
Abstract
This cross-sectional study assessed health-related quality of life (HRQOL) in ambulant and nonambulant patients with Duchenne muscular dystrophy, and explored the association between health-related quality of life and clinically assessed motor function. The Pediatric Quality of Life Inventory (PedsQL) Generic Core Scale and PedsQL Neuromuscular module were completed by 34 parent-child dyads. Association between PedsQL scores and overall motor abilities and the transfers and standing posture domain measured by the Motor Function Measure were examined. Child self-reported and parent proxy-reported mean PedsQL scores for children with Duchenne muscular dystrophy were lower than those for healthy children for the physical and psychosocial health-related quality of life. Fifty-six percent of patients reported clinically impaired psychosocial health-related quality of life scores. Several aspects of the generic and disease-specific health-related quality of life in patients with Duchenne muscular dystrophy were positively associated to overall motor function and transfers and standing posture domain. Associations remained stable when adjusted for age and corticosteroid use. The Motor Function Measure is clinically meaningful in the context of a patient’s day-to-day life.
Keywords
Duchenne muscular dystrophy is a genetic X-linked recessive disease with the second highest incidence considering all the hereditary diseases. 1 Duchenne muscular dystrophy affects 1 in 3600 to 6000 live male births. 2 Mutations in the dystrophin gene lead to the absence of the protein dystrophin, which leads to progressive muscle degeneration causing muscle weakness and resulting in loss of independent ambulation by the age of 13 years. 3
Besides functional impairment, the impact of the disease on additional biopsychosocial aspects such as quality of life should not be underestimated. Regulatory authorities, researchers, and clinicians start to recognize the importance of health-related quality of life measures in natural history and clinical trials. The impact of possible functional changes on daily living activities and, more generally, on patients’ quality of life is increasingly explored. 4,5 Health-related quality of life is a multidimensional construct, consisting at a minimum of physical, psychological (including emotional and cognitive), and social health domains defined by the World Health Organization. 6,7 The health-related quality of life is thought to be the best representation of patient perceptions concerning the impact of an illness and its treatment on their own functioning and well-being. 6,7 A variety of age-appropriate instruments are given allowing the assessment of child and adolescent health-related quality of life by means of self- and parent-reports. 8 Wei et al 9 pointed out in their review that the Pediatric Quality of Life Inventory (PedsQL) appears to be the most comprehensive and validated measure for clinical use and research in Duchenne muscular dystrophy patients. The PedsQL Generic Core Scale is the most widely used tool to assess generic quality of life in clinical studies. A specific module for neuromuscular disorders, the PedsQL Neuromuscular Module, has been validated in Duchenne muscular dystrophy and spinal muscular atrophy. 10,11 Several studies have reported the use of these instruments in Duchenne muscular dystrophy cohorts. 10,12 –16
The reports on the health-related quality of life in Duchenne muscular dystrophy patients in previous studies are still controversial. Some researchers reported reduced health-related quality of life among Duchenne muscular dystrophy patients compared to healthy children both for parent-proxy report and child self-report 12 –17 ; others have found no differences in the health-related quality of life between Duchenne muscular dystrophy patients and healthy controls except the physical domain. 18 –21
Although many functional and strength-based performance tests quantify aspects of a clinically meaningful function (eg, motor abilities), they do not directly assess the patient’s health-related quality of life or participation in daily activities. Determining the impact of a disease on health-related quality of life and understanding the association of health-related quality of life to motor function can provide useful information for medical care, education, and welfare decision making. However, until now the relationship between motor function and health-related quality of life in Duchenne muscular dystrophy patients is unclear. Additionally, research so far is often limited to only ambulant Duchenne muscular dystrophy patients. 14,18,22 A summary of previous literature investigating the association between health-related quality of life and functional outcomes is presented in Table 1.
Summary of Studies Investigating HRQOL and Functional Outcomes in DMD.
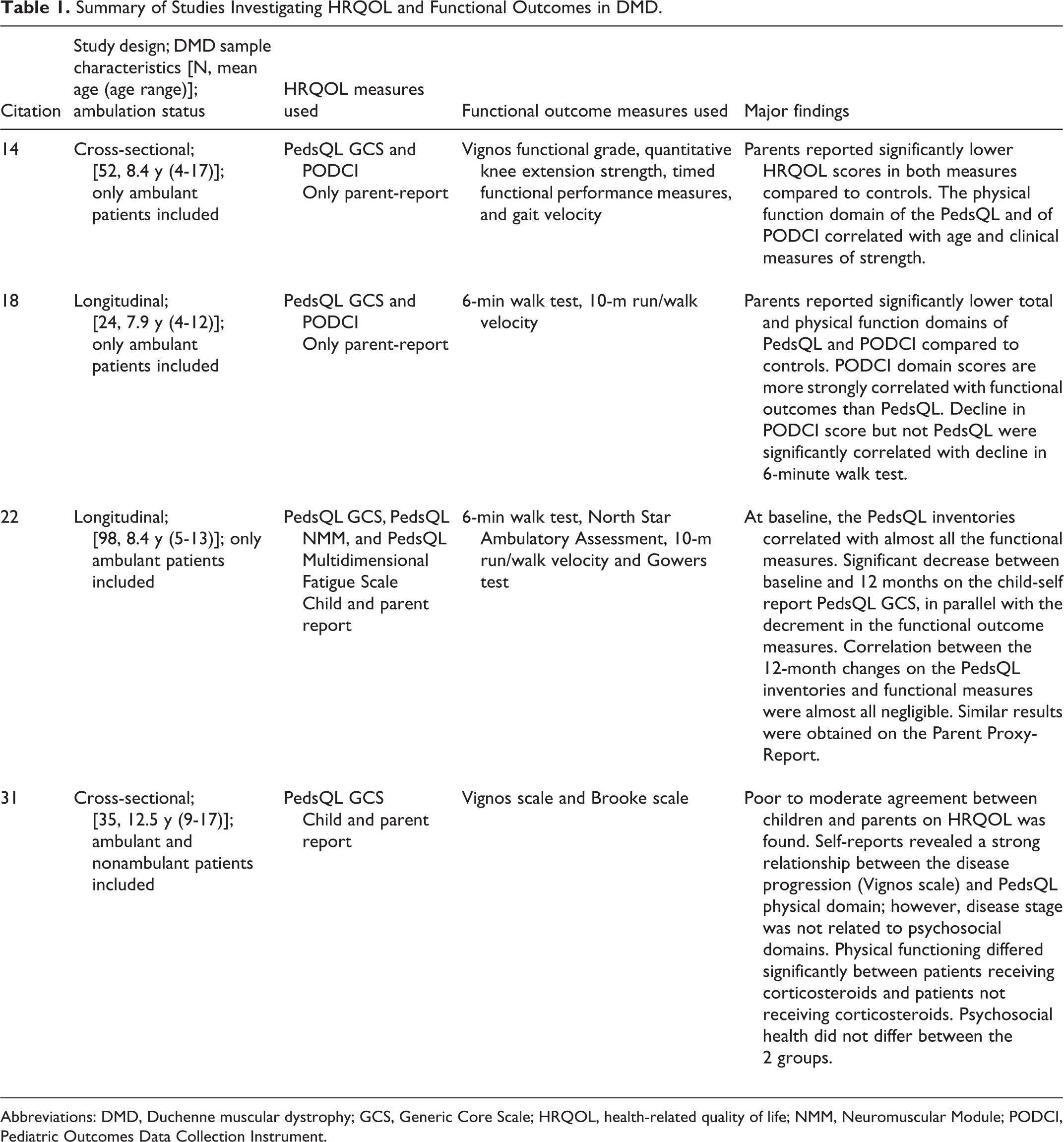
Abbreviations: DMD, Duchenne muscular dystrophy; GCS, Generic Core Scale; HRQOL, health-related quality of life; NMM, Neuromuscular Module; PODCI, Pediatric Outcomes Data Collection Instrument.
The aims of the study are to assess general and disease-specific health-related quality of life in ambulant and nonambulant Duchenne muscular dystrophy patients, to compare general health-related quality of life data with normative data of healthy children, and to assess parent-child agreement. Further, we explore the association between health-related quality of life and clinical assessment of motor function in patients with Duchenne muscular dystrophy.
