
Abstract
The purpose of this study is to investigate the surgical results and long-term outcomes of encephaloduroarteriosynangiosis for moyamoya disease in pediatric patients. We performed a retrospective analysis of 67 pediatric patients with moyamoya disease who underwent encephaloduroarteriosynangiosis in Beijing Tiantan Hospital. The case series included 36 boys and 31 girls. All the patients underwent surgical revascularization, and a total of 93 encephaloduroarteriosynangiosis procedures were performed (41 unilateral, 26 bilateral). The mean follow-up period after surgery was 30 months. During follow-up, ischemic stroke events were detected in 5 patients and the stroke rate for pediatric patients who underwent encephaloduroarteriosynangiosis procedure was 7.1% per patient-years. At the last follow-up, favorable outcomes (modified Rankin Scale score ≤ 2) were observed in 65 cases (97.0%). Our study suggests that long-term surgical outcome of encephaloduroarteriosynangiosis in pediatric moyamoya disease patients is satisfactory, and this technique has a positive impact on the prevention of stroke recurrence.
Moyamoya disease is a chronic and progressive cerebrovascular disorder of unknown etiology, which is clinically characterized by bilateral stenosis or occlusion at the terminal portion of the internal carotid artery and its main branches within the circle of Willis, following by spontaneous development of abnormal vascular networks at the base of the brain (moyamoya vessels). 1,2 Moyamoya disease is the most common pediatric cerebrovascular disease in Eastern Asian countries, 3 and it has various initial clinical manifestations, including transient ischemic attack, infarction, hemorrhage, headache, and epilepsy. Pediatric patients with moyamoya disease mainly present with ischemic strokes, whereas hemorrhagic stroke is frequently observed in adults.
Currently, surgical revascularization is considered as the standard treatment for moyamoya disease that could prevent strokes by augmenting blood flow to the affected cerebral hemispheres. The most commonly used surgical modalities include direct bypass, indirect bypass, and combined bypass. All these revascularization procedures have been used successfully to treat patients with moyamoya disease. However, children’s donor or recipient vessels usually have smaller calibers and are more fragile than those of adults; direct revascularization is frequently technically not feasible. Therefore, pediatric patients with moyamoya disease are mainly treated with indirect bypass. Encephaloduroarteriosynangiosis, as an effective surgical modality of indirect bypass, is frequently used for the treatment of pediatric moyamoya disease in our hospital.
Given the above background, we undertook this retrospective study to review clinical and surgical data in a single-center pediatric moyamoya disease series, trying to delineate the clinical features, surgical results, and long-term outcomes after encephaloduroarteriosynangiosis in these patients.
Patients and Methods
Patient Population
We reviewed 696 consecutive moyamoya vasculopathy patients who were treated in Beijing Tiantan hospital from 2009 to 2015. The study protocol was approved by the Research Ethics Board of Beijing Tiantan Hospital, Capital Medical University. All individual participants (parent or guardian) gave their informed consent before their inclusion in this study. Moyamoya disease was diagnosed by neurologists or neurosurgeons according to the criteria of the Research Committee on Spontaneous Occlusion of the Circle of Willis. 2 Patients with moyamoya syndrome secondary to the identified etiologies (including history of vasculitis, neurofibromatosis, tuberous sclerosis, retinitis pigmentosa, fibromuscular dysplasia, Down syndrome, sickle cell disease, and others) were excluded from this study. Patients who were lost to follow-up and patients with different bilateral operations were also excluded.
Baseline data of these patients were collected, including demographic data, initial presentation, treatment, and neurologic outcome. Disease duration was defined as the time interval between symptom onset and hospital admission. For patients with recurrent stroke, the disease duration was calculated from the time the patient presented with first-ever stroke to the time of hospital admission. According to the clinical manifestations, we divided the patients into three groups: Group A were patients presented with intracranial hemorrhage, Group B were cases with ischemic strokes (transient ischemic attack and cerebral infarction), and Group C were children with other symptoms (seizures and headache). The imaging data of these patients were independently examined on picture archiving and communication system (PACS) by two neurologists blinded to patients’ clinical information. When the initial interpretation differed between the two investigators, the final decision was reached by consensus. The number of neurologic events, including transient ischemic attack, cerebral infarction, and intracranial hemorrhage, were measured for each patient before and after operation. Modified Rankin Scale (mRS) score was used to assess the neurologic status of the patients at the initial visit, discharge, and the last follow-up. In our hospital, we do not perform surgical revascularization in the acute phase of stroke. Patients with ischemic stroke were admitted about 2 to 3 months after the stroke onset, and the initial modified Rankin Scale score was obtained at the time of admission.
Anesthesia and Surgical Treatment
All children received general anesthesia, which was induced with propofol, fentanyl, and rocuronium, and maintained with total intravenous anesthesia. After the patient was intubated, the end-tidal CO2 was closely measured and maintained in the range of 35-45 mmHg to achieve normocarbia. The minimum systolic blood pressure limit for anesthesia was determined according to the preoperative baseline systolic blood pressure of the patient. Intraoperative hypotension was avoided by partially replacing fluid deficits. Urine output should be kept at 2 to 4 mL/kg/h for each patient.
The surgical technique for encephaloduroarteriosynangiosis in our center has been published previously. 4 During operation, the superficial temporal artery and accompanying cuff of the galea connective tissue were meticulously dissected from the skin and temporalis fascia. Subsequently, the craniotomy was performed and the dura was opened, we sewed the superficial temporal artery onto the brain surface, and folded the dural flaps into the dural-epiarachnoid space to recruit the middle meningeal artery circulation for angiogenesis.
Postoperatively, patients were transferred to the postanesthesia care unit for observation until they were fully awake. During this period, an anesthesiologist performed hourly neurologic examinations and monitored the vital signs for the patients. Proper pain management strategy was used to prevent persistent crying and hyperventilation of the patients. In our hospital, antiepileptic drugs were routinely administered for patients who underwent encephaloduroarteriosynangiosis procedure. Because the effectiveness of medication has not been established, antiplatelet therapy is not used postoperatively for children with moyamoya disease. Patients were discharged from hospital when they were considered in stable neurologic status.
