
Abstract
Nocturnal enuresis is one of the side effects of valproic acid treatment, and generally underdiagnosed by clinicians. Studies reported that a variable incidence of valproic acid–induced nocturnal enuresis is 2.2% to 24% with unclear explanations of the reasons behind valproic acid–induced nocturnal enuresis. A retrospective study was carried out on 260 children (aged 5-12 years) diagnosed with idiopathic epilepsy, treated with valproic acid to evaluate the nocturnal enuresis secondary to valproic acid, and to discuss the characteristics of their sleep architecture. Nocturnal enuresis was reported in 28 (10.7%) patients after a mean exposure time to valproate of 18.78±8.4 days. Nocturnal enuresis was significantly associated with younger age and serum level of valproate (P = .05). The polysomnographic study suggested that the underlying mechanism may be related to impaired sleep efficiency, frequent arousals, prolonged sleep latency, snoring, or increased sleep depth which may impair a child’s ability to awaken to the sense of bladder fullness or contractions.
Clinical trial registration: ClinicalTrials.gov identifiers: NCT04191863
More than 50 years ago, valproic acid was established as an effective broad-spectrum antiepileptic drug. 1,2 It is a drug of choice in children and adults with generalized or focal types of epilepsy and generalized convulsive status epilepticus. 3 It is used in migraine prophylaxis and as a modulator of chemotherapy in cancer treatment. Moreover, valproic acid may have a potential role in neuroprotection in stroke patients and head trauma. 4 Overall, valproic acid is tolerated regarding cognitive functions, but has common dose-related side effects like fatigue, gastrointestinal disturbances, increased body weight, tremor, loss of hair, thrombocytopenia, and teratogenicity. On the other hand, pancreatitis, hepatotoxicity, and hyperammonia in the blood are less frequent side effects. 5,6
Enuresis is defined as involuntary nocturnal urination of children aged above 5 years whereas toilet training has been achieved before. 7 The prevalence of nocturnal enuresis in the general pediatric population was 18.5%, with a higher incidence in boys, which increases with stress and family troubles and decreases with increasing age. 8 A recent study investigating nocturnal enuresis risk factors in children in Egypt concluded that pinworm infestation, constipation, and consumption of caffeine are potentially reversible risk factors. 9
Nocturnal enuresis is one of the side effects of valproic acid treatment and generally underdiagnosed or overlooked by clinicians. A comprehensive review study about the effects of valproic acid did not mention that nocturnal enuresis was an adverse event of the valproate. 10 However, more recent studies reported a variable incidence of valproic acid–induced nocturnal enuresis of 2.2% to 24%. 11,12 Three major factors hypothesized to be behind enuresis are increased nocturnal urine production, detrusor hyperactivity, and impaired arousal process. Both the arousal process and the micturition reflex are mediated by nuclei in the brain stem. 13
Sleep disorders are strongly associated with childhood nocturnal enuresis. 14 Several studies have assessed the sleep architecture and characteristics in children with mainly the primary nocturnal enuresis. 15 In a trial to investigate the role of sleep characteristics and sleep stages in the primary nocturnal enuresis, the relationships between nocturnal enuresis and sleep disturbances were evaluated. 16 Ma et al 17 observed that children with nocturnal enuresis have more sleep problems like insomnia, impaired sleep duration, frequent arousal, sleep-disordered breathing, and sleepiness in the daytime more than children without nocturnal enuresis. Nocturnal enuresis occurs during the early hours of the night and mainly in deep sleep during the second sleep stage. Recent researches find variations in sleep microstructure in children with nocturnal enuresis. 15
There are conflicting results from studies assessing sleep using polysomnography in children with nocturnal enuresis as some studies have reported that the polysomnography results of children with nocturnal enuresis were similar to those of control children, whereas other studies have shown significant differences between the 2 groups. 18,19
Few studies evaluated the relationship between sleep architecture and secondary nocturnal enuresis. Therefore, we aimed to study and to evaluate the characteristics of the sleep architecture of nocturnal enuresis in epileptic children kept on valproate monotherapy.
Patients and Methods
Participants
The study was conducted on 260 children with epilepsy receiving valproate monotherapy aged 5-12 years who attended the outpatient clinic of neurology departments from September 2019 to February 2020. Twenty-eight of the 260 children maintained on valproate therapy had complications of nocturnal enuresis, the sample consisting of 16 men and 12 women aged 5-12 years (7.6 ± 2.4 years). Twenty-eight healthy controls who were age and sex matched, aged 5-12 years (8.3 ± 1.96 years), nonepileptic, and did not report enuresis (rather than healthy controls) were used for comparison with the 28 children whose sleep architecture had complications of nocturnal enuresis (Figure 1).
