
Abstract
Migraine and epilepsy are classified as chronic paroxysmal neurologic disorders sharing many clinical features, as well as possible treatment options. This review highlights the similarities between migraine and epilepsy in pediatrics, focusing on epidemiologic, pathophysiological, genetic, clinical, and pharmacologic aspects. Despite the fact that several syndromes share symptoms of both migraine and epilepsy, further research is needed to clarify the pathophysiological and genetic basis of their comorbidity. Drugs used for prophylactic therapy of migraine and epilepsy have similar pharmacologic properties. The role of epileptic pharmacotherapy in the prophylaxis of migraine is assessed, including the use of conventional antiepileptic drugs, calcium channel blockers, and nonpharmacologic methods such as dietary therapy, supplements, and vagal nerve stimulation. Further randomized, controlled clinical trials assessing pharmacologic and nonpharmacologic methods for the treatment of both disorders are essential, in order to initiate new therapeutic approaches.
Migraine and epilepsy, the most common diagnoses in pediatric neurology, belong to a group of chronic, paroxysmal neurologic disorders with recurrent attacks of nervous system dysfunction. 1 Both genetic and environmental factors have an important role in the expression of both diseases. In terms of clinical presentation, both migraine and epilepsy display similar sensorimotor and cognitive impairments, which are generated in the cerebral cortex and subject to subcortical modulation. 2 Both diseases can manifest postictal lethargy, disorders of consciousness, visual disturbances, dizziness, paresthesia, hemiparesis, and aphasia. In the beginning of the 20th century, migraine was classified as a borderland disease to epilepsy, with 2 important differences: (1) visual symptoms are shorter in epilepsy compared to migraine, and (2) migraine headaches are much more severe in comparison to postictal headaches. 3 Most important, seizures, as opposed to migraine, may be life threatening to the patient. 4 Because of the high prevalence of migraine in the general population, the comorbidity of migraine and epilepsy could be coincidental. However, it has been demonstrated that one disease is statistically more probable if the other has already manifested. 5 Moreover, a substantial overlap in terms of prophylactic pharmacotherapy exists for both migraine and epilepsy. The mechanism of comorbidity is not fully understood. A bidirectional mechanism has been proposed where epilepsy increases the risk of migraine, and vice versa. It has been suggested that cortical hyperexcitability may be an underlying pathophysiological mechanism for both entities. 4 The pediatric population is more prone to autonomic nervous system symptomatology during seizures, often having longer, isolated, ictal autonomic manifestations. Video EEG monitoring of children with temporal lobe seizures often shows the manifestations of “abdominal epilepsy,” that is, episodic abdominal pain, nausea, vomiting, and a state of confusion. In addition, symptoms of childhood occipital epilepsy are very similar to those of migraine. 3
Epidemiology
The prevalence of epilepsy in the pediatric population is between 0.4% and 1.0%, with peak prevalence in children up to 3 years of age. 6 Some epileptic syndromes are age-dependent and self-limiting, whereas others show no relation to age. In patients with benign epilepsy with centrotemporal spikes a spontaneous remission of epilepsy usually occurs in the peripubertal period. The majority of studies shows no evidence for gender-specific differences in epilepsy prevalence, with some exceptions: childhood absence epilepsy, one of the most common forms of idiopathic generalized epilepsies, is more frequent in females, whereas other syndromes (Doose, Landau-Kleffner, continuous spike-wave during slow-wave sleep) are more common in males. 6,7 Migraine is up to 20 times more common than epilepsy in the pediatric population. 2,8 The prevalence of migraine in children and adolescents is around 8%, with a significantly lower frequency under the age of 14 years. In contrast to epilepsy, migraine does demonstrate gender specificity. In the population older than 14 years, females are more susceptible to migraine than males, whereas the gender prevalence is equal in the younger age. 9 Migraine without aura has 5 times higher prevalence in children than migraine with aura, whereas in adults they are 3 to 4 times more frequent. 3,10,11 Compared to the general population, epilepsy is significantly more frequent in migraineurs. A study of 1795 pediatric patients with headaches found that 3% (56 total) of the patients also had epilepsy (the majority of whom had migraine since childhood). Headaches preceded epilepsy in 27% of patients, whereas headaches and epilepsy began the same year in 29% of patients. 11 Ludvigsson et al 12 demonstrated that there is an increased risk for unprovoked seizures in children having migraine with aura as opposed to migraine without aura. In addition, there was a 2.4 to 4.5 times higher rate of migraine in those with epilepsy in comparison to those without epilepsy. A recent pediatric study showed that 25% of children with epilepsy had migraine, whereas the prevalence in adolescents was 32%. 13
Etiopathogenesis
