
Abstract
Background:
Metagenomic next-generation sequencing offers an unbiased approach to identifying viral pathogens in cerebrospinal fluid of patients with meningoencephalitis of unknown etiology.
Methods:
In an 11-month case series, we investigated the use of cerebrospinal fluid metagenomic next-generation sequencing to diagnose viral infections among pediatric hospitalized patients presenting with encephalitis or meningoencephalitis of unknown etiology. Cerebrospinal fluid from patients with known enterovirus meningitis were included as positive controls. Cerebrospinal fluid from patients with primary intracranial hypertension were included to serve as controls without known infections.
Results:
Cerebrospinal fluid metagenomic next-generation sequencing was performed for 37 patients. Among 27 patients with encephalitis or meningoencephalitis, 4 were later diagnosed with viral encephalitis, 6 had non–central nervous system infections with central nervous system manifestations, 6 had no positive diagnostic tests, and 11 were found to have a noninfectious diagnosis. Metagenomic next-generation sequencing identified West Nile virus (WNV) in the cerebrospinal fluid of 1 immunocompromised patient. Among the 4 patients with known enterovirus meningitis, metagenomic next-generation sequencing correctly identified enteroviruses and characterized the viral genotype. No viral sequences were detected in the cerebrospinal fluid of patients with primary intracranial hypertension. Metagenomic next-generation sequencing also identified sequences of nonpathogenic torque Teno virus in cerebrospinal fluid specimens from 13 patients.
Conclusions:
Our results showed viral detection by cerebrospinal fluid metagenomic next-generation sequencing only in 1 immunocompromised patient and did not offer a diagnostic advantage over conventional testing. Viral phylogenetic characterization by metagenomic next-generation sequencing could be used in epidemiologic investigations of some viral pathogens, such as enteroviruses. The finding of torque Teno viruses in cerebrospinal fluid by metagenomic next-generation sequencing is of unknown significance but may merit further exploration for a possible association with noninfectious central nervous system disorders.
Keywords
Meningoencephalitis is a devastating disease of the central nervous system which carries the potential for high morbidity and mortality. The differential diagnosis for patients presenting with meningoencephalitis is broad and includes both infectious and noninfectious etiologies. Central nervous system infections can be caused by viruses, bacteria, fungi, parasites, and amoebae.
1,2
Noninfectious conditions among pediatric patients can include acute demyelinating encephalomyelitis, anti–myelin oligodendrocyte glycoprotein (anti-MOG), anti–N-methyl-
Metagenomic next-generation sequencing may offer a broader, more comprehensive and unbiased approach to viral identification. In this method, nucleic acids are isolated from the cerebrospinal fluid and massively sequenced, followed by bioinformatic alignment of sequences to those of known viruses. This method permits identification of viral DNA or RNA irrespective of immunocompromised status, pathogen-specific test availability, or clinical suspicion. Metagenomic next-generation sequencing has been successfully used to identify central nervous system viruses and other pathogens that were not detected by clinical diagnostic testing. 20,21 However, next-generation sequencing is currently expensive, labor intensive, and its performance characteristics in the context of false positivity or false negativity rates are not well established. The clinical application of this new methodology continues to be further complicated by identification of viral sequences of unknown clinical significance. 22 Variations in the sequencing and bioinformatic methods among different investigator groups also limits the ability to compare results across different platforms. However, these impediments can be optimized for future clinical applicability. The aim of this case series was to examine the use of cerebrospinal fluid metagenomic next-generation sequencing to diagnose potential viral etiologies in pediatric patients presenting with symptoms consistent with infectious meningoencephalitis but with negative initial cerebrospinal fluid diagnostic testing.
