
Abstract
Background:
Acute necrotizing encephalopathy (ANE) is a rare condition associated with rapid progression to coma and high incidence of morbidity and mortality.
Methods:
Clinical, electroencephalographic (EEG), and brain magnetic resonance imaging (MRI) characteristics and immunomodulatory therapy timing were retrospectively analyzed in children with ANE. ANE severity scores (ANE-SS) and MRI scores were also assessed. The associations of patient characteristics with 6-month modified Rankin scale (mRS) and length of hospitalization were determined using either univariate linear regression or one-way analysis of variance.
Results:
7 children were retrospectively evaluated. Normal EEG sleep spindles (P = .024) and early treatment (R 2 = .57, P = .030) were associated with improved outcomes (ie, decreased mRS). Higher ANE-SS (R 2 = .79, P = .011), higher age (R 2 = .62, P = .038), and presence of brainstem lesions (P = .015) were associated with longer length of hospitalization. Other patient characteristics were not significantly associated with mRS or length of hospitalization.
Conclusion:
Early immunomodulatory therapy and normal sleep spindles are associated with better functional outcome in children with ANE.
Acute necrotizing encephalopathy (ANE) is a rare condition characterized by severe and acute brain injury that usually follows acute febrile, often virus-induced, illness. 1 Viral symptoms (eg, fever, cough, gastroenteritis) are followed by rapid deterioration to seizures, altered consciousness, and liver dysfunction. 1-2 ANE can be sporadic or familial, with most known familial cases caused by mutations in the RANBP2 gene and classified as ‘infection-induced acute encephalopathy 3 (IIAE3; OMIM 608033). 2 -4 There are no consensus guidelines for acute or chronic management of ANE, although some studies suggest that early immunomodulatory treatment may be associated with favorable outcomes. 5-6
Brain magnetic resonance imaging (MRI) in patients with ANE characteristically feature bilateral symmetric thalamic involvement and can be accompanied by brainstem tegmentum, periventricular white matter, putaminal, and cerebellar lesions. 7 -9 Clinical course and prognosis of ANE patients range from full neurologic recovery to coma and death. Progression to coma can ensue within 24 hours of symptom onset, with high mortality rates seen in 1/3 of patients. Surviving patients are often left with neurologic disabilities, including focal weakness, extra-ocular abnormalities, dystonia and/or spasticity, or ataxia related to the sites of brain involvement. 10 -12 Favorable long-term neurologic outcomes have been associated with normal cerebrospinal fluid protein levels in the acute phase and a lack of brainstem lesions on initial neuroimaging. 8,12 To date, there is a paucity of literature relating timing of treatment to outcome in ANE, and no literature associating outcomes with electroencephalographic (EEG) or MRI thalamic volumetric biomarkers.
The authors’ goal was to explore associations of clinical interventions, thalamic volumetric measurements, and EEG characteristics to outcomes in children with ANE. The authors hypothesized that early treatment, normal EEG sleep features, and absence of epileptiform abnormalities would be associated with improved outcomes in children after initial presentation of ANE. The authors also hypothesized that increased thalamic volumes at presentation would be associated with worse outcomes.
Methods
Patient Population
Children who were admitted to Phoenix Children’s Hospital between January 2011 and January 2020 with a diagnosis of ANE were retrospectively analyzed. This study was performed under approval of the Phoenix Children’s Hospital Institutional Review Board (No: 20-040). Modified Rankin Scale (mRS) 13 at 6 months post-injury was the primary outcome. mRS measures the degree of disability on a 0-6 scale with 0 representing no symptoms and 6 representing death. The secondary outcome measure was length of hospitalization, measured in days. Additional collected data included age, sex, race, genetic results, virus detected at presentation, initial laboratory values on admission (platelet count, aspartate transaminase, alanine transaminase, cerebral spinal fluid white blood count, and cerebrospinal fluid protein level), presence of shock or fever upon admission, and presence of epilepsy at 6-months post-injury. The authors also investigated type and timing of treatment for ANE, which included intravenous Solumedrol, intravenous immunoglobulins, and intravenous Tocilizumab. The ANE severity score (ANE-SS) was calculated 11 as a measure of predicted prognosis based on presenting clinical findings. ANE-SS ranges from 0 to 9, with 3 points for existence of shock, 2 points for brainstem lesions, 2 points for age over 48 months, 1 point for platelet count platelet count below 100 000/µL, and 1 point for cerebrospinal fluid protein value >60 mg/dL. The authors limited their review to initial presentation of ANE for unique patients, and did not include data from recurrent presentations for any patient.