Mutations of specific genes on chromosomes 9, 12, and 14 are connected with certain migraine and epilepsy syndromes. The underlying cellular mechanisms of comorbidity of migraine and epilepsy include channelopathies, impairment of ion homeostasis in neuronal and/or glial cells, disturbance of GABA-ergic or glutamatergic systems, and disorders of mitochondrial function. 4 Mutations in calcium channel 1A (CACN1A, neuronal R/Q type Ca channels), ATP1A2 (Na+ and K+ transporter), and sodium channels 1A linked to familial hemiplegic migraine are associated with certain epilepsies of childhood, such as childhood absence epilepsy, genetic (generalized) epilepsy with febrile seizures plus, and Dravet syndrome. 6,8,14 -16 In addition, mutations in the gene SLC1A3 (which encodes excitatory amino acid transporter 1), POLG (that codifies catalytic domain of mitochondrial DNA polymerase) and C10orF2 (for mitochondrial DNA helicase Twinkle) also show a connection between migraine and epilepsy. 4 Recent studies have suggested a genetic link between several other epileptic syndromes and migraine, but specific genetic loci are yet to be identified. 6,8,15 -17 In children with benign occipital epilepsy of childhood, postictal headache was reported in 36% of cases. 17 A higher risk for migraine is also seen in those with Panayiotopoulos syndrome and benign Rolandic epilepsy. 6,8,15,16
The underlying mechanisms for migraine and epilepsy are not fully understood. Recent studies support the theory that neocortical hyperexcitability, as a manifestation of similar molecular and genetic disfunction, is the main pathophysiological substrate for both diseases. 16 In epilepsy, neocortical hyperexcitability leads to abnormal neuronal discharges and paroxysmal depolarizing shift. 2 The majority of studies suggest that migraine aura is the result of transitioning from neocortical hyperexcitability to cortical spreading depression. 18 -22 Cascading depolarization, which spreads through the cortex, also induces oscillations in the concentration of intracellular calcium and neurotransmitters, followed by long-lasting neural suppression. Although the depolarization phase has been associated with an increase in cerebral blood flow, the lowered neural activity has been associated with a reduction in blood flow. 20,21 It has been assumed that this effect of cortical spreading depression activates the trigeminal nociceptor system, leading to the neuroinflammation and pain symptoms during the migraine with aura attack. 4,16,18,19 Interestingly, the role of cortical spreading depression in migraine has recently become controversial topic. Although some authors suggest cortical spreading depression as an underlying mechanism in both migraine with and without aura, 23 others argue against the role of cortical spreading depression in migraine aura. 24 Currently, cortical spreading depression is a generally assumed overlapping phenomenon of epilepsy and migraine. A link between cortical spreading depression and epilepsy is based on evidence that neuronal synchronization precedes the onset of cortical spreading depression and neuronal excitability changes. 22 It is suggested that this synchronization is mediated by glutamate, the main excitatory neurotransmitter. Several studies have suggested that the occipital cortex seems especially sensitive to cortical spreading depression, which supports the theory that a lower activation threshold in the cortex may be involved in both migraine and epilepsy. 25 When transcranial magnetic stimulation of the occipital cortex was assessed in patients with migraine, a reduction in the phosphene induction threshold was observed. 16 Ictal headache is rarely a sole seizure manifestation occurring, perchance, through epileptic discharges–induced trigeminovascular system activation. 26 Ogunyemi et al 27 hypothesized that the efficiency of sumatriptan in postictal headache could implicate a role for serotonergic neurotransmission in this clinical phenomenon. 28 Clinical observation that postictal headaches are usually associated with occipital seizures, as well as the role of certain antiepileptic drugs in the prophylaxis of migraine attacks, supports the hyperexcitability hypothesis as a possible common pathophysiological mechanism for both diseases. 4,16 The possible interplay between cortical spreading depression and seizures involves complex mechanisms and further research is necessary. 29,30 Current investigations, related to pituitary adenylate cyclase-activating polypeptide (PACAP), reveal a possible new link between epilepsy and migraine. Acute seizure, as a stressful event, 31 increases levels of the neuropeptide PACAP which, along with glutamate, has a role in cardiorespiratory protection and prevention of sudden unexpected death in epilepsy. 32 -34 On the other hand, PACAP (similar to calcitonin gene–related peptide) contributes to neurogenic inflammation, nociception, dural vessel tone control, cranial blood flow, etc. 35,36 Acting primarily through the trigeminovascular system, PACAP-38 appears to have the ability to induce headache and migraine-like attacks, especially in patients with migraine. 37 Thus, we can presume that seizure-related induction of PACAP can trigger postictal headache. Furthermore, therapeutics targeting PACAP and PACAP receptors may represent a promising antimigraine strategy. 38 However, if PACAP modulation is to play a future role in migraine treatment, the use of such agents in patients with comorbid epilepsy would be limited by potential side effects.