In our hospital, the following principles of the surgical strategies were used. First, because pediatric moyamoya disease is characteristically progressive, the patients should be treated aggressively. We offered revascularization surgery to all pediatric patients. For patients with a specific symptomatic side, the symptomatic hemisphere was the first choice for revascularization surgery. Otherwise, according to the results of computed tomographic (CT) perfusion, the hemisphere with lower perfusion was the preferred side for operation. Second, after the first surgery, if the patient’s symptoms improved significantly and the patient did not present with symptoms of the contralateral hemisphere, an operation in the contralateral hemisphere was not considered. Third, combined and direct bypass were preferred surgical modalities for most patients; indirect bypass was performed only when the donor or recipient vessel was too small or fragile to perform artery anastomosis.
Follow-up
Follow-up information for all the patients was obtained by telephone interview or personal outpatient review. Patients were followed up at 3 to 6 months after revascularization and yearly thereafter. We inquired about (1) information of stroke events, including cerebral ischemic events and intracranial hemorrhage; (2) neurologic status (modified Rankin Scale score), which was dichotomized at ≤2/>2 to define favorable/unfavorable functional outcomes; and (3) death events. Postoperative recurrent stroke was defined as new neurologic deficits lasting more than 24 hours with radiologic evidence of a new infarct or hemorrhage on magnetic resonance (MR) or CT imaging.
Statistical Analysis
Statistical analyses were performed using SPSS software (version 21.0; Chicago, IL). Continuous variables were expressed as the mean ± standard deviation, and categorical variables were reported as the absolute number and valid percentage. The Student t test or Mann-Whitney U test was used to analyze differences in the mean or median of continuous variables between groups, as appropriate. The chi-square test or Fisher exact probability test was adopted to analyze differences in categorical variables. Ordinal variables (modified Rankin Scale scores and Suzuki stages) were analyzed using the Wilcoxon rank-sum test. Kaplan-Meier analysis was performed to estimate stroke-free survival. P values less than .05 were considered statistically significant.
Results
Demographic Data and Clinical Manifestations
Between 2009 and 2015, a total of 162 consecutive pediatric moyamoya disease patients (including the 155 patients in the previously published literature) 4 were treated in Beijing Tiantan hospital. Among them, 151 cases (93.2%) received surgical revascularization; 67 children who underwent unilateral encephaloduroarteriosynangiosis or bilateral encephaloduroarteriosynangiosis were included in this study (see Figure 1 and Supplemental Material 1). No significant differences in baseline characteristics were detected between the included and excluded patients. The demographic data and clinical characteristics of the patients are summarized in Table 1. There were 36 boys and 31 girls, and the sex ratio was 0.9:1 female-male. The age at diagnosis ranged from 3 to 18 years; the mean age was 9.8 years (Figure 2). The most common initial manifestation was transient ischemic attack (n=31, 46.3%), followed by cerebral infarction (n=19, 28.4%), headache (n=7, 10.4%), seizures (n=6, 9.0%), and intracranial hemorrhage (n=4, 6.0%). The duration of symptoms before hospital admission ranged from 2 weeks to 165.1 months (mean 25.9 months), and the mean disease durations were 4.7, 26.1, and 31.8 months in groups A, B, and C, respectively.
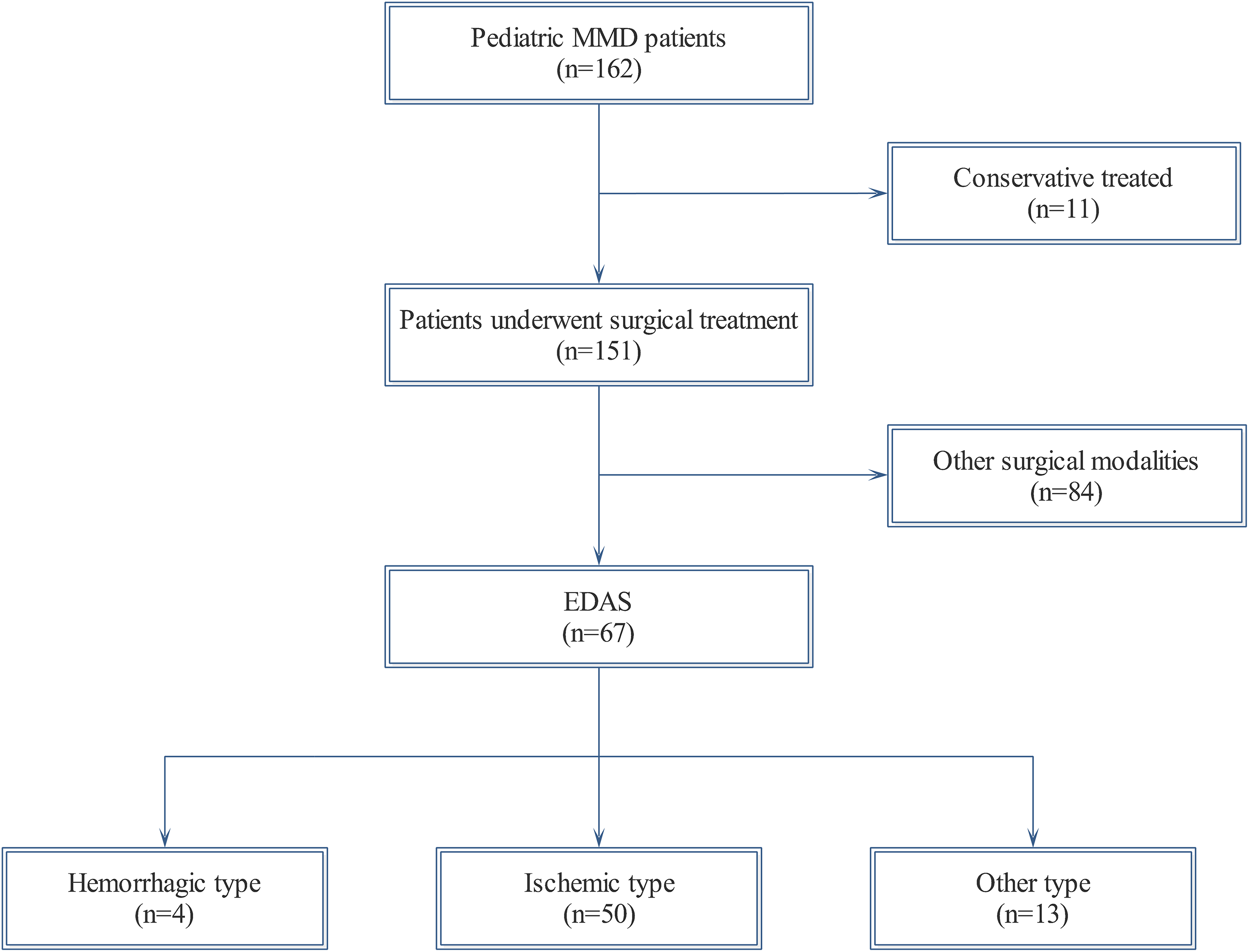
Flow diagram of the study participants.