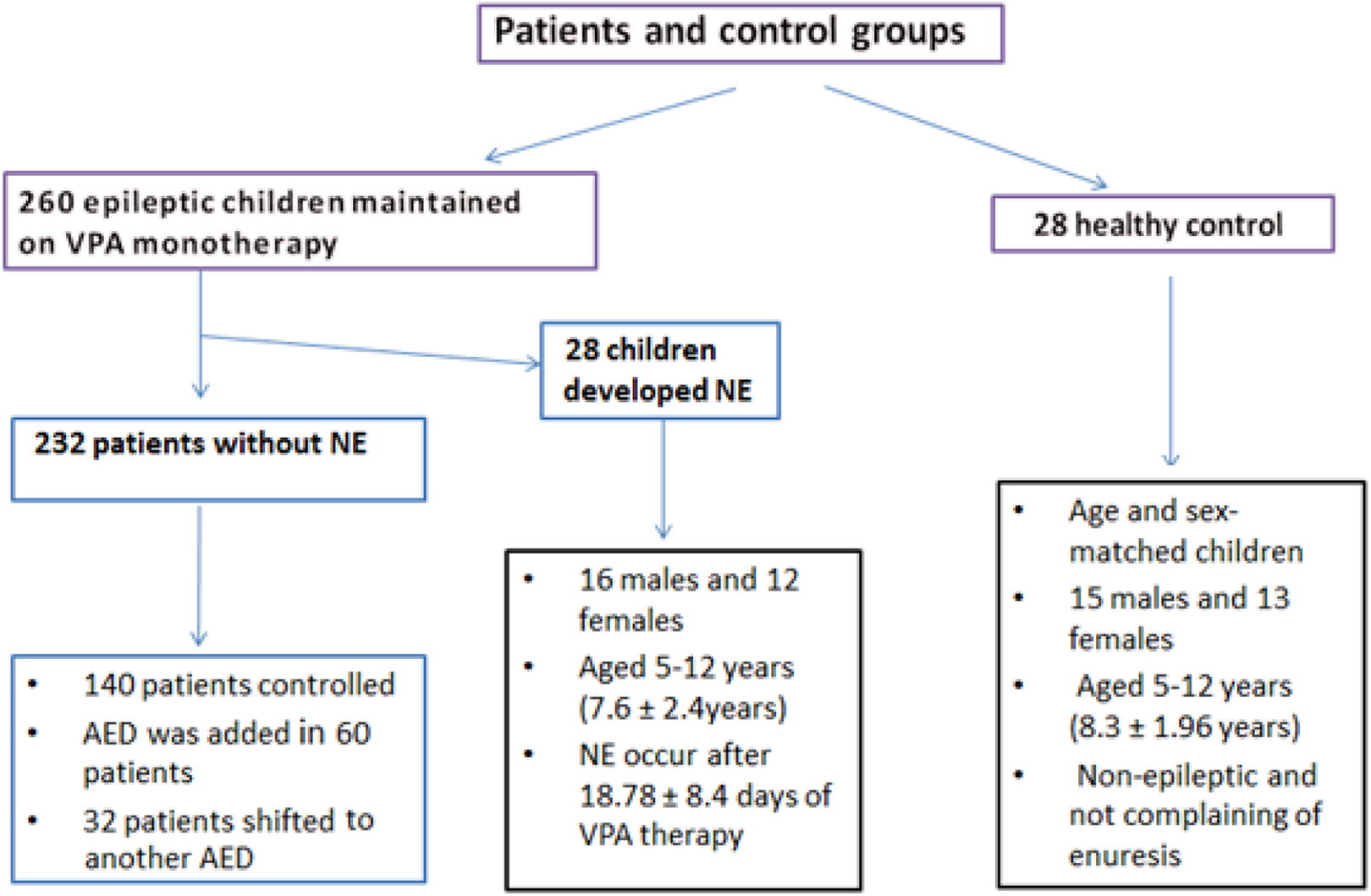
Study flow chart showing the participants included in this study.
Inclusion Criteria
Epileptic children aged 5-12 years who started and were maintained on valproate monotherapy were included. In this study, children were determined to have nocturnal enuresis based on the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria, which included “an involuntary voiding of urine during sleep, with the severity of at least twice a week, in children aged 5 years or older, in the absence of congenital or acquired defects of the nervous system.” 20
Exclusion Criteria
The exclusion criteria included primary nocturnal enuresis (children who did not accomplish any period of evening dryness over 6 successive months) and congenital or acquired defects of the nervous system, such as myelomeningocele / spina bifida, urinary system anomalies, or acquired neoplastic or inflammatory disorders of the nervous system, that interfere with the innervation of the bladder.
Also, children receiving combined therapy with other antiepileptic drugs were excluded.
Clinical, Electroencephalographic (EEG), and Laboratory Assessment (Abstracted From Each Patient Record)
The patients’ history, demographic, and complete medical and neurologic examinations were assessed. Brain CT and EEG were routinely done for all patients. An electroencephalogram was done for all patients to document the presence or absence of any epileptiform activity. Electroencephalogram (EEG) was carried out using the 10-20 International System for about 20 minutes under standard conditions and by using provocative techniques like hyperventilation and photic stimulation. Recordings were performed using EB Neuro Basis BE Hardware (Florence, Italy) and Galileo Software (Florence, Italy) for EEG data acquisition and review. The following laboratory tests were done for all patients, including blood urea nitrogen, serum creatinine, urinary pH, serum levels, and therapeutic doses of valproate. Urinary tract ultrasonography (with full and void bladder) was done for evaluation of the urinary system. Patients were therefore assessed monthly for a follow-up over a time of 6 sequential months, with extra visits as required depending on seizure recurrence or side effects.
Evaluation of the Reported Side Effects Especially Nocturnal Enuresis Associated With Valproate
Evaluation of seizures control and the reported side effects associated with valproate were determined with special consideration about the incidence of nocturnal enuresis and its frequency (daily and monthly).
The time between the initiations of valproate monotherapy to the beginning of nocturnal enuresis, the daily dose, and the duration of treatment of valproic acid (mg/kg) at the onset of enuresis and the serum level of valproic acid were reported. Also, the time of cessation of nocturnal enuresis, whether spontaneous or following discontinuation of valproate, was determined.
Polysomnography Study
Polysomnography was carried out for 28 children with secondary nocturnal enuresis and 28 age- and sex-matched control children. Polysomnography with standard EEG montage that includes bilateral electrooculography and 4 EEG leads were used. A single attended overnight polysomnographic study was performed at the Clinical Neurophysiology Unit of Mansoura University Hospitals. Children were studied in a quiet, darkened room in the presence of one of their guardians. No medications were used to induce sleep. All participants underwent 1 night of laboratory-based polysomnography.
Statistical Analysis
Information and findings of this study were analyzed with SPSS version 22. Continuous data were shown in the form of mean±SD whereas categorical data were shown in the form of numbers and percentages. Continuous data were compared using the Student t test whereas categorical comparison was done using the chi-square test. A multivariate logistic regression analysis was carried out for the following independent variables: snoring index, sleep latency, N1%, sleep efficiency, sleep arousal, age, weight, body weight, duration of treatment, daily dose of valproate, and serum valproate level.
Correlation analysis was carried out by using Pearson correlation test for the assessment of the correlations between the nocturnal enuresis and polysomnography. P value <.05 was considered statistically significant.