Methods
Patient Inclusions
Charts of patients admitted to the general pediatric, infectious diseases, neurology, or intensive care units at Nationwide Children’s Hospital, Columbus, OH, between February 1, 2017, and December 31, 2017, were reviewed by the authors (GE, SA, MS) for the admitting diagnoses of meningitis, meningoencephalitis, encephalitis, seizure, headache with fever, or altered mental status. Inclusion criteria consisted of patients aged 18 years or younger, who had undergone diagnostic lumbar puncture, and for whom sufficient remaining cerebrospinal fluid (at least 200 µL) was available. Patients were excluded if a cerebrospinal fluid test identified a nonviral infectious etiology during the hospitalization. Informed consent was obtained from patients who were hospitalized at the time of enrollment; for patients who had been discharged, cerebrospinal fluid was released from the clinical laboratory at day 7 as a remnant specimen. Records of enrolled patients were reviewed for demographic data, clinical diagnoses, laboratory and imaging results, and final diagnosis. In addition to this group, a second group of patients with positive cerebrospinal fluid PCR testing for enterovirus were included if they had sufficient cerebrospinal fluid remaining in the clinical laboratory. A third group of patients were included who had no known infection and were undergoing therapeutic lumbar puncture for primary intracranial hypertension. The patients in group 1 (pediatric encephalitis or meningoencephalitis) constituted the study group; group 2 (enterovirus meningitis) and group 3 (primary intracranial hypertension) served as known-infection or no-infection controls, respectively.
Cerebrospinal Fluid Metagenomic Next-Generation Sequencing Analysis and Validation 23
See online Supplemental Methods.
Statistical Analysis
Patient characteristics were described for each group. Categorical variables were expressed as absolute numbers and percentage compared either to the total group or the total number of performed tests (magnetic resonance imaging [MRI], electroencephalography [EEG]). Continuous variables were expressed using either means and standard deviations, or median values and ranges. The Student t test, one-way analysis of variance, or Kruskal-Wallis test with Tukey’s multiple comparison test were used to compare grouped data using Prism 8 software (GraphPad, San Diego, CA), accepting significance at P <.05.
Results
Patient Characteristics
Thirty-seven patients met inclusion criteria, 27 in group 1, 4 in group 2, and 6 in group 3. Patient characteristics are summarized in Table 1. Group 1 patients had a broad age range (median 6 years, range 27 days–16 years), whereas most patients in group 2 were infants (median age 8 weeks) and group 3 patients were generally older (median age 9 years). All patients in group 1 had clinical symptoms and/or signs consistent with encephalitis or meningoencephalitis, often with supportive neuroimaging and EEG findings, whereas group 2 patients had fever without neurologic signs and group 3 patients lacked fever or encephalitis symptoms. Cerebrospinal fluid white blood cell (WBC) counts were higher in groups 1 and 2 compared with group 3, and glucose was lower in group 2. Cerebrospinal fluid red blood cell (RBC) counts and protein were statistically similar among the 3 groups.
