
Abstract
Assessment of upper limb function, kinematic analysis, and dystonia in patients with spastic diplegia cerebral palsy and periventricular leukomalacia. Seven children with spastic diplegia cerebral palsy and 8 controls underwent upper limb kinematics. Movement duration, average and maximum linear velocity, index of curvature, index of dystonia, and target accuracy and stability were analyzed. In the patients with spastic diplegia, Gross Motor Function and Manual Ability Classification Systems were determined, and spasticity and dystonia were rated using the Modified Ashworth and the Burke-Fahn-Marsden Dystonia scales respectively. Children with spastic diplegia demonstrated a tendency toward higher index of dystonia reflecting overflow, higher index of curvature, lower velocities, and poor target accuracy and stability. All patients showed clinical evidence of dystonia in the upper limbs. Dystonia scores correlated with the Manual Ability Classification System (r = 0.86, P = .01) and with the index of dystonia (r = 0.82, P = .02). Children with spastic diplegia cerebral palsy present dystonia in the upper limbs. This is functionally relevant and can be measured with kinematic analysis.
Keywords
Cerebral palsy describes a group of disorders of the development of movement and posture, causing activity limitation, that are attributed to nonprogressive disturbance that occurred in the developing fetal or infant brain. 1 Cerebral palsy is classified according to the main type of motor disturbance. Spastic cerebral palsy, the most frequent type, is characterized by pyramidal dysfunction, while dyskinetic cerebral palsy is characterized by dystonia and/or choreoathetosis. 1 Mixed motor features often occur in these patients. 2,3
Prematurity is the leading cause of cerebral palsy, and the most frequent brain lesion in premature children with cerebral palsy is periventricular leukomalacia. 1,3,4,5 Periventricular leukomalacia is the result of an ischemic insult of the white matter occurring during a period of vulnerability of this brain region between the 23rd and 34th week of life. 3,5 Periventricular leukomalacia often results in spastic diplegia cerebral palsy, which is characterized by spasticity of the lower limbs and to a lesser extent of the upper limbs. Hemiplegia, tetraplegia, and dyskinetic cerebral palsy can also occur. 1,4,6
The identification and accurate delineation of different movement disorders in patients with cerebral palsy is central to determining appropriate treatments and evaluating outcomes. 2,3 Different clinical scales are used to gain insight into the severity of different motor disorders in these patients. 7,8 However, these scales are often insensitive to small changes in motor performance. Thus, quantitative measures such as kinematic analysis are necessary to provide more accurate means of assessment of the motor disorder. Currently, kinematic gait analysis is a useful tool to assess lower limb motor function and intervention effectiveness in children with cerebral palsy. 9 Conversely, upper limb kinematic analysis 7,10 –14 is performed less often because of uncertainty about its reliability in this population. 9
In children with spastic diplegia cerebral palsy and periventricular leukomalacia, the involvement of the upper limbs results in variable impairments in the ability to reach, grasp, transport, and release objects that are central to many activities of daily living. A few studies of upper limb kinematics in children with spastic diplegia cerebral palsy have been reported to date. 9,15 These studies have shown abnormalities in the peak velocities, reach path ratio, accuracy, and stability, 15 and also abnormal trajectory smoothness, increased trunk displacement, and decreased elbow extension. 9
Upper limb function in cerebral palsy depends on the degree of spasticity, presence of contractures, sensory loss, intelligence, and associated movement disorders such as dystonia. Dystonia is an involuntary alteration in the pattern of muscle activation during voluntary movement or maintenance of posture. In general, it is diagnosed by the observation of abnormal twisted postures or repetitive movements. It is commonly triggered or exacerbated by attempted voluntary movement and may fluctuate in presence and severity over time. 16 The contribution of dystonia in childhood motor disorders tends to be underestimated while spasticity is overestimated. 3 The presence of dystonia in patients with spastic diplegia cerebral palsy has been long recognized 4,17 ; however, documentation of this association is scarce. 9,10,15,18
The aim of this study was to characterize the upper limb movements in children with spastic diplegic cerebral palsy due to periventricular leukomalacia using quantitative 3D motion analysis. This study provides a better understanding of upper limb function in this type of cerebral palsy and documents the presence of dystonia in these children.