Clinical Features
Both diseases are characterized by paroxysmal onset and attacks occurring in distinct phases. 1,2,4,6,8,15,16 However, migraine and epilepsy are distinguished by several clinical features (Table 1).
Migraine vs Epilepsy: The Most Significant Clinical Features.
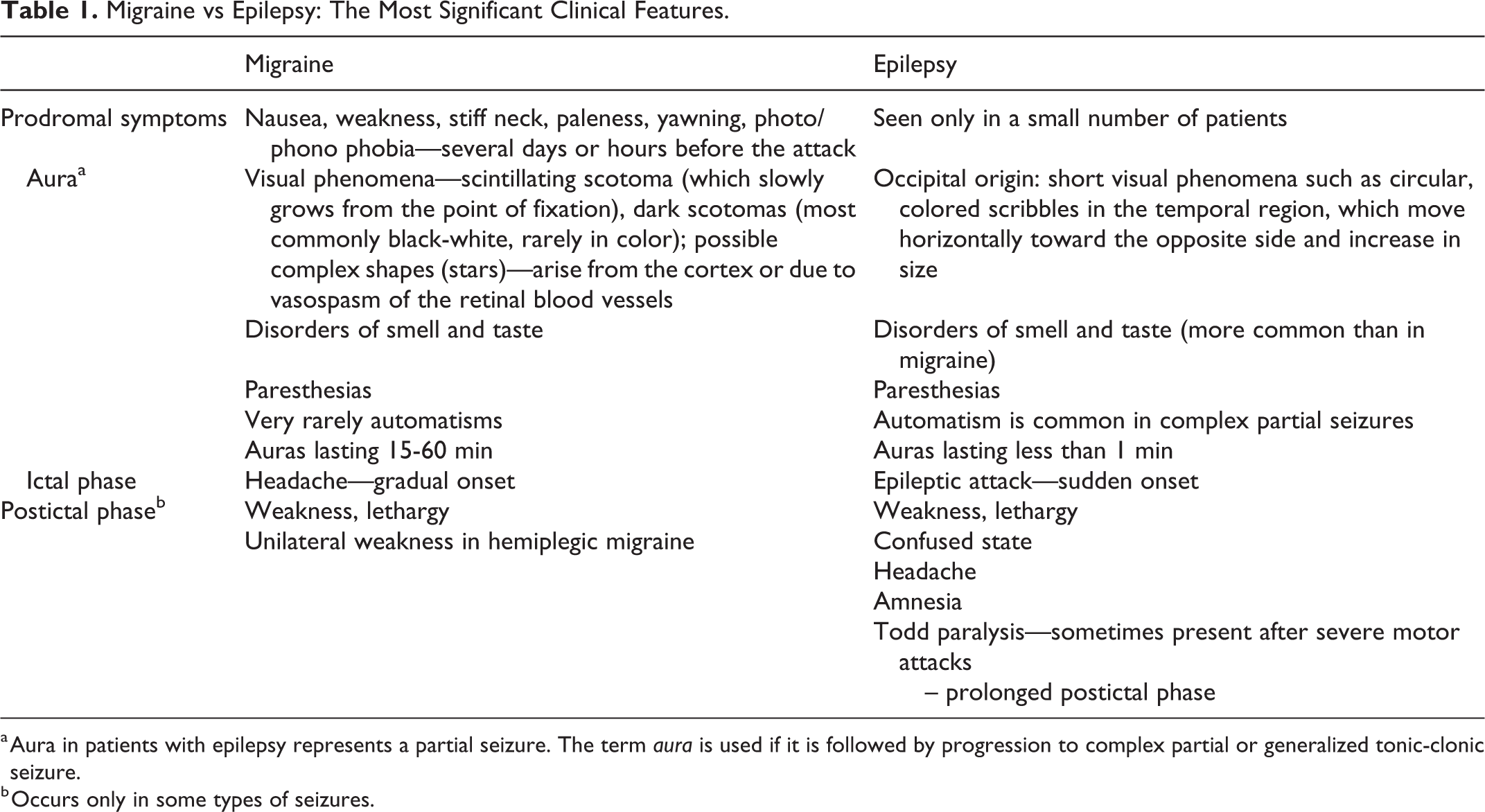
a Aura in patients with epilepsy represents a partial seizure. The term aura is used if it is followed by progression to complex partial or generalized tonic-clonic seizure.
b Occurs only in some types of seizures.
Migraine-Seizure Continuum
Headache and seizure are present in chronological order in some patients, as “migralepsy” or peri-ictal headaches (occurring preictally, ictally, and postictally). Some of these disorders are defined by the third edition criteria of the International Classification of Headache Disorders (ICDH-III), whereas others are not classified. 39
Migraine-Aura Triggered Seizure
In the third edition criteria of the ICDH-III, this disorder is classified as a complication of migraine and described as an epileptic seizure triggered by the attack of migraine with aura. The diagnostic criteria include a seizure during, or within 1 hour of, a migraine attack with aura. This phenomenon, once referred to as “migralepsy,” is a rare event seen in patients with a history of migraine with aura. Some authors consider the term “migralepsy” as obsolete, because it is most likely a phenomenon that does not exist and which often indicates the wrong qualification of symptoms. “Migralepsy” is not included in the classification of seizures by the International League Against Epilepsy. 40,41 Furthermore, occipital epilepsy may be confused for migraine-aura triggered seizures. Occipital lobe epilepsy is often difficult to properly diagnose, because visual phenomena and headache are sometimes the only symptoms. Furthermore, patients sometimes find it difficult to distinguish between visual auras and bright lights that trigger headaches or photosensitive seizures. 3
Preictal Headache
Headaches that precede a seizure but do not meet the criteria for “migralepsy” are rarely seen and not classified under ICDH-III. Moreover, it is possible that both patients and physicians neglect headache preceding a seizure. In a study by Yankovsky et al 42 including 47 patients with intractable epilepsy associated with peri-ictal headaches, preictal headaches were seen in 11 (23%) of patients (90% of which showed ipsilateral localization to the seizure focus). Using previous studies assessing cerebral blood flow in patients with temporal lobe epilepsy, the authors concluded that increased blood flow to the seizure focus, which precedes any symptoms or characteristic EEG changes, could be responsible for the headache that precedes the seizure, most likely through activation of the trigeminovascular system. 42 Further researche is needed to determinate incidence and features of preictal headache. 39
Ictal Epileptic Headache
This term has recently been included in the final version of ICDH-III. Ictal epileptic headache has been defined as a headache triggered by partial epileptic seizure and occurring as an ictal manifestation of seizure discharge. In addition, one of following features is necessary: headache is ipsilateral to the ictal discharge, and/or headache significantly improves or remits immediately after the partial seizure is terminated. 39 This condition is considered to be underestimated and under-reported. Parisi et al 43 -46 underlined the importance of becoming aware of this diagnosis in order to initiate an appropriate workup and treatment strategy. Presentation of nonconvulsive status epilepticus as a sole migraine attack, referred to status epilepticus migrainosus, had also been reported. 47 Hemicrania epileptica is a rare ictal epileptic headache, most likely a result of reactive hyperemia. To confirm a diagnosis, EEG evidence of synchronicity and ipsilaterality of manifestations should be provided. 48