Patient Demographics and Laboratory Results.
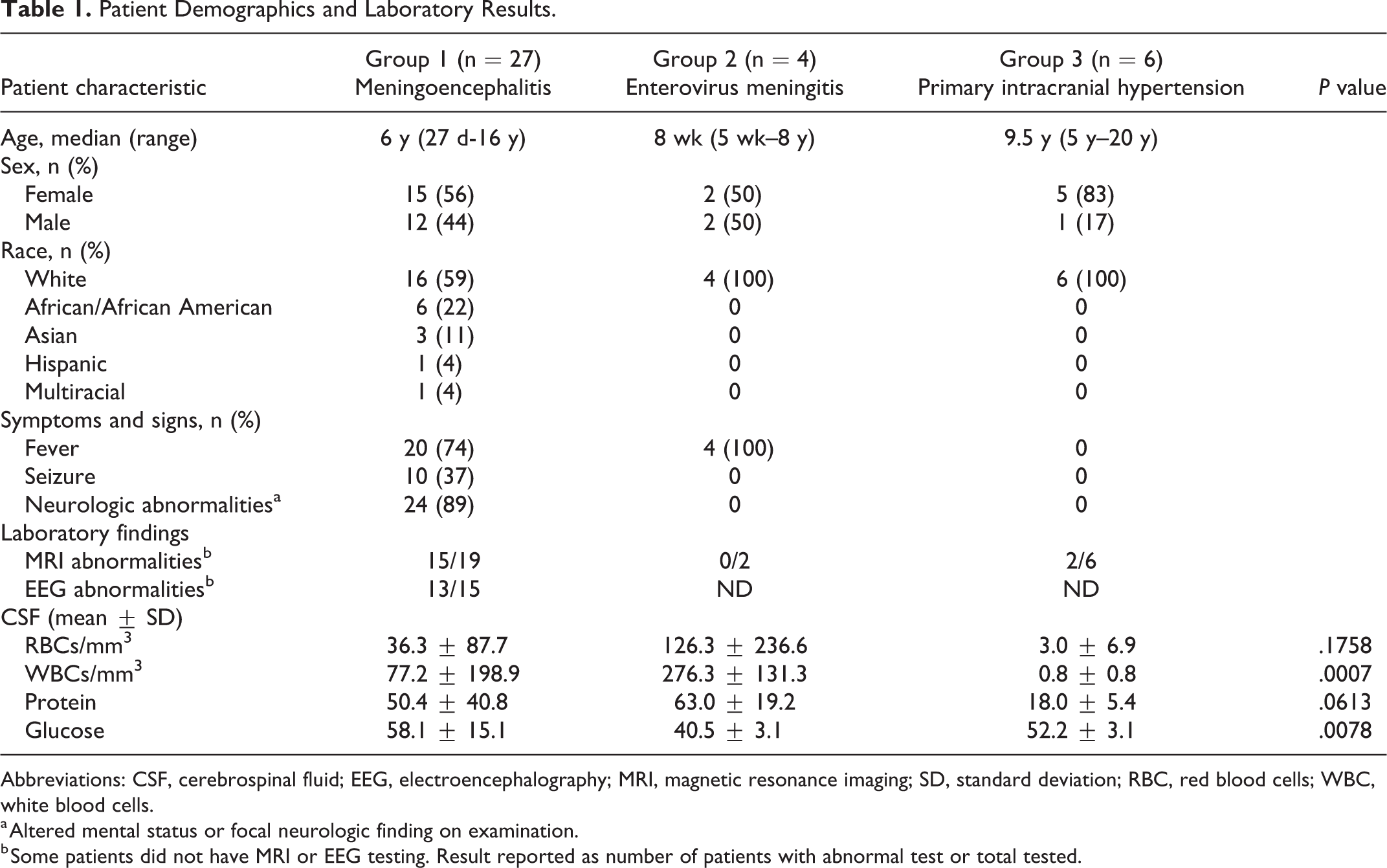
Abbreviations: CSF, cerebrospinal fluid; EEG, electroencephalography; MRI, magnetic resonance imaging; SD, standard deviation; RBC, red blood cells; WBC, white blood cells.
a Altered mental status or focal neurologic finding on examination.
b Some patients did not have MRI or EEG testing. Result reported as number of patients with abnormal test or total tested.
Metagenomic Next-Generation Sequencing for Viral Pathogen Detection in Cerebrospinal Fluid
Thirty-seven individual cerebrospinal fluid samples were analyzed by metagenomic next-generation sequencing (Table 2). After chart review, the 27 patients in group 1 were classified according to final clinical diagnosis: (1) proven viral encephalitis (n = 4); (2) probable para- or post-infectious central nervous system syndromes (n = 6); (3) no etiology identified by clinical testing (n = 6); and (4) proven noninfectious etiology (n = 11). Of the 4 patients with proven viral encephalitis, 3 had California encephalitis and 1 patient had West Nile virus encephalitis, diagnosed by blood serology. For the West Nile virus case, clinical cerebrospinal fluid PCR testing was negative (Arup Laboratories, Salt Lake City, UT). Cerebrospinal fluid sent to the Centers for Disease Control and Prevention (CDC) for research use–only testing resulted weeks later as PCR positive. Among these patients, cerebrospinal fluid metagenomic next-generation sequencing identified West Nile virus (181 unique viral nucleic acid sequences, or “reads”) but not California virus. The patient with metagenomic next-generation sequencing West Nile virus detection was immunocompromised (kidney transplant recipient), whereas the patients with California encephalitis were otherwise healthy. Among the 6 patients with probable para- or postinfectious central nervous system syndromes, 2 patients had positive testing for mycoplasma and 4 had positive multiplex viral PCR results from nasopharyngeal swabs (3 parainfluenza viruses, 1 rhinovirus/enterovirus). For all of these patients, clinical cerebrospinal fluid PCR testing was negative for the pathogens found in the nasopharynx. For the 6 patients with negative clinical diagnostic testing, 1 patient had fever, headache, and cerebrospinal fluid pleocytosis, and 5 had fever and altered mental status; among these patients, cerebrospinal fluid metagenomic next-generation sequencing did not detect viral pathogens. For the remaining 11 patients, a noninfectious etiology was later identified: glioma/gliomatosis cerebri (n = 2), Guillain-Barre syndrome (GBS, n = 3), optic neuritis (n = 1), acute demyelinating encephalomyelitis (acute disseminated encephalomyelitis [ADEM], n = 1), anti-MOG encephalitis (n = 2), and Kawasaki disease with encephalopathy (n = 2). Cerebrospinal fluid metagenomic next-generation sequencing was negative for viral pathogens among all patients with noninfectious central nervous system syndromes.