Methods
The study was performed at the Pediatric Neurology Unit of the Fist Department of pediatrics of the University of Athens at Agia Sofia hospital, and in the Gait and Motion Analysis Center at ELEPAP–Rehabilitation for the Disabled, in Athens, Greece, between September 2012 and September 2013. Patients were recruited at the cerebral palsy clinics of Agia Sofia Hospital, Penteli Children Hospital, and ELEPAP (RP, HS, AP). The study was approved by the ethics committees of Agia Sofia Hospital and ELEPAP.
The inclusion criteria were as follows: children (6-15 years old) with spastic diplegia cerebral palsy, presence of periventricular leukomalacia on brain magnetic resonance imaging (MRI), and ability to understand and follow instructions to perform kinematic analysis. Following were the exclusion criteria: children unable to sit independently, children with the inability to reach and grasp, presence of cervical and/or trunk dystonia that could impair the ability to sit and perform kinematic analysis, and antecedent of botulinum toxin injection in the upper limbs in the last 3 months prior to the kinematic analysis.
Patients were recruited during their regular visits at the cerebral palsy clinics. A total of 7 patients were enrolled, and subsequently they were further assessed by RP.
Functional status was determined by the Gross Motor Function Classification System
19
and the Manual Ability Classification System,
20
both of which are 5-level ordinal scales. The Gross Motor Function Classification System describes the gross motor function of children with cerebral palsy on the basis of self-initiated movement, with particular emphasis on sitting, walking, and wheeled mobility. A level 1 score indicates that the child can walk without restrictions but tends to be limited in some of the more advanced motor skills, and level 5 indicates that motor function is very limited even with the use of assistive technology. The Manual Ability Classification System classifies the ability of children aged from 4 to 18 years to manipulate objects during daily activities. A Manual Ability Classification System level 1 score indicates that the child handles objects easily and successfully, and level 5 indicates that the child cannot handle objects and is severely limited in the performance of even simple actions.
9
Spasticity was rated using the Modified Ashworth Scale.
21
The muscle groups tested in the upper limbs included shoulder abductors/adductors, shoulder extensors, elbow flexors/extensors, wrist pronators, wrist extensors/flexors, and finger flexors. The muscle groups tested in the lower limbs included hip abductors/adductors, knee extensors, and plantar flexors/extensors. A final score for the upper limbs and another for the lower limbs was obtained that was the mean of the muscle groups tested. Modified Ashworth Scale scores range from 0 (no increase in muscle tone) to 4 (no movement of the extremity possible, fixed in flexion or in extension). Dystonia was rated using the Burke-Fahn-Marsden Dystonia Scale (BFMS).
22
The final dystonia score corresponds to the sum of scores of 9 different body regions (maximum 120).
A control group of 8 nonaffected typically developed children was included, recruited during the same time period. They came from different backgrounds and were to an extent age matched. Selection criteria for the control group included no history of neurologic or musculoskeletal disorders, no apparent postural or motor deficits, and normal range of motion and muscle strength on examination. All subjects or their parents gave written informed consent to the research study and to publication of the results.
Movement Protocol, Kinematic Model, and Data Analysis
An extended movement protocol based on a previous reported by Vanezis et al was performed by AV and ND. 23 Briefly, 9 tasks were included in this protocol: 5 functional tasks and 4 reach-to-grasp tasks. The functional tasks signified activities of daily living: hand to contralateral shoulder, hand to back head, hand to back pocket, and drinking. Reach-to-grasp tasks included the following: reach upward and grasp with a horizontal grip, reach sideways and grasp with a horizontal grip, reach forward and grasp with a horizontal grip, and reach forward and grasp with a vertical grip. 23 Subjects performed all tasks at a self-selected speed with their dominant and nondominant arm. They performed 3 single successful trials of every movement task. A custom-made adjustable table and seat were used to ensure consistency of initial position (hips, knees, and ankles at 90°). The initial position of the hands was marked by a tape on the front of the ipsilateral knee apart from the drinking task, where forearms were positioned on a table with adjustable height. 23 Key moments and spatiotemporal and 3D kinematic data were treated and calculated as previously described. 23
One extra movement was included in the protocol, Reach and Point a target (ball) for 5 seconds, as described by Gordon et al, specifically selected as relevant for dystonia assessment. 15 Upper limb dystonia was assessed in the limb that was more involved by dystonia according to the assessment of the pediatric neurologist (RP).