Baseline Characteristics of the Included Pediatric Patients With Moyamoya Disease.
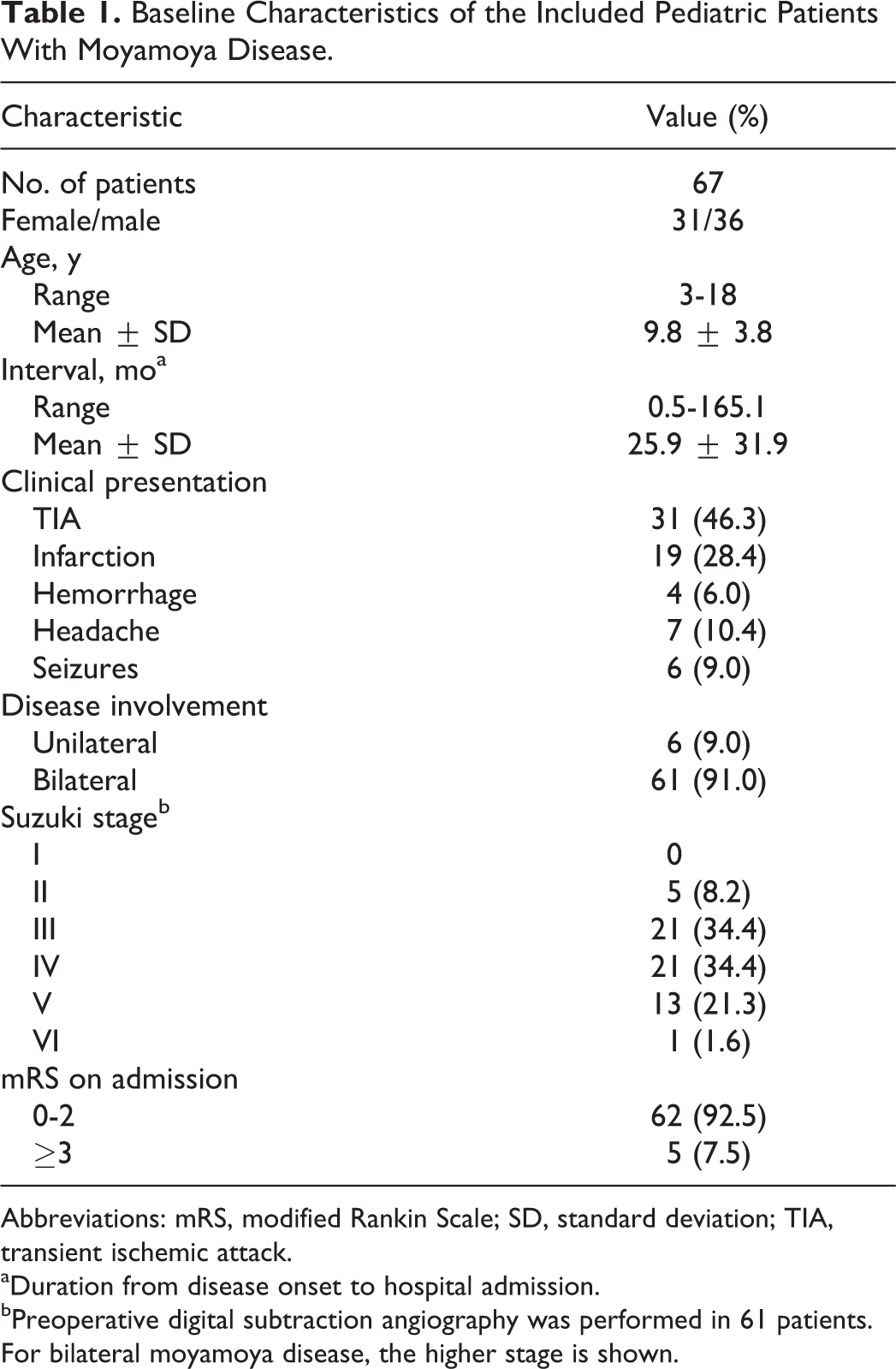
Abbreviations: mRS, modified Rankin Scale; SD, standard deviation; TIA, transient ischemic attack.
aDuration from disease onset to hospital admission.
bPreoperative digital subtraction angiography was performed in 61 patients. For bilateral moyamoya disease, the higher stage is shown.