Cerebrospinal fluid Metagenomic Next-Generation Sequencing by Patient Diagnosis.
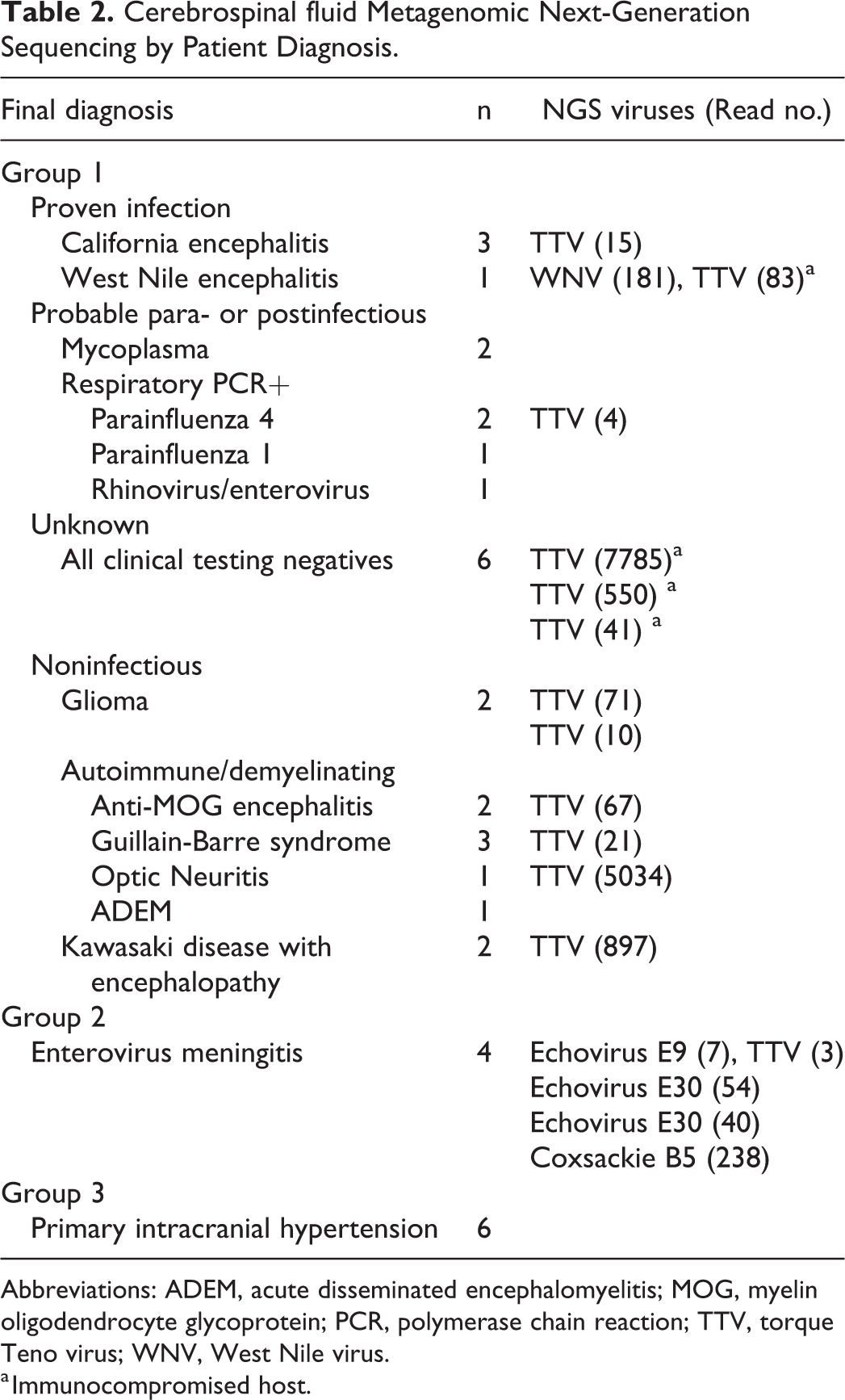
Abbreviations: ADEM, acute disseminated encephalomyelitis; MOG, myelin oligodendrocyte glycoprotein; PCR, polymerase chain reaction; TTV, torque Teno virus; WNV, West Nile virus.