The following parameters were analyzed: Movement duration: For each task, time to perform the movement was calculated. Average and maximum linear velocity: For each task, average and maximum values of the linear velocity of a marker placed on the ulnar styloid was calculated. Index of curvature: For each task, the index of curvature was measured as the ratio of the actual length of the traveled hand path to the direct linear distance between the start and the endpoint. Target accuracy: Patients were asked to reach and point their index on a target ball and hold their hand for 5 seconds (Reach and Point task). End point error was measured as the distance between the tip of the index finger and the target at the end of the first phase of movement. Hold distance was measured as the distance traveled by the wrist during the hold phase (5 seconds) and represents the ability to hold a steady position. Index of dystonia (kinematic measure of overflow
15
): During “drinking” trials, the maximum excursion of all joint rotations of the resting arm was calculated. The Joint rotations that were analyzed included shoulder (plane of elevation and elevation),
23
elbow (flexion-extension), forearm (pronation-supination), and wrist (flexion-extension and ulnar-radial deviation).
Statistical Analysis
All measurements were expressed as mean ± SD. Statistical analyses, including Pearson correlation analysis, were carried out using the SPSS statistical package (version 16.0). Alpha was set at 0.05.
Results
All patients had spastic diplegia cerebral palsy and showed evidence of periventricular leukomalacia on brain MRI. There were 4 male and 3 female patients, and mean age at the time of the study was 8.88 ± 2.85 years. In the control group, there were 4 male and 4 female patients and the mean age was 11.2 ± 2.6 years.
All children with spastic diplegia cerebral palsy had a history of prematurity with a mean gestational age of 31.43 ± 2.48 weeks and a mean birth weight of 1515.71 ± 357.16 g. The mean Gross Motor Function Classification System score was 3 ± 1.15 and the Manual Ability Classification System score 2.29 ± 0.76. One patient followed a special education program, 2 mainstream education with support, and 4 mainstream education (Table 1). All of them were able to understand and follow instructions during kinematic analysis.
Spastic Diplegic Cerebral Palsy Patients: Demographics.
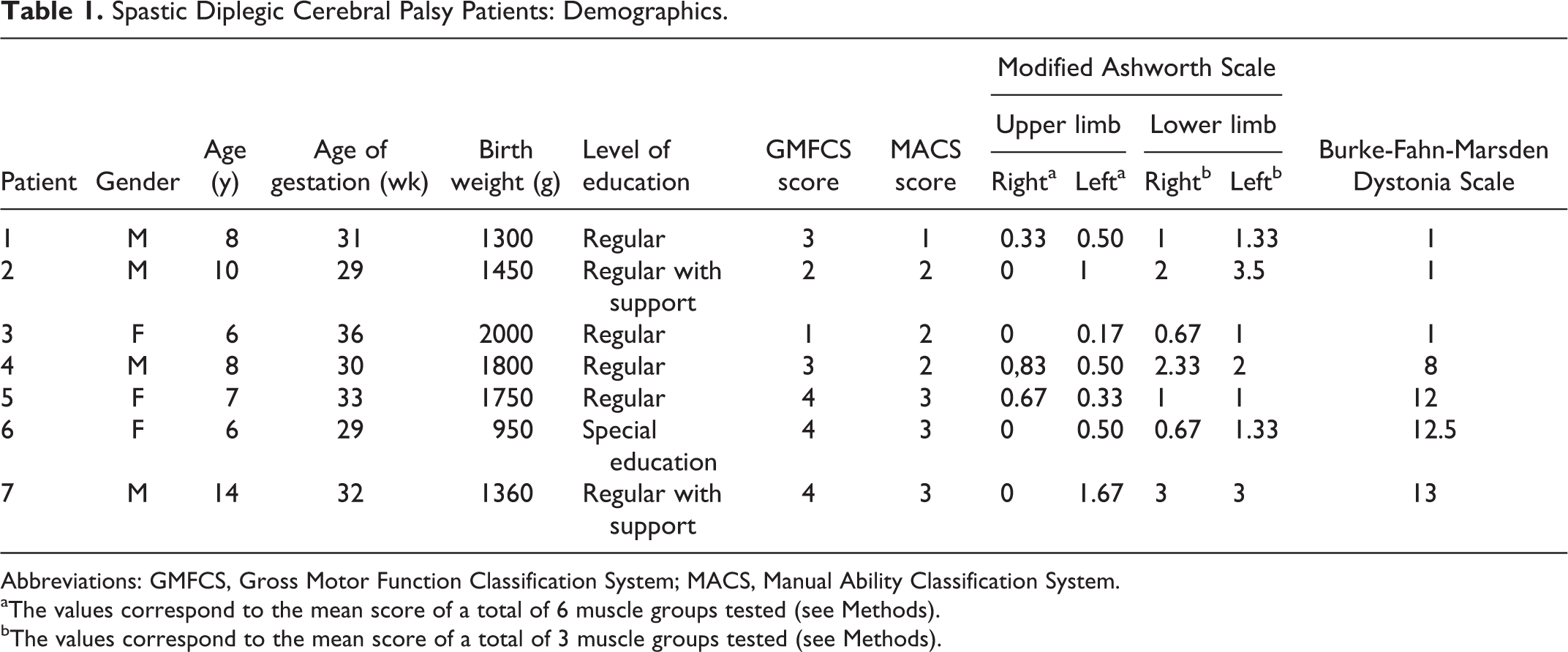
Abbreviations: GMFCS, Gross Motor Function Classification System; MACS, Manual Ability Classification System.