Methods
Participants
We performed an observational cross-sectional study of Duchenne muscular dystrophy patients who have participated in the past in 2 investigator-initiated clinical trials 23,24 at the Division of Neuropediatrics, University Children’s Hospital Basel. Former participants from both studies were invited to participate for the observational single visit 2.5 up to 5 years after completion of the clinical trial. Of the 48 former participants invited to participate, 34 (71%) subjects, 33 boys and 1 girl, with molecular diagnosis of Duchenne muscular dystrophy and their respective caregivers agreed to participate and were included in this study. The age range of the patients who did not participate in this study was 10.2-14.9 years. Inclusion criteria for this study were being able to provide informed consent and comply with the study procedures. Children aged between 8.5 and 16 years were included. The study was approved by the local ethics committee (EKNZ 2017-01028). Informed consent was obtained from study participants and their parents.
The healthy children sample was derived from a normative sample of 9566 families previously collected by Varni and colleagues. 25 Healthy children are those children who were assessed either in physicians’ offices during checkups and/or whose parents did not report the presence of a chronic health condition. Data were obtained from the children and their caregivers. We used this normative sample in our study to compare the health-related quality of life child self- and parent proxy-reports of children with Duchenne muscular dystrophy to healthy peers.
Procedures
Patients were contacted by telephone and e-mail and asked if they are willing to participate in the study. After obtaining an explanation of the study, subjects agreed to participate willingly and voluntarily by signing the informed consent or giving assent (children aged <11 years). During the visit at the hospital, each participant was assessed individually in rooms containing a mat, a stretcher, and the material required to answer the scales and questionnaires. Participants were evaluated by trained physical therapists. The Motor Function Measure was used to assess the motor functional status. 26 Health-related quality of life was assessed with the generic module PedsQL Generic Core Scale 27 and the disease-specific module PedsQL Neuromuscular Module. 11 Participants were allowed to take a short rest when necessary while answering the questionnaires. Each caregiver answered to the questionnaires while the participants were assessed with the Motor Function Measure. Eighteen patients of 34 had difficulties in getting to the hospital (mainly due to loss of ambulation) and received the questionnaires by mail and were interviewed by telephone about their current clinical status.
Measures
Generic health-related quality of life
Generic health-related quality of life was assessed with the PedsQL 4.0 Generic Core Scale. The PedsQL Generic Core Scale was developed to assess health-related quality of life in children and adolescents aged 2 to 18 years in both healthy and disease populations. 27 The PedsQL Generic Core Scale contains 23 items across 4 domains: physical (8 items), social (5 items), emotional (5 items), and school (5 items) functioning. Items are linearly transformed to a 0-to-100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0), so that higher scores indicate better health-related quality of life. Scale scores are computed as the sum of the items divided by the number of items that were answered. To create a psychosocial health summary score, the mean is computed as the sum of the items divided by the number of items in the emotional, social, and school functioning scales. The PedsQL Generic Core Scale is composed of parallel child self-report and parent proxy-report formats.
Disease-specific health-related quality of life
Disease-specific health-related quality of life was assessed with the PedsQL 3.0 Neuromuscular Module. The PedsQL Neuromuscular Module was developed specifically for use in neuromuscular diseases including Spinal muscular atrophy and Duchenne muscular dystrophy. 11 The measure contains 25 items across 3 domains: About My Neuromuscular Disease (17 items related to the disease process and associated symptomatology), communication (3 items related to the patient’s ability to communicate with health care providers and others about his or her illness), and About Our Family Resources (5 items related to family financial and social support systems). The format, instructions, Likert response scale, and scoring method for the PedsQL Neuromuscular Module are identical to the PedsQL Generic Core Scale. Higher scores on the PedsQL Neuromuscular Module indicate lower problems, and therefore better disease-specific health-related quality of life. The PedsQL Neuromuscular Module is composed of parallel child self-report and parent proxy-report formats. Both scales, the PedsQL Generic Core Scale and the PedsQL Neuromuscular Module, have previously been found to be valid and reliable in pediatric patients with Duchenne muscular dystrophy. 10
Motor function
Motor function was assessed with the Motor Function Measure. The Motor Function Measure is a validated quantitative scale used for assessment of motor abilities of both ambulant and nonambulant patients with neuromuscular disorders. 26 It includes 32 items that evaluate 3 dimensions of motor performance, including specific motor functions, such as the “transfers and standing posture” as the first dimension (D1) of the Motor Function Measure, the proximal and axial motor functions (second dimension of the Motor Function Measure; D2), and the distal motor function (third dimension of the Motor Function Measure; D3). Each item is scored on a scale from 0 (does not initiate movement) to 3 (completes the item with a standard pattern). The items are summed to comprise the overall motor function (Motor Function Measure total score) involving all of the motor dimensions, where the maximum represents normal motor function (100%). In this study, we analyzed the Motor Function Measure total score and its D1 subscore. D2 and D3 domains were not analyzed because they remain relatively stable at this disease stage and usually decline at more advanced disease stages.
Statistical Analysis
Because this was an observational study and did not test a predefined hypothesis, sample size was not dependent on a formal calculation. All subjects who performed the questionnaires were included in the analysis. Descriptive statistics were generated for demographic and clinical variables and reported as mean and SD values for continuous variables and frequencies/proportions for categorical variables. Mean PedsQL scale and total scores were calculated for the Duchenne muscular dystrophy self- and parent-proxy reports. One-sample t tests were used to investigate if the PedsQL Generic Core Scale scores of Duchenne muscular dystrophy patients differed from the scores of healthy peers from a normative sample collected by Varni and colleagues. 25 Subgroup analyses were performed where the Duchenne muscular dystrophy patients were stratified by ambulation status (ambulant vs nonambulant). The proportion of patients with Duchenne muscular dystrophy who reported clinically significant PedsQL Generic Core Scale subscores was calculated; the cutoff score for “clinical significance” was defined as >1 SD below the mean value of the healthy population sample mean. 28 Furthermore, the PedsQL scores were presented graphically. Thereby the mean and the 95% confidence interval were shown. For the healthy norm sample, the confidence interval was calculated from the SD and the number of patients reported in the literature assuming normal distribution. In order to assess parent-child agreement, intraclass correlation coefficients together with their 95% confidence intervals, calculated using 999 bootstrap replicates, were calculated between PedsQL child self-report and parent proxy-report. 29 To this end, the score was modeled in a mixed effects model using patient as random effect (1-way random effects model). The variance due to difference between patients was divided by the total variance seen in the data. Therefore, the intraclass correlation coefficient indicates the percentage of total score variance attributable to the difference between patients. The intraclass correlation coefficient has a value between 0 and 1, where 1 would indicate that the interpatient variance explains all the observed variance, and thus implies perfect agreement between parents and child. Intraclass correlation coefficients are designated as 0.40 for poor to fair agreement, 0.41 to 0.60 for moderate agreement, 0.61 to 0.80 for good agreement, and 0.81 to 1.00 for excellent agreement. 30 Furthermore, bivariate analysis using Spearman correlation was conducted to determine the association between PedsQL scores and motor function. Subgroup analyses were conducted aiming to explore the association between PedsQL scores and the D1 score in ambulant and nonambulant Duchenne muscular dystrophy patients, respectively. Correlation coefficients were interpreted as follows: 0 to 0.29 little to negligible correlation; 0.30 to 0.49 low correlation; 0.50 to 0.69 moderate correlation; 0.70 to 0.89 high correlation; and correlations ≥0.90 indicated a very high correlation. 23 No correlation for multiple testing was performed. Linear regression analyses (multivariate analysis) were conducted to determine the stability of the association between health-related quality of life and motor function when adjusted for age and corticosteroid use. For these analyses, the following variables were entered into the equations simultaneously: child age, corticosteroid use (yes/no) and D1 subscore separately, with each of the PedsQL scores, Generic Core Scale and Neuromuscular Module total scores for child self-report, and parent proxy-report as the dependent variable. Data were analyzed using R. Significance was set at P < .05 for all statistical analyses.