a Immunocompromised host.
Group 2 consisted of 4 patients with enterovirus meningitis identified by clinical cerebrospinal fluid PCR testing. For all 4 patients, cerebrospinal fluid metagenomic next-generation sequencing was positive for enteroviruses (Table 2). Viral reads mapped to the following enterovirus genotypes: Echovirus E9, Echovirus E30 (n = 2), and Coxsackie B5.
For group 3, 6 patients undergoing therapeutic lumbar puncture for primary intracranial hypertension, without known infectious conditions, were included in the study to determine whether viral sequences would be detected in the cerebrospinal fluid of individuals without clinically suspected infections. Metagenomic next-generation sequencing did not identify any viral pathogen reads in the cerebrospinal fluid from any of these patients.
Taken together, this cerebrospinal fluid metagenomic next-generation sequencing assay overall did not detect viral pathogens that would have been missed by clinical diagnostic testing. West Nile virus was detected in the cerebrospinal fluid of one immunocompromised patient by metagenomic next-generation sequencing, which required confirmation using a proprietary test at the CDC and was missed by clinically available PCR testing. Conversely, metagenomic next-generation sequencing did not detect pathogenic viruses among patients who had noninfectious conditions and did correctly identify enterovirus genotypes among patients with known viral meningitis.
Identification of Torque Teno Virus in Cerebrospinal Fluid by Metagenomic Next-Generation Sequencing
Unexpectedly, reads mapping to torque Teno virus were found in 13 of the 37 cerebrospinal fluid specimens (35%) (Table 2) and was confirmed in all specimens by qualitative PCR using pan–torque Teno virus primers. Torque Teno viruses are ubiquitous in the blood of immunocompetent individuals, and higher viral loads have been associated with immunocompromised status, so clinical records were reviewed for immunocompromising conditions. 23 -25 Four of the patients were known to be immunocompromised: 1 patient had a kidney transplant, 2 had undergone allogeneic bone marrow transplant, and 1 had an autologous bone marrow transplant and was receiving chemotherapy for medulloblastoma. Among the patients without known immunocompromising conditions, 3 had known or suspected viral infections: one had California encephalitis, one had parainfluenza respiratory infection, and one had enterovirus meningitis. In addition, 5 patients with torque Teno virus–positive cerebrospinal fluid metagenomic next-generation sequencing were later found to have noninfectious central nervous system conditions: 2 had gliomas, 1 each had Guillain-Barre syndrome, optic neuritis, and anti-MOG encephalitis. The number of torque Teno virus reads in the cerebrospinal fluid of immunocompromised patients was statistically similar to reads detected among non-immunocompromised patients (mean ± SD, 2115 ± 3787 vs 680 ± 1658 reads, P = .1483) (Figure 1, A). Among the 24 patients who did not have torque Teno virus detected in cerebrospinal fluid, only 1 was immunocompromised (Crohn disease receiving infliximab and methotrexate). None of the patients with primary intracranial hypertension (group 3) had torque Teno virus sequences detected by cerebrospinal fluid metagenomic next-generation sequencing.
