
Abstract
This study aimed to know how frontline physicians in France, Belgium, and Switzerland implement guidelines regarding the secondary prevention of childhood arterial ischemic stroke and to introduce physicians’ point of view on a clinical trial assessing the efficacy of aspirin as a preventive strategy. The authors conducted an online survey directed at specialists throughout dedicated networks and used a mixed method for data analysis. Overall, 63 physicians responded, and 88% prescribe aspirin when sickle cell disease, cardio-embolic stroke, and dissection of cervical arteries are excluded. Prescribing habits vary among respondents with respect to their specialty. A majority would choose placebo or a treatment given to historical controls to compare with an aspirin arm in a trial. In studied countries, there seems to be good adherence to guidelines regarding the secondary prevention of childhood stroke. A trial assessing the efficacy of aspirin could be well accepted if several factors regarding study design were taken into account.
Arterial ischemic stroke is rare during childhood. For example, in France, it could strike 140 to 280 children every year. 1 As the outcome might be lifelong, the socioeconomic burden continues to grow. 2 International guidelines for the management of childhood arterial ischemic stroke have already been published and, except for sickle cell disease, are mostly based on consensus and low-level evidence. 3 –5 Hence, there is a need to assess the effectiveness of current and future management strategies. 6
The objective of this study was, first and foremost, to know how European French-speaking frontline physicians are implementing childhood arterial ischemic stroke secondary prevention guidelines. The second objective was to gather their opinion with respect to the feasibility of a clinical trial assessing the efficacy of aspirin for the secondary prevention of childhood arterial ischemic stroke.
Materials and Methods
We conducted a community online survey from June 2015 to October 2016, using Survey Monkey as a Web-based tool. We included among those invited to participate physicians potentially involved in the frontline management of childhood arterial ischemic stroke. We contacted European specialists from French-speaking countries (France, Belgium, and Switzerland) using the mailing lists of existing national stroke/pediatric neurology networks. In France, for example, we approached pediatric neurologists, neurologists, neurosurgeons, and general pediatricians through discussion groups and/or Special Interest Groups, as well as several associations for childhood neurovascular disorders. The first European Pediatric Stroke Symposium held in Saint-Etienne, France, in September 2016, was an occasion to extend this network. We sent e-mail messages with a hyperlink to the questionnaire (both English and French versions), whose estimated completion time was of 10 minutes. The survey form was designed to include a combination of 11 questions, closed and open ended, as well as multiple and single choices. The full survey is available as supplemental data. The questionnaire presented a typical arterial ischemic stroke case of a 5-year-old girl with infarction in the right deep medium cerebral territory (lateral lenticulostriate artery) and was supported by 2 magnetic resonance images (MRIs) as shown in Figures 1 and 2. Respondents were divided according to the following categories: pediatric neurologists, neurologists, pediatricians, and others. We guaranteed participant anonymity through appropriate wording in our correspondence and within the survey form. We analyzed data using descriptive statistics where variables were categorical and nominal. We compared answers between physicians of different specialties using Fisher exact test. 7 With respect to question 5, where a verbal answer was provided, we used thematic analysis and classified participants’ responses into various categories. This survey was approved by the institutional review board of the Saint-Étienne Hospital.
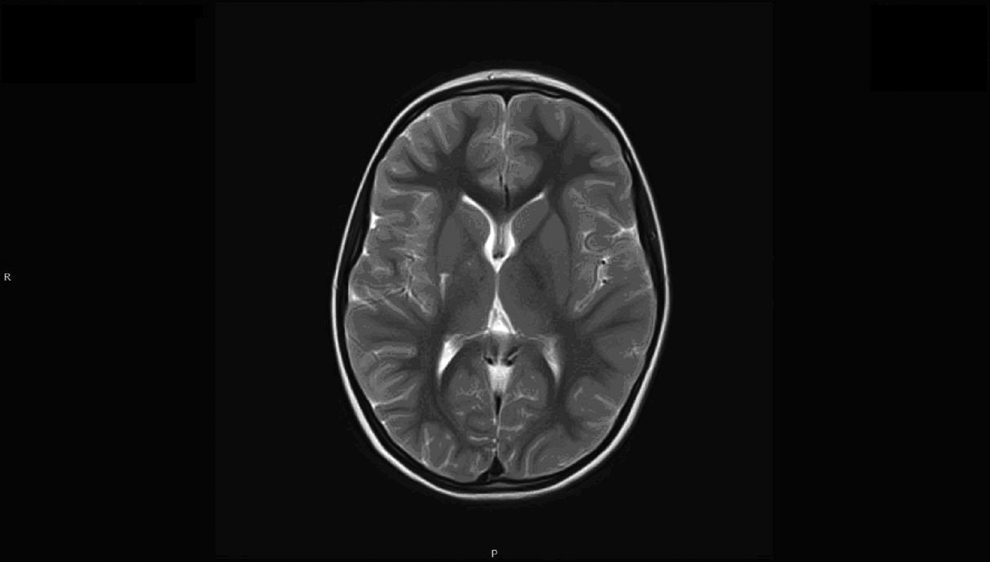
T2-weighted axial magnetic resonance imaging (MRI) showing infarct in the right lenticulostriate territory.