Results
Sample Characteristics
Thirty-three boys and 1 girl with Duchenne muscular dystrophy and their caregivers participated in the study. Demographic characteristics of the Duchenne muscular dystrophy sample and normative sample are shown in Table 2. The mean age of the participants was 11 years (range 9-14.1 years). Among all participants, 25 of 34 (73.5%) took corticosteroids (prednisone or deflazacort). In addition, 14 patients (41.2%) were ambulant and 20 were not able to walk 10 m without assistance (58.8%). No patient needed assisted ventilation. Caregiver respondents included mothers (79.4%), fathers (17.6%), and other family members (2.9%). Most parents were married (73.5%). Most families lived in a rural neighborhood (58.8%) and did not participate in a Duchenne muscular dystrophy support group (67.7%).
Demographic Characteristics in DMD Sample and Normative Sample.
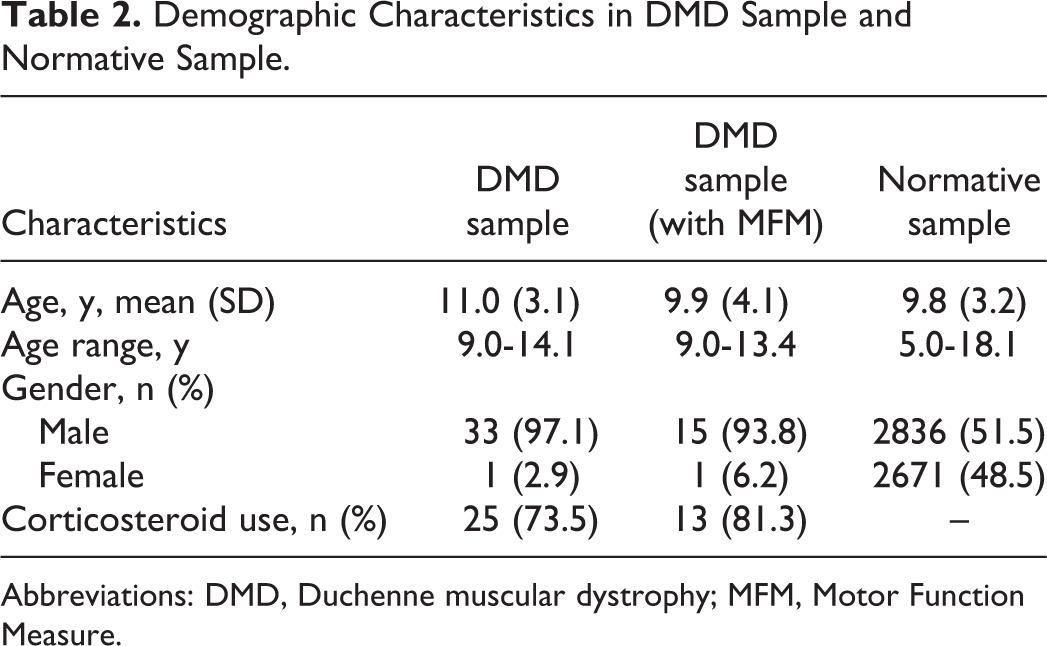
Abbreviations: DMD, Duchenne muscular dystrophy; MFM, Motor Function Measure.
Generic and Disease-Specific Health-Related Quality of Life in Duchenne Muscular Dystrophy Patients and Comparison to Healthy Sample
Descriptive statistics for the PedsQL Generic Core Scale and Neuromuscular Module child self-report and parent proxy-report and comparisons with healthy children scores are shown in Table 3. Examining the PedsQL Generic Core Scale subscores, patients and their parents rated the physical health with the lowest mean score (relating to the highest impairment) followed by social functioning, emotional functioning, and finally school functioning with the highest mean score (relating to the least impairment). The same pattern was seen in both subgroups of ambulant and nonambulant patients (Supplemental Table S1). Regarding the disease-specific PedsQL Neuromuscular Module scores in Figure 1, participants indicated About My Neuromuscular Disease with the highest score (relating to the least impairment), followed by About Our Family Resources, and communication (relating to the highest impairment). Parents rated About My Neuromuscular Disease with the highest score (relating to the least impairment), followed by communication, and About Our Family Resources.
PedsQL GCS and PedsQL NMM for Child Self-Report and Parent Proxy-Report for DMD Sample and Comparisons With Healthy Children Scores.
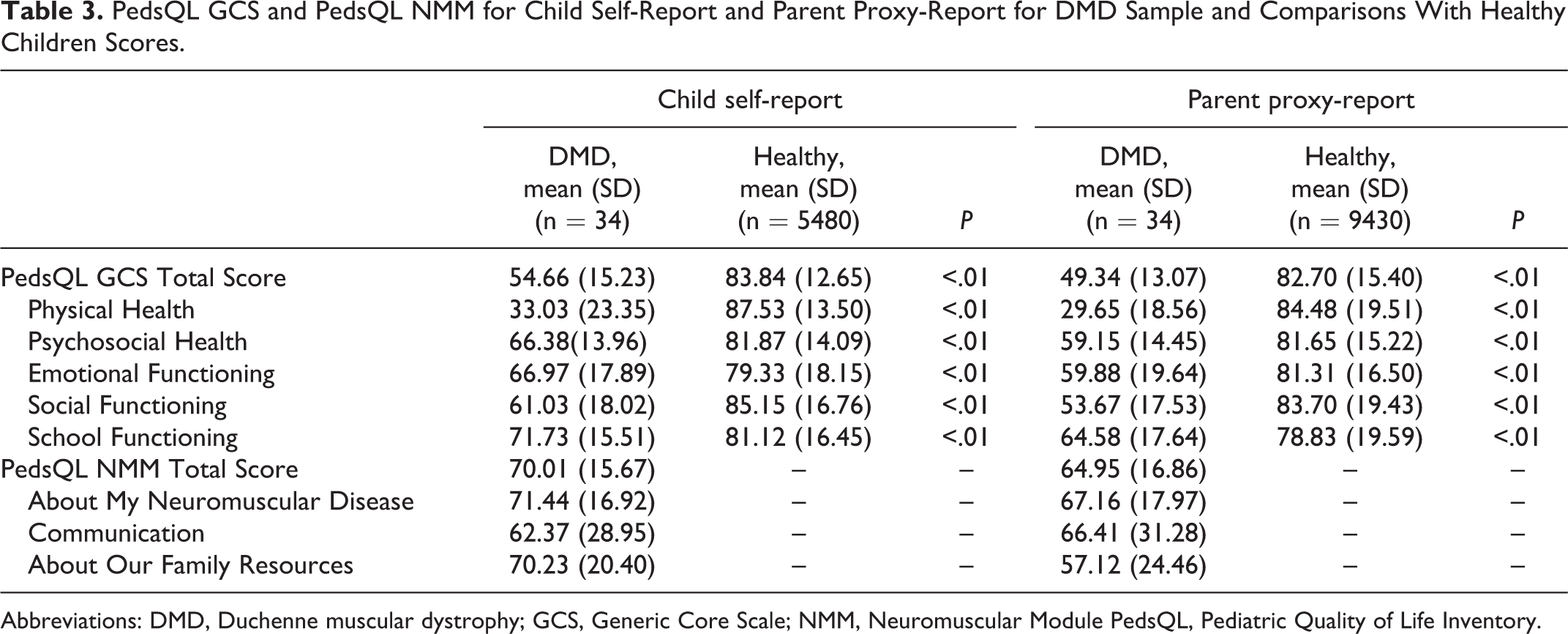
Abbreviations: DMD, Duchenne muscular dystrophy; GCS, Generic Core Scale; NMM, Neuromuscular Module PedsQL, Pediatric Quality of Life Inventory.
