
Abstract
The aim of this study was to evaluate the risk factors, clinical implications, and prognosis of new-onset seizures that occurred after pediatric liver transplantation, and to assess the efficacy of levetiracetam treatment. The clinical and laboratory data of liver transplanted 28 children who had seizures after liver transplantation and specifically of 18 children who received levetiracetam were analyzed retrospectively. Sixteen patients (88.9%) remained seizure-free and in 2 (11.1%), more than 50% reduction in seizures were detected with levetiracetam treatment. In conclusion, seizures are generally the most common complication by a spectrum of seizure types, and sometimes cause symptomatic epilepsy. The most common risk factors for seizures in transplant recipients is immunosuppressant toxicity. Currently, there isn’t a specific treatment involving the transplant patient population. Levetiracetam may be preferable in pediatric patients as it’s reliable for liver disease and has advantages in the treatment of postoperative seizures due to its intravenous usage.
Liver transplantation is now the treatment of choice for both children and adults with end-stage liver disease and acute liver failure. Neurological complications occur frequently following liver transplantation which are associated with significant mortality and morbidity, and may cause a longer stay in hospital. 1 Seizures are the most common neurological symptom after liver transplantation. 2 Although the cause of seizures after liver transplantation is usually multifactorial, the most common causes are metabolic derangements, immunosuppressive agents, hypoxic ischemic injury, cerebral structural lesions, and infections. 3
In this study, the authors evaluated the clinical course and laboratory data of pediatric liver transplantation recipients to identify the potential causes and risk factors for the onset of seizures after liver transplantation and to assess the efficacy of treatment with levetiracetam.
Materials and Method
The authors evaluated 242 pediatric patients (age < 18 years) requiring liver transplantation for different etiologies at the Inönü University Medical Center Liver Transplantation Unit from May 2006 to June 2015. Seizures were encountered in 28 patients (11.5%) after liver transplantation. The laboratory data on systemic infection, as well as function of the liver and the kidney and electrolyte levels were evaluated daily. Patients were assessed clinically and by neurologic examination, electroencephalography (EEG), and cerebral magnetic resonance imaging (MRI). EEG evaluations were performed with electrodes placed according to the international 10-20 system. EEG records were evaluated by 2 different pediatric neurologists. A follow-up EEG was routinely performed 6 months after seizure. For patients who had posterior leukoencephalopathy syndrome, a follow-up MRI was performed in 3 months after seizures.
Levetiracetam was started in 18 patients; 10 patients did not receive any treatment due to the presence of acute metabolic problems associated with seizures (hyponatremia, hypoglycemia, and hypocalcemia). Efficacy of levetiracetam was assessed in 18 patients. If seizure did not repeat and the results of the EEG were normal, levetiracetam was stopped in 6-24 months.
Statistical Analysis
Continuous variables were presented as the mean ± SD; categorical variables were presented as proportions. The chi-square test was used to compare categorical variables. The Kruskal-Wallis test and the Conover test were used for the comparison of data between groups and for comparing the pairs of groups, respectively. Statistical analyses were undertaken using SPSS version 22.0 (IBM Inc, Chicago, IL, USA). A P value < .05 was considered as statistically significant.
Results
The authors observed seizures in 28 patients (11.5%, 15 girls, 13 boys, mean age: 7.03 ± 5.47 years; range: 2 months-18 years). There was no difference in the incidence of seizures between genders (P = .2). Eleven patients had received grafts from cadaveric donors, and 17 from living donors. There was no statistically significant difference in terms of incidence of seizures between transplantation type (P = .517). The most frequent cause for liver transplantation was acute liver failure. There was no statistically significant association between the primary diagnosis and the seizures (P = .388).