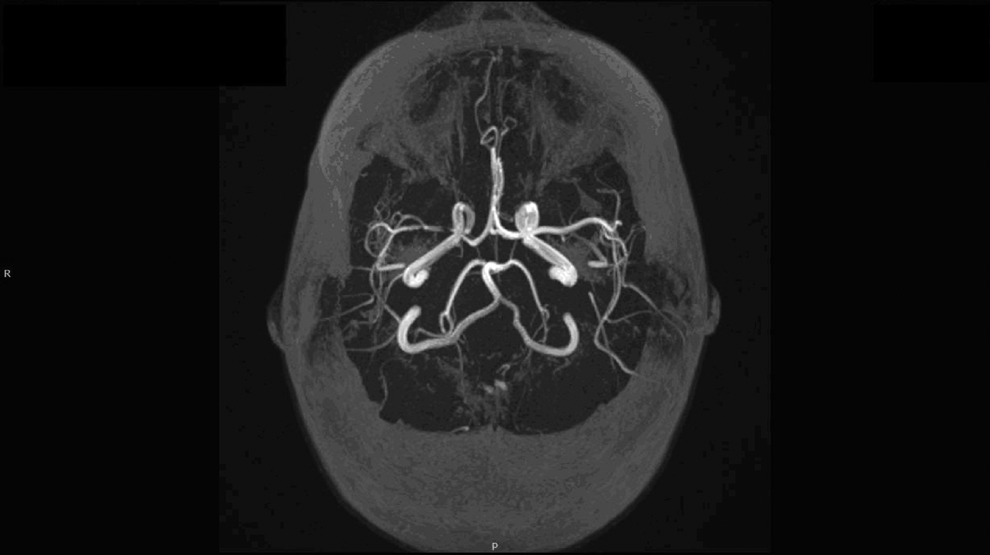
Time-of-flight magnetic resonance imaging (MRI) showing stenosis of right terminal part of internal carotid artery and proximal part of medium cerebral artery.
Results
We sent 1250 e-mail messages at the start of the study, and 59 more e-mails later on, with several recalls. A total of 63 physicians completed the questionnaire, which held a 4.8% response rate. Fifty-two participants (82%) responded to all questions. Participating physicians were categorized as follows: 26 pediatric neurologists (41%), 16 neurologists (25%), 6 pediatricians (9%), 4 others (6%), and 11 (17%) respondents did not specify their specialty.
Treatment of Arterial Ischemic Stroke in the Super-Acute Phase
Most physicians (44/63, 70%) treated with oral aspirin alone or in association with heparin (5 cases). When heparin was chosen, it was mainly low molecular weight (13/63, 21%). Pediatric neurologists and general pediatricians (15/32) treated more often with heparin than neurologists (2/16, P = .02). Neurologists (15/16) prescribed more often aspirin alone than pediatric neurologists and general pediatricians (17/32, P < .01) (Figure 3).