Results
A total of 260 children in the range of 5 and 12 years who were maintained on valproate (153 males and 107 females) were included in this study. Regarding the types of epilepsy in our cases, there were 122 epileptic children diagnosed as idiopathic generalized epilepsy, 79 epileptic children diagnosed as an idiopathic focal type of epilepsy, 30 epileptic children diagnosed as absence epilepsy, and 20 epileptic children diagnosed as myoclonic epilepsy. Neurologic and medical examinations for all of these children were normal.
Side Effects
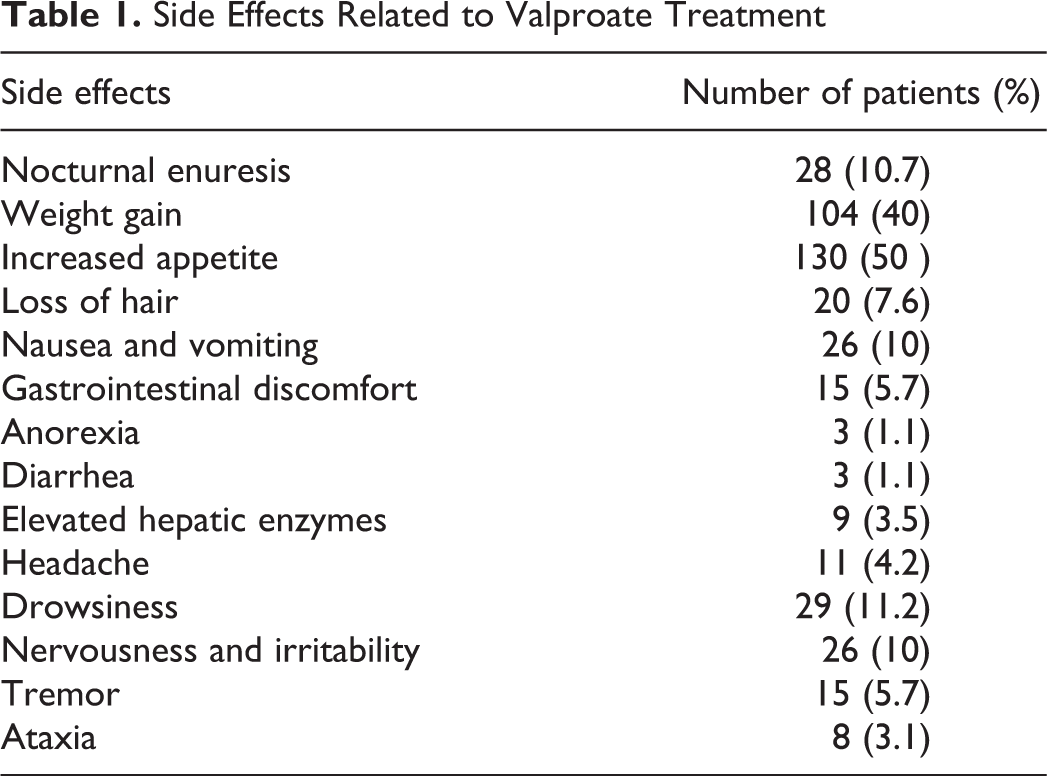
Table 1 showed the side effects that were present in children during treatment by valproic acid. The most common side effects were increased appetite and body weight (50% and 40%, respectively). Nocturnal enuresis happened in about 10.7% and drowsiness in 11.2%. Nervousness and irritability was reported in 10% of children, and nausea and vomiting occurred in 10% of children. In contrast, other side effects like tremor, dizziness, ataxia, headache, anorexia, diarrhea, gastrointestinal discomfort, loss of hair, and elevated hepatic enzymes were less common.
