
Abstract
Infants with congenital heart disease are at risk of impaired neurodevelopment, which frequently manifests as motor delay during their first years of life. This delay is multifactorial in origin and environmental factors, such as a limited experience in prone, may play a role. In this study, we evaluated the motor development of a prospective cohort of 71 infants (37 males) with congenital heart disease at 4 months of age using the Alberta Infant Motor Scales (AIMS). We used regression analyses to determine whether the 4-month AIMS scores predict the ability to walk by 18 months. The influence of demographic and clinical variables was also assessed. Fifty-one infants (71.8%) were able to maintain the prone prop position (AIMS score of ≥3 in prone) at 4 months. Of those, 47 (92.2%) were able to walk by 18 months compared to only 12/20 (60%) of those who did not maintain the position. Higher AIMS scores were predictive of a greater likelihood of walking by 18 months (P < .001), with the scores in prone having a higher predictive ability compared to those in other positions (Exp(B) 15.2 vs 4.0). Shorter hospital stays and female gender were also associated with an earlier onset of walking. In conclusion, our study demonstrates that early ventral performance in infants with congenital heart disease impacts the age of acquisition of walking and could be used to guide referral to rehabilitation.
Medical advances in pediatric cardiology and cardiac surgery have led to increased survival rates of infants with congenital heart disease (CHD). Concurrently, neurodevelopmental dysfunction has become the most disabling outcome, manifesting as both motor and/or cognitive impairments. 1 As such, there is an important need to develop efficient strategies to improve neurodevelopmental outcomes in this population.
Neurodevelopmental impairment in congenital heart disease is thought to arise from a complex combination of cumulative brain insults occurring both pre- and postnatally. 2 We increasingly recognize that neonates with congenital heart disease experience a delay in brain development and brain injury, which is detected in approximately 50% of patients, both before and after surgery. 3 –6 In addition, innate and environmental factors such as the genetic background and the length of hospital stay, respectively, have also been shown to affect neurodevelopment. 7 –9 As such, it is of utmost importance to gain a better understanding on how brain alterations and environment interact in order to reduce the burden of developmental disability in congenital heart disease and improve quality of life.
During infancy, impaired neurodevelopment primarily manifests as gross motor delay, which is observed in 62% of babies with congenital heart disease. 7 Both brain injury and limited motor experience may contribute to this delay. 8 Although motor delay tends to improve with age, 10,11 of concern is its persistence into the school age years and the emergence of a host of other problems that affect virtually all developmental domains. As many as 49% and 39% of preschool survivors of congenital heart disease present with gross motor and fine motor impairment, respectively, whereas 20% to 30% also experience language and core communication, cognitive, and behavioral problems. 10,12,13 Of note, in other at-risk populations such as preterm babies, early rehabilitation programs have shown benefits not only for motor but also for cognitive outcomes, 14 which underlines the importance of early intervention.
The long-term rehabilitation costs associated with treating children with congenital heart disease are unknown. However, a recent study highlights that overall medical costs are substantially higher for children with extra cardiac comorbid conditions. 15 Hence, identifying at-risk congenital heart disease patients and gaining a better understanding of how different modifiable factors affect neurodevelopment in infants with congenital heart disease may help develop interventions that will not only reduce the burden of overall developmental disability but may also decrease the health care costs.
At the neurocardiac follow-up clinic of Montreal’s Sainte-Justine University Hospital Center, we have observed that a significant proportion of babies with congenital heart disease are unable to acquire an optimal position in prone at 4 months, which may be due to a lack of early prone positioning owing to frequent hospitalizations, surgeries, pain, and parental apprehension. 1,7,10,11,16,17 However, the implications of prone vs supine positioning on the long-term motor development of infants remain unclear. Several studies of typically developing infants highlight the importance of the prone position on the acquisition of later motor milestones. 12,18,19 Others report that performance in both the supine and prone positions predict motor outcome. 20,21 Pin et al’s systematic review showed that healthy term and low-risk preterm infants having had less experience in prone initially presented with delayed development but walked independently within a normal time frame. 22 As the studies were limited to a normal and low-risk infant population, the authors recommended conducting studies on the effects of the prone position in non typically developing infants.
