
Abstract
Although neuropsychological studies have demonstrated specific cognitive impairments in children with childhood absence epilepsy (CAE), the potential role of the frontal lobe in these cognitive deficits remains unclear. We therefore evaluated cognitive functions related to and unrelated to the functionality of the frontal lobe in childhood absence epilepsy patients and control subjects. Thirty-seven childhood absence epilepsy patients and 37 age- and gender-matched healthy control subjects were recruited and assessed using a computerized neuropsychological test battery. Childhood absence epilepsy patients, especially a drug-naïve subgroup, showed cognitive deficits in reasoning, visual attention, and executive function, which are typical cognitive functions of the frontal lobe. In contrast, treated childhood absence epilepsy patients only exhibited cognitive deficits in visual attention. There were no significant between-group differences for other cognitive tests. Our findings suggest that frontal lobe–related cognitive deficits represent the characteristic neuropsychological profile associated with childhood absence epilepsy.
Childhood absence epilepsy is an idiopathic generalized epilepsy syndrome that constitutes approximately 8% of preschool and school-age child epilepsy cases. 1 Childhood absence epilepsy is clinically characterized by frequent staring spells and generalized 3-Hz spike-wave discharges on electroencephalography (EEG). 2 Although childhood absence epilepsy has historically been considered to be a benign disorder, children affected by childhood absence epilepsy often suffer neurocognitive deficits. Indeed, neuropsychological studies of childhood absence epilepsy patients have reported cognitive deficits in visual-spatial skill, 1 attention, 3 verbal memory, 4 executive function, 5 and motor control. 6 Patients with absence epilepsies also have greater psychosocial difficulties in terms of academic-personal and behavioral skills. 7,8 In particular, attention and executive function may be prominently impaired in childhood absence epilepsy patients, even when seizures are adequately controlled with medication. 9,10 One report suggested that childhood absence epilepsy patients treated with valproic acid had impairments in planning tasks, phonological and categorical fluency, and sustained and divided attention. 11 Another study of 24 children with childhood absence epilepsy reported marked impairments in components of attention such as alertness, divided attention, impulsivity, and selective attention. 12 Moreover, functional magnetic resonance imaging (fMRI) of a childhood absence epilepsy patient during a sustained attention task revealed impaired functioning of the attention network involving the frontal operculum and medial frontal cortex. 13
Some researchers have suggested that the underlying epileptogenic mechanism of absence seizures selectively involves the frontal cortical circuits. 14,15 Video-electroencephalography has been used to confirm that characteristic generalized 3-Hz spike-wave discharges in childhood absence epilepsy can be attributed to activity in the frontal lobe. 16 Magnetic resonance imaging (MRI) studies exploring the localization of generalized spike-wave discharges in childhood absence epilepsy patients have reported significantly smaller gray matter volumes in the frontal gyrus relative to control subjects. 17 Additionally, it is known that blood oxygen level–dependent (BOLD) responses peak in the prefrontal and dorsolateral cortices after the onset of absence seizures. 18 Other research has confirmed that childhood absence epilepsy patients have significantly increased resting interhemispheric functional connectivity in the lateral orbitofrontal cortex relative to normal control subjects. 19
The frontal lobes play important roles in attention, executive function, and fluid intelligence. 20 -22 These findings, together with the concurrent observation of both frontal lobe dysfunction and core deficits in attention and executive function in childhood absence epilepsy patients, suggest that cognitive deficits in childhood absence epilepsy may be associated with changes in the frontal lobe. However, no study to date has established these deficits as typical of childhood absence epilepsy by evaluating other cognitive deficits not classically associated with the frontal lobe in childhood absence epilepsy patients. The present study thus employed a computerized cognitive test battery to evaluate the various cognitive abilities of children with childhood absence epilepsy, with a focus on attention, executive function, and fluid intelligence. We first hypothesized that neurocognitive dysfunction in childhood absence epilepsy patients would be associated with frontal lobe functionality, and secondly compared the performance of childhood absence epilepsy patients and controls in cognitive tests associated and not typically associated with frontal lobe functionality.