All seizures occurred during the first 2 weeks after surgery (mean: 6.22 ± 3.82 days, range: 1-16 days). Twenty-one patients (75%) showed focal seizures and 7 patients (25%) showed generalized seizures. The most common etiology of seizures was the use of immunosuppressive drugs and posterior reversible encephalopathy syndrome. Six of the patients with seizures (21.4%) had concomitant posterior leukoencephalopathy syndrome and they had high blood pressure at the time of seizures. Hypertension was defined as elevated systolic or diastolic blood pressure greater than values found in the 95th percentile for the relevant age categories. The immunosuppressive regimen was based on the use of tacrolimus in 15 patients and cyclosporine in 10 patients. Four of the 6 posterior reversible encephalopathy syndrome attacks in this study were caused by tacrolimus, and 2 by cyclosporine. The patients were all afebrile, and none were on any other medications that could cause convulsions. Patients had tacrolimus levels between 4-30 ng/mL and cyclosporine between 33-250 ng/mL at the time of seizures. There was no statistically significant association between the presence of seizures and the type of immunosuppressant (P = .24). Multivariate analysis showed that the serum trough tacrolimus and cyclosporine levels were independent risk factor associated with seizures after surgery (P < .001). But according to the area under the ROC curve, tacrolimus and cyclosporine had no effect on the classification of seizure. If the patient was on tacrolimus, it was switched to cyclosporine but if was already on cyclosporine, the therapy was switched to everolimus or mycophenolate mofetil. The authors encountered no acute rejections after drug conversions.