Electroencephalography
Continuous and routine EEG was captured using institutional standard clinical hardware (Xltek®; Natus Medical, Pleasanton CA) under the International 10-20 system with a sampling rate of 512 Hz, low frequency filter of 1 Hz and high frequency filter at 70 Hz. All patients underwent continuous EEG upon presentation for the initial 48 hours of monitoring and had subsequent routine EEG studies performed as part of their inpatient hospitalization. All recordings were independently reviewed by 2 board certified epileptologists (BA, JF) for the presence of normal sleep spindles (symmetric and asynchronous under 2 years of age, symmetric and synchronous after 2 years of age) and epileptiform abnormalities (interictal epileptiform discharges or seizures) during inpatient EEG recordings. Consensus was obtained by both epileptologists without discrepancy in interpretation.
Magnetic Resonance Imaging
MRI abnormalities were identified in the T2/fluid-attenuated inversion recovery sequences within the thalamus, brainstem, white matter involvement in the cerebellum and cerebrum, and the presence of intracranial cavitation or hemorrhage. From these findings, the authors calculated the ANE MRI score based on previously described methods 8 (using “calculation A” accounting for both brainstem and white matter involvement). Thalamic volumetric measurements were calculated from the 3D T1-weighted and fluid-attenuated inversion recovery imaging sequences using FreeSurfer software (version 6.0). 14-15 The normalized thalamic volume was computed as 10 000 * total thalamic volume / estimated total intracranial volume.
Statistics
The authors investigated relationships between outcomes (mRS and length of hospitalization) and patient laboratory values on admission, age, normalized thalamic volume, sex, ANE-SS, ANE MRI Score, time to treatment, as well as the presence of fever, shock, age appropriate sleep spindles, and interictal epileptiform discharges. For statistical purposes, the authors scored 6 for a single patient who did not receive immunomodulatory treatment, which represented the length (in days) of hospitalization before the patient died. Statistical analysis was completed using either univariate linear regression or one-way analysis of variance, as appropriate to the variable type. Statistical analyses were performed using R studio version 3.4.1.
Results
Population
The authors evaluated 7 unique children with ANE hospitalized for acute neurologic deterioration (Table 1). Ages ranged from 10 months to 14 years (0.9 ± 1.6 years [median ± interquartile range]). 4/7 patients were female (57.1%). All patients presented with seizures, fever and had bilateral thalamic lesions on Brain MRI. 1/7 patients (Patient 2, 14.3%) presented with shock. 6/7 patients were treated with immunomodulatory therapy (85.7%), including intravenous Solumedrol, intravenous immunoglobulin and intravenous Tocilizumab within 0-5 days of presentation (Table 1). The child (Patient 1) who did not receive immunotherapy died on day 6 of acute hospitalization. Length of hospitalization ranged from 6-69 days (12.0 ± 32 days). ANE-SS ranged from 0-7 (2.0 ± 2.5). MRI severity scores ranged from 1-4 (2.0 ± 1.0). 6-month mRS ranged from 0 to 6 (5.0 ± 2). 4/6 surviving patients (66.7%) developed epilepsy. All patients underwent DNA sequence analysis for RANBP2 mutations, all returning normal. Influenza A was detected in 2/7 patients (28.6%), influenza B was detected in 2/7 patients (28.6%), and rhinovirus, cytomegalovirus, and parainfluenza 3 were each separately detected in 1/7 patients (14.3%). 1/7 patients (Patient 6) later had ANE recurrence prompting readmission 1 year after initial injury. 2/7 patients (Patients 1 and 3) were siblings.
Patient Information.
