
Abstract
The present study examined whether serum biomarkers can predict the prognosis of childhood epilepsy, including seizure frequency, electroencephalographic (EEG) changes, and cognitive impairment. We measured serum concentrations of high mobility group protein B1 (HMGB1), interleukin-1β (IL-1β), S100 calcium-binding protein B (S-100B), glial fibrillary acidic protein (GFAP), and α1-antichymotrypsin (AACT) in 180 children with new-onset epilepsy and 40 healthy children. Cognitive evaluations were performed 18 months after the initial seizure episodes at diagnosis (ie, baseline visit). The relationship between serum biomarkers and epilepsy prognosis was investigated using Pearson correlation coefficients, logistic regression analyses, and receiver operating characteristic curves. Sixty-seven patients had generalized tonic-clonic seizures, 92 had focal motor seizures, and 21 had epileptic spasms. Serum concentrations of HMGB1, IL-1β, S-100B, and GFAP were significantly higher in the epilepsy group within 24 hours of a seizure episode than in the control group. Furthermore, HMGB1 and IL-1β were significant predictors of epilepsy prognosis. Receiver operating characteristic curve analysis revealed that HMGB1 could more accurately predict seizure frequency than IL-1β; when the serum concentration of HMGB1 was >9.625 ng/mL, there was 80.6% sensitivity and 92.5% specificity for predicting seizure frequency reduction. In conclusion, HMGB1 and IL-1β have a predictive value for epilepsy prognosis in children.
Epilepsy is one of the most common neurologic disorders in children and has its highest incidence in the younger ages, with rates of 300 to 600 per 100 000, producing a tremendous societal burden. It is a chronic neurologic disorder characterized by sudden, abnormal neuronal discharges that lead to transient brain dysfunction. 1 Generally, prognosis refers to the probability of attaining seizure freedom on treatment. Prognostic factors include etiology, electroencephalographic (EEG) abnormalities, type of seizures and the number of seizures experienced before treatment onset, and poor early effects of drugs. In addition to debilitating seizures, epilepsy can cause intellectual disability with reduced quality of life. A key requirement for preventing epilepsy is to predict which individual will develop epilepsy prior to the onset of spontaneous seizures in early childhood. Therefore, there is an urgent need to develop both sensitive and specific biomarkers in the blood or cerebrospinal fluid that can predict the progression of epilepsy in children. A recent study reported that the inflammatory response is closely related to the initiation and progression of epilepsy. 2 Astrocytes are pivotal cells involved in both the induction and perpetuation of the inflammatory response to epileptogenic injuries or seizures. Accordingly, current research has focused on the role of inflammation-related interleukin-1 (IL-1) receptor/Toll-like receptor (IL-1R/TLR) superfamily of proteins in the pathogenesis of epilepsy. 3 This has revealed that TLRs are activated under pathological conditions by endogenous molecules that are released from damaged or activated cells. One such molecule, the high mobility group box 1 (HMGB1) protein, is secreted by various cells in the brain, including activated astrocytes, which produce HMGB1 in response to stimulation with lipopolysaccharide, tumor necrosis factor-α, and IL-1β. 4 Secreted HMGB1 then binds to TLR2, TLR4, and receptor for advanced glycation end products (RAGE) to activate intracellular nuclear factor κB (NF-κB) and other signaling pathways. This promotes the expression of pro-inflammatory cytokines. Considering its immune and inflammatory functions, the role that the HMGB1/TLR4 signaling might play in various neurologic diseases has attracted increased attention. 5
Previous studies in animal models of epilepsy demonstrated that the activation of the HMGB1/TLR4 signaling pathway significantly increases the seizure frequency. 6 –9 Specifically, HMGB1/TLR4 signaling promotes neuronal excitability by facilitating the release of endogenous ligands, including HMGB1, S100 calcium-binding protein B (S-100B), and pro-inflammatory cytokines, such as IL-1β. 10 S-100B, a marker of activated or damaged astrocytes, is primarily found in the central nervous system. 11 Activated hyperplastic astrocytes overexpress glial fibrillary acidic protein (GFAP), which is necessary for reactive astrogliosis. 12 Furthermore, α1-antichymotrypsin (AACT) is an acute-phase protein secreted by glial cells in response to infection, trauma, ischemia, or exogenous toxins; therefore, it may be upregulated following seizure. 13
The etiology of epilepsy is associated with increased expression of pro-inflammatory mediators prior to the onset of chronic spontaneous seizures. This suggests that these mediators participate in the onset and/or maintenance of epilepsy. Walker et al 14 showed that circulating isoforms of HMGB1 may serve as mechanistic biomarkers of epileptogenesis in animal models and drug-resistant epilepsy in humans. Although Diamond et al 15 indicated that IL-1β is associated with post-traumatic epilepsy development, it remains unknown whether these inflammatory mediators can be detected and quantified in the peripheral circulation as specific prognostic biomarkers of epilepsy in children. Therefore, this study aimed to examine the hypothesis that changes in serum concentrations of HMGB1, IL-1β, S-100B, GFAP, and AACT can predict the prognosis of childhood epilepsy, including seizure frequency, epileptiform discharges, and cognitive function. To achieve this, we prospectively analyzed 180 pediatric patients with new-onset epilepsy who were followed up for 18 months.
Materials and Methods
Participants
We recruited 192 patients between 1 month and 13 years of age from the Department of Neurology at Nanjing Children’s Hospital between January 2012 and December 2013. All patients had a diagnosis of new-onset epilepsy and met the diagnostic and classification criteria of the International League Against Epilepsy. 16 All patients’ routine blood (platelet counts and bleeding and clotting times) and liver function tests were normal.
Exclusion criteria were systemic diseases that can lead to epileptic seizures, such as hypoglycemia; malignant diseases; progressive or degenerative diseases; severe liver and kidney diseases; poor compliance to antiepileptic drug treatment; irregular lifestyle and obvious epilepsy-inducing factors, such as sleep deprivation and fever; and seizure types other than those specified above, concurrent illness at the time of presentation since that could also elevate the serum markers (serum HMGB1, IL-1β, S-100B, GFAP, AACT) such as encephalitis, pneumonia, skin infections, and urinary tract infection.
In addition, we recruited 40 age-matched healthy children from the Physical Examination Centre of Nanjing Children’s Hospital to serve as the control group. No subjects in the control group reported a history of febrile convulsions or other neurologic or psychiatric disorders. Furthermore, their electroencephalography (EEG) and cranial magnetic resonance imaging (MRI) results were normal.
The seizure types studied met the International League Against Epilepsy (2011) classification of epileptic seizure. 17 According to the new classification scheme, patients were classified as primary or secondarily generalized tonic-clonic seizures (GTCS), focal motor seizures, or epileptic spasms.