aThe values correspond to the mean score of a total of 6 muscle groups tested (see Methods).
bThe values correspond to the mean score of a total of 3 muscle groups tested (see Methods).
All children with spastic diplegia cerebral palsy showed evidence of spasticity in the lower limbs, and to lesser degree in the upper limbs (Table 1). None of them was receiving antispasticity medication. There was no correlation between Manual Ability Classification System scores, reflecting manual functionality, and upper limb spasticity scores as per the Modified Ashworth Scale (r = 0.37, P = .41).
All patients showed evidence of dystonia of the upper limbs (Table 1). Dystonia severity ranged from 1 to 13 measured by the Burke-Fahn-Marsden Dystonia Scale for dystonia. Three patients (1-3) showed slight dystonia on the nondominant upper limb that was detected during examination of rapid alternating movements of the hands and fingers. Four patients (4-7) showed action dystonia with many tasks. In 1 patient (4), dystonia was mild in both hands; in the others, dystonia was worse in the nondominant hand and ranged from moderate (5, 6) to severe (7). Manual Ability Classification System scores showed significant correlation with dystonia severity scores (r = 0.86, P = .01).
Spastic Diplegic Cerebral Palsy vs Typically Developed Children
Spatiotemporal analysis
Maximum and average velocities (meters/second), duration (seconds), and index of curvature of all the studied motor tasks followed a normal distribution. Their means and SD are depicted in Table 2. Children with spastic diplegia cerebral palsy demonstrated a tendency to lower average velocities (difference = 0.23 m/s), longer durations (difference = 1.4 s), and increased index of curvature (difference = 0.27) compared to controls. Given the small size of these samples, statistic analyses to establish differences between the groups could not be performed.
Upper Limb Kinematic Parameters in Controls and Spastic Diplegia Cerebral Palsy.
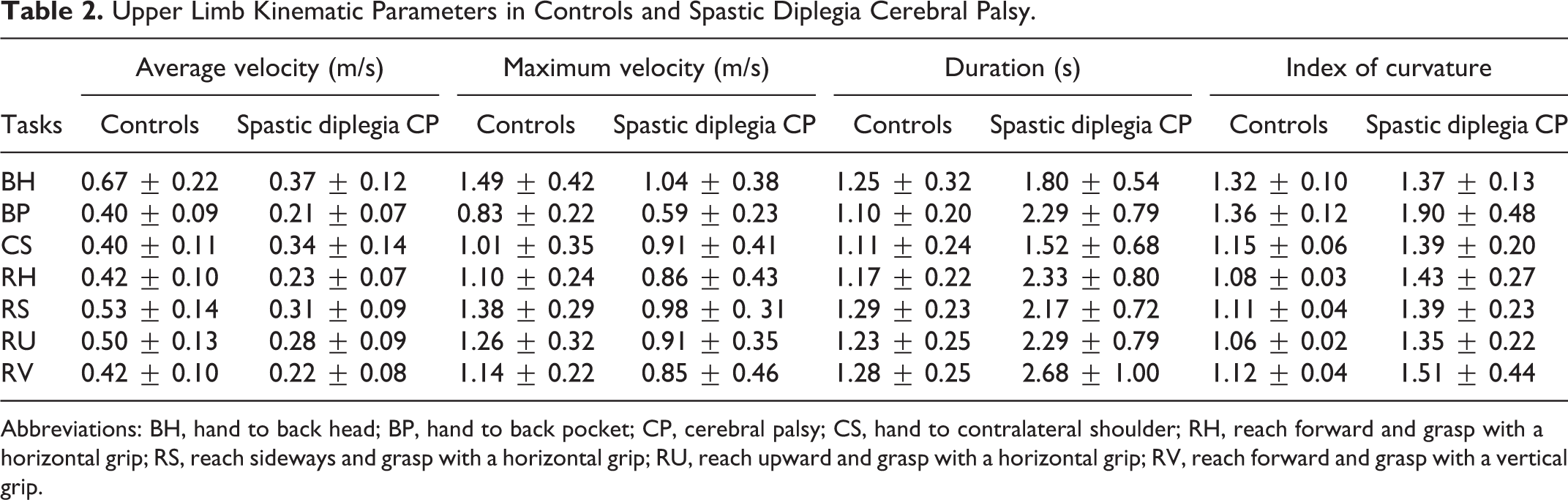
Abbreviations: BH, hand to back head; BP, hand to back pocket; CP, cerebral palsy; CS, hand to contralateral shoulder; RH, reach forward and grasp with a horizontal grip; RS, reach sideways and grasp with a horizontal grip; RU, reach upward and grasp with a horizontal grip; RV, reach forward and grasp with a vertical grip.
Kinematic analysis
Spastic diplegia cerebral palsy patients showed a tendency to greater wrist flexion in all tasks, they were unable to reach sufficient elbow extension and forearm supination and they showed increased trunk flexion-extension range of motion. Shoulder elevation was similar in controls and in children with spastic diplegia cerebral palsy.
Assessment of Dystonia
Index of dystonia