As such, in this longitudinal study, we hypothesized that a reduced motor performance in prone is associated with a later onset of walking in infants with congenital heart disease. Specifically, we sought to determine the impact of the performance in prone at 4 months on the ability to walk by 18 months. Furthermore, we explored how a series of disease-specific and environmental factors influence this relationship.
Methods
Participants
We recruited a prospective cohort of 88 infants presenting with congenital heart disease, followed longitudinally at the Clinique d’Investigation Neuro-Cardiaque (CINC) of the Sainte-Justine University Hospital Center between September 2013 and June 2017. The clinic was established in 2013 following recommendations by the American Heart Association and the American Academy of Pediatrics for systematic surveillance and early intervention in children with congenital heart disease. 1
Seventy one babies with congenital heart disease referred to the clinic who underwent standardized motor evaluations at 4 months ± 2 weeks and who had follow-up evaluations at 18 months ± 2 weeks were included in the study. A total of 17 babies were excluded: 12 patients had evaluations outside the pre-established 4- and 18-month time frames, 2 patients died and 3 had incomplete evaluations. The clinical and the available developmental characteristics of these patients were not different from those of the entire cohort. Babies with trisomy 21 or 22q11 deletion spectrum with congenital heart disease were not recruited for this study as they are followed in thematic clinics and not referred to the Clinique d’Investigation Neuro-Cardiaque.
Demographic, perinatal, diagnostic, surgical, critical care, and other clinical variables were collected from the medical charts (Table 1).
Clinical Characteristics of the Infants with Congenital Heart Disease (CHD).a
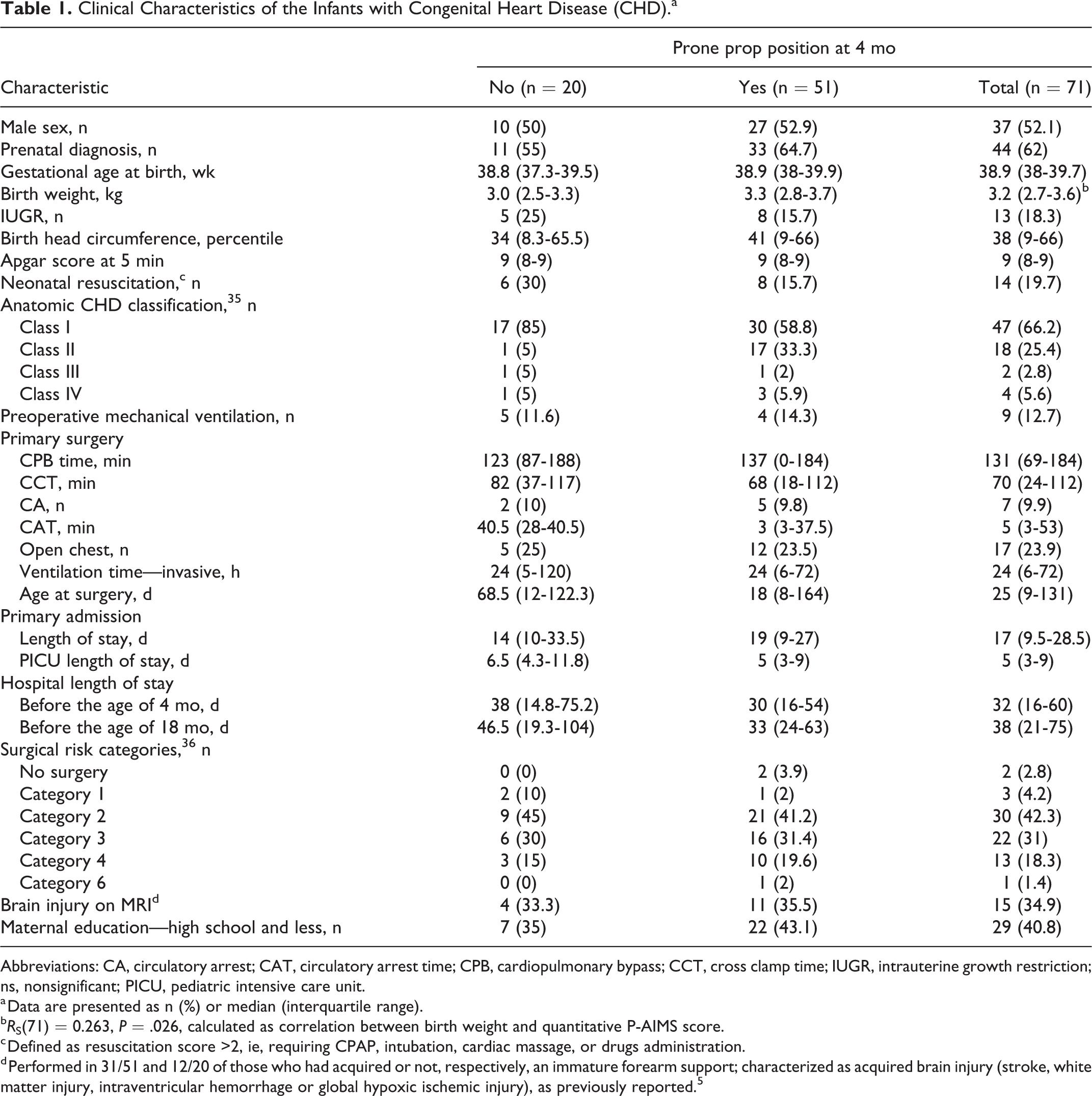
Abbreviations: CA, circulatory arrest; CAT, circulatory arrest time; CPB, cardiopulmonary bypass; CCT, cross clamp time; IUGR, intrauterine growth restriction; ns, nonsignificant; PICU, pediatric intensive care unit.