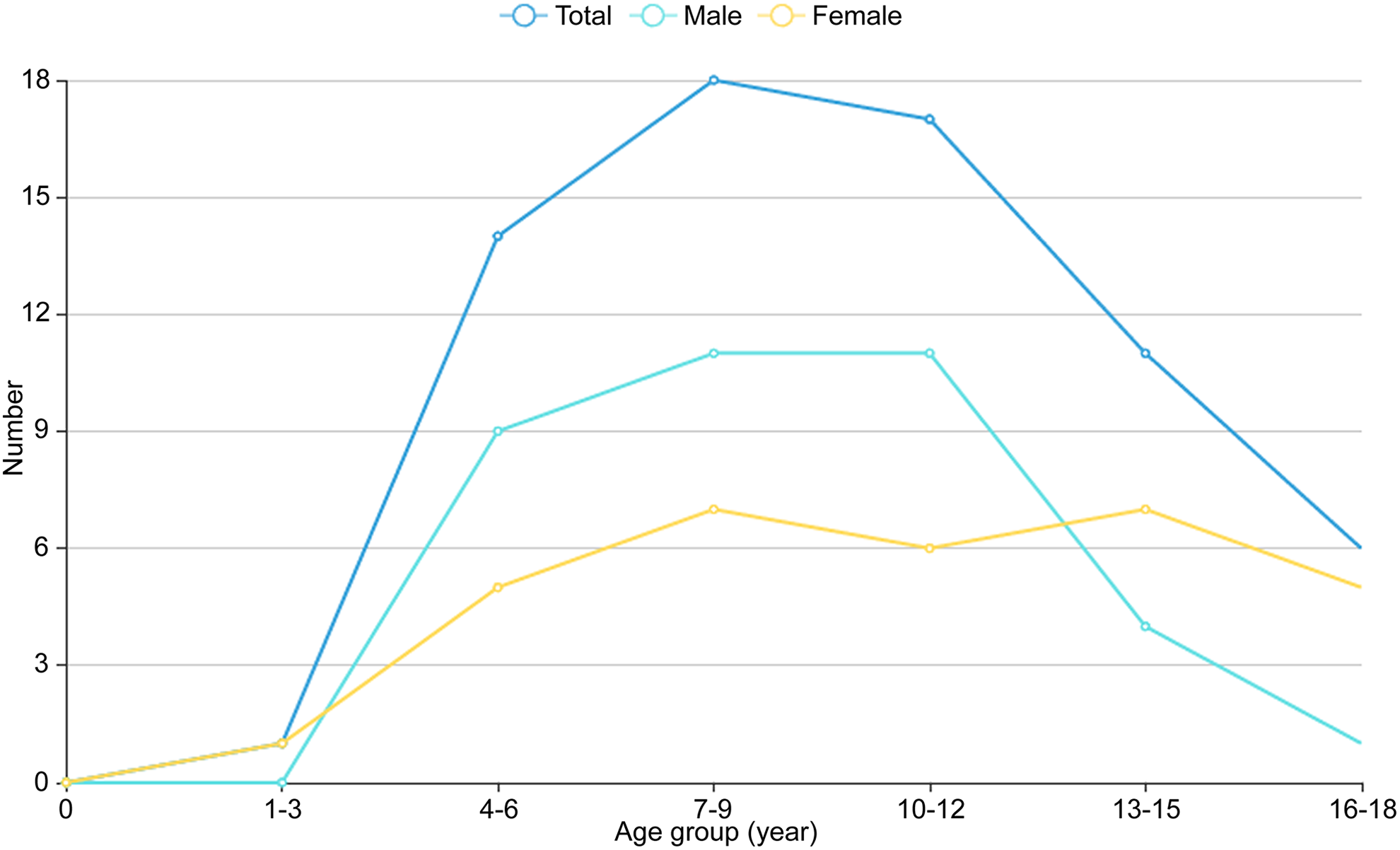
Age distribution of the 67 pediatric patients with moyamoya disease.
According to preoperative digital subtraction angiography or magnetic resonance angiography results, 6 patients (9.0%) were diagnosed with unilateral moyamoya disease and 61 patients (91.0%) with bilateral involvement. Preoperative digital subtraction angiography images were obtained and analyzed in 61 cases (91.0%); the majority of our series presented with Suzuki angiographic grade III or IV (68.8%). Thirty-four patients (50.7%) underwent preoperative CT perfusion examination; 22 of them (64.7%) had decreased cerebral blood flow, and 24 patients (70.6%) had abnormal cerebral blood volume. The mean modified Rankin Scale score on admission was 1.5 ± 0.7; 5 patients (7.5%) had significant disability (modified Rankin Scale score ≥3) on admission. There was no significant difference in the modified Rankin Scale score across different groups (P = .836).
Treatment, Outcomes, and Follow-up
Surgical findings and clinical outcomes are summarized in Table 2. All the patients underwent surgical revascularization and a total of 93 encephaloduroarteriosynangiosis procedures were performed, including 41 unilateral and 26 bilateral surgery. The mean surgical duration was 146 minutes (range, 70-300 minutes); there was no significant difference between different groups (P = .374). Postoperative complications were detected in 2 cases (3.0%), both experienced a new infarction within 48 hours after revascularization.
Summary of Surgical Findings and Clinical Outcomes of the Patients.