Postictal Headache
According to ICDH-III, postictal headaches are headaches that occur within 3 hours of an epileptic seizure and resolve within 72 hours of seizure termination. Postictal headaches can be manifested as a tension type headache or migraine. 39 They are the most frequent type of peri-ictal headaches. Through the various study cohorts, different frequencies of headache after epileptic seizures (from 12% to 52%) have been reported. 49 -52 A lower prevalence of postictal headache is noted in patients with lower frequency of seizure attacks and shorter disease duration. 50,51 In addition, a significant association between postictal headache and antiepileptic polytherapy was observed. 51 Other groups at risk for this headache type are young adults, former headache sufferers, patients with early-onset seizures, patients experiencing generalized tonic-clonic seizures, as well as those with occipital epilepsy. 52
Migraine and Epilepsy Syndromes
Early-onset benign occipital epilepsy of childhood, known as Panayiotopoulos syndrome, usually presents between years 3 and 6; is characterized by rare, partial seizures; and is often prolonged in duration; with roughly two-thirds of cases occurring nocturnally. 53 The seizures consist of a combination of autonomic and behavioral symptoms with disturbances of consciousness. Preictal headache may be present. Predominant features are occipital EEG abnormalities and autonomic symptoms such as vomiting, paleness, mydriasis, and sweating. Sometimes syncope is the sole ictal event. 54 Because ictal vomiting occurs in about half of patients, these seizures could be misdiagnosed as abdominal migraine. 2,4,15,40 Late-onset benign occipital epilepsy of childhood (Gastaut syndrome) is a rare condition. 40 It begins between ages 3 and 15, with a peak incidence at years 8-9. 55,56 Characteristic findings include short, partial seizures with typical visual symptoms (amaurosis, phosphene, illusions, or figurative hallucinations) and long-lasting postictal headache often with nausea and vomiting (in 25%-40% of patients). Interictal EEG shows normal background activity, with occipital spikes suppressed by eye-opening. Although these EEG patterns may help to differentiate Gastaut syndrome from migraine with visual aura, they are also frequently found in children younger than 4 years, during myoclonic and absence seizures, and in photosensitive epilepsy. 17,56 Benign epilepsy with centrotemporal spikes (benign Rolandic epilepsy) represents the most common (13.4%-24% of childhood epilepsies) type of pediatric idiopathic focal epilepsy. 57,58 Usually beginning between the ages of 7 and 10, the seizures consist of unilateral sensorimotor facial manifestations (30% of patients) usually progressing to 1 arm, unilateral paresthesias inside the mouth (53%), and anarthia. 55 In addition, these patients show increased rates of episodic abdominal pain and headaches. 59 The clinical studies have shown a strong association between benign Rolandic epilepsy and migraine. 60 The prognosis of this disorder is not as good as once thought. Actually, new data indicate subtle but real neurocognitive difficulties observed in children with benign Rolandic epilepsy. 61