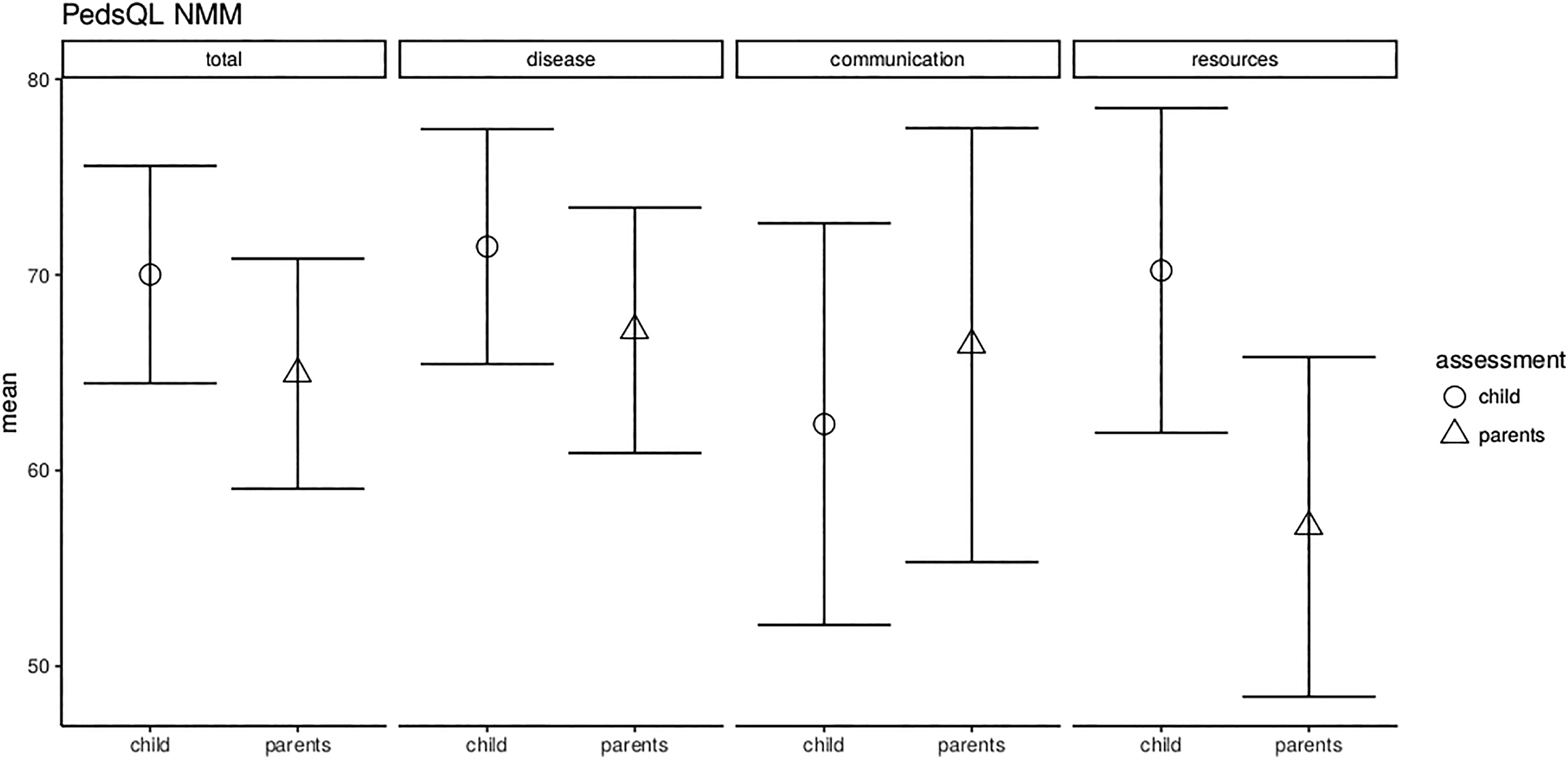
PedsQL NMM subscores for parent proxy-report and child self-report for the Duchenne muscular dystrophy sample. Thereby, the mean and the 95% confidence interval (CI) are shown. (NMM, Neuromuscular Module)
As shown in Figure 2, Duchenne muscular dystrophy patients revealed significantly lower scores in all subscores, both for parent-proxy report and child self-report, compared to the normative values of healthy children (P < .01). The largest difference in mean scores for the Duchenne muscular dystrophy patients compared to healthy children was seen in the physical health and the smallest in the school functioning. Subgroup analyses revealed that child self-report and parent-proxy report of nonambulant Duchenne muscular dystrophy patients display significantly lower scores in all subscores compared to the normative values of healthy children (P < .01). The same pattern was detected for ambulant Duchenne muscular dystrophy patients, with exception for child self-report emotional functioning (P = .07) and school functioning (P = .08) that did not differ significantly from normative data.
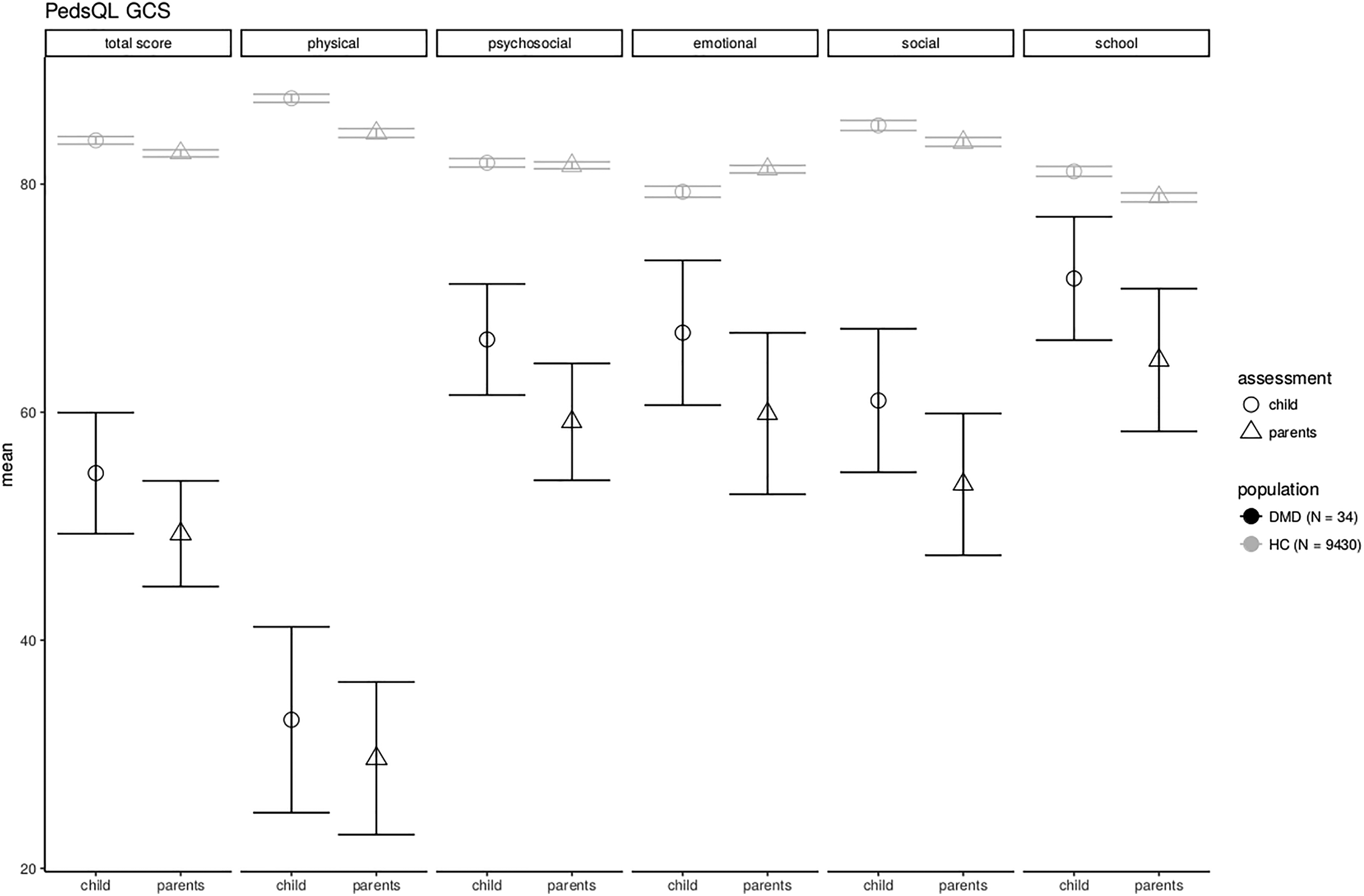
PedsQL Generic Core Scale subscores for child self-report and parent proxy-report for the Duchenne muscular dystrophy sample compared to the HC sample. Thereby, the mean and the 95% confidence interval (CI) are shown. (GCS, Generic Core Scale; HC, Healthy control)
By self-report, 55.9% of all patients had a psychosocial health summary score below 66.03, the cutoff point for significantly impaired psychosocial health-related quality of life in the general pediatric population. 28 Noticeably, 64.7% of the patients had a social score below the cutoff point of 66.61. As reported by the parents, 60.6% of the children with Duchenne muscular dystrophy had psychosocial health summary scores below 64.38, the cutoff score for significantly impaired psychosocial health-related quality of life. 28
Parent-Child Concordance of Health-Related Quality of Life
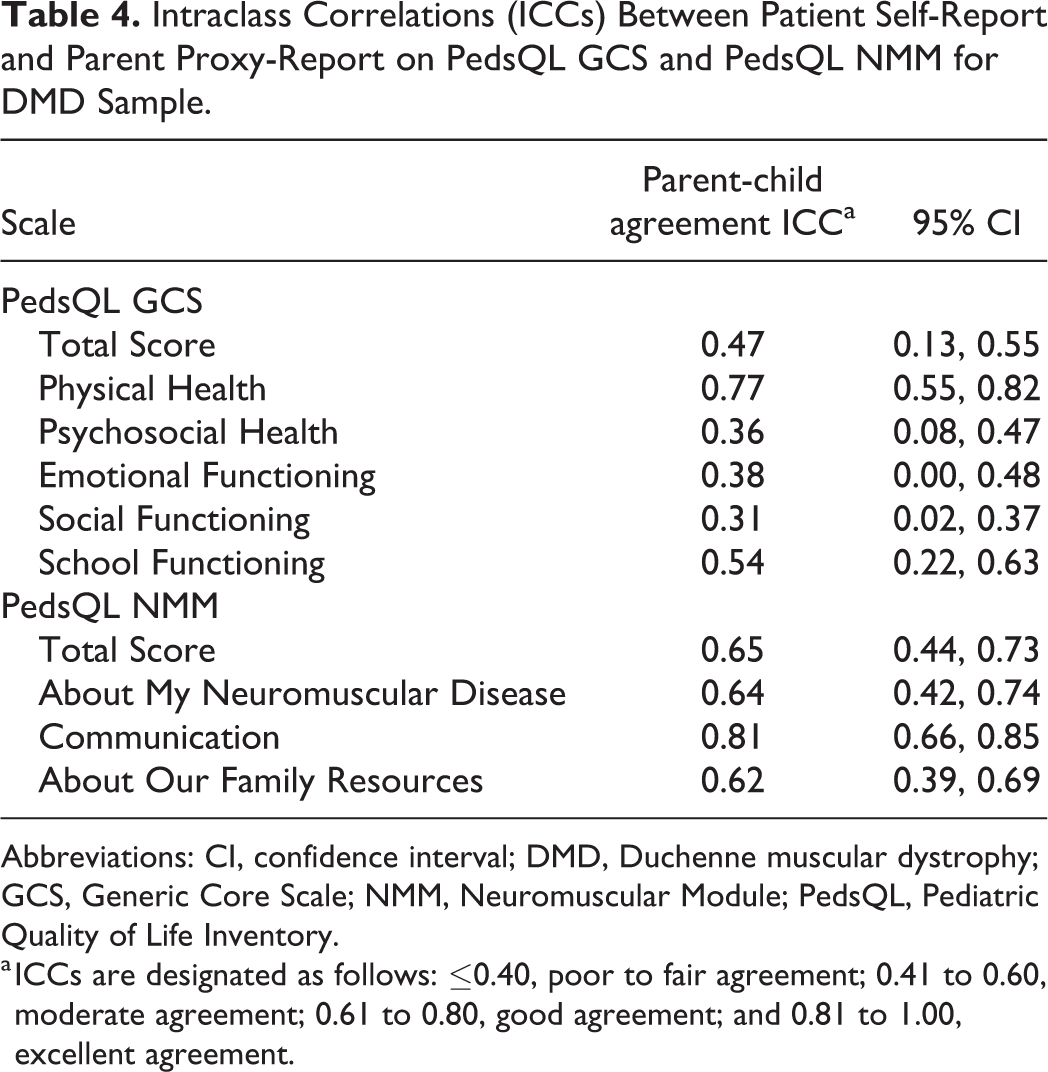