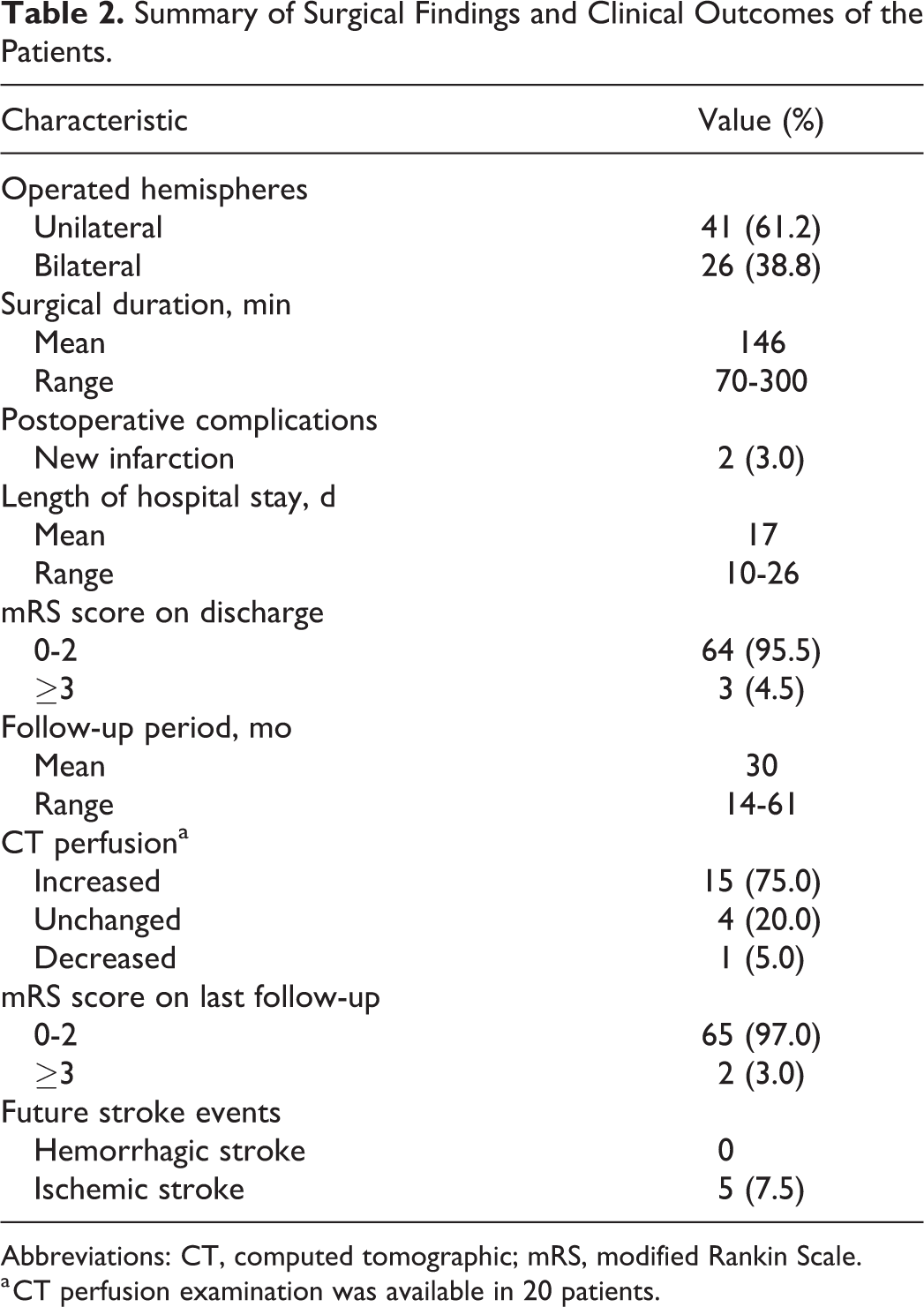
Abbreviations: CT, computed tomographic; mRS, modified Rankin Scale.
a CT perfusion examination was available in 20 patients.
The follow-up period ranged from 14 to 61 months, with a mean of 30 months. No patient died in the postoperative period. Of the 20 patients (29.9%) who underwent CT perfusion examination during follow-up, 15 (75%) had improved cerebral blood flow in previous hypoperfused areas, 4 cases (20%) had no change, and one child (5%) had decreased cerebral blood flow. During follow-up, ischemic stroke events were detected in 5 patients (4 cases in group B, 1 case in group C). No hemorrhagic event was observed. The shortest interval from revascularization surgery to stroke event was 1 month, and the longest was 30 months, with a median interval of 7 months. The stroke rate for pediatric patients who underwent encephaloduroarteriosynangiosis procedure is 7.1% per patient-years. The Kaplan-Meier curve for the stroke-free interval is shown in Figure 3. The mean number of neurologic events before surgery was 1.21, and this figure had gone down to 0.07 postoperatively at the time of the last follow-up (P < .001).