Demographic and Clinical Features of the Patients
We recorded the following information for each patient: sex; age at enrolment (months) and time of the first episode (months); predominant seizure type; cranial MRI findings (the types of brain MRI abnormalities) and the apparent diffusion coefficient value of lesion areas; video EEG findings before and after treatment (normal or abnormal; abnormal EEGs included abnormal nonepileptic and epileptic spikes/waves); febrile convulsion history; family history of febrile convulsion, including direct relatives (parents, siblings); family history of epilepsy, including direct relatives; and perinatal high-risk factors, including factors that influence the scoring of newborns, such as significant preterm birth, history of dystocia, history of asphyxia, advanced maternal age, low birth weight (<2500 g), maternal history of miscarriage, intrauterine distress, infections during pregnancy, eclampsia, and placental abruption.
MRI Data Acquisition
Diffusion-weighted imaging data were analyzed for all participants who underwent routine seizure protocol MRI. The examination included anatomical T2-weighted axial imaging, fluid-attenuated inversion recovery axial imaging, oblique T2-weighted coronal imaging, 3-dimensional gradient echo T1-weighted coronal imaging, and diffusion tensor imaging sequences. MRI was performed on a 1.5-Tesla scanner (Skyra; Siemens, Erlangen, Germany) with a 20-channel Sensitivity Encoding (SENSE) head coil. Diffusion tensor imaging was performed using single-shot spin echo-echo planar imaging with SENSE factor 2. The imaging parameters were as follows: 2-mm iso-voxel data acquisition with 5-mm slice thickness; field of view, 128 mm; echo time, as low as 20 milliseconds (ms); repetition time, 10 000 ms (according to slice number); number of signal acquisitions, 2; b-value, 1000 s/mm2; and diffusion gradient directions, 32. Data were processed on a computer equipped with an MRI scanner-operating console. A semiquantitative analysis was performed for regions of interest drawn over lesion sites or the left temporal lobe (at the level of the temporal horn of the lateral ventricle) in the absence of an obvious lesion on MR images.
Evaluation of Neurologic Function
A detailed clinical history, baseline neurologic examination, and routine blood biochemistry tests (such as liver and renal function, electrolytes, and myocardial enzymes) were performed for each subject. Additionally, the Chinese revised versions of the Wechsler Intelligence Scale for Children (for children ≥36 months of age) and the Bayley Scales of Infant Development (for children ≤36 months of age) were used to assess the development of intelligence at baseline and 18 months later.
Video EEG Acquisition
Each patient underwent 4 hours of video EEG monitoring (including flash stimulation and hyperventilation) to confirm a diagnosis of epilepsy. Three additional sessions were completed for regular monitoring at baseline and at 6, 12, and 18 months. The video EEG results were interpreted by EEG specialists and a pediatric neurologist.
Blood Collection and Analysis
Peripheral venous blood (∼2 mL) was collected within 24 hours after seizure onset at diagnosis (ie, baseline visit). In healthy control subjects, 2 mL of venous blood was collected between 06:00 and 08:00 after fasting. Serum was obtained after centrifugation for 10 minutes at 3000 rpm and stored at −80°C until use. Children were re-examined at the 18-month follow-up, and 2 mL of peripheral venous blood was collected >1 week after the most recent seizure attack and processed as described above. Serum concentrations of HMGB1, IL-1β, S-100B, GFAP, and AACT were measured using commercially available enzyme-linked immunosorbent assay kits, as follows: HMGB1 (Cusabio, catalog number: CSB-E08223 h; Shanghai, China), S-100B (Cusabio, catalog number: CSB-E08065 h), GFAP (Cusabio, catalog number: CSB-E08601 h), AACT (Cusabio, catalog number: CSB-E08957 h), and IL-1β (4A Biotech, catalog number: CHE001; Beijing, China). Assays were performed per manufacturer instructions. All blood samples were analyzed in the same laboratory.
Follow-up
All children received antiepileptic drug therapy. Follow-up registration forms were created for all children. Patients were followed up at 6 and 18 months after baseline; the complete follow-up period was 18 months. We prospectively collected information about epileptic seizures, video EEG results, other significant events, type and dose of antiepilepsy drugs, attack control, and mental development (which was based on parental observation, schoolteacher evaluations, academic performance, and intelligence quotient testing) during in-clinic visits and via telephone interviews.
Prognosis Determination
Changes in the Frequency of the Predominant Seizure Frequency
The frequency of the predominant seizure was evaluated at baseline, 6 months, and 18 months. Changes (reduction) in seizure frequency were calculated using the formula (A−B) / B, where A is the frequency of seizures every 28 days while on a maintenance dose of medication and B is the baseline frequency of seizures (monthly frequency during the 12 weeks before the study). Treatments resulting in decreases in seizure frequency of ≤50%, 50% to 75%, 75% to 99%, and 100% were considered ineffective, effective, very effective, and full seizure control, respectively.
Changes in the Number of Interictal Epileptiform Discharges
Changes in the time course of interictal epileptiform discharge compared with that at baseline were evaluated. Treatments resulting in decreases in the time course of interictal epileptiform discharges of 76% to 100%, 51% to 75%, 25% to 50%, and <25% (or increased epileptiform discharges) were considered very effective, effective, improved, and ineffective or deterioration, respectively.
Intelligence
Changes in the development of intelligence were calculated as numerical changes in Wechsler Intelligence Scale for Children (children >36 months of age) or Bayley Scales of Infant Development scores.
Statistical Analyses
All statistical analyses were performed using SPSS, version 17.0 (SPSS Inc, Chicago, IL). Numerical variables are presented as the mean ± standard error of the mean. We used parametric and nonparametric tests in accordance with the homogeneity of variance. One-way analyses of variance were used to identify differences among the groups and Student-Newman-Keuls tests were used for multiple comparisons when data had equal variance. Rank-sum tests were used for numerical data with unequal variance. Frequency data are presented as the frequency (composition ratio) and analyzed using χ2 tests. Logistic regression analyses were used to evaluate the predictive values of different variables. Receiver operating characteristic curves were used to evaluate the predictive ability of serological markers for the prognoses of children with epilepsy. The threshold for statistical significance was set at P < .05.
Results
Clinical and Biochemical Data
The final analysis included 180 of 192 patients with epilepsy initially enrolled in the study; 1 patient died and 11 were excluded because of dropout or lack of follow-up. The patients were divided into 3 groups by epileptic seizure type: generalized tonic-clonic seizures (n = 67), focal motor seizures (n = 92), and epileptic spasms (n = 21). A comparison of the clinical and biochemical data between children with epilepsy and healthy control subjects is shown in Table 1.