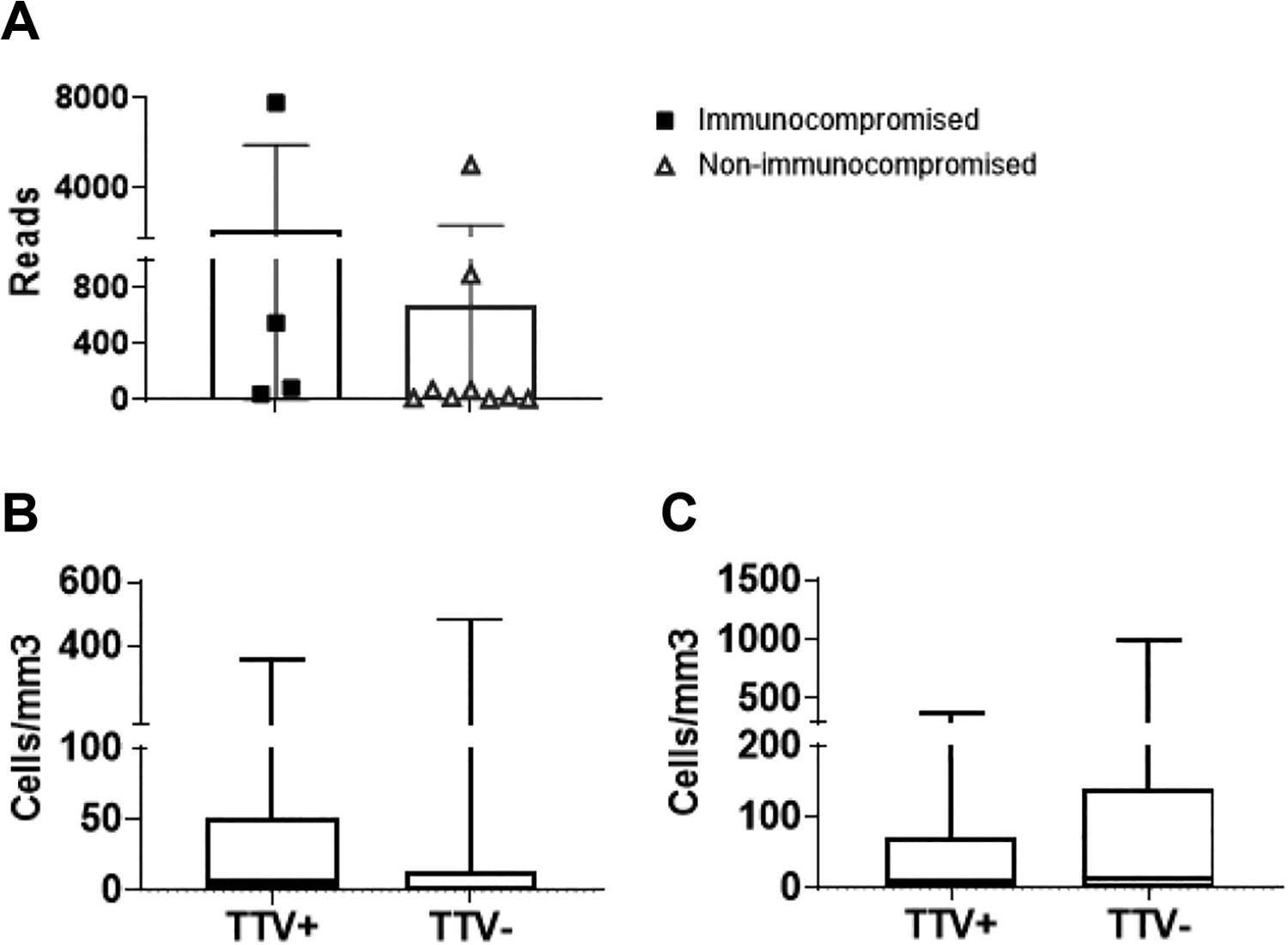
Cerebrospinal fluid characteristics according to TTV detection. (A) Among patients who had TTV sequences identified in cerebrospinal fluid samples, the cerebrospinal fluid TTV read numbers were compared between patients with known immunocompromising conditions (kidney or hematopoietic cell transplant) and those without known immunocompromise. (B, C) Cerebrospinal fluid red blood cell counts (B) and white blood cell counts (C) were compared between patients with (+) or without (–) TTV detected by cerebrospinal fluid metagenomic next-generation sequencing. TTV, torque Teno virus.