Methods
Participant Selection
This study recruited 37 childhood absence epilepsy patients (15 males and 22 females) from the Department of Pediatric Neurology at the Capital Institute of Pediatrics. The mean age at the time of testing was 8.0 years (range 5-15 years) and the average age of onset was 6.2 years (range 4.1-9.4 years). Children with childhood absence epilepsy were selected based on the following criteria: (1) a diagnosis according to the epileptic classification of the International League Against Epilepsy (frequent daily manifestation of absence seizures as a brief consciousness disorder with or without automatism) 23 and (2) the presence of normal background and 2.5- to 3.5-Hz generalized spike-wave discharges on EEG during hyperventilation-induced seizures. Exclusion criteria included (1) the manifestation of any other seizure type, including tonic-clonic, myoclonic, and partial seizures; (2) any brain MRI abnormality or other neurologic disease; and (3) an inability to complete the experimental tasks independently. At the time of testing, 15 of 37 patients were newly diagnosed and drug-naïve and 22 patients were on antiepileptic drug therapy. Of the patients receiving therapy, 20 patients were receiving monotherapy (valproic acid = 17-20 mg/kg/d or clonazepam = 0.02-0.04 mg/kg/d) and 2 patients were receiving polytherapy. In terms of antiepileptic drug treatment duration, 8 patients were treated for less than 12 months, 5 patients were treated for 12 to 24 months, and 9 patients were treated for more than 24 months. The control group included 37 healthy participants (15 males and 22 females) who were recruited from a local primary school in Beijing. The mean age at the time of testing was 8.5 years (range 5-15 years). Childhood absence epilepsy patients and control subjects were matched according to age and gender. Approval for this project was granted by the Human Research Ethics Committees at the Capital Institute of Pediatrics. Written informed consent was obtained from the parents of all subjects prior to participation.
Computerized Test Battery
The neuropsychological assessment battery included 10 cognitive tests. Three tests including Raven’s Progressive Matrices, visual tracing, and the Wisconsin Card Sorting Test were used to evaluate cognitive functions associated with the frontal lobe. Raven’s Progressive Matrices was used to measure basic fluid intelligence or reasoning. Visual tracing was used to measure visual attention. Finally, the Wisconsin Card Sorting Test was used to assess executive function (response inhibition and mental flexibility). Other control cognitive tests included choice reaction time, number magnitude comparison, mental rotation, simple subtraction, word semantics, paired associative learning, and word rhyming.
All tests were programmed using web-based applications from the Online Experimental Psychological System (OPES) (www.dweipsy.com/lattice). 24 For all but 2 tests, responses were indicated by pressing 1 of 2 keys (P or Q) on a standard computer keyboard; for visual tracing and the Wisconsin Card Sorting Test, responses were indicated by mouse click. Participant responses were automatically recorded to an online server.
Raven’s Progressive Matrices
A simplified version of the Raven’s Progressive Matrices test 25 was used to assess general intelligence. For this task, participants were asked to identify the missing segment that would complete a figure’s pattern. Two candidate answers were presented side-by-side beneath each problem; participants were instructed to press Q if the missing segment was on the left and P if it was on the right. The test was time-limited (3 minutes) and consisted of 80 trials.
Visual tracing
The visual-tracing task was adapted from Groffman’s visual-tracing test. 26 Several curved lines were interweaved with one another in a square, starting from the left side and ending on the right. Participants were asked to track a particular line from beginning to end using only their eyes (ie, the use of a finger or cursor was prohibited) and to mark the correct end point. The degree of difficulty (ie, the number of lines) increased from trial-to-trial. There were 12 pictures used in each of 3 trials. This task was also time-limited (4 minutes).