Comparison of Clinical Data Between Children With Epilepsy and Healthy Control Subjects.a
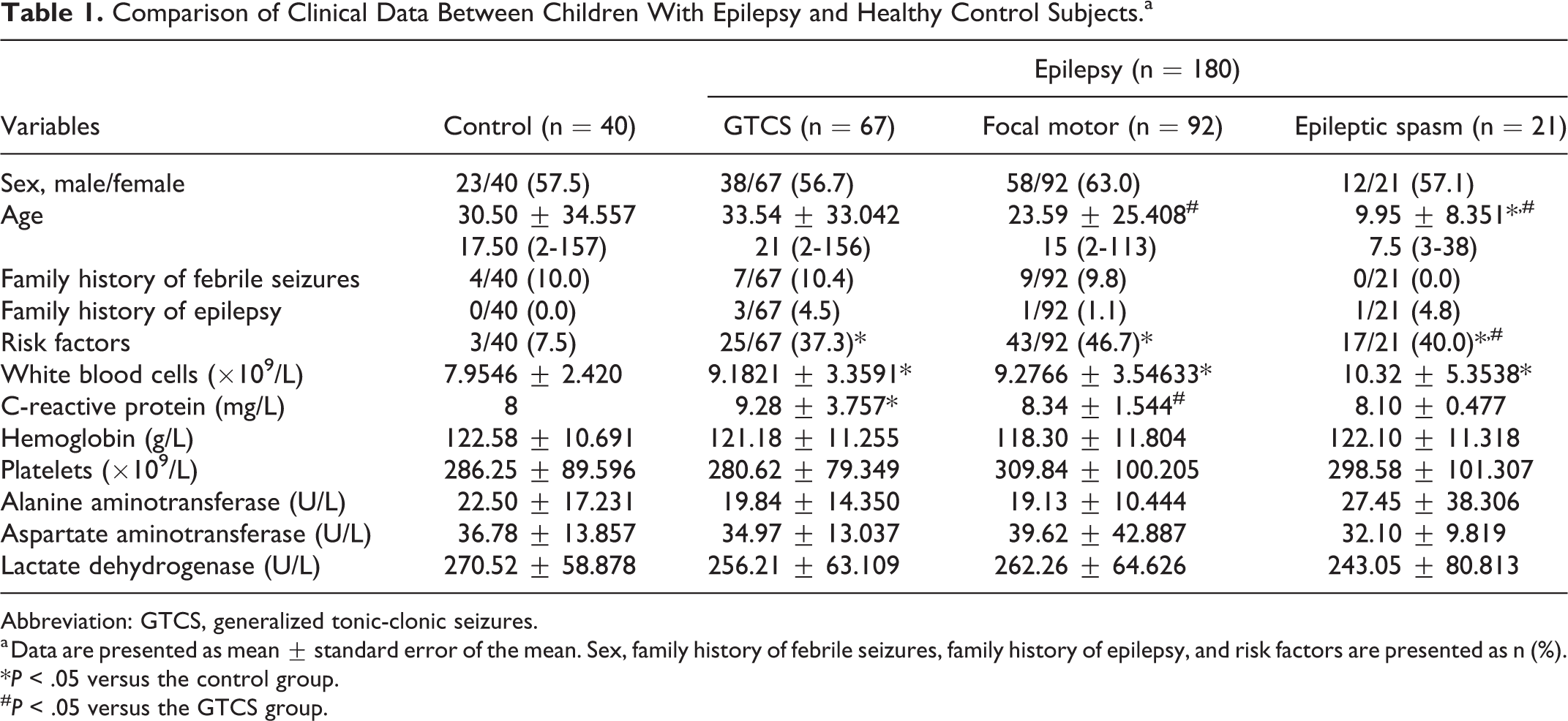
Abbreviation: GTCS, generalized tonic-clonic seizures.
a Data are presented as mean ± standard error of the mean. Sex, family history of febrile seizures, family history of epilepsy, and risk factors are presented as n (%).
*P < .05 versus the control group.
#P < .05 versus the GTCS group.
Cranial MRI and Video EEG Data Before Treatment
All 180 patients underwent cranial MRI examination. Patients with epilepsy had more intracranial lesions than control subjects. In addition, patients in the epileptic spasm group had higher rates of abnormal MRI findings (71.4%) than the generalized tonic-clonic seizures and focal motor groups (44.8% and 47.8%, respectively; P < .05). The same trend was noted with the diffusion-weighted imaging apparent diffusion coefficient values (P < .05), which were higher in the epileptic spasm group (1074.33 ± 115.90) than the generalized tonic-clonic seizures (999.87 ± 95.92) and focal motor groups (1017.92 ± 112.87; P < .05). Moreover, apparent diffusion coefficient values were higher in the epilepsy groups than those in the healthy control group (P < .05). Patients with epilepsy also had higher rates of abnormal video EEG findings than the control subjects (0%) at baseline; video EEG results were abnormal in all patients in the epileptic spasm group, 61.2% of patients in the generalized tonic-clonic seizures group, and 67.4% of patients in the focal motor group (Table 2). In the case of generalized tonic-clonic seizures, 30/67 (44.8%) cases had abnormal findings according to MRI, in the case of focal motor 44 (47.8%), whereas cases had abnormal findings. In the patients with epileptic spasm, the number of abnormalities detected through MRI findings were 15/21 (71.4%). Findings were categorized as focal and nonfocal lesions. Focal lesions were detected in 30 (13.64%) and nonfocal lesions demonstrated in 74 (41.1%) of the patients. Abnormal findings are summarized in Table 3. The most commonly demonstrated pathology was generalized atrophy, at 20% (n = 36). Cerebellar atrophy was reported in 2.8% (n = 5) of patients. The second most common abnormality was hypomyelination encountering in 5% (n = 9). Focal lesions (encephalomalacia, ischemic lesion, gliosis, hemorrhage) were found in 9 of the patients, constituting 5% of the study population. Three (1.7%) of the patients had encephalomalacia. Corpus callosum abnormalities were detected in 2.2% (n = 4) of the patients. Periventricular leukomalacia were recorded in 4 (2.2%) patients. Tuberous sclerosis was demonstrated in 3 patients, accounting for 1.7% of the population. Mega cisterna magna was noted in 3 patients (1.7%). Cysts were found in 2 (1.1%) patients, among whom one had choroidal cysts and the other arachnoid cysts. Heterotropy was detected in 5 (2.27%) of the patients. Hydrocephaly, heterotrophy (pachygyria, polymicrogyria), and increased signal intensity were each detected in 2 patients of group 3, at 1.1% each.