Because torque Teno viruses are commonly detected in blood as well as peripheral blood mononuclear cells, it is possible that torque Teno virus reads in the cerebrospinal fluid were secondary to blood contamination during lumbar puncture. 26,27 To examine this, cerebrospinal fluid RBC and WBC indices were compared between patients with or without torque Teno virus detection (Figure 1, B and C). The cerebrospinal fluid RBCs (mean ± SD) for torque Teno virus–positive patients was 65 ± 120 cells/mm3, compared with 29 ± 100 cells/mm3 for torque Teno virus–negative patients (P = .3450). The cerebrospinal fluid WBCs (mean ± SD) were 54 ± 105 vs 108 ± 224 cells/mm3 for torque Teno virus–positive and torque Teno virus–negative patients respectively and did not reach statistical significance (P = .4242). However, given the number of patients in each group, a Type II error could account for these statistical results.
Discussion
The etiology of encephalitis is identified in less than half of cases, exposing the well-recognized inadequacies of current diagnostic options. 28 Metagenomic analysis using next-generation sequencing is a new approach that could potentially overcome the limitations of targeted diagnostic methods. 19,22 The purpose of this study was to determine whether metagenomic next-generation sequencing could identify viral pathogens for pediatric patients with undiagnosed meningoencephalitis. Of the 27 patients in our group 1, only 1 had a viral pathogen identified by metagenomic next-generation sequencing that was not identified by other techniques. In this case, West Nile virus was identified in the cerebrospinal fluid of one renal transplant patient. In contrast to West Nile virus, next-generation sequencing did not detect California virus sequences in the cerebrospinal fluid of several immunocompetent patients. Conventional PCR does not reliably detect California virus in the cerebrospinal fluid and is not clinically available as a diagnostic test. This lack of detection is thought to be due to low viral RNA quantities in the cerebrospinal fluid. 29 Our results are similar to another cerebrospinal fluid metagenomic next-generation sequencing study that reported lack of California virus detection by cerebrospinal fluid metagenomic next-generation sequencing among serologically proven cases, suggesting that metagenomic next-generation sequencing may not be clinically useful for diagnosis of California virus encephalitis. 30 Similarly, we and other groups were not able to identify causative viral agents for most patients presenting with acute encephalitis, demonstrating no advantage of cerebrospinal fluid metagenomic next-generation sequencing in distinguishing infectious from noninfectious etiologies of meningoencephalitis among immunocompetent patients at the onset of their central nervous system symptoms. 19,22,30
As performance characteristics of metagenomic next-generation sequencing are not well described, patients with known enterovirus meningitis were evaluated by metagenomic next-generation sequencing, which correctly identified enterovirus sequences for all cases and enabled classification of echovirus and coxsackie virus genotypes for each patient. Thus, metagenomic next-generation sequencing could potentially be used for phylogenetic characterization of outbreaks and overall epidemiology of central nervous system viral infections. 28,31 Cerebrospinal fluid specimens from patients without infection (group 3, primary intracranial hypertension) were included to address the known problem of identifying nucleic acids from environmental contaminants by metagenomic next-generation sequencing. In this study, no viral reads were identified among the primary intracranial hypertension patients, supporting the specificity of our metagenomic next-generation sequencing pipeline.
Unexpectedly, torque Teno viruses were identified by metagenomic next-generation sequencing in approximately one-third of the cerebrospinal fluid samples. The torque Teno virus family of viruses are nonpathogenic commensal viruses with a seroprevalence greater than 90% in some populations. 32 -35 Blood torque Teno virus viral loads are higher among immunosuppressed individuals and have been proposed to serve as a potential marker of over-immunosuppression among transplant recipients. Compared to blood viral loads, torque Teno virus detection in cerebrospinal fluid has not been well characterized. In separate reports, torque Teno viruses were not detected by metagenomic next-generation sequencing among 18 immunocompetent pediatric patients with encephalitis, whereas torque Teno virus reads were found in 11 cerebrospinal fluid samples (31.4%) among 35 bone marrow transplant patients. In our small group of 5 immunocompromised patients, the 80% torque Teno virus positivity is higher than other published studies and suggests the need for prospective studies to define cerebrospinal fluid torque Teno virus prevalence and correlation with blood torque Teno virus PCR results in immunocompromised hosts.