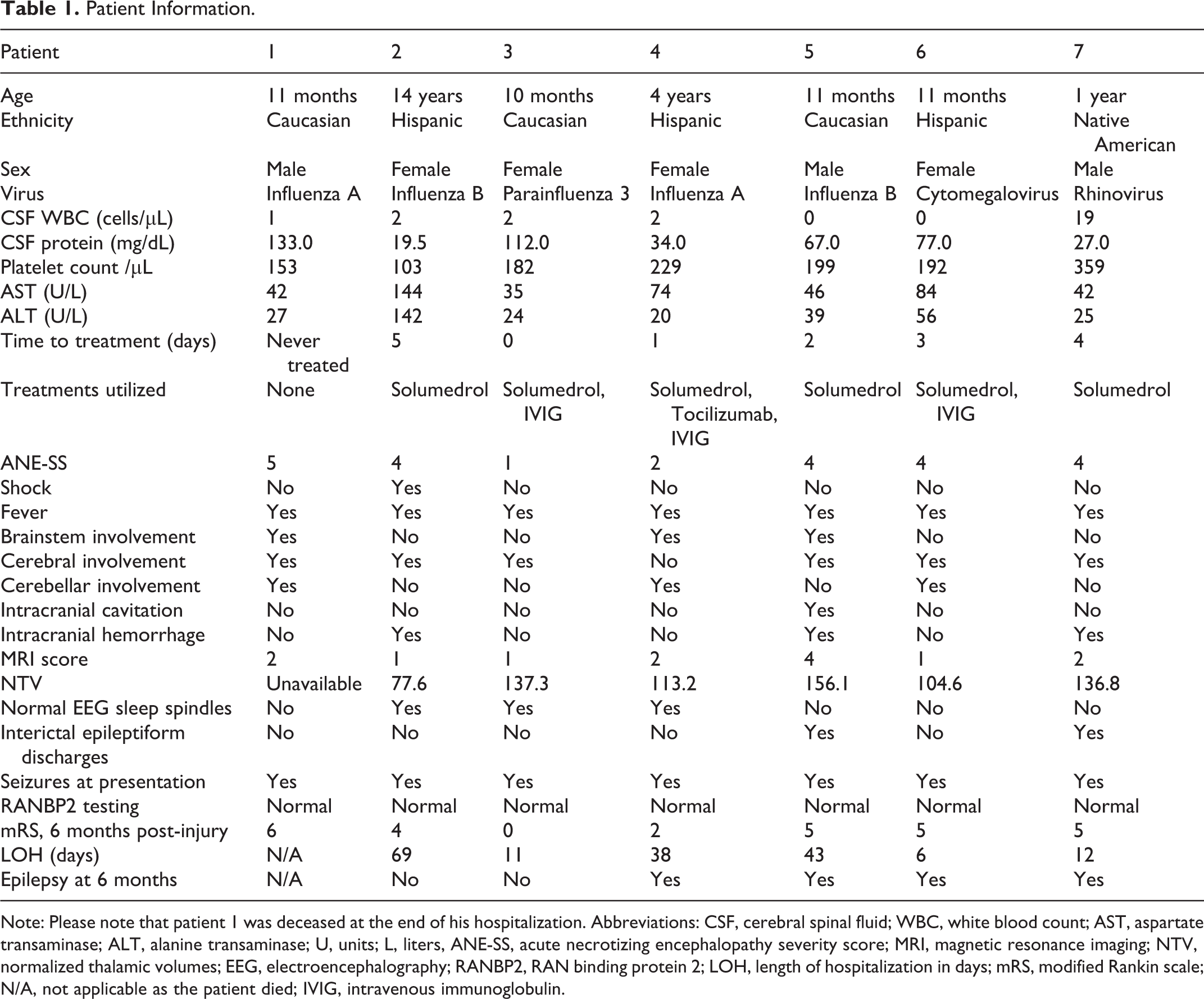
Note: Please note that patient 1 was deceased at the end of his hospitalization. Abbreviations: CSF, cerebral spinal fluid; WBC, white blood count; AST, aspartate transaminase; ALT, alanine transaminase; U, units; L, liters, ANE-SS, acute necrotizing encephalopathy severity score; MRI, magnetic resonance imaging; NTV, normalized thalamic volumes; EEG, electroencephalography; RANBP2, RAN binding protein 2; LOH, length of hospitalization in days; mRS, modified Rankin scale; N/A, not applicable as the patient died; IVIG, intravenous immunoglobulin.
Association of Patient Characteristics with Clinical Outcomes
The relationship of outcomes to patient characteristics are summarized in Table 2. Normal sleep spindles (P = .024) and early time to treatment (R 2 = .57, P = .030, Figure 1) were associated with better functional outcomes (6-month mRS). mRS was not significantly associated with age, cerebrospinal fluid white blood count, cerebrospinal fluid protein, platelet count, aspartate transaminase, alanine transaminase, ANE-SS scores, ANE MRI scores, specific MRI location abnormalities, normalized thalamic volume, epileptiform discharges or the presence of shock or intracranial hemorrhage, although the small sample size limited statistical power.
Association of Biomarkers With Outcomes.