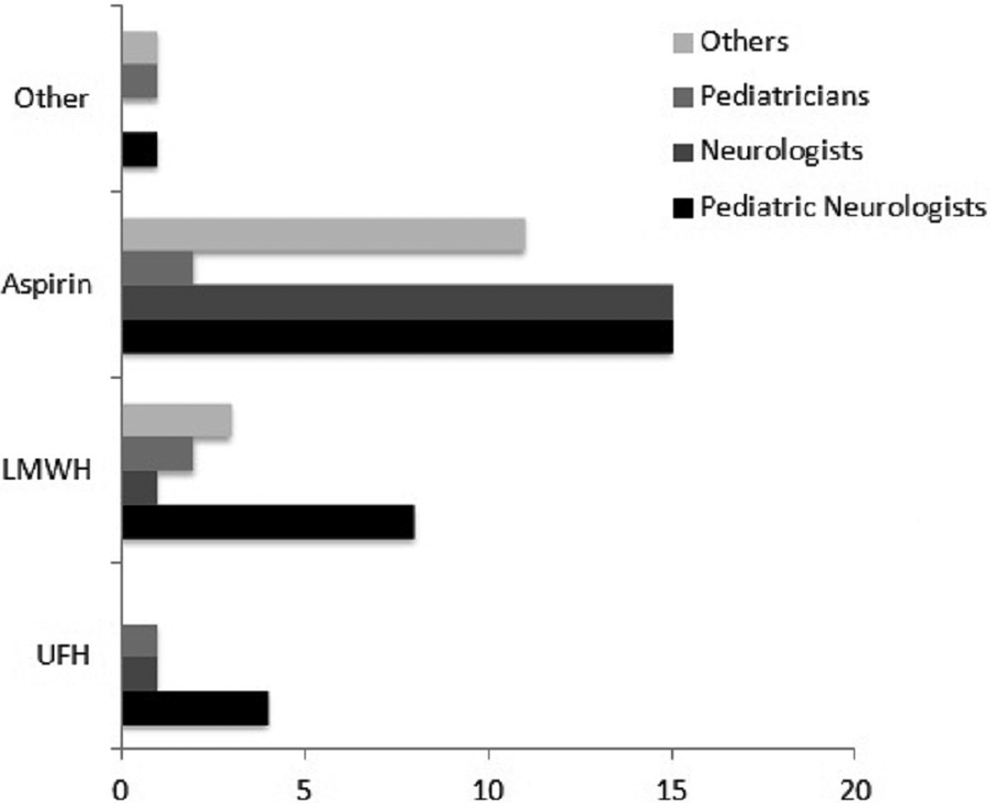
Histogram showing number of responses to question 1 (treatment in the super-acute phase of childhood arterial ischemic stroke) in function of physician specialty (total responders n = 63). LMWH, low-molecular-weight heparin; UFH, unfractionated heparin
Treatment of Transient/Focal Cerebral Arteriopathies 8
When transient cerebral arteriopathy was highly probable (as in our clinical vignette), and cardioembolism or dissection had been ruled out, 88% (53/60) of physicians prescribed aspirin alone. Only 2 pediatric neurologists treated with low-molecular-weight heparin, whereas all neurologists went for aspirin. Two physicians with unknown specialty and 1 pediatric physical therapist added steroids to aspirin.
Transient Cerebral Arteriopathy and Stuttering Presentation
When clinical signs of ischemic stroke had a stuttering presentation on a short-relapsing course (without new infarction on brain imaging), 62% (37/60) of surveyed physicians changed their treatment. This attitude was not statistically different between pediatric neurologists and neurologists, whereas general pediatricians had a tendency to maintain aspirin.
Treatment Modification in Case of a Stuttering Presentation
All physicians who decided to modify their treatment (n = 37) had initially prescribed oral aspirin alone (except in 1 case with a combination of aspirin and steroids). When treatment was switched (29/37, 78%), it was generally switched to low-molecular-weight heparin (14 cases), unfractionated heparin (UFH, 5 cases), clopidogrel (5 cases), or vitamin K antagonists (VKA, 4 cases). Some physicians (7/37, 19%) added other treatments to aspirin, mainly low-molecular-weight heparin or clopidogrel. Most pediatric neurologists chose low-molecular-weight heparin (switch or add-on, 14/18 vs 1/10, P < .01), whereas neurologists went for clopidogrel (switch or add-on, 6/10 vs 1/18, P < .01). Only 2 physicians added steroids.