Side Effects Related to Valproate Treatment
Children With Enuresis
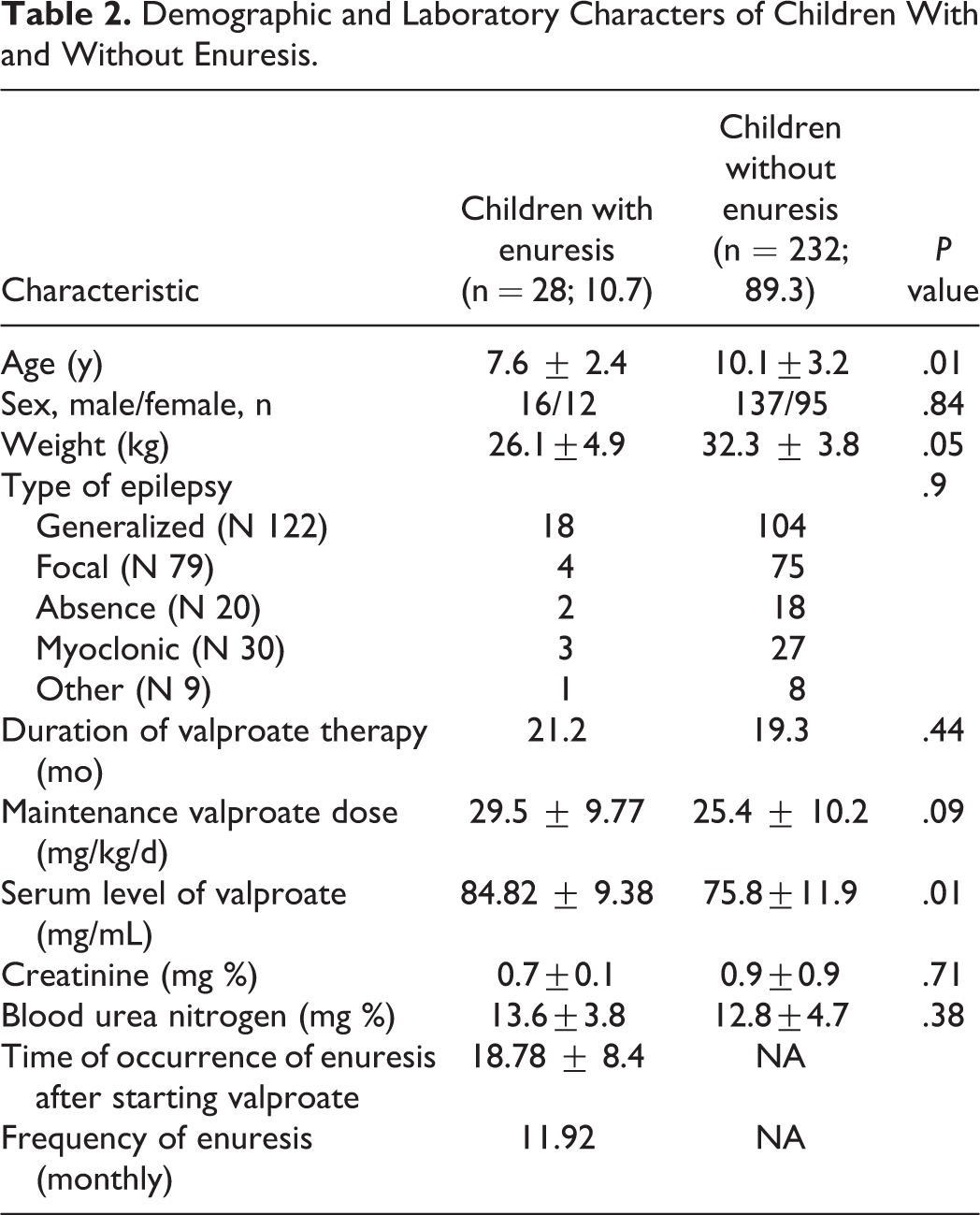
Nocturnal enuresis following initiation of valproate therapy occurred in 28 children (10.7%; 16 male and 12 female). The mean time of nocturnal enuresis to occur after initiation of valproate monotherapy was 18.78 ± 8.4 days. Table 2 showed the features of children with secondary nocturnal enuresis in comparison with children who did not develop enuresis. Also, clinical and laboratory features of patients with valproic acid–induced nocturnal enuresis were presented in detail in Table 3.
Demographic and Laboratory Characters of Children With and Without Enuresis.
Clinical and Laboratory Features of Patients With Valproic Acid–Induced nocturnal Enuresis.
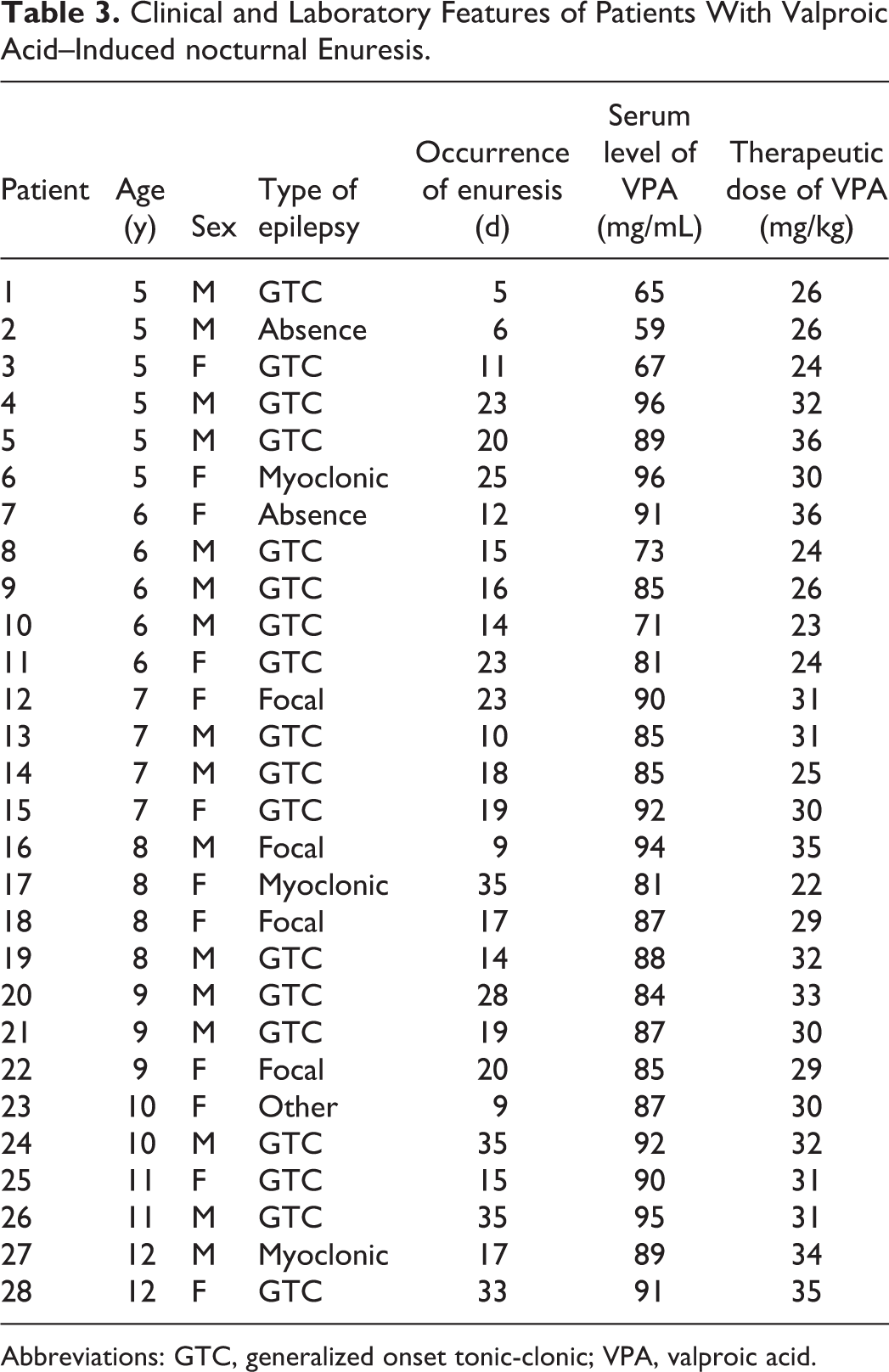
Abbreviations: GTC, generalized onset tonic-clonic; VPA, valproic acid.