Familial hemiplegic migraine is a rare, autosomal dominant disorder characterized by migraine with a specific aura including motor weakness. The aura in hemiplegic migraine consists of completely reversible motor weakness with visual disturbance, sensory symptoms and/or speech/language symptoms. 39 There are 3 subtypes of familial hemiplegic migraine currently known, caused by specific gene mutations and characterized by different probabilities for epilepsy. 2 More than half of patients with familial hemiplegic migraine have familial hemiplegic migraine type 1, resulting from a mutation in the CACNA1A gene located on chromosome 19p13, encoding an alpha subunit of the P or Q type calcium channels. 62 This mutation, linked to facilitated cortical spreading depression and neuronal hyperexcitability, can manifest as absence seizures and familial hemiplegic migraine, as well as episodic ataxia type 2 and spinocerebellar ataxia type 6. 4 The S218 L CACNA1A gene mutation results in a more severe familial hemiplegic migraine type 1 phenotype, with cerebellar symptoms, prolonged hemiplegic migraine, and seizures during migraine attack. 63 The T666 M CACNA1A mutation is linked with high frequency of familial hemiplegic migraine, nystagmus and severe coma episodes. 64 Familial hemiplegic migraine type 2 is caused by a ATP1A2 mutation on chromosome 1q23, which encodes the pore forming a subunit of the Na+/K+-ATPase. 55 Epilepsy is present in 20% of these families. Epilepsy is more frequently associated with familial hemiplegic migraine type 2, in comparison to other familial hemiplegic migraine subtypes. 65 In families with comorbid migraine and epilepsy, in addition with a positive family history of either disorder, screening for ATP1A2 mutations might be considered. 66 Familial hemiplegic migraine type 3 is associated with a mutation in the SCN1A gene (located on chromosome 2q24), which encodes the alpha-1 subunit of the voltage-gated sodium channel. Dravet syndrome, genetic (generalized) epilepsy with febrile seizures plus, and several other types of epilepsy are also connected to this mutation. 62 Heterozygous missense mutation (Gln1489Lys) in the gene SCN1A might express similarly to CACNA1A mutations, with neuronal hyperexcitability and milder functional abnormalities. 67 Recently, the proline-rich transmembrane protein (PRRT2) gene (located on chromosome 16p11.2) was discovered as a cause of paroxysmal kinesigenic dyskinesia. Paroxysmal kinesigenic dyskinesia is characterized by movement-induced or stimulus-sensitive paroxysmal attacks and comorbidity with episodic ataxia, infantile convulsions, epilepsy, migraine, or hemiplegic migraine. 68 In fact, it is shown that PRRT2 mutations cause a spectrum of paroxysmal disorders, so hemiplegic migraine or epileptic syndromes may represent the main phenotypic manifestations. 69