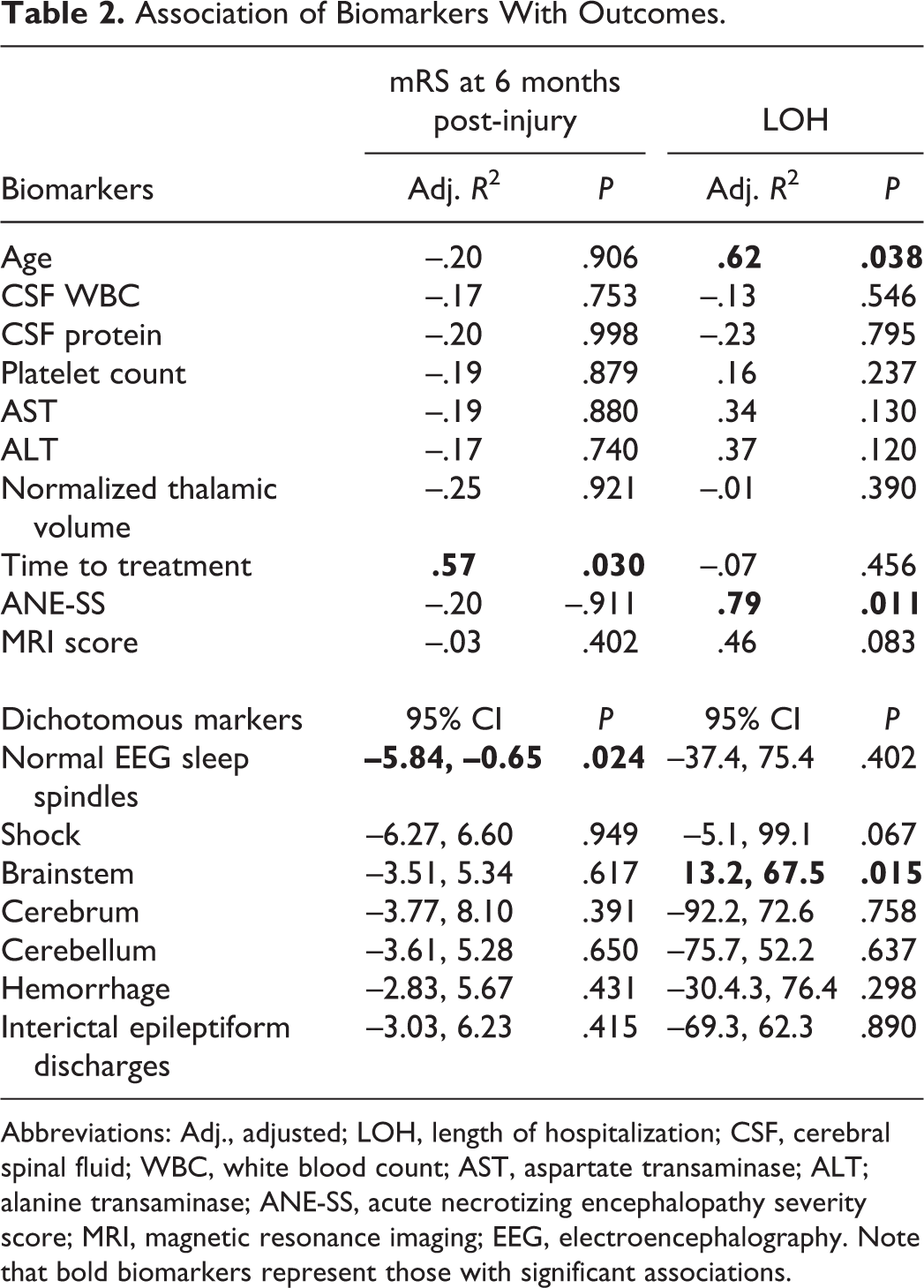
Abbreviations: Adj., adjusted; LOH, length of hospitalization; CSF, cerebral spinal fluid; WBC, white blood count; AST, aspartate transaminase; ALT; alanine transaminase; ANE-SS, acute necrotizing encephalopathy severity score; MRI, magnetic resonance imaging; EEG, electroencephalography. Note that bold biomarkers represent those with significant associations.