EEGs were performed on 19 patients, of whom 11 (57.8%) had abnormal EEGs. Six (31.5%) patients showed continuous generalized slow wave discharge and 5 (26.3%) patients had epileptic activity (localization related spike and sharp wave activity) on EEG. Cranial neuroimaging was performed in all patients within the day seizures occurred. The most frequent neuroimaging finding after seizures was posterior leukoencephalopathy syndrome. They had characteristic findings of hyperintensity of the white matter on T2-weighted images and fluid-attenuated inversion recovery sequence on MRI.
There was no statistically significant association between the presence of seizures and pathological findings of cranial MRI (P = .121). Results of multivariate analysis of risk factors for seizures after liver transplantation are summarized in Table 1.
Risk Factors for Seizures After Liver Transplantation: Multivariate Analysis.
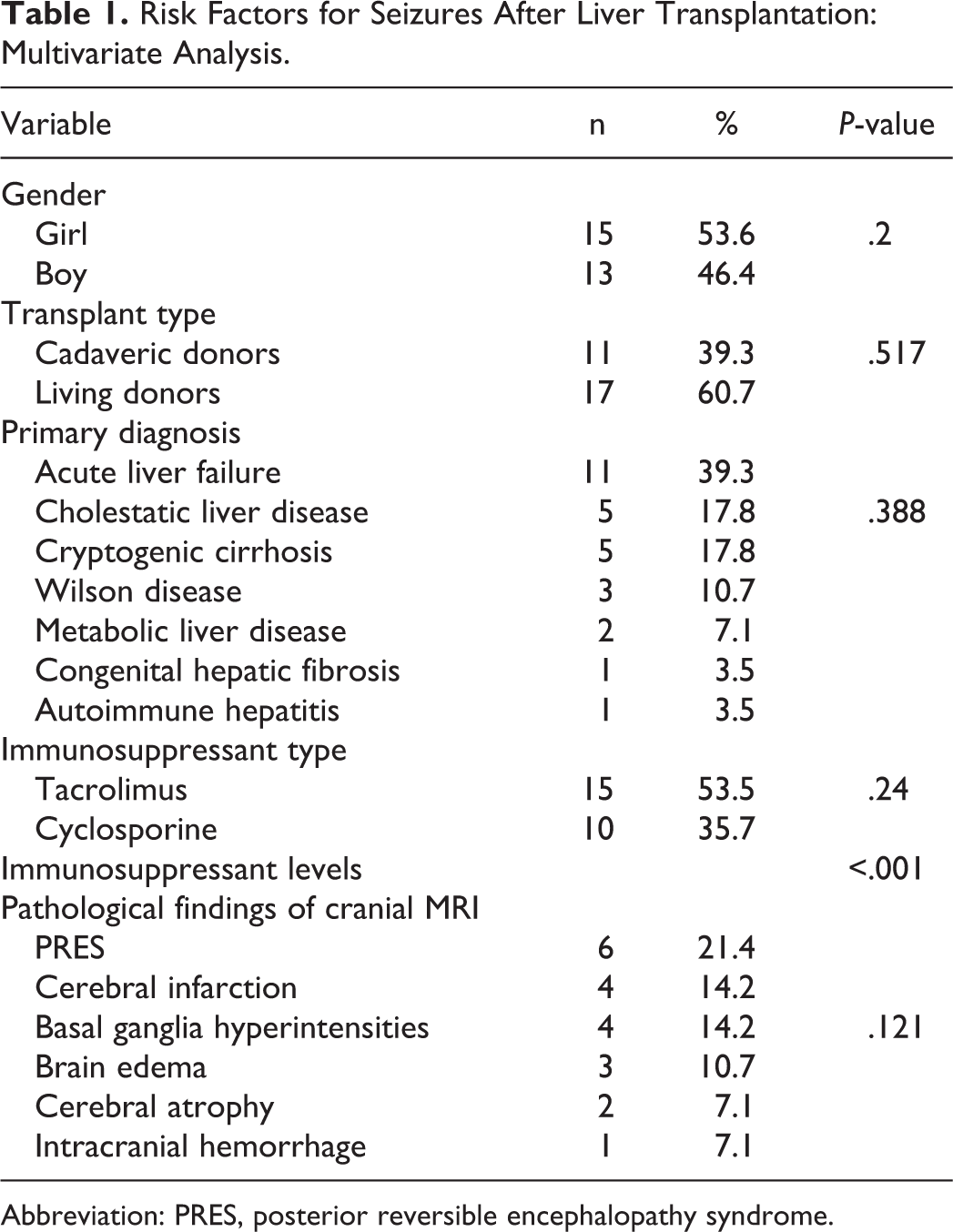
Abbreviation: PRES, posterior reversible encephalopathy syndrome.
Of 28 patients with seizures, 18 received levetiracetam along with drug conversion at the time of seizures. Levetiracetam was used with a mean of 33.3 ± 13.7 mg/kg/day (15-60 mg/kg/day). Seizures completely ended in 16 patients (88.9%) who used levetiracetam. In 2 patients (11.1%), whose seizure reduced more than 50% with levetiracetam, a second antiepileptic drug (topiramate or clonazepam) was added in follow-up. These patients continued to use levetiracetam 60 mg/kg/day. In the acute period the authors did not observe drug-related side effects in patients. There were no significant changes of hematological and biochemical data before and after the use of levetiracetam. Antiepileptic therapy was terminated in 13 patients at an average follow-up of 13.25 ± 16.4 months (range: 1-48 months).
Death, unrelated to seizure, occurred in 3 of 18 patients on levetiracetam (16.6%) within 3 months after liver transplantation.
Demographic data, primary liver disease, seizure type, etiology of seizure and outcome of 18 patients with epileptic seizures after liver transplantation are summarized in Table 2.
Demographic Data of 18 Patients With Epileptic Seizures After Liver Transplantation Who Were Treated With Levetiracetam.