Criteria for Discontinuing Treatment in Transient Cerebral Arteriopathy
This question had the lowest response rate (52/63, 82%). Most responders (19/52, 36%) relied on radiologic criteria alone (disappearance of cerebral arteriopathy in 12 cases, nonprogression in 7 cases) to discontinue treatment. Eleven physicians used a combination of clinical and radiologic criteria to stop treatment (usually, absence of stroke recurrence and no progression of arteriopathy). Seven others relied solely on a good clinical outcome, whereas 5 others treated for a certain period of time without further precision. Seventeen responders (33%) proposed a treatment duration that varied between 6 and 24 months. In comparison to their counterparts, pediatric neurologists more often considered nonprogression of cerebral arteriopathy (9/22 vs 2/22, P = .03) in the treatment discontinuation process.
Chosen Comparator to Aspirin in an Arterial Ischemic Stroke Secondary Prevention Trial
A majority of physicians would have chosen placebo (17 cases) or historical controls (19 cases) to compare with aspirin for the secondary prevention of arterial ischemic stroke. Responses did not statistically significantly vary between specialties. One physician answered that such a trial is questionable given the fact that stroke treatment depends upon its cause.
Chosen Comparator to Aspirin in a Transient Cerebral Arteriopathy Secondary Prevention Trial
Most physicians would have chosen placebo (17 cases) or historical controls (16 cases) to compare with aspirin. There was no statistically significant difference in the choice for placebo between neurologists (5/16) and pediatric neurologists (11/26). Only 5 physicians would have chosen aspirin + steroids versus aspirin alone (Figure 4).
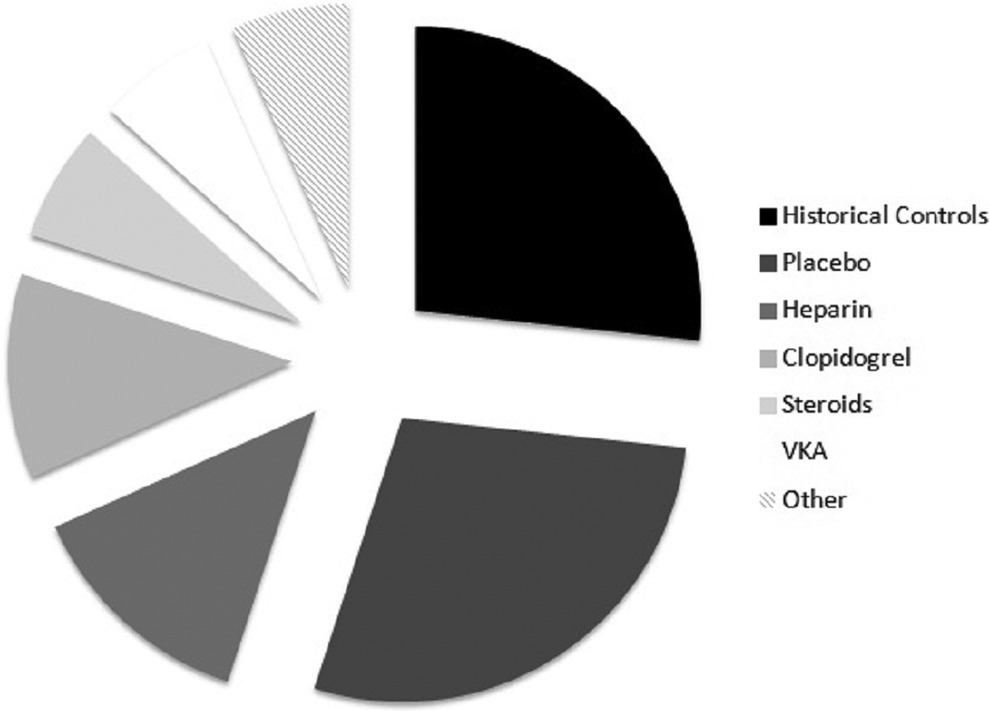
Diagram showing number of responses to question 7 (preferred comparator in an aspirin trial for secondary prevention of transient cerebral arteriopathy, total of responders n = 52).
Treatment of Ischemic Stroke Related to Dissection
Seventy percent (35/50) of physicians would treat stroke related to cervical artery dissection with anticoagulants or a combination of aspirin and another agent, with only 30% choosing aspirin alone (15/50). Answers did not significantly differ between pediatric neurologists and pediatricians on one side and neurologists on the other.