Comparison of MRI and Pretreatment Video EEG Findings Between Children With Epilepsy and Controls.a
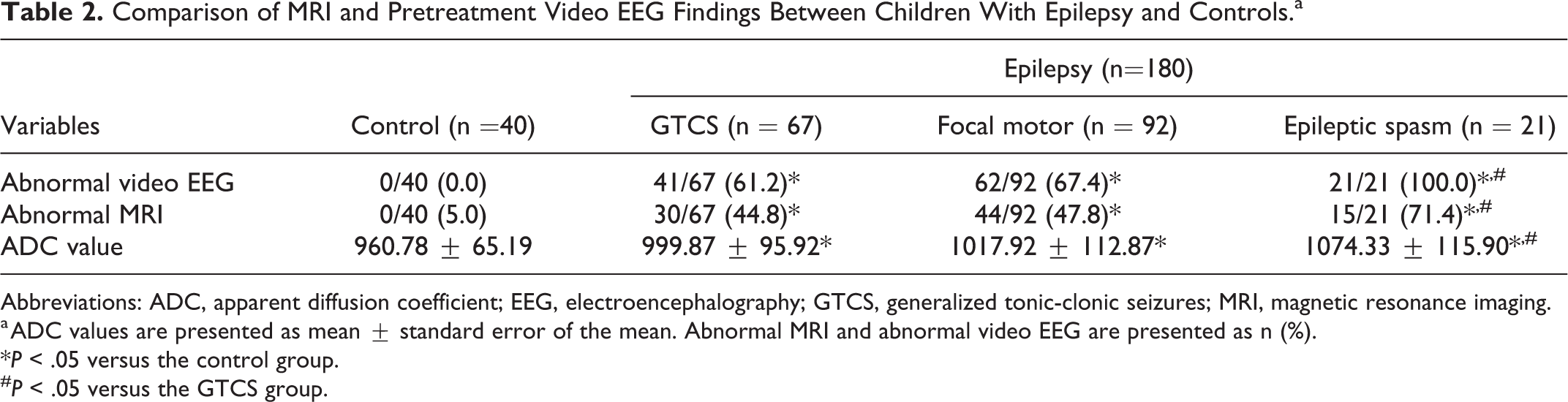
Abbreviations: ADC, apparent diffusion coefficient; EEG, electroencephalography; GTCS, generalized tonic-clonic seizures; MRI, magnetic resonance imaging.
a ADC values are presented as mean ± standard error of the mean. Abnormal MRI and abnormal video EEG are presented as n (%).
*P < .05 versus the control group.
#P < .05 versus the GTCS group.
Types and Breakdown of Brain MRI Abnormalities Within the Groups.a
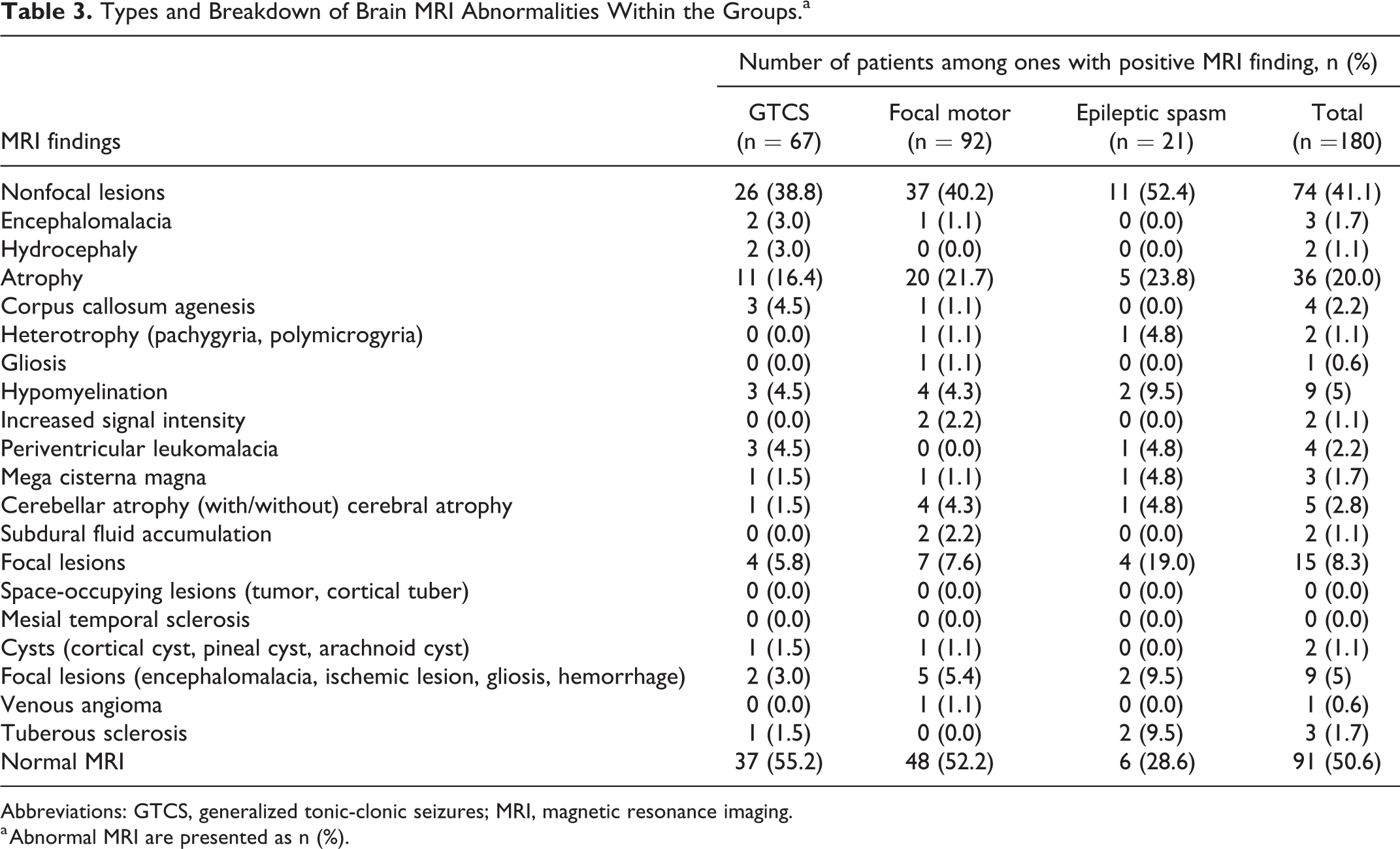
Abbreviations: GTCS, generalized tonic-clonic seizures; MRI, magnetic resonance imaging.
a Abnormal MRI are presented as n (%).
Concentration of Serum HMGB1, IL-1β, S-100B, GFAP, and AACT in the Acute Stage and Between Epileptic Episodes
Serum concentrations of HMGB1, IL-1β, S-100B, and GFAP were higher in patients with all types of epilepsy within 24 hours after seizure onset at baseline than in controls (P < .05 for all comparisons). Serum concentrations of these factors were significantly higher in the epileptic spasm group than the other epilepsy groups. Furthermore, serum concentrations of these factors were significantly lower >1 week following the most recent seizure attack after the 18-month treatment and follow-up than 24 hours after seizure onset at baseline, but remained higher than those in the control group (P < .05; Figure 1).