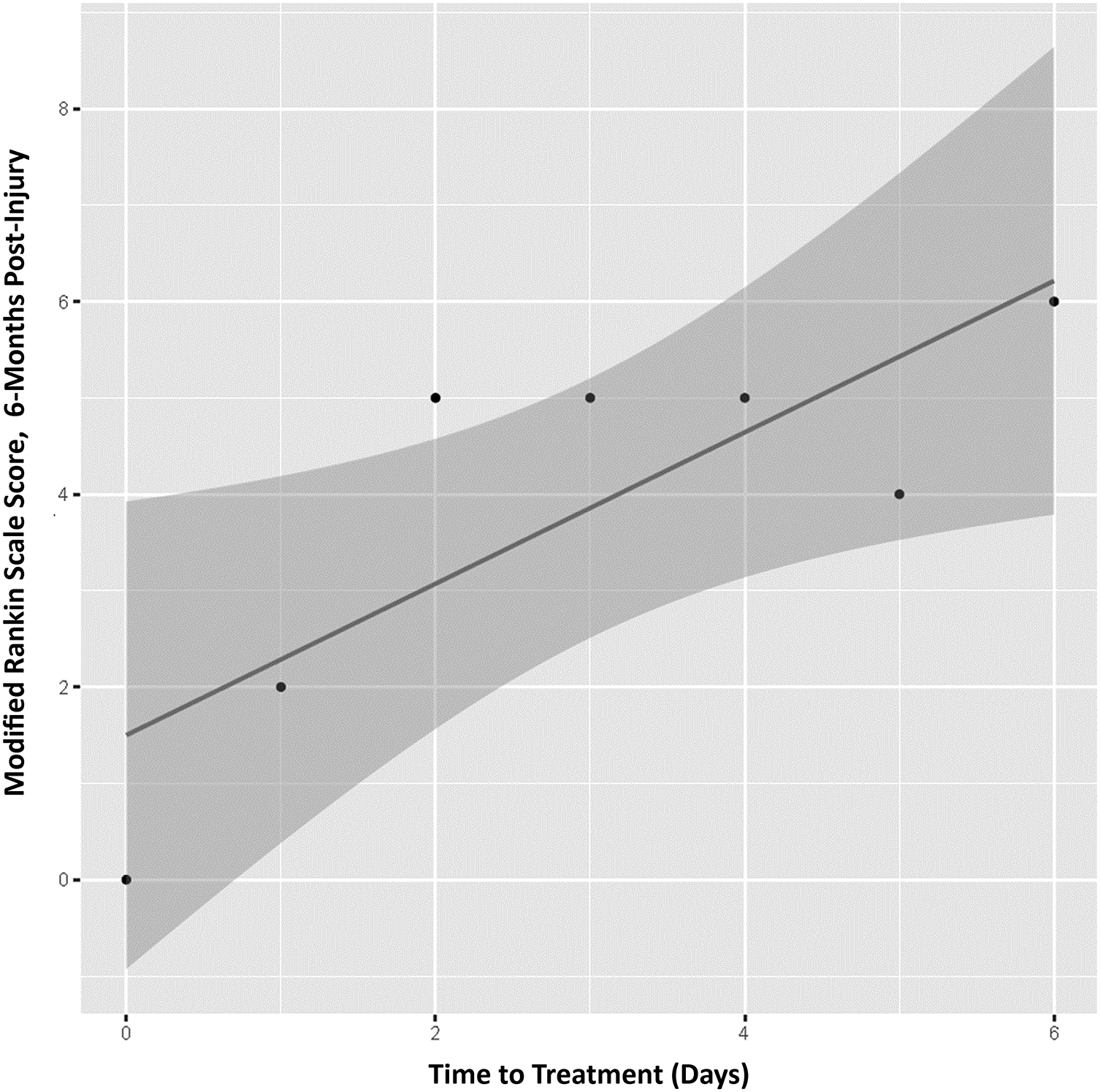
Association of treatment timing to modified Rankin Scale scores, 6 months post-injury. Early treatment is associated with decreased modified Rankin Scale scores at 6 months post-injury, indicative of better outcomes.
The authors observed that higher ANE-SS scores (R 2 = .79, P = .011), higher age (R 2 = .62, P = .038), and the presence of brainstem lesions (P = .015) were associated with longer length of hospitalization. The authors did not find significant associations between any other patient characteristics and length of hospitalization.
Discussion
The authors explored relationships between functional outcomes and treatment timing as well as clinical, MRI and EEG characteristics in children hospitalized for ANE. Better outcomes were associated with normal sleep spindles and early time to treatment. This study is the first to explore EEG biomarkers and volumetric MRI characteristics in association with outcome in children with ANE, and one of only a few studies to investigate treatment timing in relation to functional outcome.
The authors observed that time to treatment carries significant association with clinical outcomes after injury from ANE; a condition for which no consensus-based treatment recommendations exist. Immunomodulation is hypothesized to improve outcomes by acting on viral-induced hypercytokinemic responses known to mediate ANE pathogenesis. 16 Intravenous glucocorticoids, immunoglobulins, plasmapharesis, and Tocilizumab have been studied in retrospective cohorts with conflicting results. 17 -28 Timing of immunomodulatory treatment has been considered potentially critical in improving outcomes. Okumura et al retrospectively investigated 34 children with ANE and noted that in 17 children without brainstem lesions, steroid treatment administered within 24 hours after onset was associated with good outcome (no or mild cognitive deficit) and poor outcomes were noted in all patients without brainstem lesions who did not receive early steroids. 5 They did not find an effect for timing of treatment with either intravenous glucocortcoids or intravenous immunoglobulins in children with brainstem involvement. The authors investigated time to treatment in relation to outcome irrespective of brainstem lesions (4/7 of the patients had brainstem lesions). The authors noted 1 case (Patient 4) with brainstem involvement who received treatment on day 1 post-injury and had evidence of slight disability on 6-month follow-up (mRS = 2; Figure 2). This patient received intravenous Solumedrol and intravenous Tocilizumab 1 day after presentation, followed by intravenous immunoglobulins 3 days after presentation. Tocilizumab is a monoclonal antibody against the interleukin-6 receptor which may target the hypercytokinemic response seen in ANE and has been recently reported in a series of 3 children to be associated with good recovery. 6 While the authors did not observe that higher ANE-SS scores were associated with poor functional outcome, they did note that it was significantly associated with length of hospitalization. The ANE-SS score accounts for specific characteristics such as platelet count and shock, which relate to the potential of multisystem organ involvement in this condition. The need to treat those symptoms may relate to increased length of hospitalization. The findings suggest that early immunomodulatory therapy may improve outcomes for children with ANE.