Mitochondrial encephalomyopathy, lactic acidosis, and strokelike episodes (MELAS) is defined as a genetically heterogeneous mitochondrial disease, consisting of central nervous system signs and symptoms (seizure, hemiparesis, hemianopsia, cortical blindness, deafness, and/or occasional vomiting) and headaches. The headaches are either symptoms of strokelike episodes, or recurrent episodes of migraine-like attacks. 39 Biochemical findings suggest an impaired mitochondrial function that may lead to astrocyte and neuronal energy deficits and provoke cortical spreading depression. 70 Sturge-Weber syndrome is characterized by nevus flammeus and ipsilateral leptomeningeal angiomas, which can cause contralateral hemiparesis and hemiatrophy, glaucoma, seizures, and mental retardation. Focal seizures occur in 90% of patients, whereas 40% to 60% have associated migraine headaches. 71 Neurologic manifestations are most likely secondary to compression of the brain parenchyma by the leptomeningeal angioma, with consequential hypoxia. 16 Furthermore, it is postulated that frequent postictal headaches associated with Sturge-Weber syndrome could be due to epileptic hypersynchronization, facilitating cortical spreading depression. 72
EEG Findings
EEG abnormalities are often present in patients with hemiplegic migraine. Ictal and postictal EEG findings are often marked by a moderate to severe degree of delta activity in regions contralateral to the hemiplegia. 16 In a study by Brinciotti et al, 73 126 children diagnosed with epilepsy or migraine showed that unilateral occipital EEG spikes accompanied with the epileptiform photoparoxysmal response indicate epilepsy, whereas bilateral occipital changes with absence of epileptiform photoparoxysmal response were associated with migraine. Video EEG monitoring may be useful in differentiating between migraine aura and epileptic aura. Paroxysmal spikes, which are sometimes seen during migraine auras, can be similar to an ictal epileptiform EEG, with an important difference: EEG readings during migraine aura show alterations in amplitude separated by normal EEG activity, whereas ictal epileptiform EEG patterns show a higher frequency with lower amplitude and progression into rhythmic epileptiform discharge of high amplitude. 74
Overlap of Treatment and Prophylaxis
The use of conventional antiepileptic drugs has been supported by clinical studies in the prophylaxis of adult migraine. 2,4,6,8,15,16,75 In adults, valproate (500-1500 mg/d) and topiramate (200 mg/d) showed the strongest evidence for migraine frequency reduction, whereas the evidence for gabapentin (900-2400 mg/d) is still insufficient. 75 -77 Topiramate, Food and Drug Administration (FDA)-approved for the prophylaxis of migraine in patients aged 12 and older, previously has been shown to have efficacy for the prophylaxis of pediatric migraine in doses of 100 to 200 mg. 78 However, data from the CHAMP trial, assessing migraine prophylaxis in patients aged 8 to 17, have shown that topiramate and amitriptyline were not more effective than placebo for migraine prevention 79 ; 55% of patients with topiramate treatment experienced a reduction in the number of days with headache vs the placebo group with the same decrease in 61% of children. Although adult migraine trials of placebo show a 35% response rate, the pediatric trials with placebo show response rates of 50% or more, strongly suggesting a therapeutic benefit of placebo in the treatment of pediatric migraine. 80 It has been shown that valproate might be effective in prophylaxis of adult migraine, but the evidence is still lacking for pediatric migraine. 81 Lamotrigine showed efficacy in the treatment of Sturge-Weber syndrome with chronic headache and hemiplegic seizures. 82 The benefit of other antiepileptic drugs (pregabalin, zonisamide, levetiracetam) is not confirmed in the treatment of migraine. 