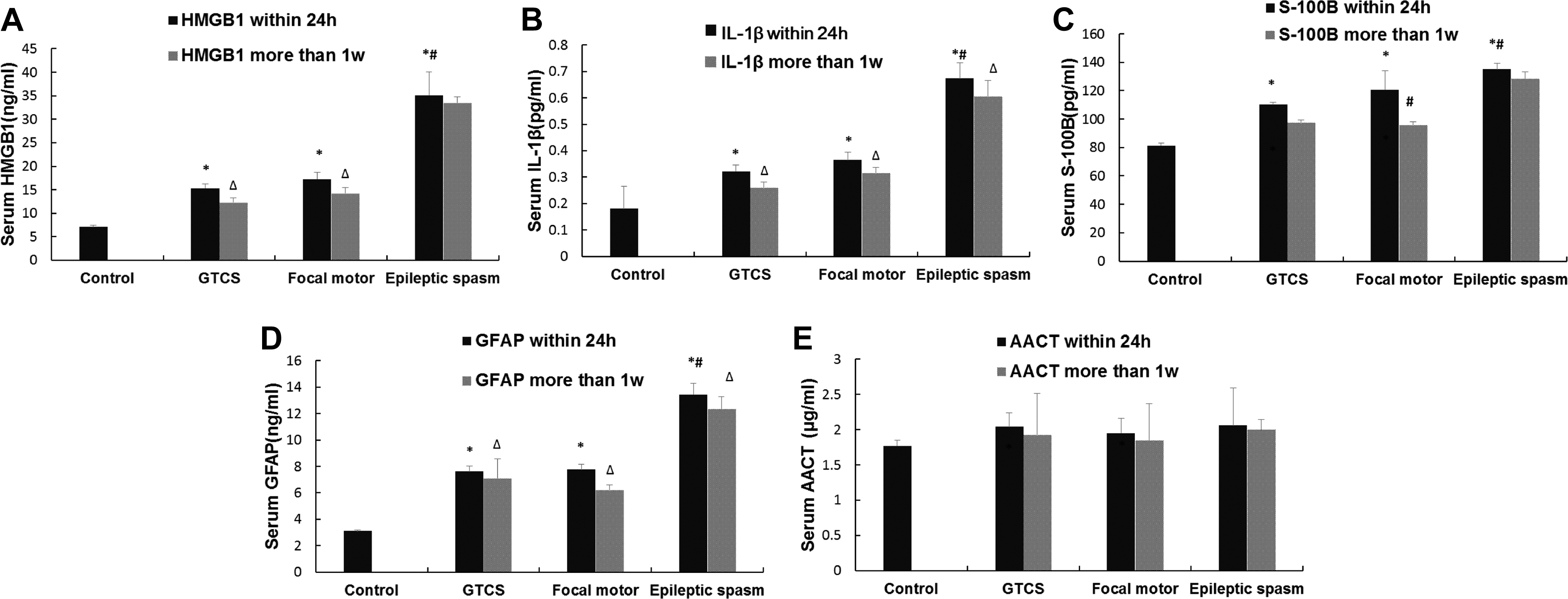
The serum HMGB-1, IL-1β, S-100B, GFAP, and AACT concentrations within 24 hours after seizure onset and more than 1 week after the most recent seizure attack after treatment (at 18 months) of subjects. Histograms are used for expressing the serum high mobility group protein B1 within 24 hours after seizure onset and more than 1 week after the most recent seizure attack after treatment (18 months) (HMGB-1) (A), interleukin-1β (IL-1β) within 24 hours after seizure onset and more than 1 week after the most recent seizure attack after treatment (18 months) (B), and S100 calcium-binding protein B within 24 hours after seizure onset and more than 1 week after the most recent seizure attack after treatment (18 months) (S-100B) (C), glial fibrillary acidic protein within 24 hours after seizure onset and more than 1 week after the most recent seizure attack after treatment (18 months) (GFAP) (D), α1-antichymotrypsin (AACT) within 24 hours after seizure onset and more than 1 week after the most recent seizure attack after treatment (18 months) (E) concentrations of the subjects. *P < .05 compared with the control group; #P < .05 versus the GTCS group; ▵P < .05 versus the serum concentrations within 24 hours after seizure onset. (GFAP, glial fibrillary acidic protein; GTCS, generalized tonic-clonic seizures.)
Factors Influencing the Prognosis of Newly Diagnosed Epilepsy in Children
Logistic regression analyses were used to test the predictive value of patients’ age, apparent diffusion coefficient value, and serological markers for epilepsy prognosis (ie, seizure frequency, interictal epileptiform discharge, and intelligence). Abnormal video EEG findings (odds ratio [OR] = 0.290, 95% confidence interval [CI] = 0.096-0.875), serum HMGB1 (OR = 0.983, 95% CI = 0.977-0.989), and serum IL-1β (OR = 0.904, 95% CI = 0.876-0.933) were associated with a poor prognosis for seizure frequency (P < .05; Table 4). A multivariate analysis indicated that these variables were independent risk factors for increased seizure frequency (P < .05). In addition, serum HMGB1 (OR = 0.989, 95% CI = 0.985-0.993) and IL-1β (OR = 0.951, 95% CI = 0.935-0.967) were associated with a poor prognosis in terms of the number of epileptiform discharges (Table 5). A multivariate analysis indicated that these variables were independent risk factors for increased epileptiform discharges (P < .05). Finally, serum HMGB1 (OR = 1.003, 95% CI = 1.001-1.0060), serum IL-1β (OR = 1.026, 95% CI = 1.012-1.040), and serum S-100B (OR = 1.067, 95% CI = 1.044-1.090) were associated with a poor prognosis for intellectual development (Table 6). A multivariate analysis showed that these variables were independent risk factors for intellectual disability (P < .05).
The Effect of Age, Risk Factors, and the Serum Concentrations of Biomarkers on Seizure Prediction in Children With Epilepsy by Logistic Regression Analysis.