In light of observed differences between the perceptions of children and their parents, intraclass correlation coefficients were examined for each of the PedsQL Generic Core Scale and Neuromuscular Module scales. As shown in Table 4, the majority of intraclass correlation coefficients for the PedsQL Generic Core Scale indicated poor to moderate parent-child agreement for the general health-related quality of life. For the PedsQL Neuromuscular Module, the majority of the intraclass correlation coefficients were of good agreement, indicating that parents and children tend to agree well in their evaluation for the disease-specific health-related quality of life. The greatest overall agreement was found on the PedsQL Neuromuscular Module communication scale.
Intraclass Correlations (ICCs) Between Patient Self-Report and Parent Proxy-Report on PedsQL GCS and PedsQL NMM for DMD Sample.
Abbreviations: CI, confidence interval; DMD, Duchenne muscular dystrophy; GCS, Generic Core Scale; NMM, Neuromuscular Module; PedsQL, Pediatric Quality of Life Inventory.
a ICCs are designated as follows: ≤0.40, poor to fair agreement; 0.41 to 0.60, moderate agreement; 0.61 to 0.80, good agreement; and 0.81 to 1.00, excellent agreement.
Correlation Between the Subscales of Health-Related Quality of Life and Motor Function
The mean of the Motor Function Measure total score was 65% (SD = 18.96) and the D1 subscore 31% (SD = 32.40). As expected, the subscores D2 and D3 were only mildly impaired at this disease stage (D2: mean = 87.85, SD = 13.41; D3: mean = 88.69, SD = 10.98) and were therefore excluded from the analysis.
PedsQL Child Self-report
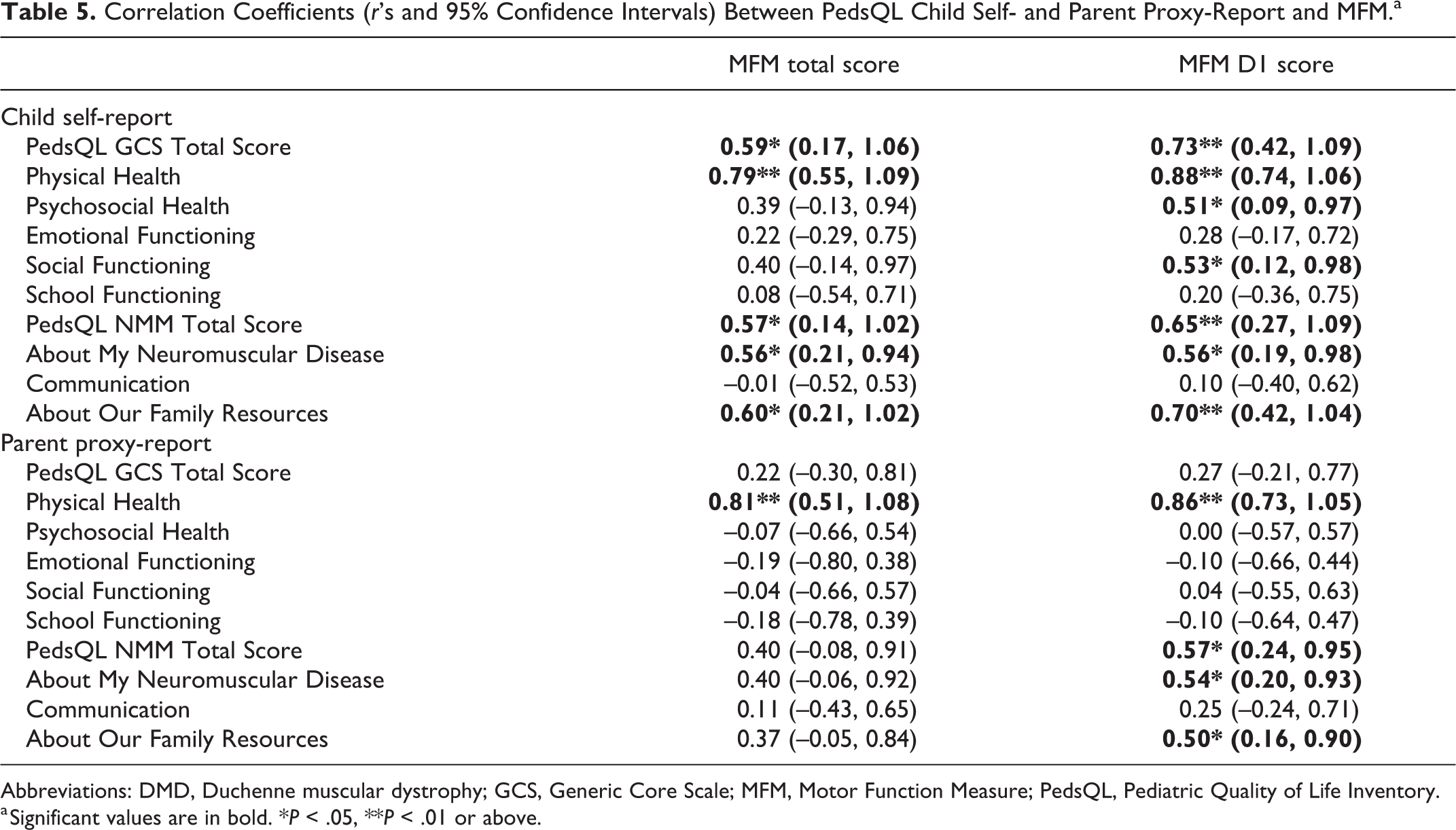
As shown in Table 5, the correlation between the PedsQL Generic Core Scale total score showed moderate positive correlation with the Motor Function Measure total score (r = 0.59, P = .02) and high positive correlation with the D1 score (r = 0.73, P < .01), indicating that higher generic health-related quality of life could be seen in patients with better motor function and better standing and transfer abilities. A high positive correlation between the domain physical health and the Motor Function Measure total score (r = 0.79, P < .01) and the D1 score (r = 0.88, P < .01) was found, which shows that patients with Duchenne muscular dystrophy, who have better overall motor function as well as standing and transfer abilities, perceive their physical health as better. A moderate positive correlation was found between the domains psychosocial health and social functioning and the D1 subscore (psychosocial: r = 0.51, P = .04; social: r = 0.53, P = .03), indicating that lower psychosocial and social health could be seen in patients with worsening ability to stand and transfer on their own.