Factors Preventing Recruitment in a Transient Cerebral Arteriopathy Secondary Prevention Trial
For a majority of responders (29/52, 56%), the context of emergency in which arterial ischemic stroke occurs represented a barrier to recruitment. In second position came the emotional burden surrounding stroke diagnosis (22/52, 42%), and in third, lack of time to inform families before consent to participate (15/52, 29%). They also considered that the trial’s protocol design should not overload clinicians with more tasks than what they usually perform on a routine basis (14/52, 27%). Absence of one of the parents at consent was of less concern (9/44, 20%). Compared to pediatric neurologists, neurologists were of the opinion that the emotional burden surrounding diagnosis (10/16 vs 9/26, P = .11) and absence of child assent (3/16 vs 0/26, P = .04) were limiting factors. On the other hand, pediatric neurologists and pediatricians paid more attention to the study protocol burden and to the emergency setting of childhood arterial ischemic stroke, although this did not turn out to be statistically significant.
Participation in a Secondary Prevention Trial
Most responders (44/51, 86%) would have liked to be involved in a childhood arterial ischemic stroke secondary prevention trial, with a significant difference between pediatric neurologists and other physicians (26/26 vs 18/23, P = .02).
Discussion
Our study may suggest that in 2015, in France, Belgium, and Switzerland, physicians potentially involved in the secondary prevention of childhood arterial ischemic stroke usually follow international guidelines. Furthermore, it seems that a transient cerebral arteriopathy secondary prevention trial comparing aspirin to another comparator (mainly placebo or historical controls) would be well accepted if several limiting factors (from the clinicians’ point of view) were taken into account.
When a child is diagnosed with arterial ischemic stroke, antithrombotic treatment is usually promptly started while first investigations try to identify the cause. British guidelines published in 2004 recommend the use of 5 mg/kg oral aspirin, whereas in 2008 and 2012, Northern American publications consider the use of heparin or aspirin until cardioembolic and dissection subtypes are excluded. 5,9 In the present survey, a majority of physicians would use aspirin alone, heparin alone or a combination of both. Interestingly, neurologists seem more prone to treat with aspirin alone even when cardioembolic causes and dissection remain of possible concern. Presentation of our clinical vignette, showing a typical case of transient cerebral arteriopathy, might have biased answers to the first question, resulting in less reluctance to prescribe aspirin. Furthermore, the use of antiplatelet agents as a stroke secondary prevention strategy is now well established in the adult stroke medical culture worldwide. 10 Fear of intracranial bleedings (much more frequent in adult patients than during childhood) could also play a role, and published literature supports the use of anticoagulation in children because it has proved to be safe and not superior to antiplatelet treatment. 4,11 Notwithstanding this, pediatric neurologists prescriptions in our survey stay in line with published class II-C recommendations, and the use of aspirin as a secondary prevention treatment of transient cerebral arteriopathy seems widely adopted. 4,5,9 However, we do not know if this is linked with a good adherence to published guidelines, or a slow transmission of an “aspirin prescribing habit” from the adult neurology world to the pediatric one, a process that may have started prior to publication of the first guidelines. 12
Published data show that fluctuating and recurring mode of onset of index stroke (what we call a stuttering presentation) is common in transient and postvaricella cerebral arteriopathy. 13 –15 Transient ischemic attacks might also occur in the first week poststroke. 15 Our survey showed that in such situations, frontline physicians are very likely to change their patient’s treatment, although infarct recurrence has not been evidenced on repeat brain imaging. This is of crucial importance in a trial enrolling patients soon after index stroke and might cause failure to comply with treatment protocol. Therefore, optional treatments should be anticipated in order to keep children in. Preference for clopidogrel among neurologists could be furthermore explained by recent evidence that dual antiplatelet therapy could be a preferable choice to prevent stroke in adult patients who have had a previous stroke or transient ischemic attack. 16 However, to date, clopidogrel has only been the subject of safety and tolerance studies in the pediatric population, and is not recommended to prevent stroke. 17
Discontinuation of treatment in transient cerebral arteriopathy is another important issue that has never reached consensus in the childhood stroke community. Thus, it is not surprising that answers come so disparate in the present survey. Transient cerebral arteriopathy being a childhood-specific entity, pediatric neurologists express predictably enough concern for nonprogression of cerebral arteriopathy. Moreover, they would probably feel comfortable for a 6 to 18 months’ treatment duration in a secondary prevention trial.