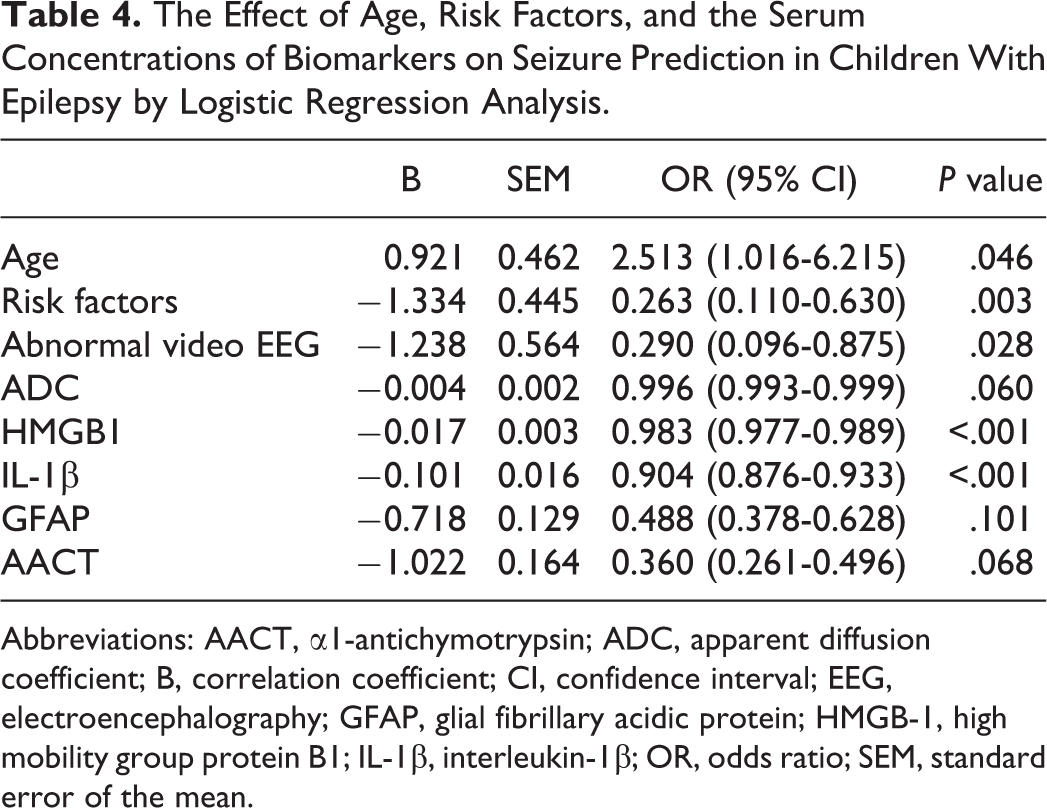
Abbreviations: AACT, α1-antichymotrypsin; ADC, apparent diffusion coefficient; B, correlation coefficient; CI, confidence interval; EEG, electroencephalography; GFAP, glial fibrillary acidic protein; HMGB-1, high mobility group protein B1; IL-1β, interleukin-1β; OR, odds ratio; SEM, standard error of the mean.
The Effect of Risk Factors and the Serum Concentrations of Biomarkers on Epileptiform Discharge Prediction in Children With Epilepsy by Logistic Regression Analysis.
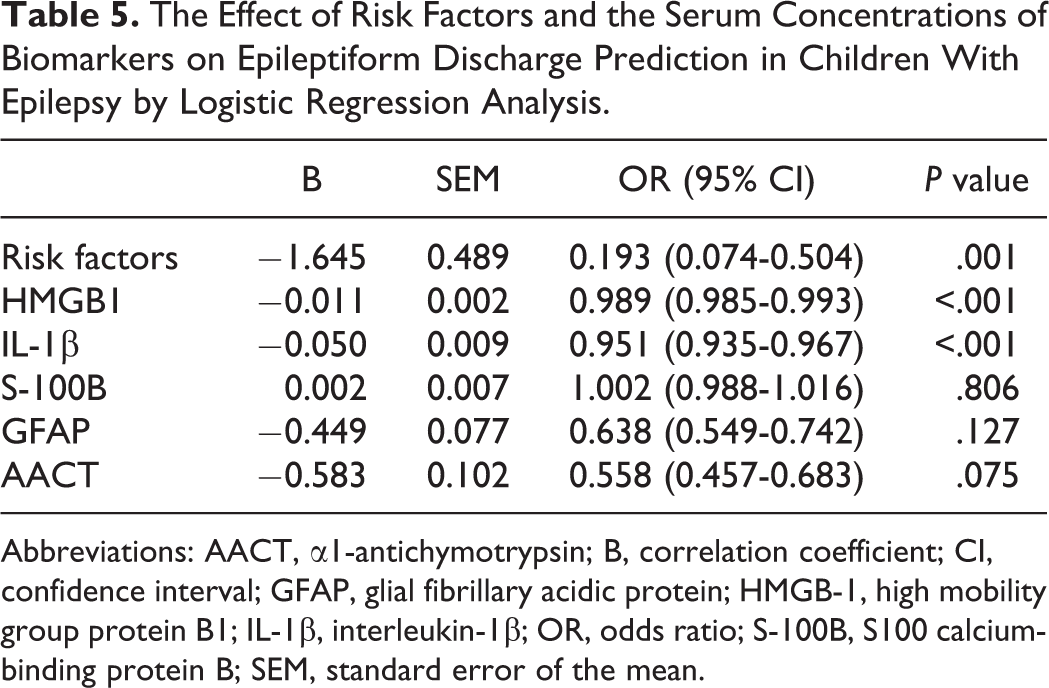
Abbreviations: AACT, α1-antichymotrypsin; B, correlation coefficient; CI, confidence interval; GFAP, glial fibrillary acidic protein; HMGB-1, high mobility group protein B1; IL-1β, interleukin-1β; OR, odds ratio; S-100B, S100 calcium-binding protein B; SEM, standard error of the mean.
The Effect of Age, Risk Factors, Abnormal Video EEG, Abnormal MRI, and the Serum Concentrations of Biomarkers on Poor Mental Development Prediction in Children With Epilepsy by Logistic Regression Analysis.