Figure 2 demonstrates that the incidence of nocturnal enuresis was mostly affecting children aged 5-8 years old, in 19 children (67.9%), compared with only 9 children (32.1%) who were older than 8 years (P = .004).
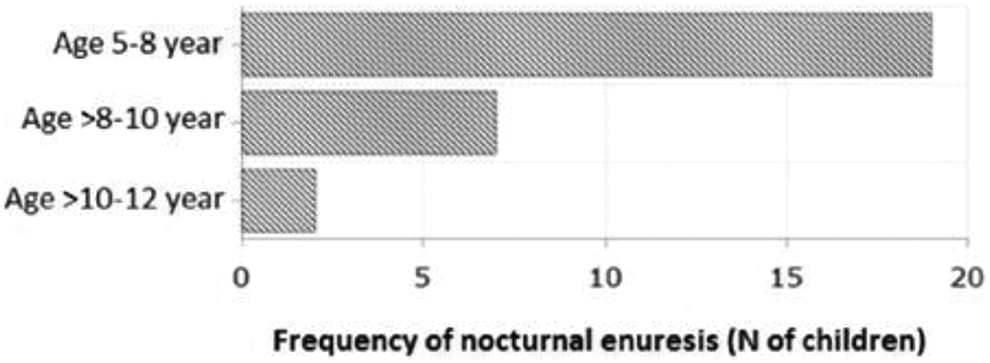
Frequency of secondary nocturnal enuresis according to age group.
Outcome of Enuresis
In 27 children (94%) with secondary nocturnal enuresis, the enuresis was completely resolved in 18 children spontaneously although the children were still on valproic acid therapy, whereas in the remaining 9 children, the enuresis stopped after cessation of the valproate after 19.9 days (median 11, range 9-55).
Polysomnography Results
Twenty-eight children with nocturnal enuresis aged 5-12 years (7.6 ± 2.4 years) were compared with 28 healthy matched children aged 5-12 years (8.3 ± 1.96 years) (Table 4). A comparison between polysomnography findings in nocturnal enuresis patients and controls showed that sleep latency and stage N1 percentage were significantly increased in cases than in controls (P = .001). Although total sleep time, sleep efficiency, rapid eye movement (REM) sleep percentage, and lowest oxygen saturation were significantly reduced in nocturnal enuresis patients than in controls (P = .001, P = .001, P = .001, and P = .02, respectively).
Comparison of Polysomnographic Parameters Between Nocturnal Enuresis Children and Controls.
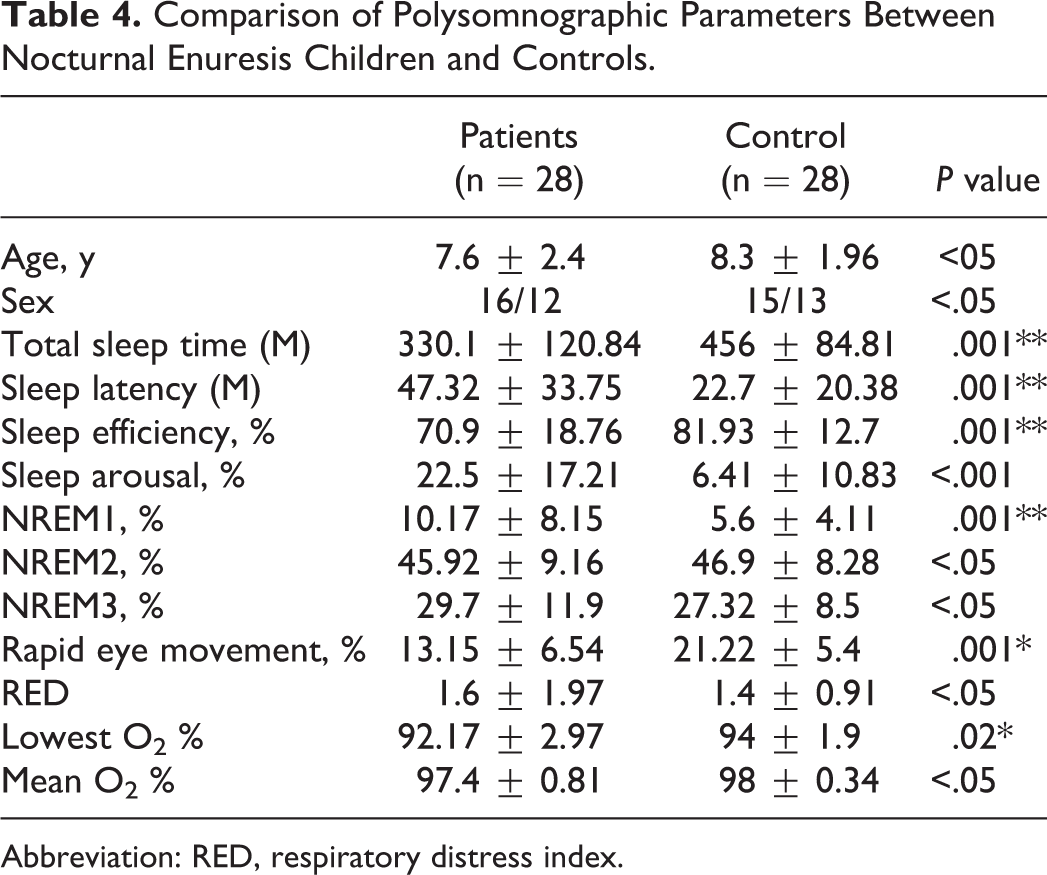
Abbreviation: RED, respiratory distress index.
Also, patients showed a significantly higher number of awakenings during total sleep time (P = .001). In addition, a statistically significant decrease in delta-wave sleep was found in children with nocturnal enuresis as compared with normal children (P = .002).