In such a trial, it is nothing less than perplexing that many responders would choose a placebo to compare with aspirin. Indeed, some data might indicate that before aspirin was introduced in the treatment of transient cerebral arteriopathy, recurrence rates might have been as high as 20%. 18,19 Therefore, equipoise would probably not be reached among neurovascular pediatricians and placebo could be judged unethical. Nonetheless, our results indicate that acceptance of an aspirin versus placebo trial might not be as low as expected. Use of placebo is deeply embedded in our scientific psyche as a seemingly experimental scheme, and this could partly explain our results. 20 Moreover, a third of interviewed physicians would consider comparing an aspirin arm with historical controls an option that might be useful in pediatric rare diseases although comparability between groups is of concern. 21 Interestingly, only 4 responders would choose steroids in a transient cerebral arteriopathy trial, which could mean that the inflammation theory is not shared with all physicians who deal with childhood stroke. Furthermore, this is in contrast with a recent survey conducted in Australia and Europe (Steinlin M, MD, and Mackay M, MBBS, Evaluation of arterial ischemic stroke treatment trial in childhood stroke: a Delphi process to find agreement on the study design. Personal oral communication, International Child Neurology Conference, Amsterdam, May 4th 2016). 22 Results conclude that a trial comparing aspirin and a combination of aspirin and steroids would be preferred. However, responders were only stroke-oriented pediatric neurologists involved in research, thus not reflecting the views and opinions of hands-on clinicians.
Finally, our results show that a secondary prevention trial should assess several issues in order to enhance recruitment and adherence. Consent to participate should be obtained in a reasonable time window poststroke and within a playing-down atmosphere. Enrolment and follow-up should not overload clinicians with more than what is usual. Parent’s representation and child assent should be pointed out.
First strength of our survey lies in the fact that our sample of responders is representative of the clinicians being nowadays involved in the management of childhood stroke. In France, most parents bring their child to emergency room or pediatric emergency room, in secondary or tertiary care centers, usually hospitals. 23 It is highly probable that a vast majority of children with acute strokes come first managed in the aforementioned facilities, where the frontline and on-call specialists will be, depending on the geographical location, a general pediatrician, pediatric neurologist, or neurologist (especially those working in stroke-oriented units). Decisions on investigations and treatments often rely on their first recommendations. Furthermore, it is also likely that those physicians would be the one to seek for parent’s consent to participate in a trial. This is why we aimed to know their point of view on a study design in which they would be the first concerned and involved, and we believe this to be the second strength of our work.
Limitations come from the fact that our survey sample is small, so results should be interpreted with caution. Possible barriers may have included lack of time, e-mail fatigue, limited recall, complexity of the survey, or concern about the anonymity of the responses. 24 Moreover, there’s a selection bias inherent to any online survey, responders being more likely to be intellectually involved in the management of childhood stroke than nonresponders. 25 Substantial proportion of participants declined to reveal their specialty, and this may also have biased comparisons. Finally, pediatricians were not sufficiently represented in this survey. When considering that they are truly “frontline physicians,” identifying potential stroke cases and referring them to neurologists, this inevitably limits the generalizability of our results.
To conclude, this is the first survey exploring practices of frontline French-speaking European physicians potentially confronted with childhood arterial ischemic stroke. Our results suggest that aspirin is widely adopted as a first-line treatment to prevent childhood arterial ischemic stroke recurrence, as recommended by international guidelines. They also seem to show that a secondary prevention trial aiming at proving the efficacy of oral aspirin may be not only feasible but desirable. We identified several factors that will have to be taken into account in study design in order to increase clinicians’ participation and adherence to protocol.
Footnotes
Acknowledgments
The authors thank Dr Christian Zix for the creation and management of the French-speaking Pediatric Neurology Online Talking Group (Yahoo), which helped us transmit this study.
Author Contributions
SD designed and conducted the study, analyzed the data, and drafted the manuscript. MR participated in the design of this study. JF and SL helped design this study and, along with LB and SC, reviewed the draft for content. SL helped design this study and reviewed the draft for content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the institutional review board of the Saint-Étienne Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.