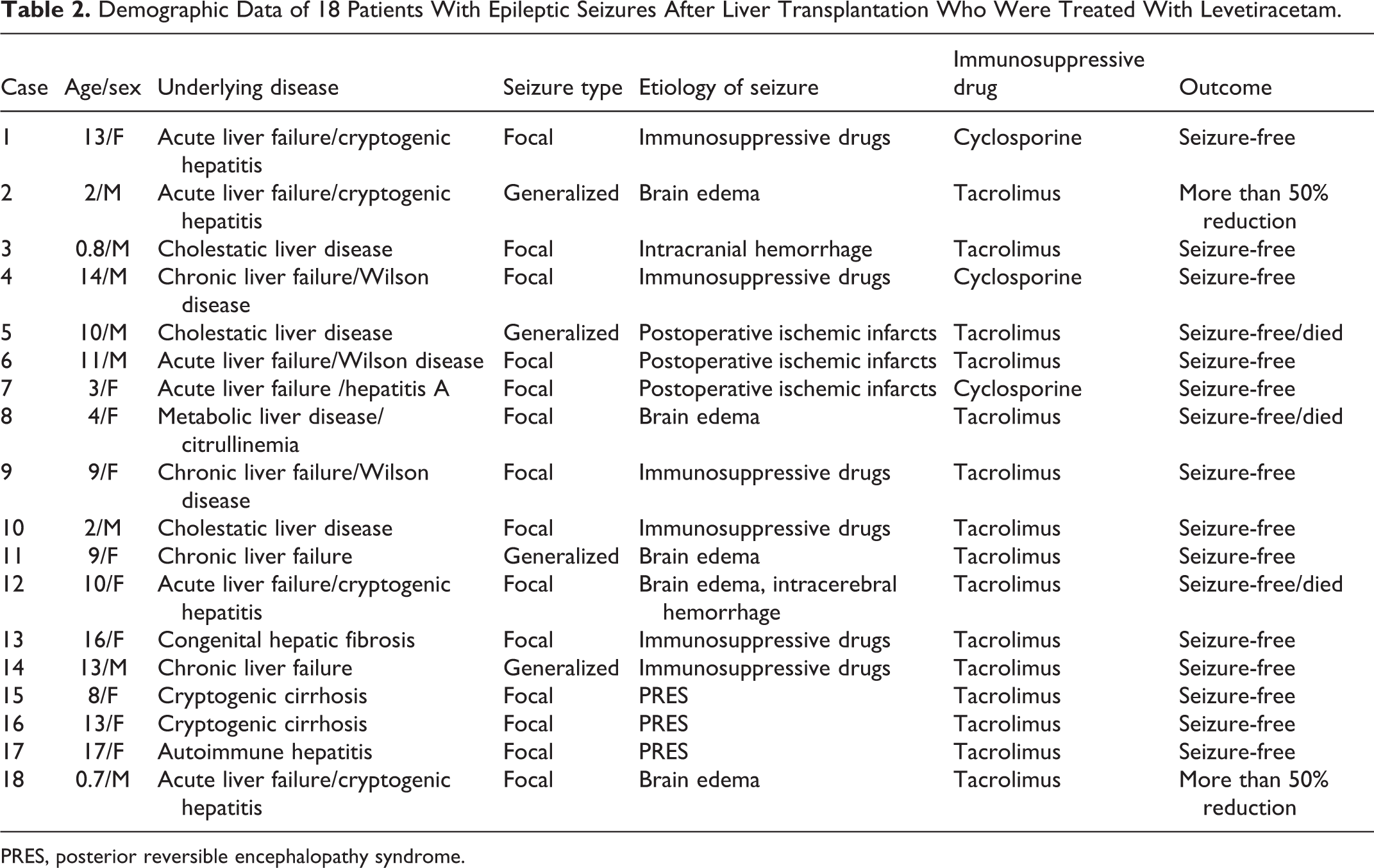
PRES, posterior reversible encephalopathy syndrome.
Discussion
Neurological complications might occur in 1/3 of patients who underwent liver transplantation with high mortality and morbidity. Among them, seizures are the most common ones occurring with a frequency of 2.8-42%. 3 -6 In this series, the incidence of seizures was 11.5%. The majority of seizures after liver transplantation are thought to occur in the early postoperative period, and the risk decreases over time, a trend also observed in the current cohort. It is presumed that metabolic derangements caused by liver transplantation and alteration in the permeability of the blood-brain barrier may contribute the occurrence of seizures. In this study, seizures occurred during the first 2 weeks after surgery (1-16 days). However, one recent study found that most seizures in children receiving liver transplantation occurred 3 months after surgery. 7 The influence of gender on postoperative seizures in adult liver transplantation recipients has been examined in a few studies, but a consensus has not been reached. 3 In this series, the authors found no difference between girls and boys (P = .2).