Correlation Coefficients (r’s and 95% Confidence Intervals) Between PedsQL Child Self- and Parent Proxy-Report and MFM.a
Abbreviations: DMD, Duchenne muscular dystrophy; GCS, Generic Core Scale; MFM, Motor Function Measure; PedsQL, Pediatric Quality of Life Inventory.
a Significant values are in bold. *P < .05, **P < .01 or above.
For the PedsQL Neuromuscular Module, a moderate positive correlation was found between the total score and the Motor Function Measure total score (r = 0.57, P = .03) and the D1 subscore (r = 0.65, P < .01), indicating that better general motor function and their standing and transfer abilities are associated with higher disease-specific health-related quality of life in Duchenne muscular dystrophy patients. In accordance, we found a moderate positive correlation between the About My Neuromuscular Disease domain and the Motor Function Measure total score (r = 0.56, P = .032) and the D1 (r = 0.56, P = .031). Additionally, a moderate to high correlation between the About Our Family Resources domain and the Motor Function Measure total (r = 0.60, P = .019) and the D1 subscore (r = 0.70, P < .01) existed, indicating that poorer motor function could be seen in patients with worsening family financial and social support system resources. All the other correlations were not significant.
Subgroup analysis for ambulant patients revealed high positive correlation between the PedsQL Generic Core Scale total score and the Motor Function Measure total score (r = 0.77, P = .02) and the D1 score (r = 0.74, P = .02) (Supplemental Table S2). Also, the domain physical health correlated with the Motor Function Measure total score (r = 0.80, P < .01) and the D1 score (r = 0.79, P = .01). No significant correlations were found for nonambulant patients.
PedsQL Parent Proxy-report
For the PedsQL Generic Core Scale, a high positive correlation was found between physical health and the Motor Function Measure total score (r = 0.81, P < .01) as well as the D1 subscore (r = 0.86, P < .01), indicating that parents perceive a higher patients’ physical health in patients with better motor function and ability of stand and transfer. Similarly, for the PedsQL Neuromuscular Module, a moderate positive correlation was found between the total score and the D1 subscore (r = 0.57, P = .02). Additionally, a moderate correlation existed between the About My Neuromuscular Disease domain, the About Our Family Resources, and the D1 subscore (Neuromuscular Disease: r = 0.54, P = .03; Family Resources: r = 0.50, P = .048). All the other correlations were not significant. Correlations of the specific subscales of the PedsQL Generic Core Scale and Neuromuscular Module and motor function derived from the Motor Function Measure are shown in Table 5. In Figure 3, the association between the physical health and Motor Function Measure total score as well as D1 subscore for both parent proxy-report and child self-report are presented.
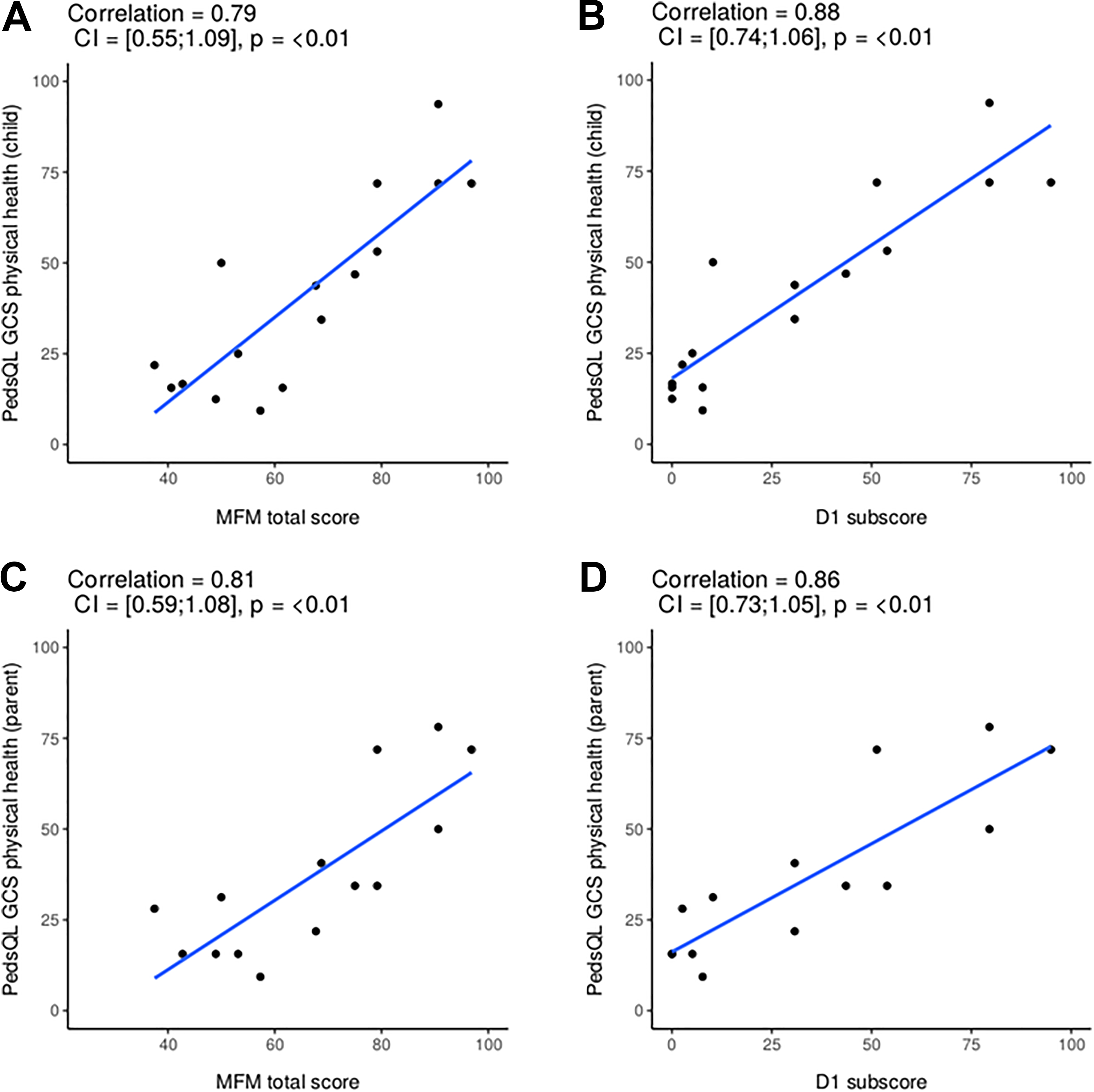
Correlations between PedsQL physical health score and functional measures for child self- (A and B) and parent proxy-report (C and D).