In this study, almost half (46%) of the patients with torque Teno virus detection in the cerebrospinal fluid had noninfectious central nervous system conditions, including central nervous system malignancies, autoimmune encephalitis, and demyelinating conditions. This finding is consistent with that of Sospedra et al, 36 who found torque Teno virus sequences in brain tissue from 5 of 11 patients with multiple sclerosis and 32 of 41 brain tumors, suggesting the possibility that torque Teno viruses may be associated with immune dysregulated conditions of the central nervous system. Several groups have examined cerebrospinal fluid torque Teno virus using conventional PCR among patients with noninfectious central nervous system conditions, in which torque Teno viruses were identified in the cerebrospinal fluid of some patient groups (multiple sclerosis) but not others (acute lymphocytic leukemia). 37 The significance of torque Teno virus in the cerebrospinal fluid of patients with noninfectious central nervous system disorders is unknown and may benefit from further study among larger populations.
Limitations of this study include lack of comparative performance characteristics between our metagenomic next-generation sequencing methods and those of other investigators. Larger patient populations will be needed to validate this approach and to establish the limits of pathogen detection. In our patient group, viral pathogens were only identified in the cerebrospinal fluid from patients that were already clinically suspected or identified by clinical testing, so the utility of next-generation sequencing as a clinical diagnostic test is not currently supported. Turn-around time is another potential limitation of the metagenomic next-generation sequencing methodology. Currently, commercial laboratories perform diagnostic metagenomic next-generation sequencing of blood and other clinical specimens with a turn-around time ranging from 2 days up to 2 weeks, supporting the possibility that cerebrospinal fluid metagenomic next-generation sequencing could be performed in a clinically actionable time frame in the future. For this exploratory study, there is potential risk of selection bias, as patients were identified through referral to the infectious disease clinical team at our hospital and who had sufficient remnant cerebrospinal fluid in the lab for next-generation sequencing testing.
Metagenomic next-generation sequencing could be used in diagnosis of viral pathogens in acute meningoencephalitis, though its performance characteristics are still unproven, current turnaround time is still not in a clinically actionable time frame, and for patients in this study did not offer a diagnostic advantage over clinically available testing. In addition, arboviruses were not be detected in this study by cerebrospinal fluid metagenomic next-generation sequencing. The findings in this study also suggest the possible use of next-generation sequencing for epidemiologic investigations and phylogenetic analysis of viral pathogens. The detection of torque Teno viruses in the cerebrospinal fluid was unexpected, and although currently of unknown significance, torque Teno viruses in the cerebrospinal fluid may also deserve further investigation.
Supplemental Material
2020-9-2_JCN_revised_supplemental_methods - Cerebrospinal Fluid Analysis for Viruses by Metagenomic Next-Generation Sequencing in Pediatric Encephalitis: Not Yet Ready for Prime Time?
2020-9-2_JCN_revised_supplemental_methods for Cerebrospinal Fluid Analysis for Viruses by Metagenomic Next-Generation Sequencing in Pediatric Encephalitis: Not Yet Ready for Prime Time? by Guliz Erdem, Irina Kaptsan, Himanshu Sharma, Arvind Kumar, Shawn C. Aylward, Amit Kapoor and Masako Shimamura in Journal of Child Neurology
Footnotes
Acknowledgments
We acknowledge Debabrata Ghosh, MD, for valuable discussions regarding study design. We thank the pediatric infectious diseases and neurology specialists at Nationwide Children’s Hospital for assisting with case identification.
Author Contributions
GE and MS equally contributed to this work, they designed the study, analyzed data, and wrote the manuscript; IK, HS, AK, SA, AK contributed to study design, analyzed data, and helped write the manuscript, HS, AK, AK and IK performed experiments, provided data, and edited manuscript. All authors contributed intellectually and reviewed and revised the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Nationwide Children’s Hospital Wexner Research Center Infectious Diseases Consortium Intramural Award mechanism.
Supplemental Material
Supplemental material for this article is available online.
Ethical Approval
The study was approved by the Nationwide Children’s Hospital Institutional Review Board (IRB16-01240).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.