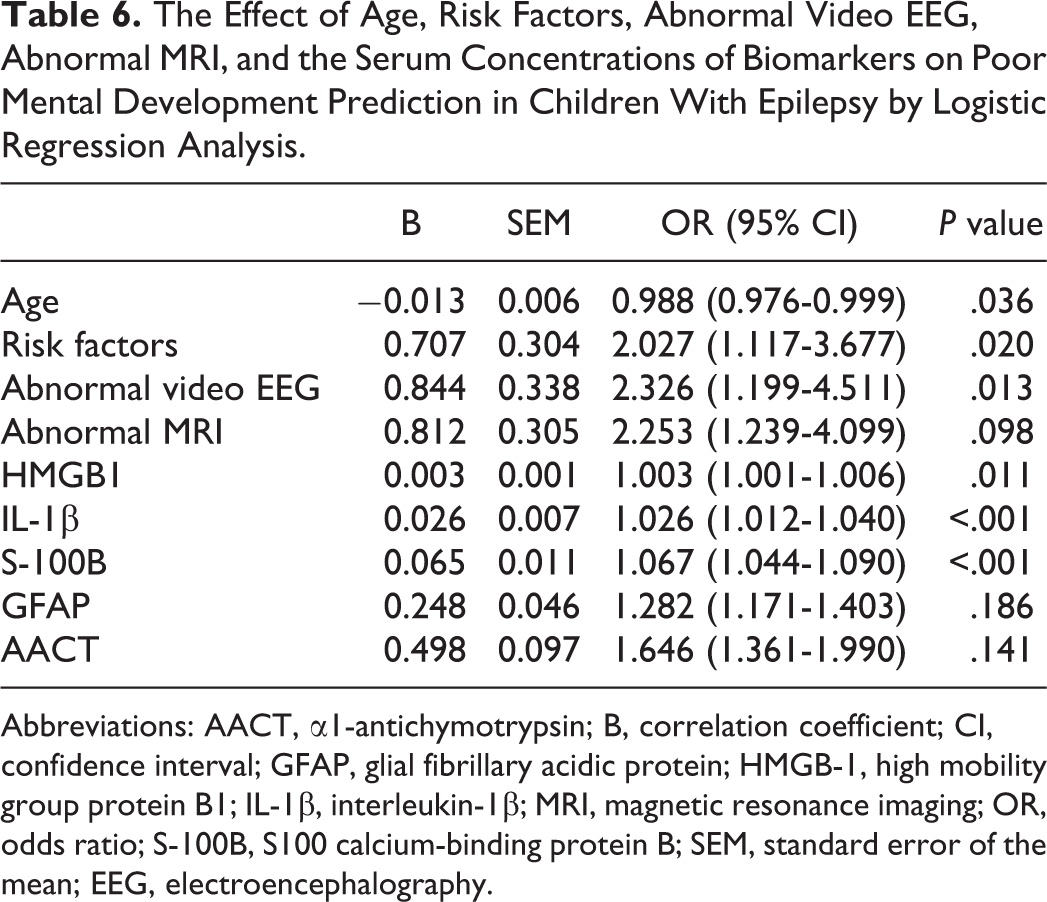
Abbreviations: AACT, α1-antichymotrypsin; B, correlation coefficient; CI, confidence interval; GFAP, glial fibrillary acidic protein; HMGB-1, high mobility group protein B1; IL-1β, interleukin-1β; MRI, magnetic resonance imaging; OR, odds ratio; S-100B, S100 calcium-binding protein B; SEM, standard error of the mean; EEG, electroencephalography.
Receiver Operating Characteristic Curve Analysis
We generated receiver operating characteristic curves to determine the ability of the serum HMGB1 and IL-1β concentrations to predict seizure frequency. The results indicated that a threshold serum HMGB1 concentration of 96.25 ng/dL had an area under the curve of 0.947, sensitivity of 80.6%, and specificity of 92.5% for predicting seizure frequency. A threshold serum IL-1β value of 20.60 ng/dL had an area under the curve of 0.834, sensitivity of 77.8%, and specificity of 62.5% for predicting seizure frequency. The area under the curve of HMGB1 was significantly larger than that of IL-1β (P < .05). These findings suggested that the serum HMGB1 concentration was a better predictor of seizure frequency than the serum IL-1β concentration (Figure 2).
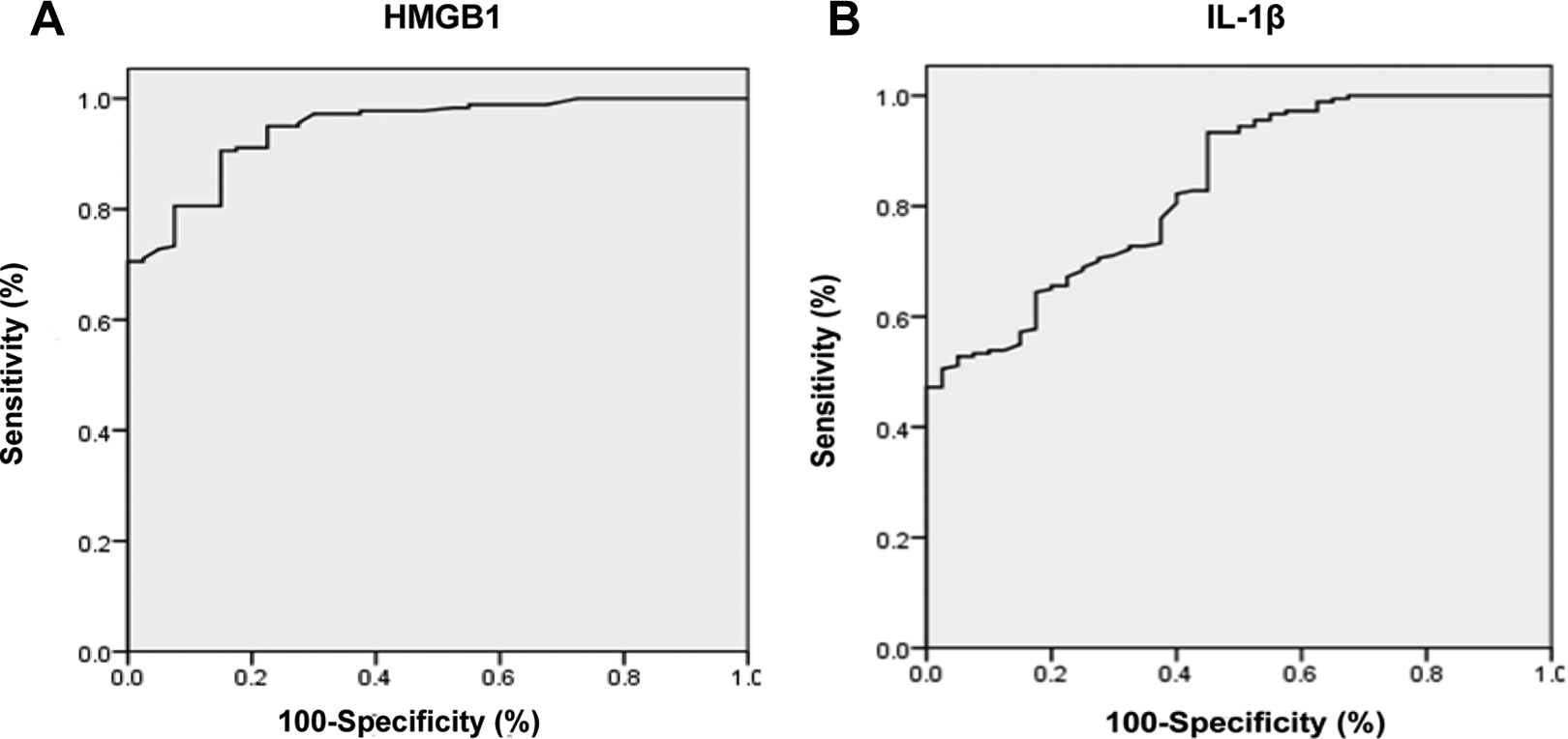
Receiver operating characteristic curves demonstrating the ability of serum high mobility group protein B1 (HMGB1) and interleukin-1β (IL-1β) to predict seizure frequency
Discussion
To our knowledge, the present study is the first to demonstrate the utility of serological markers, including HMGB1, IL-1β, S-100B, and glial fibrillary acidic protein, to predict the prognosis of epilepsy in children. Notably, no significant difference in serum concentrations of AACT was identified between children with epilepsy and healthy control subjects, suggesting that this acute-phase protein is not involved in epilepsy progression. Conversely, serum concentrations HMGB1 and IL-1β were significantly higher in patients with epilepsy than healthy control subjects within 24 hours of seizure onset and subsequently decreased between seizure episodes. Further statistical analyses demonstrated that serum concentrations of HMGB1 and IL-1β were negatively associated with patients’ intelligence scores and positively associated with frequency of seizures and the number of epileptiform discharges. Logistic regression analyses confirmed 3 independent risk factors for increased seizure frequency: serum HMGB1 and IL-1β, and abnormal EEG. The latter finding is consistent with a previous study demonstrating that abnormal EEG, especially in the presence of epileptiform waves, is a relapse risk factor in patients with epilepsy. 18 Serum concentrations of HMGB1 and IL-1β were also identified as independent risk factors for epileptiform discharges. These findings suggest that serum HMGB1 and IL-1β are potentially involved in the initiation and progression of epilepsy or epileptic lesions and are potential predictive factors for epilepsy prognosis.