Subgroup analysis for ambulant patients revealed a high positive correlation between the PedsQL Generic Core Scale physical health domain and the Motor Function Measure total score (r = 0.82, P < .01) and the D1 score (r = 0.75, P = .02). The physical health domain indicated high negative correlation with the Motor Function Measure total (r = –0.89, P = .04) in nonambulant patients, showing that parents of nonambulant patients who have high overall motor function evaluate their physical health as poor. Moreover, a high negative correlation was found between the PedsQL Neuromuscular Module total score and the Motor Function Measure total score (r = –0.79, P = .05), indicating that better general motor function is associated with lower parent-rated disease-specific health-related quality of life in nonambulant Duchenne muscular dystrophy patients.
Table 6 presents multivariate analysis only for the D1 subscore, because the D1 score revealed higher correlations with health-related quality of life scores than the Motor Function Measure total score in the univariate analysis. Significant associations between PedsQL scores and Motor Function Measure total score from the univariate analysis retained their independent significance in the multivariate analyses, when adjusted for age and corticosteroid use. Results of the multivariate analysis that had the PedsQL Generic Core Scale total score (child self-report) as the dependent variable and the D1 score, age, and corticosteroid use as the independent variables indicated that the D1 score contributed significantly to the regression model (β = 0.42, confidence interval: 0.21, 0.62, P < .01), when adjusted for age and corticosteroid use. Similarly, for the PedsQL Neuromuscular Module total score child self-report and parent proxy-report, the D1 score was found to be a significant contributor to the regression model (child self-report: β = 0.43, confidence interval: 0.09, 0.55, P = .01; parent proxy-report: β = 0.36, confidence interval: 0.09, 0.63, P = .01).
Summary of Regression Analyses for the Impact of Different Variables on Generic and Disease-Specific Health-Related Quality of Life in DMD Patients.
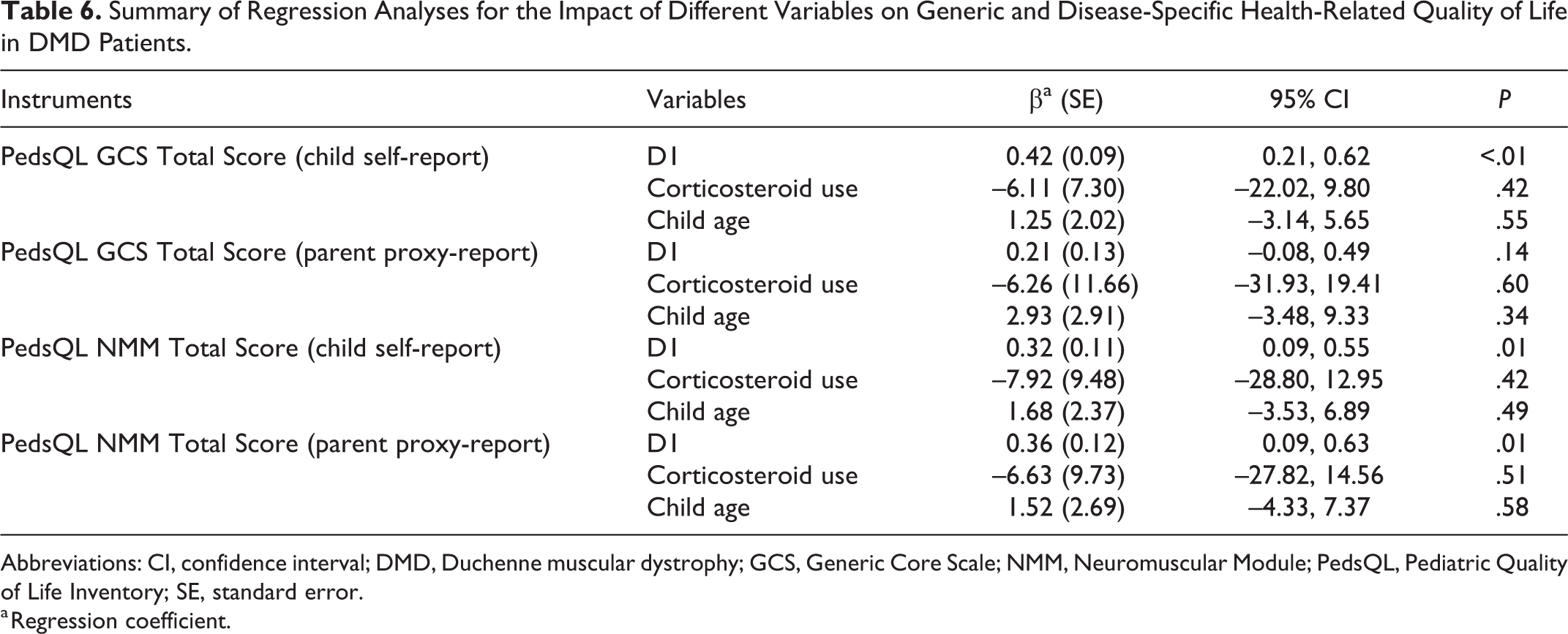
Abbreviations: CI, confidence interval; DMD, Duchenne muscular dystrophy; GCS, Generic Core Scale; NMM, Neuromuscular Module; PedsQL, Pediatric Quality of Life Inventory; SE, standard error.
a Regression coefficient.
Discussion
This cross-sectional study demonstrated several moderate to high correlations between different aspects of the generic and disease-specific health-related quality of life in Duchenne muscular dystrophy patients and their functional motor function. The aim of this study was not to duplicate previous reports on health-related quality of life in Duchenne muscular dystrophy or their correlation with different demographic data, but to establish the value of the PedsQL in assessing health-related quality of life in relation to possible functional changes of the Motor Function Measure. As expected, the physical health correlated with the Motor Function Measure and its standing and transfer subdomain both on child self-report and parent-proxy report. This finding is in line with previous study results including different functional outcomes. 14,22,31 To our knowledge, this is the first observational study to show a significant association between the self-reported psychosocial health, the social functioning, and the standing and transfer functional score of the Motor Function Measure. A possible explanation for this could be that due to the progressive physical weakness experienced by children affected by Duchenne muscular dystrophy, their ability to participate in a variety of physical and social activities is limited. Children may miss out on the opportunity to maintain relationships and participate in social activities, where wheelchair access is not given. 32 Further, periods in which disease severity increases (eg, losing the ability to stand and to transfer, becoming wheelchair dependent) may be associated with experiencing more emotional difficulties such as feeling anxious or depressed.
At a variance with previous studies, 14,18,31 we also used the PedsQL Neuromuscular Module, which was developed specifically for the use in neuromuscular diseases and has previously been found to be valid and reliable in Duchenne muscular dystrophy. 10 Notably, its use did not appear to increase the level of significance compared to the general module except for the family resources domain that correlated better with the motor function in the children’s questionnaire. Poorer patients’ motor function was associated with worsening of family financial and social support system resources. Therefore, families are overburdened by the illness and by the responsibilities of caring for their child that they are more likely to experience chronic emotional stress because of overcommitment, family conflict, and the demands of caring for their child with complex medical needs. 33,34 Other problems that are frequently addressed are the social isolation and financial considerations of the families, which also may be a burden. 35 –37 Another explanation could be that the socioeconomic status of the family may have an influence on the health-related quality of life, so that children with chronic disease from lower socioeconomic backgrounds experience reduced health-related quality of life compared with their wealthier counterparts independent of the neurologic course of the disease. 38
The subgroup of ambulant patients reported that their generic health-related quality of life and their physical health correlated with the Motor Function Measure and its standing and transfer subdomain. Although parents of ambulant patients reported that their physical health is positively associated with the overall motor function, in nonambulant patients this association was negative, indicating that parents rate the physical health of nonambulant patients who have better overall motor function as poor. A possible explanation for this finding may be that because in general parents’ ratings tend to be lower than patient self-reports, parents may underrate the health-related quality of life of nonambulant patients and patients may have already adapted to their physical difficulties although their parents still have not.