Wisconsin Card Sorting Test
The Wisconsin Card Sorting Test was adapted from the manual version, 27 which is one of the most widely used tasks to assess executive function. 26 The task contained stimulus cards and response cards, and participants were instructed to flip over and match the response card to one of the stimulus cards according to one of 3 principles (ie, color, form, and quantity). There were 4 stimulus cards with the following symbols: (1) a red triangle, (2) 2 green stars, (3) 3 yellow crosses, or (4) 4 blue circles. During the test, participants were asked to guess the sorting principle on the basis of face feedback (a smiling face indicated positive feedback and a sad face indicated negative feedback) after each response. This task was time-limited (20 minutes).
Choice reaction time
For each trial, a white dot was presented on a black screen to the left or right of a fixation cross. The position of the dot was within 15 degrees of the visual angle from the cross. Participants were asked to press the Q key if the dot appeared on the left and the P key if it appeared on the right. There were 30 trials in total presented in a random order (15 trials with the dot on the left and 15 trials with the dot on the right). The size of the screen on which the dot appeared varied randomly across trials. The interstimulus interval varied randomly between 1500 and 3000 milliseconds. This task was used to measure response speed.
Number magnitude comparison
The number magnitude comparison task was adapted from a number-comparison test used in previous research. 28 Eighty-four pairs of single-digit Arabic numbers of varying sizes were presented in a random order. For each pair, participants were asked to indicate the number of larger numerical magnitude while ignoring differences in the physical sizes of the numbers. Participants pressed the Q key to choose the answer on the left and the P key to choose the answer on the right. The magnitudes of the numbers were congruent, incongruent, or neutral with respect to physical size (eg, if the pair of numbers was 3-8, the 3 could be physically smaller, larger, or the same size as the 8). In pairs of differently sized numbers, the ratio of the physical size of the 2 numbers was 1:2. The number-comparison test consisted of 3 sessions (28 trials per session) that were separated by two 30-second rest periods. This task evaluated numerical processing.
Mental rotation
The mental rotation task was adapted from the mental rotation task used by Vandenberg and Kuse. 29 For each trial, a 3-dimensional image was presented on the upper half of the screen whereas 2 more were presented on the lower half of the screen. Participants were asked to choose the image from the bottom of the screen that matched the image at the top. The matching image could only be identified by using mental rotation, whereas the nonmatching image was a rotated mirror image of the target. The rotation angles of the matching images ranged from 15° to 345° (interval, 15°). Participants pressed the Q key to choose the image on the left and the P key to choose the image on the right. The mental rotation test consisted of 180 trials. This test was time-limited (3 minutes) and evaluated spatial perception.
Simple subtraction
A total of 92 simple mathematical subtraction problems were presented. The minuends were 18 or smaller, and the differences were single-digit numbers. Two candidate answers were presented beneath each problem. Participants were asked to press the Q key to choose the answer on the left and the P key to choose the answer on the right. For this task, each incorrect candidate answer was within the range of the correct answer plus or minus 3 (ie, ±1, ±2, or ±3). This task was time-limited (2 minutes) and was used to evaluate mathematical ability.
Word semantics
This task was similar to one used in previous research. 30,31 Materials in the task were adapted from textbooks used in primary schools from first grade to ninth grade. In each trial, a sentence missing one word was presented in the middle of the computer screen. Participants were asked to complete the sentence by selecting one of 2 candidate words presented beneath the sentence by pressing the Q key or the P key. The stimulus remained on the screen until participants responded. This task evaluated language ability.
Paired associative learning
The paired-associative learning task required the pairing of 2 items, with the first as the stimulus and the second as the response. Previous studies have shown that paired-associative learning is related to memory and learning ability. 32,33 We formed pairs using 2-character nouns and Arabic numbers, such as “天#空→季节” (tian#kong→season) and 9#3→2 8 (nine#three→two eight). Participants were first asked to try and memorize 15 word pairs and 15 number pairs. Each pair was presented for 10 seconds in the middle of the screen during the learning stage. During the test stage, participants were asked to indicate by key press whether pairs were the ones that they had seen in the learning stage. Each trial lasted 3 seconds. The learning and test stages were repeated after the first series, and the percentage of correct answers in the second test was analyzed. This task evaluated memory and learning ability.