Neuropsychological examinations performed on patients at 18 months after the initial seizure episode at diagnosis (ie, baseline visit) revealed different degrees of intellectual dysfunction. Serum concentrations of HMGB1 and IL-1β were negatively associated with the intelligence test score, including Wechsler Intelligence Scale for Children or Bayley Scales of Infant Development score. Logistic regression analysis confirmed that serum concentrations of HMGB1, IL-1β, and S-100B were independent risk factors for poor intellectual development. Previous research indicated that in drug-resistant and newly diagnosed patients, the presence of disulfide HMGB1 is not detected in the sera of healthy individuals or patients with well-controlled epilepsy. Persistent elevation of disulphide HMGB1 following epilepsy diagnosis was associated with likelihood of subsequent seizures, thus suggesting that it may be a useful prognostic and predictive biomarker of seizure relapse and response to therapy. 14 Whether the predictive value of blood HMGB1 levels is associated with any specific form of (eg, focal vs generalized) seizure type in the epilepsy children remains unclear. There is also a strong positive correlation between early traumatic brain injury–induced changes in IL-1β levels would be associated and post-traumatic epilepsy (PTE). 15 Similarly, Lu et al 19 observed higher serum S-100B in patients with temporal lobe epilepsy than in healthy control subjects. Accordingly, S-100B may represent a biomarker of temporal lobe epilepsy rather than the forms of epilepsy studied herein. Moreover, numerous studies have identified pathologic changes, including glial cell proliferation, neuronal damage, and demyelination, in association with epilepsy; the apoptosis and necrosis of hippocampal neurons has been documented in patients with epilepsy. 20 The activation of astrocytes is one of the most prominent cellular changes occurring in the brain after various epileptogenic injuries. Studies in experimental models of epilepsy showed that activated astrocytes produce and release an array of proinflammatory mediators during epileptogenesis that potentially contribute to spontaneous seizures generation, 21 cell loss, and comorbidity. 22 Because of the potential mechanistic role of neuroinflammation in epilepsy, monitoring this process using noninvasive approaches may generate potential biomarkers of ictogenesis and epileptogenesis. This study found that serum HMGB1, IL-1β, and S-100B were higher in patients with all types of epilepsy within 24 hours after seizure onset at baseline than in controls. Serum concentrations of these factors were significantly higher in the epileptic spasm group than the other epilepsy groups. Therefore, changes in serum concentrations of HMGB1, IL-1β, and S-100B may have clinical significance for the pathologic progression of epilepsy (especially for the epileptic spasm) and help predict intellectual outcomes. The early detection of intellectual impairments may facilitate the use of treatments to prevent further brain damage, reducing the number of sequelae in patients with epilepsy.
Dirik found that abnormality in MRI examination in newly diagnosed epileptic children was high and summarized the types of abnormal Brain MRI findings. These high rates may be due to enrollment of children with new emerging epilepsy on a chronic neurologic disorder. Secondary lesions were detected in cases with corpus callosum abnormality, atrophy, encephalomalacia and hydrocephaly. 23 We have the similar conclusions. However, it remains unknown whether the types of structural abnormalities in MRI findings is directly related to the prevalence and types of seizures in the children who has newly diagnosed as epilepsy, further studies are needed to confirm these findings.
We found that the apparent diffusion coefficient values were higher in the epilepsy groups than the healthy control group; however, no significant correlation was found between apparent diffusion coefficient values and seizure frequency. This result is consistent with a previous study. 24 However, recent studies have shown that multimodal functional magnetic resonance imaging is important for early epilepsy detection and prognosis. 25 Restriction of the axolemma and myelin sheath in white matter restrains water molecules along fibers, resulting in an inconsistent dispersion rate in 3-dimensional space on diffusion-weighted images. This inconsistency can be captured and displayed using diffusion tensor imaging.
The receiver operating characteristic analyses performed in this study revealed that although a threshold serum IL-1β value of 0.206 pg/mL significantly predicted the changes in the frequency of seizures after the first episode, a threshold serum HMGB1 value of 9.625 ng/mL had far better sensitivity (80.6%) and specificity (92.5%). Accordingly, HMGB1 was a more useful and accurate predictor of seizure frequency reduction in this study. Seizure-free rates are clinically important for measuring epilepsy outcomes; therefore, HMGB1 may be an important biomarker for epilepsy prognosis. Future studies should corroborate and explore this conclusion in a larger patient population with a longer follow-up period.
This study has several limitations. First, this was a single-center study; multicenter trials with larger cohorts are needed. Second, a longer follow-up period should be used to assess the predictive ability of these biomarkers with long-term prognosis. In conclusion, our findings suggest that HMGB1 and IL-1β are potential biomarkers for epileptogenesis in the children. Furthermore, they can predict prognostic effects, including seizure frequency, epileptiform discharges, and intellectual function. Further studies are necessary to be conclusive.
Footnotes
Acknowledgments
We thank Brad Peterson for revising the article.
Author Contributions
YX designed the study, interpreted the data, and revised the manuscript. MZ, JC, and HG did the experiments. MZ, JC, LD, and YZ did the experiments and analyzed the data. MZ wrote the paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (81401864, Zhu) and the Science and Technology Development Fund Project of Nanjing Medical University of China (2013NJMU097, Zhu).
Ethical Approval
This clinical study was approved by the Ethics Committee of Nanjing Children’s Hospital. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.