Correlations Between the Nocturnal Enuresis and Polysomnography
The frequency of nocturnal enuresis was positively correlated with N3% of total sleep period, sleep stage transition index, and snore index (r = 0.69, P ≤ .01; r = 0.72, P ≤ .01; and r = 0.82 P < .005, respectively). Although the frequency of nocturnal enuresis was inversely correlated with the age of the child, N1%, N2%, and REM % of total sleep time (r = –0.85, P ≤ .005; r = –0.81, P ≤ .005; r = –0.71, P ≤ .01; and r = –0.70, P < .01, respectively). But there was no correlation between the frequency of nocturnal enuresis and PLM index (r = 0.33, P = .08) (Table 5).
Correlations Between the Nocturnal Enuresis and Polysomnography.
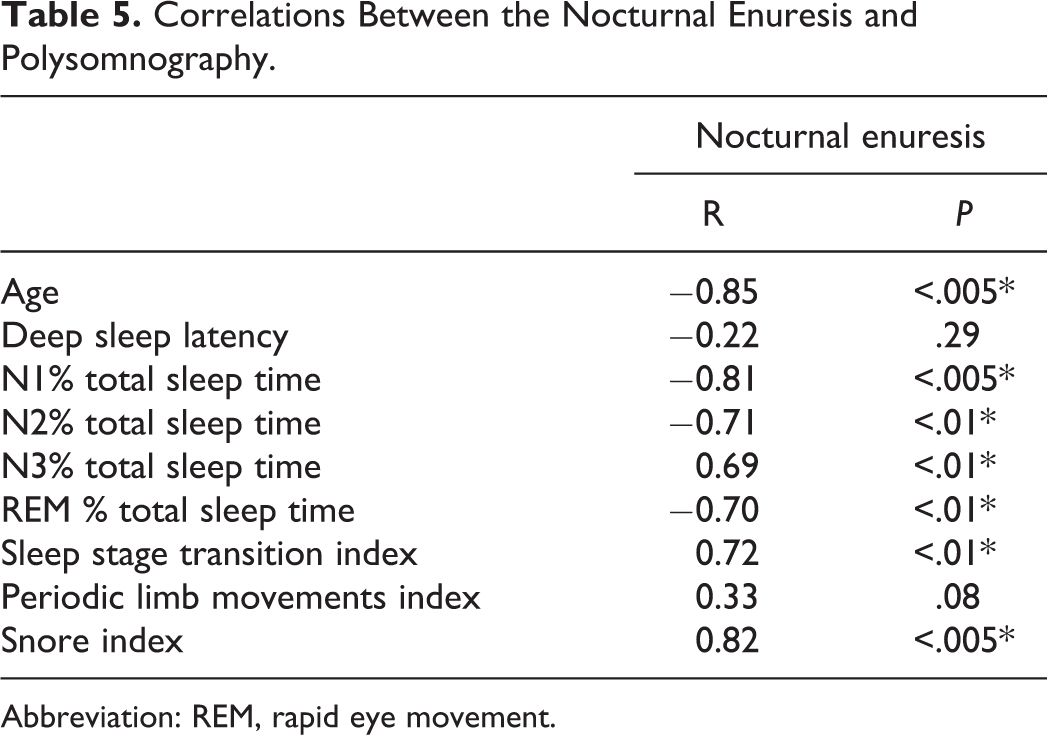
Abbreviation: REM, rapid eye movement.
Comparison Between Nocturnal Enuresis Patients With and Without Elevated Apnea-Hypopnea Index
The respiratory distress index was similar in the nocturnal enuresis and control groups. Different respiratory distress index abnormality cutoff values were previously used, including a cutoff of an apnea index more than 1, 21 obstructive apnea-hypopnea index more than 1.4, 22 and respiratory distress index more than 5. 23 Table 6 shows the polysomnography results using cutoffs of 1 and 5 for apnea-hypopnea index abnormality. Four nocturnal enuresis children had an apnea-hypopnea index more than 5, and those children showed more frequent snoring (P = .005), prolonged latency of sleep (P = .02), prolonged N1% (P = .03), and a significant decrease of sleep efficiency percentage (P = .04) (Table 6).
Polysomnographic Pattern Comparison Between Enuretic Children Regarding Different Apnea-Hypopnea Index Cutoffs.
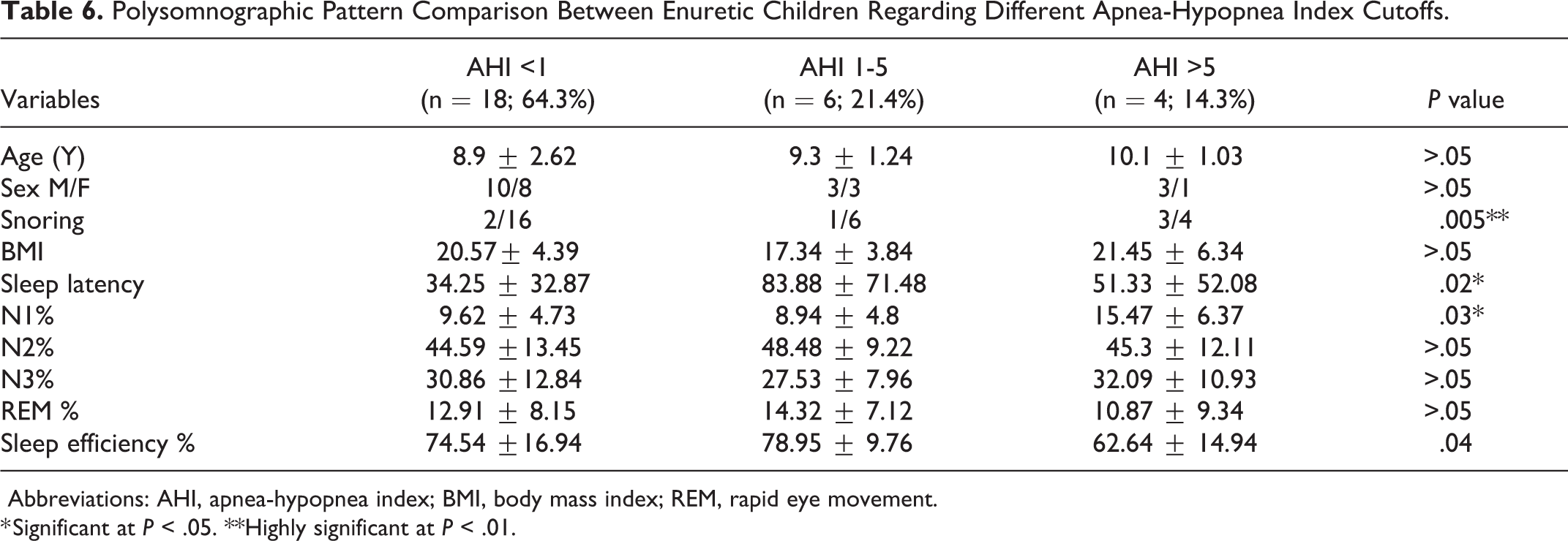
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; REM, rapid eye movement.