a Data are presented as n (%) or median (interquartile range).
bRS(71) = 0.263, P = .026, calculated as correlation between birth weight and quantitative P-AIMS score.
c Defined as resuscitation score >2, ie, requiring CPAP, intubation, cardiac massage, or drugs administration.
d Performed in 31/51 and 12/20 of those who had acquired or not, respectively, an immature forearm support; characterized as acquired brain injury (stroke, white matter injury, intraventricular hemorrhage or global hypoxic ischemic injury), as previously reported. 5
Evaluation of Motor Development
At 4 months ± 2 weeks of corrected age, gross motor development was assessed by certified physiotherapists using the Alberta Infant Motor Scales (AIMS) 23 , shown to be sensitive to motor impairment in congenital heart disease. 7 The AIMS is a standardized norm-based tool developed through observation of 2202 infants in Alberta from 1990 to 1992. It is deemed reliable and valid to quantify gross motor development from birth to 18 months of age. The intra- and inter-rater reliability of this standardized tool is excellent, with intraclass correlations of 0.99 for both. 23
The AIMS evaluates motor performance according to a total of 58 items scored in the supine, prone, sitting, and standing domains. The total raw AIMS score is derived by adding the scores in each of these domains, with a score of 1 given to each position observed. 24 We used the prone domain to quantify the ventral performance at the age of 4 months. Higher AIMS scores in this domain reflect a more mature antigravity movement repertoire. For instance, a score of 2 indicates the baby’s ability to raise his head while lying in prone; a score of 3 reflects the ability to maintain the prone prop position with elbows behind the shoulders; and a score of 4 represents the baby’s capacity to raise his head and chest while weight-bearing on the forearms. To differentiate between the impacts of the performance in ventral as opposed to all other domains, we retained for analyses the raw scores in prone (P-AIMS) as opposed to the sum of the raw scores in the supine, sitting, and standing domains (3S-AIMS).