Word rhyming
The task was similar to the word rhyming task used by Tan et al. 34 Two Chinese characters were presented simultaneously on the screen and participants were asked to judge whether the 2 characters rhymed by pressing the P key or the Q key. The stimuli remained on the screen until participants responded or until 4 seconds had elapsed. This task evaluated language ability.
Testing Procedure
The computerized test battery was administered to participants during two 45-minute sessions in an examination room. For each test, instructions were given and followed by a practice session. The practice session for each task consisted of either 4 or 6 trials that were similar to those used in the formal test. Computer feedback was provided after each practice trial. For all tests, the feedback for a correct response was “Correct! Can you go faster?” and the feedback for an incorrect response was “It is wrong. Try again.” Participants were allowed ask questions during the practice session. After completion of the practice session and any questions, participants were invited to press any key to begin the formal test.
Tests were administered in the same order for all participants. Each participant was monitored by one tester who was familiarized with and trained regarding standardized testing procedures.
Statistical Analysis
Both the childhood absence epilepsy group and the control group completed all tests. For all but 1 test (ie, the choice reaction time test), corrected scores were calculated to control for the effect of guessing by subtracting the number of incorrect responses from the number of correct responses. 35 -38 For the choice reaction time test, each participant’s median reaction time was calculated. Independent sample t-test analyses were conducted to compare performances between the childhood absence epilepsy group and the control group for all tests. Epilepsy-related clinical variables such as type of antiepileptic drug treatment (drug-naïve vs antiepileptic drug–treated) and duration of antiepileptic drug treatment were also analyzed. An analysis of variance (ANOVA) was conducted to test differences between childhood absence epilepsy groups according to type of antiepileptic drug treatment and the control group, with post hoc pairwise analyses using the Bonferroni correction. Differences in the duration of antiepileptic drug treatment were analyzed using the Kruskal-Wallis test (with chi-square values).
Results
Population Characteristics
The demographic and neurologic characteristics of participants are summarized in Table 1. No differences between the childhood absence epilepsy and control groups were found with respect to age (F = 0.63, P = .44) or gender (χ2 = 0, P = 1.00). Similarly, no significant differences were observed among drug-naïve, antiepileptic drug–treated, and control participants with respect to age (F = 1.63, P = .20) or gender (χ2 = 1.71, P = .43). Lastly, there were no significant differences among childhood absence epilepsy patients with different durations of antiepileptic drug treatment and controls according to age (F = 1.01, P = .40) or gender (χ2 = 1.06, P = .79).
Demographic and Neurologic Characteristics of Participants.
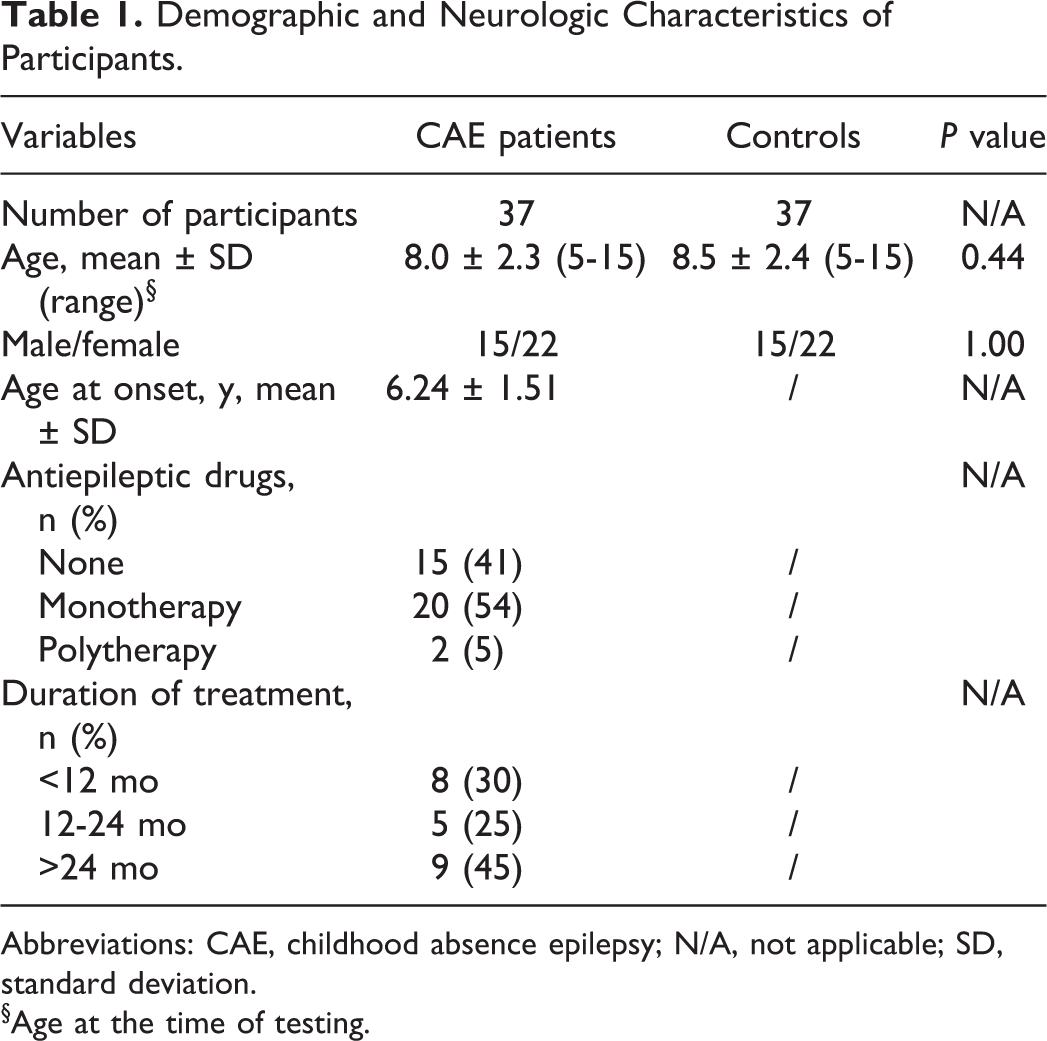
Abbreviations: CAE, childhood absence epilepsy; N/A, not applicable; SD, standard deviation.
§Age at the time of testing.
Neurocognitive Profiles