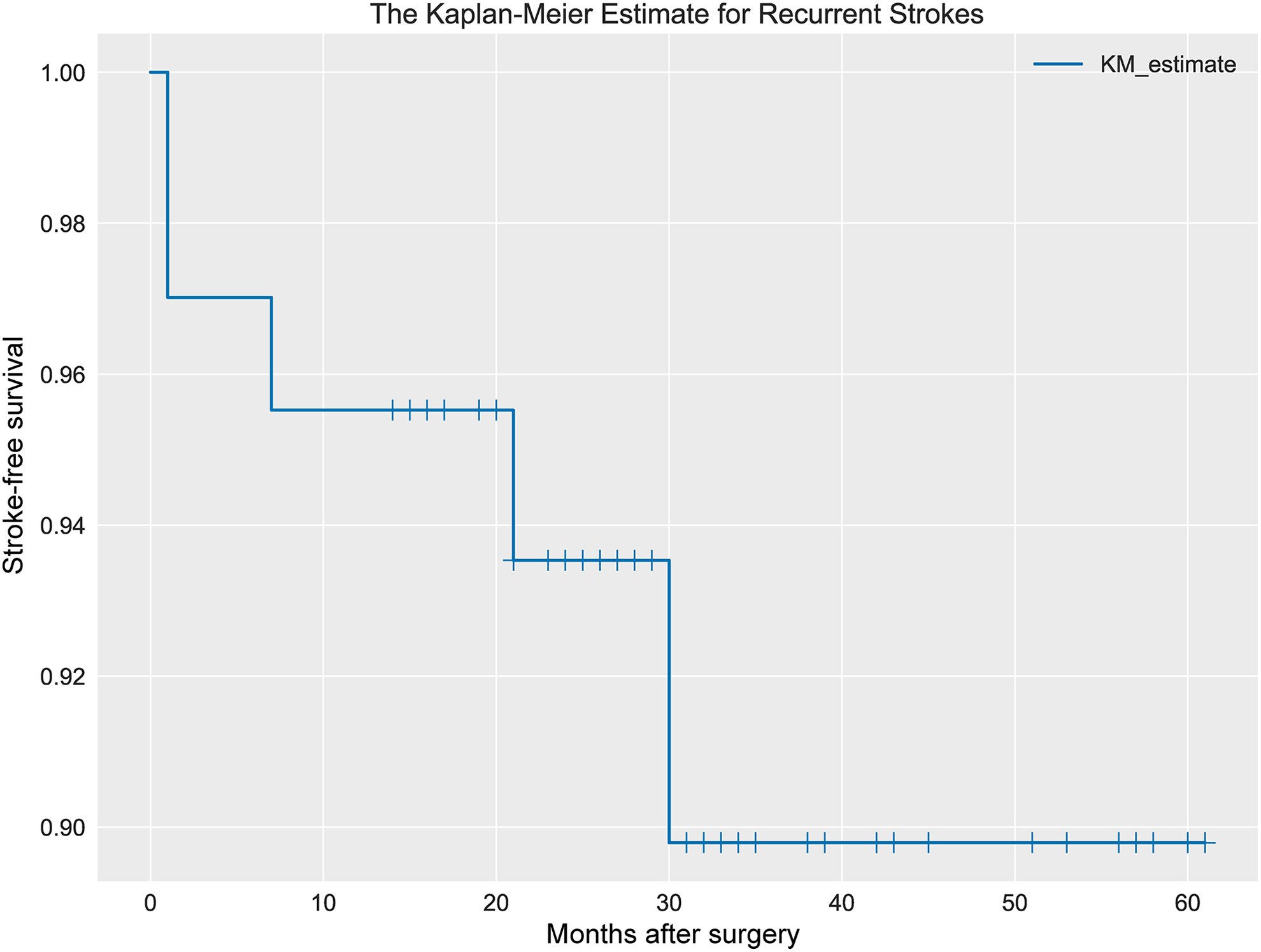
Kaplan-Meier curve for stroke-free survival after surgery for pediatric patients treated by encephaloduroarteriosynangiosis.
The functional outcomes are shown in Table 3 and Figure 4. After revascularization surgery (average length of stay, 17.0 days), neurologic status was improved in the majority of patients (n=51, 76.1%) and unchanged in 14 cases (20.9%). Two patients (3.0%) exhibited a deteriorated functional outcome due to moyamoya disease progression. At the last follow-up (mean follow-up period, 30 months), favorable outcomes (modified Rankin Scale score ≤ 2) were observed in 65 cases (97.0%), and the mean modified Rankin Scale score was significantly lower than that on admission (P < .001).
Summary of Preoperative Status and Functional Outcomes at the Last Assessment.
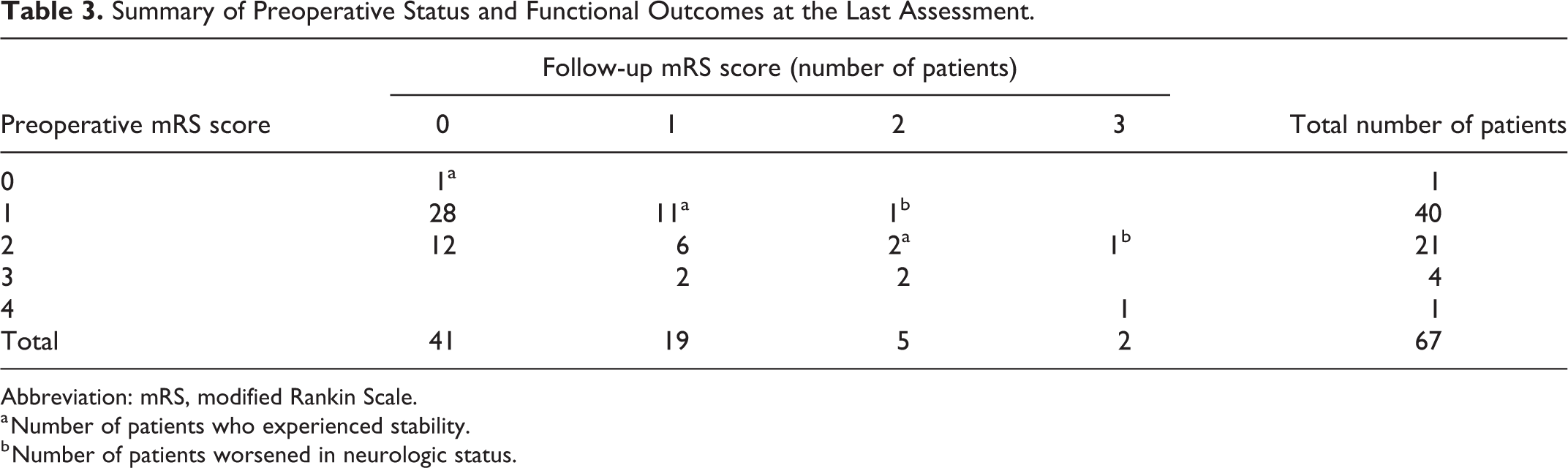
Abbreviation: mRS, modified Rankin Scale.
a Number of patients who experienced stability.
b Number of patients worsened in neurologic status.