* Significant at P < .05. **Highly significant at P < .01.
Prediction of Nocturnal Enuresis Induced by Valproate Therapy in Epileptic Children
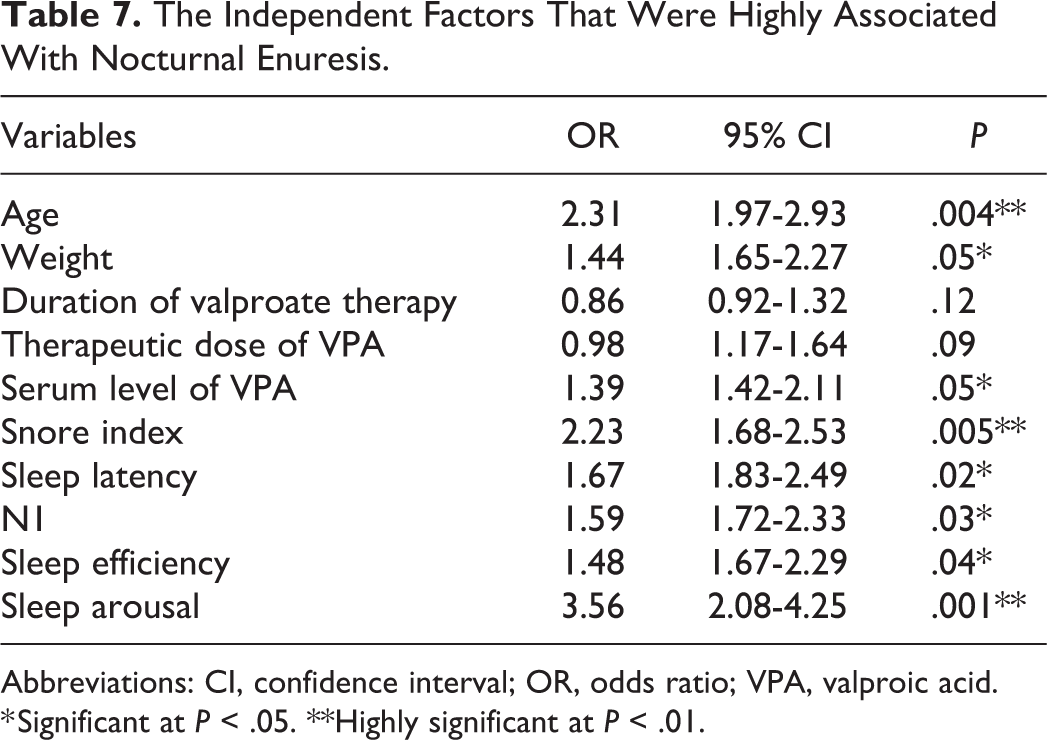
Multivariate logistic regression analysis showed that the independent factors accompanied by nocturnal enuresis were younger age (OR 2. 31, 95% CI = 1.97-2.93, P = .004), followed by weight and serum level of valproic acid (OR 1.44, 95% CI = 1.65-2.27, P = .05, and OR 1.39, 95% CI = 1.42-2.11, P = .05, respectively). Although the therapeutic dose and the treatment duration with valproate were not significantly associated with nocturnal enuresis (OR 0.98, 95% CI = 1.17-1.64, P = .09, and OR 0.86, 95% CI = 0.92-1.32, P = .12, respectively). Regarding polysomnography, the most significant independent factors associated with nocturnal enuresis were sleep arousal and snoring index (OR 3.56, 95% CI = 2.08-4.25, P = .001, and OR 2.23, 95% CI = 1.68-2.53, P = .005, respectively) followed by sleep latency, N1%, and sleep efficiency (OR 1.67, 95% CI = 1.83-2.49, P = .02; OR 1.59, 95% CI = 1.72-2.33, P = .03; and OR 1.48, 95% CI = 1.67-2.29, P = .04, respectively) (Table 7).
The Independent Factors That Were Highly Associated With Nocturnal Enuresis.
Abbreviations: CI, confidence interval; OR, odds ratio; VPA, valproic acid.
* Significant at P < .05. **Highly significant at P < .01.
Discussion
This is a retrospective study planned for deciding the frequency, features, and risk factors accompanied by the occurrence of secondary nocturnal enuresis in epileptic children treated with valproate as a monotherapy.
Side Effects of Valproic Acid
Our results indicated that nocturnal enuresis is a typical side effect in 10.7% of children treated by valproate monotherapy in epileptic children aged 5-15 years. Valproic acid has various side effects, ranging from vomiting to fulminant hepatitis, which can be life-threatening. 24
Children With Enuresis
Enuresis is difficult to differentiate in pediatric patients. It may be normal for age, because of epilepsy, or because of the medication itself. Moreover, the drug-induced nocturnal enuresis may be under-reported by parents or they consider it normal for their child’s age. 25
Previous research studies assessing the side effects of valproic acid found that nocturnal enuresis was a potential reaction to this medication, with a documented frequency of 7% to 24%. 12,26,27 The frequency of nocturnal enuresis in our study was 10.7% (28 patients), which was similar to prior studies. Nocturnal enuresis was reported by the parents in only 12 of the 260 cases (4.6%) in our study; the remaining 16 cases were detected by specifically asking about nocturnal enuresis, because this side effect is usually under-reported by parents.