It is important to note that the statistically significant positive correlation between generic and disease-specific health-related quality of life and the standing and transfer subdomain of the Motor Function Measure obtained in the bivariate analysis was also observed in the multivariate analysis, when adjusted for age and corticosteroid use. Previous findings indicated no significant effects of corticosteroids on PedsQL measures in Duchenne muscular dystrophy patients, confirming our findings. 14 This is the first study to describe a significant association between different aspects of the health-related quality of life such as psychosocial health, social functioning, family resources, and functional outcome measures. Because previous studies examined only ambulant Duchenne muscular dystrophy patients, 14,18,22 our aim was to include both ambulant and nonambulant Duchenne muscular dystrophy patients. This may reveal different results because of neglect of the natural disease progression. In one study, the PedsQL Generic Core Scale physical health score and the PedsQL Neuromuscular Module score About My Neuromuscular Disease were significantly different in full-time wheelchair users versus part-time/full-time ambulatory patients. 10 However, it is important to note that our results are to be interpreted with caution as only 16 participants (47%) performed the Motor Function Measure and the separate patient groups stratified by ambulation status were very small.
Consistent with results of previous studies, 10,12,14 –16 our findings reflect that the health-related quality of life of children with Duchenne muscular dystrophy is considerably affected in the physical and psychosocial domain compared to healthy peers. An impaired psychosocial health was detected in more than half of the children. These data confirm previous findings showing that between 30% and 50% of Duchenne muscular dystrophy boys have psychosocial problems. 15,39,40 A possible explanation could be that younger children with Duchenne muscular dystrophy may not have developed effective coping strategies yet and therefore still have difficulties adjusting emotionally to living with the disorder. Several studies found a trend toward improved psychosocial functioning with advancing age, indicating that adolescents with Duchenne muscular dystrophy tend to report better psychosocial functioning than younger affected individuals. 15,40 Additionally, confrontation with the consequences of the disease (such as increased physical complaints and wheelchair dependency) can be associated with emotional difficulties. 41 Noticeably, the social functioning was found to be the second most impaired domain. More than 60% of the participants reported significantly impaired social functioning. This finding supports previous studies that suggested that children with Duchenne muscular dystrophy score significantly worse on the Social Problems scale than either unaffected siblings or children with cerebral palsy, independent of their cognitive abilities or motor impairment. 42 This may be due to the fact that children with Duchenne muscular dystrophy appear to have mild difficulties in matching facial affects, suggesting that they may lack the subtle social perception skills that are necessary for optimal interpersonal integration. Hendriksen and colleagues found that functioning in peer relations decreased with increasing age. 40 It is essential to identify those children who show early signs of social adjustment difficulties to initiate behavioral counseling services such as social-skills training in expedient manner as secondary and tertiary preventive interventions. 43
Subgroup analyses indicated that ambulant and nonambulant patients and their parents rated the health-related quality of life as lower compared to healthy peers in all domains, apart from the finding that ambulant patients rated their reported emotional and school functioning as comparable to healthy peers. However, it is important to note that this finding is to be interpreted with caution as the ambulant patients group consisted of only 14 participants.
Our findings suggest that parents generally rated their child’s health-related quality of life lower than children themselves did, which has been consistently observed in Duchenne muscular dystrophy patients and across a number of other pediatric chronic illnesses. 10,15,31,44 This difference tends to be greater in the psychosocial domains than in the physical domain. There are a number of possible explanations for this observation: children may have adapted better to their illness than their parents have, and parents may not always have the most accurate assessment of their child’s emotional state. In addition, parents’ own worries and fears about their child’s disease may influence their assessment of their child’s health-related quality of life. Until now, few studies included both child self-reports and parent proxy-reports about health-related quality of life in Duchenne muscular dystrophy and investigated the level of agreement between children’s self-reports and parents’ reports. Poor to moderate parent-child agreement was found for the PedsQL Generic Core Scale and good parent-child agreement for the PedsQL Neuromuscular Module. In studies that used the PedsQL Generic Core Scale, we could replicate the findings revealing that only the school domain had moderate concordance, whereas other domains had poor concordance. 10,15,31 Taken together, the data suggest that Duchenne muscular dystrophy patients and their parents tend to agree better on disease-specific health-related quality of life aspects than on general health-related quality of life. Evaluating both children’s and parents’ perspectives regarding health-related quality of life should be the standard for routine assessment in clinical practice and clinical trials for children with neuromuscular disorders because their different perspectives potentially provide different unique information.
This study documented association between different aspects of patient-reported generic and disease-specific health-related quality of life and clinician-measured motor abilities. This lent support to the concept that the commonly used Motor Function Measure is “clinically meaningful” in the context of a patient’s day-to-day-life. In the present study, we observed that several aspects of health-related quality of life in patients with Duchenne muscular dystrophy (specifically the physical health, psychosocial health, social functioning, etc) are positively related to motor function. Further studies on longer time frame may help to explain the complexity of the relationship between health-related quality of life and functional performances. McDonald and colleagues concluded that the Pediatric Outcomes Data Collection Instrument is more sensitive to Duchenne muscular dystrophy disease progression than the PedsQL. 14 Future studies should include additional tools measuring health-related quality of life, such as the Pediatric Outcomes Data Collection Instrument and/or specific questionnaires addressing changes in activity of daily living.
There are a number of important limitations of this analysis. This study included only 1 cross-sectional assessment; therefore, longitudinal studies are needed in order to confirm the association between motor function and patient-reported health-related quality of life. Although both global and disease-specific health-related quality of life were correlated with the functional status of the patients, other factors (eg, socioeconomic status) may also influence health-related quality of life. Another limitation is that the association between health-related quality of life and motor function was adjusted for age and corticosteroid use, which is only possible to a limited extent because of the study’s small sample size. It will be important to replicate these findings in a larger sample. Moreover, all included patients participated already in a clinical trial, which may bias the results. Because the motor function assessment was performed in less severely affected Duchenne muscular dystrophy patients, a selection bias can be assumed for the estimated motor function.
Supplemental Material
Supplementary_Tables - Association Between Health-Related Quality of Life and Motor Function in Ambulant and Nonambulant Duchenne Muscular Dystrophy Patients
Supplementary_Tables for Association Between Health-Related Quality of Life and Motor Function in Ambulant and Nonambulant Duchenne Muscular Dystrophy Patients by Vanya Gocheva, Simone Schmidt, Anna-Lena Orsini, Patricia Hafner, Sabine Schaedelin, Nicole Rueedi, Peter Weber and Dirk Fischer in Journal of Child Neurology
Footnotes
Acknowledgments
We would like to acknowledge our patients who participated in the study and made a major contribution to advance knowledge in Duchenne muscular dystrophy. We would also like to acknowledge Sabine Hobi for linguistic revision. This study was funded by the Neuromuscular Research Association Basel (NeRAB), Switzerland; we’d like to thank for this financial support.
Author Contributions
VG participated in the design of the study, acquired data, and drafted the manuscript. PH, AO, and SiS participated in the design of the study and acquired data. VG and NR participated in patient recruitment. NR and VG participated in the organization and the conduct of the study. SaS performed the statistical analysis. PW revised the manuscript critically for important intellectual content. DF designed the study, analyzed data, and drafted the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DF is principal investigator for studies on spinal muscular atrophy sponsored by Hofmann-La Roche Ltd. There are no other activities related to commercial companies. All authors declare that they have no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Neuromuscular Research Association Basel (NeRAB), Switzerland.
Supplemental Material
Supplemental material for this article is available online.
Ethical Approval
Ethics approval has been obtained from the local Ethics Committee (EKNZ 2017-01028). All the research meets the ethical guidelines, including adherence to the legal requirements of the study country.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.