Although several studies have found that postoperative seizures after liver transplantation are associated with high mortality and morbidity, 8,9 most investigators stated that the underlying causes of the seizures, rather than the seizures, perse, are the main determinants of prognosis. 8 -10 The authors found death in 3 of 18 patients on levetiracetam (16.6%) unrelated to seizure. The authors observed infarction, intracerebral hemorrhage and brain edema in these patients. This situation illustrates the etiology of seizures and that seizure detection is very important in the prevention of postoperative complications.
Some studies have reported that preoperative hepatic encephalopathy was predictive of neurologic complications in adults but only one child suffered from hepatic encephalopathy before liver transplantation and was without seizures postoperatively. 11,12 In this study the authors did not come to the conclusion that preoperative hepatic encephalopathy is associated with seizure after liver transplantation (P = .68). The authors did not find significant association between the primary diagnosis and seizures, either (P = .38).
Saner et al 13 reported that liver transplantation from cadaveric donors was associated with a higher incidence of neurologic complications in adults compared with living donors liver transplantation. The authors did not observe a statistically significant correlation with transplantation type and seizure (P = .517).
Generalized seizures were more frequently reported after liver transplantation in recently published studies. 3 Conversely, in this study, focal seizures (75%) determined by clinical semiology were found to be higher than generalized seizures.
Seizures after liver transplantation are usually tonic-clonic. 14 The largest study investigating seizure types, causes, and outcomes in a transplant population examined 630 liver transplant patients and found that generalized tonic-clonic seizures were the most common seizure type, occurring in 28 patients. 4 In this study the authors found tonic-clonic seizure type more frequently (64.2%). Of these patients, 38.9% were primary generalized, and 61.1% were secondarily generalized.
The etiology of seizures in patients who underwent liver transplantation was found to be related to immunosuppressant drugs (mainly cyclosporine and tacrolimus), metabolic derangements, cerebrovascular events, and central nervous system infections. 15 In this study, the authors found immunosuppressant drugs, posterior reversible encephalopathy syndrome, postoperative ischemic infarction and metabolic disorders as the causative factors, as well. The pathophysiological mechanism of immunosuppressant-related seizures is not fully understood and the relationship between elevated serum trough immunosuppressant levels and neurotoxicity is also unclear. It has been reported that seizures may occur even when the trough tacrolimus level lies within the therapeutic range, 2 -16 though the authors found a statistically significant association between serum tacrolimus and cyclosporine levels and seizures after liver transplantation (P < .001). Xie et al 12 also found that serum trough tacrolimus level is the risk factor for seizures after surgery.
The presence of neurological abnormalities and seizures may be associated with pathological changes in MRI or EEG. 3 The most common neuroimaging findings were posterior reversible encephalopathy syndrome, involvement of the basal ganglia because of hepatic encephalopathy, intracerebral hemorrhage, cerebral infarction, cerebral edema, and cerebral atrophy in this series. The authors found that cranial MRI abnormalities and seizures were not statistically correlated (P = .121).
Goals of treatment in liver transplantation patients are similar to those in other patients with seizures and epilepsy. First, seizures should be controlled and prevented with antiepileptic drug treatment 17,18 with particular respect to avoidance of adverse impacts on the transplanted organ as well as drug interactions that could lead to altered immunosuppressive drug levels that place the organ at further risk. Second, underlying causes should be promptly recognized and treated to prevent seizure recurrence and further neurological complications. After controlling seizures, provoking factors such as toxic immunosuppressant levels, abnormal electrolyte or glucose levels, hypertension, or infection should be identified and corrected. 19 For recurrent seizures or a single seizure with potentially epileptogenic abnormalities on brain imaging or EEG, antiepileptic drug therapy should be continued. Seizures observed after liver transplantation usually self-limiting but refractory epilepsy may develop in some patients. 20 In this study, 88.9% of patients became seizure-free with levetiracetam treatment.