Onset, Outcome, and Possible Explanations of Nocturnal Enuresis
Our information indicated a causal connection between valproic acid and nocturnal enuresis, as a result of the nearby connection between the start of valproic acid therapy and the beginning of nocturnal enuresis. Furthermore, the presence of a causal connection is strengthened by the cessation of nocturnal enuresis after the stoppage of valproic acid. Likewise, in 2 cases that were reported by Elyasi and Darzi 28 about quetiapine and valproate-induced enuresis, the episodes of urinary incontinence were found to stop 24 hours after decreasing the dose of quetiapine and sodium valproate.
Nocturnal enuresis developed in children after 18.78 ± 8.4 days of the start of valproic acid therapy. This is comparable to 2 published case reports that determined that nocturnal enuresis happened within 14 days of beginning valproate treatment. 27,29
Interestingly, enuresis eventually stopped spontaneously in 18 children despite that the children were still on valproic acid. The reversibility of enuresis while children were still on valproic acid suggested the development of tolerance to this side effect. Ozan et al 30 concluded that the enuresis happened for the most part during the initial 30 days following the start of valproic acid therapy and that it was reversible.
The most notable explanations and mechanisms of nocturnal enuresis include nocturnal polyuria, accompanied disturbances in sleep arousal, 31 valproate may cause changes in renal tubules, 32 limited capacity of the bladder, overactivity of the detrusor muscle, delayed global maturation, and genetics factor. Nocturnal enuresis doubtlessly is a disorder caused by a blend of these etiologies in a multifaceted way. 33,34
Valproic acid–induced nocturnal enuresis is an underreported yet common side effect, especially in children aged between 5 and 8 years, is frequently not spontaneously complained by the parents, and is reversible upon cessation of valproic acid. Clinicians need to know about this side effect, because nocturnal enuresis in epileptic children may indicate an increase in the dose of valproic acid. What is more, nocturnal enuresis can affect children psychologically, including social avoidance, depressed mood, disgrace, loss of self-esteem, and behavioral problems. 35
Polysomnographic Findings in Nocturnal Enuresis
Soster et al 36 demonstrated that children with nocturnal enuresis had elevated arousal thresholds mostly in the first 2 or 3 nights where non-REM was predominant (indicating deep sleep). 37 However, our results differ from those of Bader et al, 38 who reported no differences in depth of sleep between children with nocturnal enuresis and healthy controls. Also, Averous et al 39 reported that abortive REM sleep in the early period of the night may be more in children with nocturnal enuresis compared with normal children. It was also found that in children with nocturnal enuresis, the ratio of REM sleep is lower and REM latency is longer than that of normal children. 40 However, according to Gu et al, there was no significant difference in sleep architecture between children with nocturnal enuresis and healthy controls. 41
In our study, REM sleep percentage was low in children with nocturnal enuresis compared with controls. This polysomnographic finding may be explained by the first-night effect. Also, it may be because the abortive REM sleep episodes in the early part of the night were more common in children with nocturnal enuresis compared with normal control children. 42,43
Relationship of Nocturnal Enuresis and Apnea-Hypopnea Index
The relationship between nocturnal enuresis and sleep-disordered breathing is controversial, and studies reporting both positive and negative associations have been published. 44,45 The respiratory distress index difference was not significant between our nocturnal enuresis patients and controls. Our polysomnography results using cutoffs of 1 and 5 for apnea-hypopnea index abnormality showed that 4 nocturnal enuresis children had an apnea-hypopnea index more than 5, and those children showed more frequent snoring and lighter sleep than the other nocturnal enuresis patients.
Factors Related to Sleep Architecture Accompanied by Nocturnal Enuresis
Finally, the multivariate logistic regression analysis, detected the most significant independent factors related to sleep architecture accompanied by nocturnal enuresis, were sleep arousal and snoring index (OR 3.56, 95% CI 2.08-4.25, P = .001, and OR 2.23, 95% CI 1.68-2.53, P = .005, respectively) followed by sleep latency, N1%, and sleep efficiency (OR 1.67, 95% CI 1.83-2.49, P = .02; OR 1.59, 95% CI 1.72-2.33, P = .03; and OR 1.48, 95% CI 1.67-2.29, P = .04, respectively). Similarly, an updated study of Malthe et al 15 concluded that children with nocturnal enuresis experience more cortical arousals; their sleep may be fragmented and of poor quality. This may lead to changes in the autonomic nervous system and hence hemodynamics, resulting in excess urine production as well as bladder overactivity. Disturbed sleep may also impair the child’s ability to awaken to the sensation of bladder contractions.
Limitations
The main limitation of this study was the small number of children with nocturnal enuresis induced by valproic acid monotherapy and the impact of controlled vs uncontrolled seizures or epileptogenic vs nonepileptogenic EEGs on the presence or absence of nocturnal enuresis need a larger number of cases to be evaluated. Also, there were no previous polysomnography studies of secondary nocturnal enuresis for comparison with our results.
Conclusions
Nocturnal enuresis is a common, mostly reversible, side effect of valproic acid in children. Risk factors for nocturnal enuresis are younger age, higher serum level of valproate, elevated sleep arousal and snoring index, increased sleep latency, decreased percentage of time spent in N1, and decreased sleep efficiency. The underlying mechanism may be related to impaired sleep efficiency, frequent arousals, prolonged sleep latency, snoring, or increased sleep depth that may impair a child’s ability to awaken to the sense of bladder fullness or contractions.
Footnotes
Acknowledgments
The authors thank the study participants and their parents/families, and the additional investigator (Dr Ahmed Hamdy, who participated in neurophysiological studies for the participants).
Author Contributions
AE, ME, HE, MA, and LB designed the study and acquired data. AE, ME, and HE performed data analysis, statistical analysis, drafted the manuscript, and carried out the revisions. MA and LB reviewed the final manuscript and provided insightful advice. All authors gave final approval and agree to all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Research Board (IRB) of Departments of Neurology, Mansoura University, Egypt. Parents of the children who were subjected to the study were told about the study in detail and written informed consent by the parents was taken.