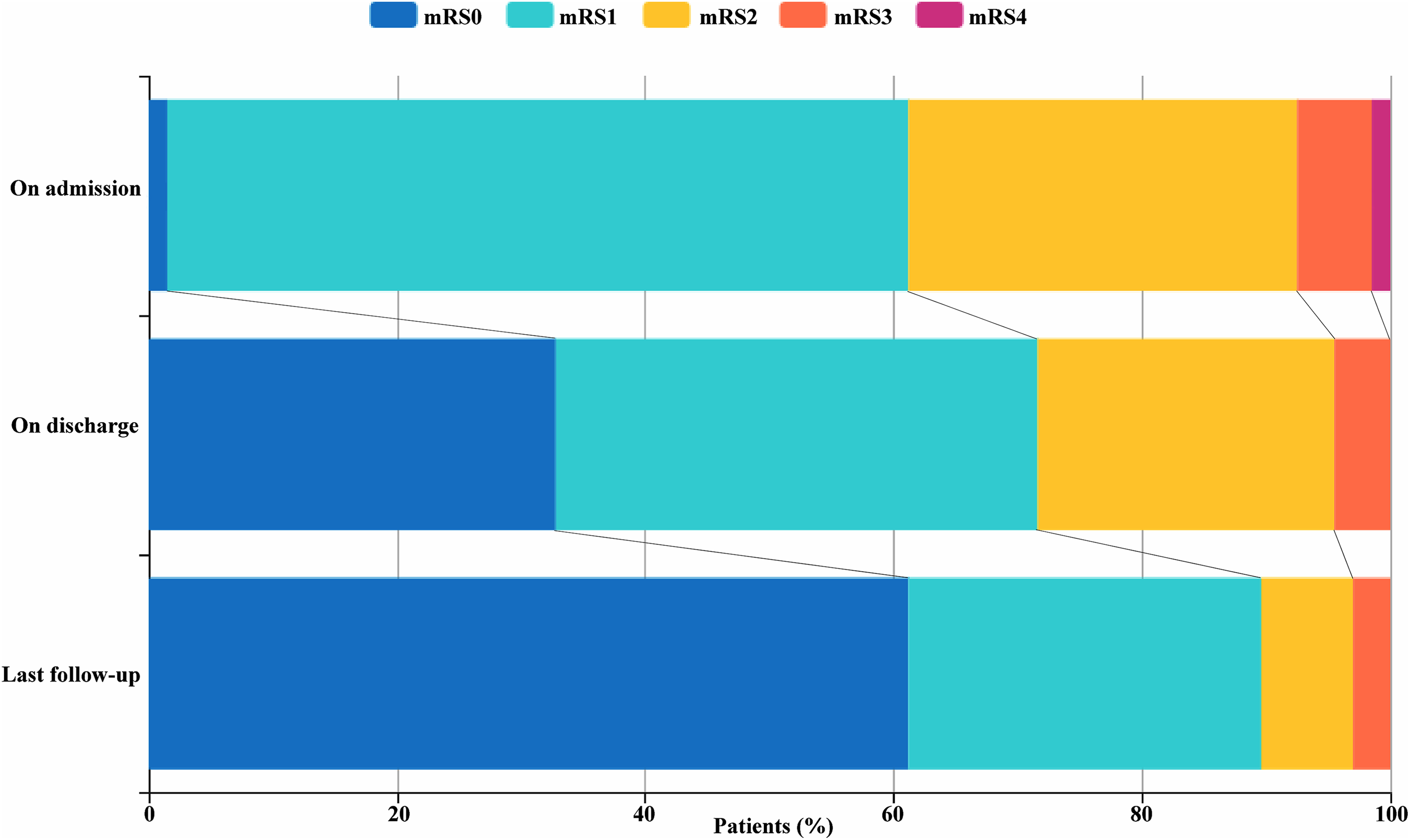
Stacked bar chart demonstrating the distribution of the mRS scores in pediatric patients with moyamoya disease at different time points. On admission: the mean disease duration was 25.9 months. On discharge: the mean length of hospital stay was 17 days. Last follow-up: the mean follow-up period was 30 months. mRS, modified Rankin Scale.
Discussion
Moyamoya disease is a rare cerebrovascular disease mainly found in East Asian countries. In recent years, the number of patients diagnosed with moyamoya disease has increased significantly in China, which may be due to the wide use of MR or CT angiography examinations. In the current study, we presented a relatively large series of pediatric moyamoya disease patients treated with encephaloduroarteriosynangiosis from a single neurosurgical center. Our results indicated that encephaloduroarteriosynangiosis showed a protective effect on the stroke recurrence in pediatric moyamoya disease patients.
According to epidemiologic studies, there are 2 age peaks of incidence in moyamoya disease: the first peak occurs in children who are approximately 5 years of age and the second in adults in their mid-40s. 3 The present study also supported the age peak in children, but the peak was at 7-9 years. In addition, the peaks of age distribution were similar between boys and girls (Figure 2). Moyamoya disease was reported to have a female predominance in other countries, with a sex ratio (male-female) of 1:1.8 to 4.25. 5 -7 In our cohort, the sex ratio was female-male 0.9:1, which demonstrated that there was no obvious difference in the sex distribution. Our results are in accordance with the previous studies in mainland China. 8,9
The clinical presentation of moyamoya disease is highly variable. Ischemia and hemorrhage are the two most common types of moyamoya disease in Asian populations. 3,7,9 Pediatric patients with moyamoya disease usually present with ischemic symptoms, especially transient ischemic attack, which is provoked by hyperventilation. 10 This was also observed in our series; ischemic type accounted for 74.6% of all the patients, and transient ischemic attack was the most common initial presentation. Seizures and headache are also common presentations in pediatric patients, with the prevalence to be approximately 5% and 21.6%, respectively. 11,12 As shown in Table 1, there are 6 patients (9.0%) presented with seizures and 7 patients with headache (10.4%) in our series. The pathogenesis of seizures and headache in moyamoya disease remains unclear; it has been reported that both symptoms could be cured after revascularization procedures, suggesting the causes may lie in cerebral hypoperfusion. 12 Digital subtraction angiography was considered as the most important diagnostic examination for moyamoya disease; the majority of patients in our cohort presented with Suzuki angiographic grade III or IV (68.8%), which tallied with previous studies. 10,13 -15
As the pathogenesis of moyamoya disease is still unknown, there is no definitive medical treatment that could inhibit the disease progression or stabilize the course of moyamoya disease. 10 Bypass surgery is gaining acceptance as the primary treatment strategy for moyamoya disease nowadays. The goal of surgical revascularization is to augment cerebral blood flow and to prevent further stroke events in moyamoya disease patients. Hitherto, various direct and indirect surgical modalities have been advocated for the treatment of moyamoya disease, but the optimal surgical procedure remains controversial. Compared with direct bypass, indirect revascularization is easier to perform and more feasible in patients whose donor or recipient vessels are inadequate. 3 Encephaloduroarteriosynangiosis is the most commonly used indirect procedure in our hospital. 4 Theoretically, direct bypass could improve cerebral hemodynamics immediately after operation. Indirect procedures can also lead to surgical collaterals but it may take up to 4 months for neoangiogenesis to develop. 16 In the last few years, many studies on the effects of encephaloduroarteriosynangiosis in pediatric patients have been reported. 17 Bao et al 10 performed 512 encephaloduroarteriosynangiosis procedures in 288 pediatric patients; they observed 20 stroke events occurred in 17 cases (5.9%) during follow-up, and they found that the older age of symptom onset was related to favorable outcomes. In another study, encephaloduroarteriosynangiosis was performed on 43 hemispheres of 23 pediatric patients; excellent clinical outcomes were shown in 48% cases and the favorable hemodynamic changes based on single-photon emission CT examinations were found in 65% of the patients. 13 In the present study, 7.5% patients experienced ischemic stroke events during follow-up period, but the association between the age of symptom onset and the clinical outcome could not been found.