Index of dystonia in controls was 20° ± 10°, and in patients with spastic diplegia cerebral palsy it was 102° ± 59°. In the 3 patients with slight dystonia scores on the Burke-Fahn-Marsden Dystonia Scale (1-3), the index of dystonia was 58° ± 8°, whereas in the 4 patients with higher dystonia scores (4-7) it was 136° ± 30°. A significant correlation between the index of dystonia and dystonia score was detected (r = 0.82, P = .02).
Target accuracy
In the control group, end point error was 0.014 ± 0.006 m and hold distance was 0.025 ± 0.008 m. In patients with spastic diplegia cerebral palsy, end point error was 0.018 ± 0.006 and hold distance was 0.105 ± 0.078. There was no significant correlation of target accuracy parameters with dystonia scores.
Discussion
In this study, we assessed upper limb function and the presence of dystonia in 7 patients with spastic diplegia cerebral palsy and periventricular leukomalacia. On 3D kinematic analysis, patients demonstrated a tendency to longer duration of arm movements, lower average velocities, greater wrist flexion, and insufficient elbow extension and forearm supination. To understand the contribution of upper limb dystonia to the 3 D kinematic pattern of these patients, we applied an extended movement protocol and analyzed several kinematic parameters that were representative of this movement disorder, including angular displacement of the opposite limb (index of dystonia), index of curvature, target accuracy, and maximum linear velocity.
All patients showed evidence of upper limb dystonia on neurologic examination. Dystonia was variable in severity, it was mainly distal, and in the majority it was asymmetric. Functional impairment of the upper limbs was variable, with Manual Ability Classification System scores ranging from 1 to 3. Although the Manual Ability Classification System does not take into account the type of motor disorder leading to functional disturbance, the correlation of Manual Ability Classification System with the dystonia severity scores (r = 0.86, P = .01) and lack of correlation with the spasticity scores supports the role of dystonia in the motor functional disturbance of these patients.
Dystonia is often initiated or worsened by voluntary action and is associated with overflow muscle activation, even in the limb not performing the task. Gordon et al studied a kinematic measure of overflow as an indicator of dystonia (index of dystonia), which was the sum of arm joint motion during attempted rest while performing an action with the contralateral arm. 15 This measure of dystonia correlated with the Barry-Albright Dystonia Scale in cerebral palsy patients with mixed motor features, but not with spasticity measurements. 15 In our study, spastic diplegia cerebral palsy patients showed significant correlation of Index of Dystonia and qualitative dystonia scores (r = 0.82, P = .02), thus supporting that this kinematic measure is capturing clinically significant elements of dystonia.
