms may persist or even worsen over the course of several months. Although most patients with cisplatin-related peripheral neuropathy improve, their recovery may not be complete. 101 The ototoxicity associated with cisplatin use is characterized by high-frequency sensorineural hearing loss. The risk for ototoxicity, which is generally irreversible, is highest in children younger than 5 years of age and is related to the cumulative cisplatin dose. The impact of hearing loss on academic performance and social-emotional interactions can be substantial. 102,103
Posttherapy quality of life and psychosocial outcomes are increasingly recognized as vital factors in decision making regarding therapy. Historically, less emphasis was placed on these long-term outcomes than on survival. However, as survival has improved over the past decades, and will hopefully continue to improve with the development of molecularly targeted agents for medulloblastoma, the discussion regarding quality of life will become increasingly important both in the context of decision making regarding therapy and in the design of future cooperative protocols that may consider quality of life to be a second primary endpoint along with survival. 104
Surveillance
In cases of disease recurrence, relapses encountered on surveillance imaging are associated with improved survival as compared to those detected through the emergence of clinical symptoms. 105 Although there remains a lack of consensus on the ideal frequency of surveillance evaluations, clinical and radiographic follow-up is generally recommended at 3-month intervals during the first year following completion of planned therapy, at 3- to 4-month intervals in the second year, every 6 months during the third year, and annually thereafter. Patterns of disease recurrence were evaluated by Perreault et al in a series that included 26 patients with relapsed medulloblastoma. The incidences of local, distant, and combined relapses were relatively evenly distributed. 106 It is generally agreed upon that surveillance imaging of the brain is indicated in all patients and that imaging should include full spinal MRI in patients with a history of disseminated disease at diagnosis. Isolated spinal relapse was shown to be less frequent than brain or combined brain and spine relapse in another retrospective review by Perreault et al that included 89 medulloblastoma patients. Five patients in this series had an isolated spinal recurrence detected on screening MRI, 2 of whom did not have radiographic evidence of spinal disease at the time of diagnosis. Spinal recurrence was detected within 3 years in all 5 cases. As 1 patient with isolated spinal relapse in their series was treated with low-dose craniospinal irradiation, the authors suggested that patients treated with reduced-dose radiotherapy may benefit from closer spinal radiographic monitoring. 107 The utility of surveillance imaging of the spine has been a matter of debate. Investigators from the Hospital for Sick Children in Toronto reviewed paired brain and spine MRIs from 24 patients with relapse and found no isolated spinal recurrences. 108 However, in a series of 16 relapsed patients from Massachusetts General Hospital who were treated with proton beam radiotherapy, isolated spinal recurrence was the most frequently encountered pattern of failure. Four of the 6 patients with relapsed spine-only disease did not have evidence of metastatic disease at the time of diagnosis. 109 There remains a lack of consensus regarding the utility and recommended frequency of spinal surveillance imaging.
Similarly, surveillance lumbar puncture is generally indicated if cerebrospinal fluid cytology was positive at the time of diagnosis, although the frequency varies by institution and protocol. Endocrine screening and neuropsychological testing are also recommended for patients who were treated with craniospinal irradiation.
Conclusions/Future Directions
Despite marked improvements in overall survival for medulloblastoma patients over the past decades, considerable work remains to be done in order to improve survival within specific patient subgroups as well as to attenuate treatment-related morbidities and improve quality of life for survivors. There has been a recent striking increase in our understanding of the biology of medulloblastoma. Molecular subgrouping has allowed investigators to further characterize medulloblastomas in ways that have both prognostic and therapeutic significance. As increased attention is given to posttherapy quality of life and the risk of long-term treatment-related side effects, ways in which treatment intensity can be appropriately reduced as well as novel, less toxic, and more targeted agents are being sought. For example, a phase I study of vismodegib, an inhibitor of the Sonic Hedgehog pathway at the level of the smoothened (SMO) protein, demonstrated that this SMO inhibitor was well tolerated in pediatric patient with recurrent or treatment-refractory medulloblastomas. 110 Incorporating this type of targeted therapy into multimodal treatment planning may allow further reduction of radiation dose and cytotoxic chemotherapy with subsequent mitigation of the negative sequelae of treatment and improved quality of life for medulloblastoma survivors. Although our understanding of the biology of medulloblastomas has evolved considerably in recent years, these advances in molecular pathology have yet to be incorporated into the treatment of medulloblastoma.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.