Studies on the natural history of moyamoya disease indicated that it was a chronic and progressive cerebrovascular disease. 1,17 If not treated, 23.8% to 38.9% of moyamoya disease patients will experience inevitable disease progression, leading to symptoms aggravation and neurologic deficits. 18,19 Previous literatures suggested that encephaloduroarteriosynangiosis was effective in achieving early disappearance of the ischemic events. 17,20,21 Fung et al 22 performed a literature review of a large number of pediatric patients; they found that after operation, 51.2% of patients (592/1156) became completely symptom free, and 35.5% of patients (411/1156) achieved significant improvement. Indirect bypass (mainly encephaloduroarteriosynangiosis) and direct/combined bypass have similar effects in the rate of positive outcomes. 22 Matsushima et al 23 reported that 73.7% (42/57) patients with preoperative ischemic attacks became asymptomatic within 1 year after encephaloduroarteriosynangiosis surgery. As witnessed in our cohort, only 5 patients (7.5%) experienced ischemic stroke events during the follow-up period and the number of neurologic events was significantly decreased after encephaloduroarteriosynangiosis procedure, further suggesting its role in reducing the risk of further cerebrovascular ischemic events.
Perioperative complications after revascularization should be worthy of attention because they could affect the brain development of children. 24 The most common complications after encephaloduroarteriosynangiosis were the surgery-related ischemic events, including postoperative transient ischemic attack and cerebral infarctions of variable size. 10 The reasons may lie in the following. First, due to fear and anxiety after the surgery, pediatric patients are prone to cry and hyperventilate, which can lead to cerebral ischemia. Second, compared with adult counterparts, pediatric patients have lower body weight and they are more sensitivity to the changes of external temperature. These factors could promote the occurrence of ischemic complications. 14 Third, young children could not describe their symptoms accurately, which increased the chance of ischemic complications. 15 In a large pediatric cohort, ischemic complications occurred in 4.8% of the patients, and the majority of them recovered successfully during follow-up. 10 Kim et al 25 conducted a retrospective study of 410 pediatric patients treated by indirect bypass for moyamoya disease, they found the postoperative infarction was the most common complication, with a incidence of 13% per patient. We detected 2 patients (3.0%) who experienced a new infarction after surgical treatment; the incidence of complication in our series is lower than that of previous studies. Several feasible methods have been proposed to prevent the occurrence of these complications. During the perioperative period, maintaining adequate hemodynamic status, satisfactory pain relief to avoid hyperventilation, and reduced surgical duration and operative trauma are all helpful to decrease the incidence of complications. 10,16,25,26 Moreover, careful perioperative management, good anesthesia, and early recovery training are also beneficial for the treatment of moyamoya disease in pediatric patients. 14
There are several limitations to our study that should be noted. First, this study is a single-center retrospective study that lacks randomization between groups for ethical reasons. Second, encephaloduroarteriosynangiosis is performed if the donor or recipient vessel is too fragile for direct bypass. Therefore, potential bias in surgery selection is unavoidable. Third, recurrent stroke is determined according to the neuroradiologic examination; potential underestimation may occur because subclinical new ischemia is common in moyamoya disease. Fourth, as an invasive examination, follow-up digital subtraction angiography was not performed in most of the pediatric patients. Accordingly, we were unable to ascertain the hemodynamic changes after revascularization intervention. Last but not least, the patient number is relatively small; a further multicenter clinical trial with a larger sample size is warranted to provide better insights of encephaloduroarteriosynangiosis.
Conclusion
This study enhances our understanding of the clinical features, surgical results, and long-term outcomes of pediatric patients who underwent encephaloduroarteriosynangiosis for moyamoya disease. Encephaloduroarteriosynangiosis is an effective surgical modality for pediatric patients with moyamoya disease; this technique has a positive impact on the prevention of stroke recurrence.
Supplemental Material
Supplementary_file_1 - Encephaloduroarteriosynangiosis for Pediatric Moyamoya Disease: A Single-Center Experience With 67 Cases in China
Supplementary_file_1 for Encephaloduroarteriosynangiosis for Pediatric Moyamoya Disease: A Single-Center Experience With 67 Cases in China by Chengjun Wang, Meng Zhao, Jia Wang, Shuo Wang, Dong Zhang, Kai Wang, and Jizong Zhao in Journal of Child Neurology
Footnotes
Acknowledgments
We would like to thank Dr Meng Wang for her valuable advice in proofreading.
Author Contributions
CW conceptualized the study, reviewed the literature, and wrote the initial and final drafts. MZ and JW worked on conception and interpretation of data. All authors participated in critically revising the manuscript’s form and content. JZ critically revised manuscript and gave the final approval for final publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81371292) and the “13th Five-Year Plan” National Science and Technology supporting plan (2015BAI12B04).
Ethical Approval
This study was approved by the Research Ethics Board of Beijing Tiantan Hospital, Capital Medical University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.