Dystonia is associated with a disturbance to maintain steady positions and undershooting or overshooting during reaching tasks. 15 In addition, large fluctuations of the pauses at targets are noted during alternate reaching tasks. 10 Target accuracy and ability to hold a steady position was assessed in our study. Patients with higher dystonia scores (≥8 on the Burke-Fahn-Marsden Dystonia Scale) showed a tendency for poor target accuracy and greater instability holding a position, whereas patients with lower dystonia scores (<8 on the Burke-Fahn-Marsden Dystonia Scale) showed good targeting but poor stability (data not shown).
Index of curvature, reflecting more curved movement paths, and decreased speed are demonstrated in kinematic analysis of children with dystonia. 10,15,18,24 In our study, spastic diplegia cerebral palsy patients also showed a higher index of curvature and a trend toward slower maximum linear velocities. Despite the slower velocities in patients with spastic diplegia cerebral palsy, the ones with severe dystonia scores (≥8 on the Burke-Fahn-Marsden Dystonia Scale) demonstrated faster movements than the ones with mild dystonia (<8 on the Burke-Fahn-Marsden Dystonia Scale). These findings suggest that in the patients with milder dystonia, the slower execution occurs in order to achieve quality movement and results in low index of curvature and better targeting during reaching tasks. In contrast, in patients with worse dystonia, the trend of higher velocities may be indicative of less motor control and is associated with higher index of curvature scores, and poorer stability and target accuracy.
In this study, we confirm the presence of dystonia in the upper limbs of patients with spastic diplegia cerebral palsy in the setting of periventricular leukomalacia. Dystonia has been previously assessed by 3D kinematic analysis in patients with cerebral palsy. 9,10,15,18 However, it has not been assessed in a homogenous group of patients. In this study, despite the differences in the severity of motor impairment, the sample was considered homogenous because all patients had the same type of cerebral palsy, the same distribution of the motor deficit and the same type of brain lesion. A limitation of this study is that our patient sample was too small to reach statistical significance for several of the produced parameters. The fact that there was an age difference between controls (11.2 ± 2.6 years) and patients (8.88 ± 2.85 years) represents another limitation, although the tasks analyzed were simple and could be performed by young children. A larger number of patients, with a more closely matched group of controls, and more expanded analysis of different body parts will need to be studied to define in more detail dystonia in this group of patients.
A number of conditions are associated with dystonia, and it is thought that variable pathophysiological mechanisms and neuroanatomic substrates can lead to this movement disorder, probably sharing a common path. 25 Although many forms of childhood dystonia are attributable to lesions in the basal ganglia, 26 more recent findings envision dystonia as a network disorder involving basal ganglia–thalamo-cortical and the cerebello-thalamo-cortical networks. 25 In periventricular leukomalacia, there is a distinctive cerebral white matter injury that is often associated with neuronal and axonal disease including the thalamus, basal ganglia, cerebral cortex, brain stem, and cerebellum. 5 Descending motor tract injury along with overlying cortical volume reduction and reduced functional connectivity appears to play a role in the pathophysiology of motor dysfunction in spastic diplegia cerebral palsy and periventricular leukomalacia. 15 Conversely, there is also evidence of sensory pathway damage that has also been implicated in motor dysfunction in periventricular leukomalacia. 3,26,27 Many of these periventricular leukomalacia anatomical substrates share common paths with the ones leading to dystonia, thus providing a potential explanation for why dystonia occurs in periventricular leukomalacia.
Conclusions
In this work, we described the kinematic upper limb motor pattern of 7 patients with spastic diplegia cerebral palsy in the setting of periventricular leukomalacia. We identify and delineate the presence of dystonia in the upper limbs of these patients which correlates with their functional disability. These findings may help in determining appropriate treatments and evaluating outcomes of these patients. Further studies in larger populations will help to confirm and further delineate the findings in this report.
Footnotes
Author Contributions
RP, AV, and ND conceived and organized the research project. AV and ND designed the project. All authors contributed to the execution, reviewing, and critical analysis of the project. PR wrote the first draft of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board of Agia Sofia Hospital and ELEPAP.