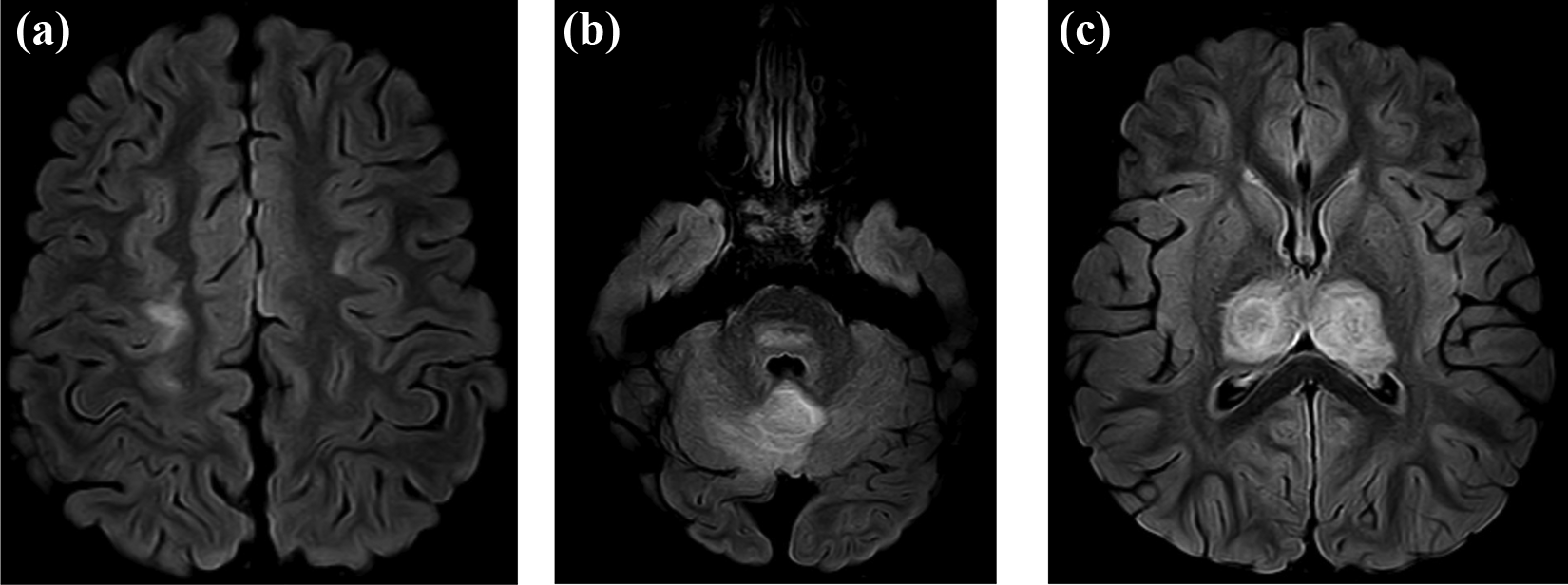
Example of brain magnetic resonance imaging scoring. Evidence of (a) cerebral white matter, (b) cerebellar white matter and pontine, and (c) bilateral thalamic involvement from fluid-attenuated inversion recovery images of patient 4 on day 1 post-injury. The patient received intravenous Solumedrol and Tocilizumab the same day after neuroimaging. Given brainstem and white matter involvement without hemorrhage or cavitation, her magnetic resonance imaging score is 2. At 6 months post-injury, she has a modified Rankin scale of 2, indicative of slight disability.