We noted the toddler’s ability or inability to walk by 18 months ± 2 weeks as documented in the medical chart from the physicians’ reports or the physiotherapists’ evaluations. The ability to walk was defined as the ability to take at least 5 steps unaided. 23
Statistical Analyses
Descriptive statistics were used to characterize the total group of infants with congenital heart disease and to differentiate between the infants having achieved the prone prop position with elbows behind the shoulders at the age of 4 months as opposed to those who had not (P-AIMS ≥ 3 and P-AIMS ≤ 2, respectively). Frequencies (sample size and percentages) were reported for dichotomous and categorical variables (Table 1). Median and interquartile ranges were reported for continuous variables. The groups (P-AIMS ≥ 3 and P-AIMS ≤ 2) were compared using the Mann-Whitney U test and the Spearman rank correlation coefficient for dichotomous and continuous clinical variables, respectively.
Logistic regression analyses were used to appreciate the association of the P-AIMS and 3S-AIMS scores at 4 months and their interaction with the ability to walk independently by 18 months. The influence of a series of risk factors (Table 1) was assessed using stepwise selection and P < .1 as selection criterion. We used the Box-Tidwell procedure to test for linearity between predictors and outcomes.
Significance level was set to P < .05.
Results
Clinical and Developmental Characteristics
Clinical characteristics of the recruited cohort are presented in Table 1. Patients who achieved the prone prop position with elbows behind the shoulders at 4 months of age (P-AIMS ≥ 3) were similar to those who did not, except for a higher birth weight (P = .026).
Of the 71 infants included in our study, 51 (71.8%) were able to maintain the prone prop position at 4 months ± 2 weeks. Of the 51 who achieved this milestone, 47 (92.2%) were able to walk by 18 months compared to only 12/20 (60%) of those who did not.
Predictive Value of the 4-month Performance in Prone Compared to other Positions
The results of the univariate and multivariable regression analyses are presented in Table 2. A multivariable analysis demonstrated that both P-AIMS and 3S-AIMS scores independently predicted the likelihood of walking by the age of 18 months, with the scores in prone having higher predictive ability (Exp(B) 15.2 vs 4.0). Additionally, girls compared to boys were more likely to walk by 18 months, and the length of hospital stay before 18 months of age had a small but significant contribution to the model.
Predictors of Walking Assessed using Logistic Regression.
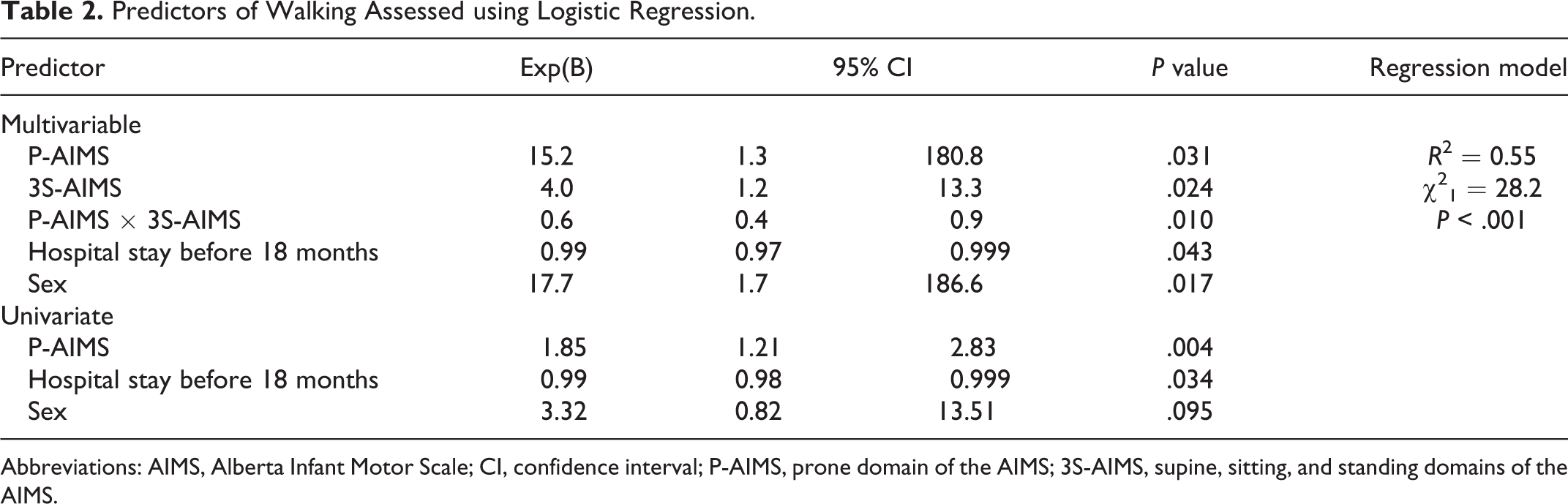
Abbreviations: AIMS, Alberta Infant Motor Scale; CI, confidence interval; P-AIMS, prone domain of the AIMS; 3S-AIMS, supine, sitting, and standing domains of the AIMS.