The primary considerations when selecting an antiepileptic drug for treatment of a liver transplantation patient include efficacy for the certain seizure type, and safety and the tolerability profile, as in other patient groups. Since limiting the potential drug–drug interactions is crucial in liver transplantation patients, selecting the antiepileptic drugs with minimal protein binding and minimal hepatic metabolism, induction, or inhibition is particularly desirable. 17,18,21 Most older and some newer antiepileptic drugs that have extensive hepatic metabolism, enzyme induction, significant protein binding, and drug–drug interaction potential should be avoided in transplant patients, except for the use of intravenous lorazepam or fosphenytoin for reliable and prompt termination of acute repetitive seizures or status epilepticus. The older antiepileptic drugs, phenytoin, phenobarbital, and carbamazepine, all have significant drug interactions with immunosuppressive agents by increasing metabolism of immunosuppressants and corticosteroids via induction of the hepatic cytochrome P450 enzymes. 22 Similarly, valproate is highly discouraged in liver transplantation patients, as it is primarily metabolized in liver and has been associated with hepatic failure. 23
Newer antiepileptic drugs are typically preferred for their favorable adverse effect profiles and minimal drug interactions 11,18,21 in liver transplantation patients. In addition to better patient tolerability, newer antiepileptic drugs provide greater flexibility for treating partial and primary generalized seizure types. However, certain newer antiepileptic drugs are still relatively undesirable for use in transplant patients. 19 Levetiracetam is the drug of choice for posttransplant seizures given its broad-spectrum efficacy across a broad range of seizure types throughout the lifespan, including infants, children, and adults, as well as its rapid and linear oral absorption conferring rapid efficacy, favorable side effect profile, flexible availability as an oral tablet, syrup, and intravenous formulations, and lack of significant hepatic metabolism or drug-drug interactions. 24 -26 The target for levetiracetam is binding of intravesicular synaptic vesicle protein 2A, thereby modulating neuro-transmitter release in rapidly discharging neurons. 27 No interactions were found between levetiracetam and 11 different drug-metabolizing enzymes. 28 Of particular relevance to transplant patients, levetiracetam does not affect immunosuppressant metabolism. 29 The authors used levetiracetam safely and seizures completely ended in 88.9% of patients who used levetiracetam. An intravenous formulation has been demonstrated to be bioequivalent to the oral formulation, providing another potential option for acute seizure management, preferably for those who are not in convulsive status epilepticus, as the evidence basis for acute seizure termination remains limited and uncontrolled. 30,31 Somnolence, asthenia, infection, and dizziness are the most frequent adverse effects of levetiracetam. Behavioral abnormalities such as irritability, personality change, and psychosis, and mild leukopenia are possible. 32,33 In this study the authors did not observe drug-related side effects and hematological and biochemical data changes in patients treated with levetiracetam.
In conclusion, seizures commonly follow pediatric liver transplantation and are significant sources of morbidity and mortality in liver transplant recipients. A careful approach to recognition and diagnosis of seizures after liver transplantation and prompt treatment would help to improve the management of liver transplantation recipients. In addition, for long-term maintenance treatment of seizures after liver transplantation, it is preferable to avoid medications which can affect immunosuppressant’s pharmacokinetics. Levetiracetam can be used as an effective and safe treatment option for seizure treatment.
Footnotes
Author Contributions
BK collected and analyzed data, and wrote the first draft of the manuscript. SG conceptualized and designed the study, analyzed data and revised the manuscript. MAS conceptualized and designed the study, performed statistical analysis, and critically reviewed the manuscript. MA and SY coordinated and supervised data and performed study procedures collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Institutional Review Board of the Inönü University.