The finding that abnormal sleep spindles are associated with poor outcomes is previously unreported in the ANE literature (Figure 3). The potential for sleep spindles to be used as a biomarker for risk stratification is noteworthy, as sleep spindles serve as a surrogate of corticothalamic function 29 and ANE has predilection for affecting the thalami. The preservation of sleep spindles has been associated with good outcome after other acquired neurologic conditions such as anoxic ischemic encephalopathy after cardiac arrest. 30 This finding suggests that continuous EEG monitoring with evaluation for sleep spindles may be helpful during critical care management. The authors explored quantitative thalamic volumetric measurements on initial MRI scans to determine if they may represent an important biomarker for prognosis as well, although they did not find significance. The lack of association may be related to dynamic physiologic changes that occur during the first week of injury. 31 Thalamic volumetric measurements during the subacute or chronic time periods may be more predictive of outcome, but these were not explored in this study. The findings are in potential conflict with recent work suggesting that brainstem involvement and lower ANE MRI-scores were associated with worse outcome, 32 although timing of treatment initiation was not noted in that study. This further emphasizes that treatment timing may be a critical component in investigating the association of immunomodulation with outcomes.
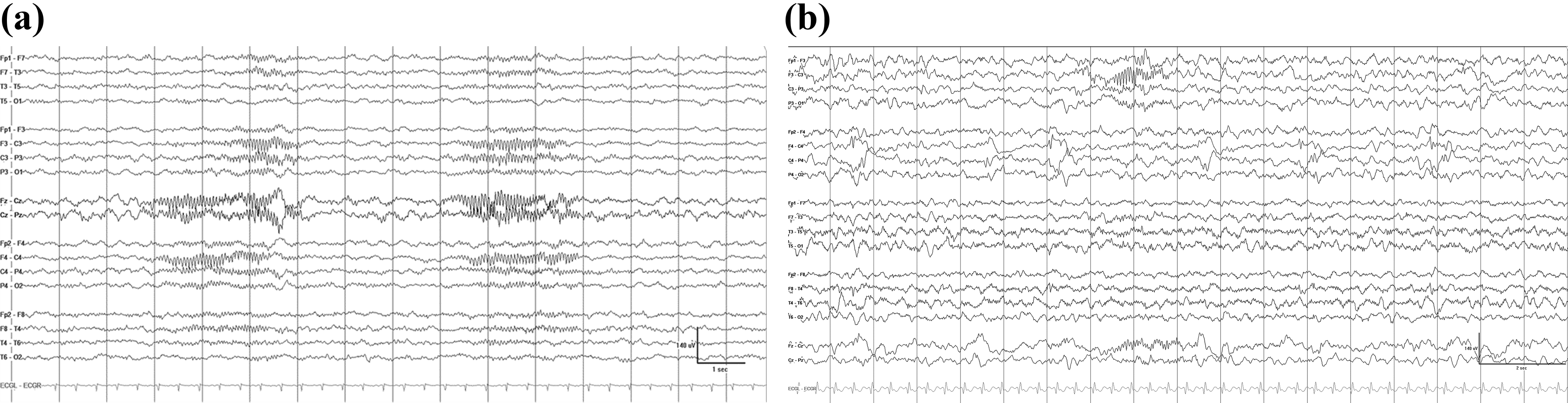
Sleep spindles on electroencephalography. Symmetric sleep spindles were observed from Patient 3 (a) who had good outcomes (6 months post-injury modified Rankin scale of 0). In contrast, absent right hemispheric sleep spindles were observed in Patient 7 (b) who also has right hemispheric interictal epileptiform discharges and poor outcome (6 months post-injury modified Rankin scale of 5).
It is noteworthy that within the series of 7 patients, all returned negative for RANBP2 mutations. Two children within the cohort were siblings, and 1 patient had recurrence of ANE later. These findings, along with other case reports, 33-34 indicate that there are likely other genes that predispose children to ANE as well as disease recurrence. There exists a need to identify whether such genetic biomarkers, once identified, would offer prognostic risk stratification. Knowledge regarding genetic susceptibility and implications for response to treatments may also contribute to precision-based care of acute ANE occurrences.
The study was limited by a small sample size and its retrospective nature. ANE is an exceedingly rare condition and there are substantial limitations in the ability to collect prospective data on these patients or to evaluate the effects of treatments on clinical outcomes, even in large centers. As a result of their institutional experience and the work of others, the authors have proposed a pathway for evaluating for suspected ANE and initiating early immunomodulatory therapy when suspicion is high (Figure 4). There exists a strong need to affirm whether specific therapies and timing of treatment are important in improving outcomes, and what biomarkers may be important for disease severity stratification. The development of concise interinstitutional protocols will help to implement effective strategies, thereby identifying patients early, characterizing biomarkers for injury severity and neurologic prognostication, and providing timely and appropriate treatment which can improve long-term outcomes.