2 Other non-antiepileptic prophylactic medications for migraine are tricyclic antidepressants, beta-blockers, and calcium channel blockers. 81 Calcium channel blockers (such as verapamil or flunarizine) may be effective in the prophylaxis of migraine, but are also occasionally used as an additional therapy in order to raise concentrations of antiepileptic drugs in the brain. 15 Flunarizine showed the highest clinical efficacy in migraine prevention at doses 0.1 to 0.2 mg/kg qid. 78 Its efficacy has been confirmed in the pediatric population, as well. 78,81
Nonpharmacologic treatments, such as vagal nerve stimulation, have been shown to be effective for both migraine and epilepsy. 83,84 Their effectiveness could be related to EEG desynchronization, change in thalamic blood flow, neurochemical change of cerebrospinal fluid, etc. 1 Dietary therapy has been effective in the treatment of epilepsy, especially drug-resistant epilepsy. A ketogenic diet is the preferred dietary treatment in pediatric and adult epilepsy. 85 For patients with complete absence of seizures after ketogenic diet initiation, discontinuation after 2 years can be considered, with 80% of those patients remaining seizure free after discontinuation. 86 Furthermore, a role for the ketogenic diet in migraine prevention has been assessed; a study of 96 overweight female migraine sufferers showed migraine reduction in those receiving the ketogenic diet compared to those on standard diets, with ketosis shown to be important in the efficacy of the diet for migraine prevention. Ketogenic diet treatment in a small group of pharmacoresistent adolescents with migraine did not result in significant migraine preventive effects. 86,87 The very small sample sizes of these studies and low compliance limit any conclusions drawn. Several other case reports indicate a possible benefit of the ketogenic diet in migraine treatment, but larger randomized controlled studies are needed. 87
Conclusion
Despite increasing clinical data, the overlap of migraine and epilepsy in the pediatric population remains a challenge for both classification and therapeutic strategies. In certain circumstances, such as in channelopathies, questions arise as to whether migraine and epilepsy are comorbid disorders or whether symptoms represent a single specific syndrome. A genetic etiology has been identified for some syndromes of migraine and epilepsy, but for other syndromes with overlap, the specific mutations or polygenic patterns of inheritance have yet to be identified. Finally, certain medications might be beneficial in both disorders. The latest findings suggest that pharmacodynamically effective agents in epilepsy might have a placebo effect on migraine in children. Further randomized, controlled clinical trials assessing pharmacologic and nonpharmacologic methods for the treatment of both disorders are needed in the pediatric population in order to initiate new therapeutic approaches.
Footnotes
Acknowledgments
Jasna Jancic is supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia (Grant No: 175031). John van den Anker is supported by NIH (K24DA027992, R01HD048689, U54HD071601) and the European Commission (TINN [223614], TINN2 [260908], NEUROSIS [223060]). Janko Samardzic is supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia (Grant No: 175076).
Author Contributions
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.The authors have no relevant conflicts.