Discussion
We increasingly recognize the burden of developmental disability in congenital heart disease, primarily manifesting as a delay in motor development during the first months of life. 1,7,8,10,11 This study was specifically carried out to investigate the impact of the prone performance on motor development in a cohort of babies with congenital heart disease. We demonstrated that at 4 months of age, the AIMS scores in prone rather than the cumulative scores in supine, sit, and stand predicted the ability to walk by 18 months of age. Both innate and environmental risk factors influenced this association. Not surprisingly, longer total hospital stays interfered with gross motor development throughout infancy and worsened motor outcomes. Furthermore, girls were more likely than boys to walk by 18 months.
Currently, important collaborative efforts are under way to identify modifiable risk factors that may improve outcomes in congenital heart disease. Our study contributes to these efforts by illustrating that the inability to maintain the prone prop position at 4 months may lead to a later onset of walking in this population. Of the infants included in our study, only 72% were able to maintain the prone prop position at 4 months, whereas as many as 90% of babies in the general population reach this milestone at just prior to 3 months of age. 23
Our study also carefully identified demographic, perinatal, diagnostic, surgical, critical care, and other clinical variables that might influence the ability of early prone performance to predict motor development. Consistent with previous reports, 7 –9,25 a longer cumulative hospital stay had a weak but detrimental effect on the age of onset of walking. Hospital stay may reflect surgical complexity and need for postoperative support, and early discharge might not be an option. However, similar to other studies, 26,27 cardiac anatomy, intraoperative, and surgical complexity variables had no decisive effect on neurodevelopmental outcomes. In light of these findings, promoting early ventral experience may palliate the effects of lengthy hospitalizations and represent a promising avenue for improving motor outcomes. Our and others’ data 25,28 suggest that early intervention might be even more important in boys who are at a greater risk of motor impairment compared to girls, which might be explained by their increased vulnerability to hypoxic-ischemic brain injury. 29 Altogether, the 4-month AIMS performance, the length of hospital stay, and gender accounted for 55% of the likelihood of walking by 18 months. This is high enough to justify 4-month developmental screenings to identify patients with congenital heart disease at risk of motor impairment and guide referral to rehabilitation services.
Accumulating evidence suggests an important role of antenatal and preoperative factors at the origin of neurodevelopmental impairment in congenital heart disease. 2 –5 Consistent with these data, our study shows lower birth weights in babies who were not able to maintain the prone prop position at 4 months. However, birth weight did not influence the relationship between the 4-month performance in prone and the ability to walk at 18 months.