Group means and standard deviations for all test scores are summarized in Table 2. The childhood absence epilepsy group showed poorer performance than the control group on 4 tests: choice reaction time (t = −2.36, P < .05), Raven’s Progressive Matrices (t = −2.87, P < .01), visual tracing (t = −4.43, P < .001), and the Wisconsin Card Soring Test (t = −2.98, P < .01). No significant between-group differences were found for other tests.
Means (SD) and Independent Sample t-Test Analyses of Cognitive Test Scores in CAE Patients (n = 37) and Control Subjects (n = 37).
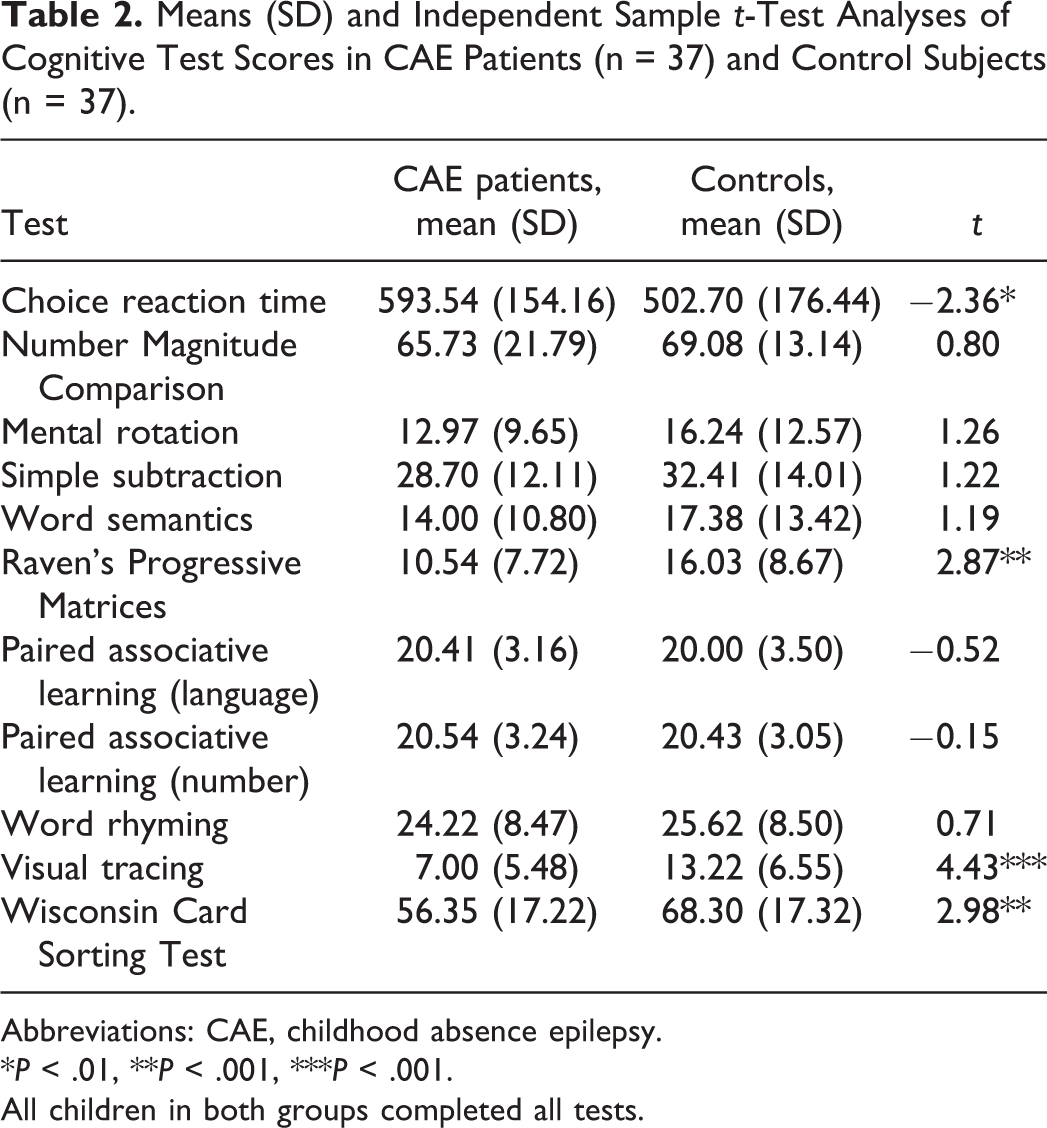
Abbreviations: CAE, childhood absence epilepsy.
*P < .01, **P < .001, ***P < .001.
All children in both groups completed all tests.
Significant main effects of antiepileptic drug treatment type were identified for Raven’s Progressive Matrices (F = 4.37, P < .05), visual tracing (F = 9.67, P < .001), and the Wisconsin Card Sorting Test (F = 4.67, P < .05) (Table 3). Further analyses indicated that the drug-naïve childhood absence epilepsy subgroup performed more poorly than the control group on Raven’s Progressive Matrices, visual tracing, and the Wisconsin Card Sorting Test (all P < .05). Alternatively, the antiepileptic drug–treated childhood absence epilepsy subgroup only performed poorly on visual tracing relative to the control group (P < .05). There were no significant differences between drug-naïve childhood absence epilepsy subgroup and antiepileptic drug–treated childhood absence epilepsy subgroup. No significant between-group differences were found according to the duration of antiepileptic drug treatment.
Means (SD) and Statistical Analysis of Epilepsy-Related Clinical Variables for Participants.