Our study could not establish an association between brain injury, detected on the brain magnetic resonance imaging (MRI) scans, and motor development. A recent study reported an association between perioperative white matter injury and worse school-age cognition, whereas motor problems were observed only in cases of posterior limb of internal capsule involvement. Our study could not bring new arguments in this sense as MRI scans were performed in less than two-thirds of patients. 30 Only 3 of them had moderate-to-severe white matter injury, with no posterior limb of internal capsule involvement, and only 1 out of 3 was still not walking at the age of 18 months. Furthermore, we cannot exclude the presence of perioperative brain injury in those not submitted to brain imaging as it remains clinically silent in most neonates with congenital heart disease undergoing surgery. 31
Even in the absence of brain injury, recent data suggest that preoperatively delayed brain development may lead to functional connectivity alterations. 5,32 Functional connectivity is understood to reflect covariance of activity between cortical areas, enabling the emergence of complex behavior and cognition. It would be interesting to investigate in future prospective studies whether connectivity perturbations contribute to impaired neurodevelopment and whether early intervention such as early prone positioning can modify connectivity patterns.
At the Clinique d’Investigation Neuro-Cardiaque, all patients with congenital heart disease undergo interdisciplinary developmental evaluations at the age of 4 months. Consequently, all of the babies who were unable to maintain the prone prop position at 4 months were referred to physiotherapy. In the absence of a control no-intervention group, we can only presume the beneficial effects of encouraging prone positioning in babies with congenital heart disease. Accordingly, multiple studies document a higher risk of motor delay in healthy babies with a reduced experience in prone. 16,17 Hence, we speculate that an intervention prior to the 4-month visit at the clinic may have been even more beneficial as professionals could have educated the families as to the importance of early and frequent positioning in prone during wake times, while respecting the baby’s tolerance. Moreover, our study did not systematically collect data on the time spent in prone during waking hours prior to the acquisition of walking, which is also a limitation. These data would have enabled us to determine the impact of the prone experience on walking in a more exclusive and quantifiable manner.
At the Sainte-Justine University Hospital Center, cardiac surgeons now encourage prone positioning of the infants during wake times as soon as 48 hours following surgery or after they are extubated. Prone positioning with bilateral pillows to avoid compression of the anterior chest wall early after the surgery was shown to improve respiratory distress. 33 For those with an open sternum following surgery because of extracorporeal membrane oxygen or other reasons, the ventral position is postponed until closure. The babies included in our cohort did not receive systematic developmental interventions during their hospital stay, with the exception of chest physiotherapy. The practice is now changed and we encourage prone positioning as babies tolerate it remarkably well.
Finally, we cannot rule out that babies referred to our clinic were more severely affected and selected to receive more intense intervention. However, such a selection bias should have decreased rather than increased the association between the performance in prone and the ability to walk.
In further studies, it would be of interest to evaluate the impact of the prone experience on motor function as well as on other spheres of development at school age. It would also be beneficial to reproduce this study with other pediatric populations in order to establish generalizability of the prone prop position as a motor sign for later development.
Conclusions
Our study supports the multifactorial origin of developmental delay in congenital heart disease and demonstrates that early ventral performance is predictive of the onset of walking in this population. We suggest that parents should be encouraged and educated to place their infants with congenital heart disease in the prone position during wake times as early as possible during infancy, while respecting their tolerance and medical limitations. Similar to the endorsement of “tummy time” by the American Academy of Pediatrics for typically developing infants, physicians should also advocate frequent prone positioning for short periods for this vulnerable population. 34 This could help reduce motor impairment and may prove to be more cost effective for society in the long term. Furthermore, we propose that the inability to maintain the prone prop position at 4 months should warrant consideration for early referral to rehabilitation for babies with congenital heart disease.
Footnotes
Acknowledgments
We are grateful to all patients and their families who participated in this study.
Author Contributions
LD, MM, BD, MCV, AD, JP, KG, ML, AMN, NP, LBG, LC, and AB contributed to conception and/or design. LD, MM, and AB drafted the manuscript. All authors contributed to data analysis and interpretation and critical review, and approved the final manuscript as submitted.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Garnier Kids Foundation, the Mach-Gaensslen Foundation of Canada, the “Conseil Multidisciplinaire” of the Sainte-Justine University Hospital Center (SJUHC) and the SJUHC Research Center.
Ethical Approval
The study was approved by the Sainte-Justine University Hospital Center research ethics board (IRB number 2017-1356). Parents provided written informed consent for their children’s participation and for the publication of the results.