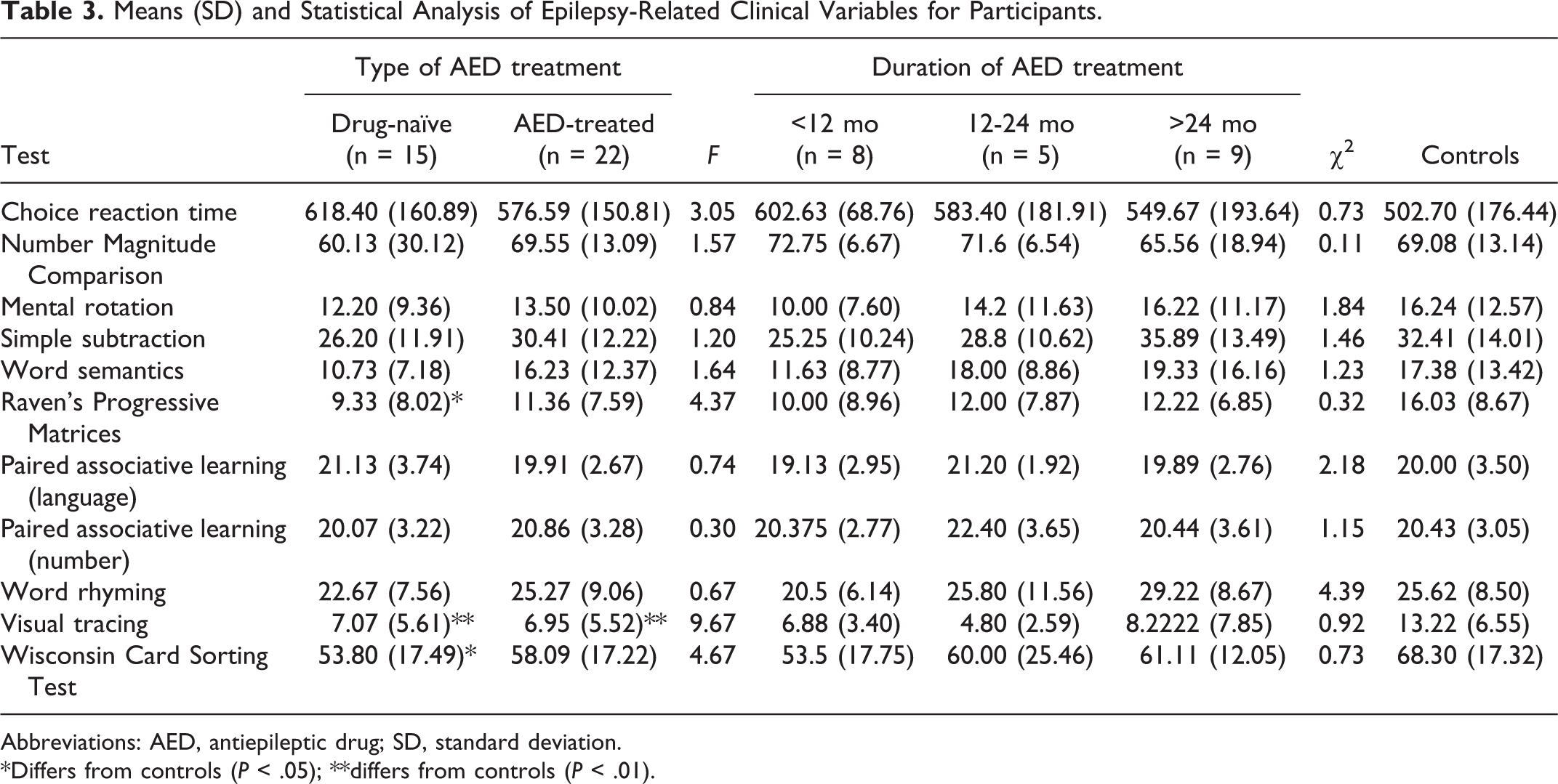
Abbreviations: AED, antiepileptic drug; SD, standard deviation.
*Differs from controls (P < .05); **differs from controls (P < .01).
Discussion
In the present study, we applied a battery of computerized cognitive tests to compare the cognitive function of childhood absence epilepsy patients with that of age- and gender-matched control participants. Our results demonstrated that children with childhood absence epilepsy had deficits in cognitive functions related to the frontal lobe such as fluid intelligence, visual attention, and executive function. Further analysis showed that drug-naïve childhood absence epilepsy patients exhibited deficits in cognitive domains including of fluid intelligence, visual attention, and executive function, whereas childhood absence epilepsy patients receiving antiepileptic drug treatment only showed impairments in visual attention. Importantly, deficits were not detected in processing speed, numerical processing, spatial perception, language processing, memory, or learning ability. These results suggest that children with childhood absence epilepsy have a distinct pattern of neurocognitive dysfunction that relates to the functionality of the frontal lobe. Furthermore, this specific series of deficits may represent the typical neuropsychological profile associated with childhood absence epilepsy, and the aspects of this profile that are sensitive to antiepileptic drug therapy.
The role of the frontal cortex in high-level cognition and academic achievements is well supported by evidence from lesion and neuroimaging studies. 39 For example, frontal lesions impair fluid intelligence in patients. 40 To this end, studies of brain development indicate that the level of fluid intelligence is associated with the trajectory of cortical development, primarily in frontal regions implicated in the maturation of intelligent activity. 22 The frontal cortex is also thought to support visual attention and executive function via processes including attentive tracking and cognitive control. Bilateral activation of the frontal cortex (the frontal eye fields and precentral sulcus) occurs during attentive tracking versus passive viewing. 21 Additionally, the Wisconsin Card Sorting Test has been reported to produce widespread activation of the frontal lobe, and similarly, impairments in performance on this test have been reported following frontal lobe damage. 20 Our data are consistent with these previous reports: impairments in fluid intelligence, visual attention, and executive function in childhood absence epilepsy patients fully reflected the compromised functionality of the frontal lobe in our study. In contrast, other cognitive abilities not directly related to the frontal lobe (ie, processing speed, numerical processing, spatial perception, language processing, memory, and learning ability) were unaffected by childhood absence epilepsy. 41 -45 As childhood absence epilepsy patients have been reported to have network impairments involving the frontal operculum and medial frontal cortex, 14,19 neurocognitive dysfunction related to frontal lobe may be due to neural network abnormalities.
A comparison of drug-naïve childhood absence epilepsy patients, childhood absence epilepsy patients receiving antiepileptic drug treatment, and age/gender-matched controls revealed that cognitive functions related to the frontal lobe were especially impaired in newly diagnosed, untreated subjects. In contrast, both drug-naïve childhood absence epilepsy patients and those receiving antiepileptic drug treatment showed deficits in visual attention. Although childhood absence epilepsy patients have consistently demonstrated impairments despite adequate seizure control in previous studies, 9,46 our data suggest that some impairments may in fact be sensitive to antiepileptic drug therapy, independent of treatment duration. The present study thus extends previous neuropsychological findings by confirming the presence of frontal lobe-related cognitive deficits as characteristic of children with childhood absence epilepsy. We conclude that the cognitive function of the frontal lobe may play an important role in childhood absence epilepsy pathology as well as neuropsychology. Future neuropsychological assessment studies using larger cohorts are required to validate our findings and further improve the current understanding of absence epilepsy.
Footnotes
Acknowledgments
We thank Jike Qin for her helpful comments.
Author Contributions
DZC and QC conceived and designed the study. ZJG and XLZ acquired the data and KMX and XLZ analyzed and interpreted the data. DZC and QC drafted the manuscript. XXY, KMX, and XLZ critically revised the manuscript for important intellectual content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Beijing Excellent Talents program (2014000021469G227) and the Cultivation Plan Fund for the Capital Institute of Pediatrics (PY-15-02) and Beijing Municipal Administration of Hospitals’ Youth Programme (QML20151202) to DZC, as well as a grant from the Beijing Municipal Science and Technology Commission (Z131107002213027) and the Capital Health Research and Development of Special (2016-2-2103) to QC.
Ethical Approval
Approval for this project was granted by the Human Research Ethics Committees at the Capital Institute of Pediatrics (SHERLL 2015023).