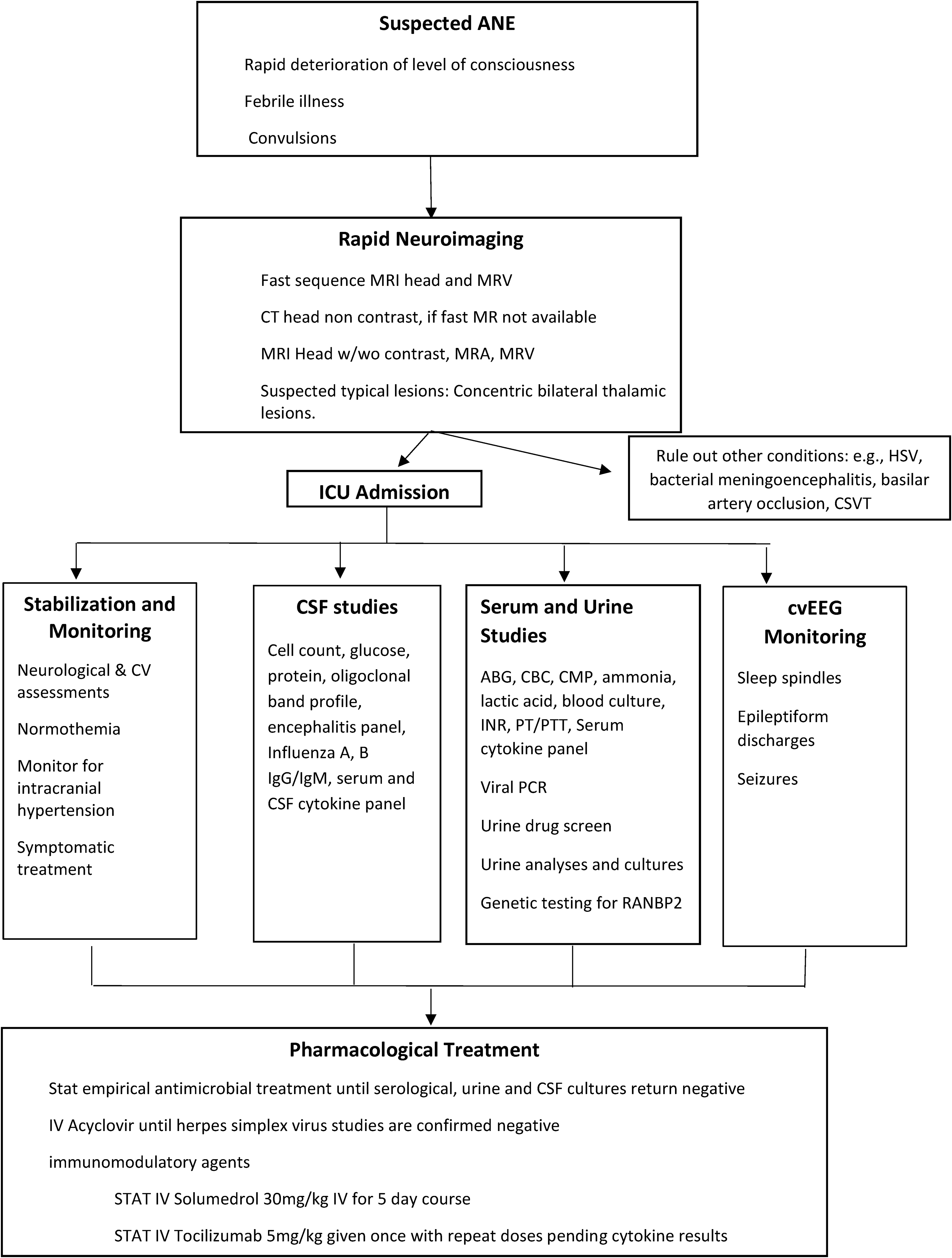
Proposed institutional pathway for evaluation and acute management of acute necrotizing encephalopathy. Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; w/wo, with and without contrast; MRA, magnetic resonance angiography; MRV, magnetic resonance venography; ICU, intensive care unit; HSV, herpes virus; CSVT, cerebral sinus venous thromboses; CV, cardiovascular; IgG, immunoglobulin G; IgM, immunoglobulin M; CSF, cerebral spinal fluid; ABG, arterial blood gas; CBC, complete blood count; CMP, complete metabolic panel; PT, prothrombin time; PTT, partial thromboplastin time; PCR, polymerase chain reaction; RANBP2, RAN binding protein 2; cvEEG, continuous video electroencephalogram; IV, intravenous; mg/kg, milligrams per kilograms; IVIG, intravenous immunoglobulin.
Footnotes
Author Contributions
BA and MK contributed significantly to the conception and design of the work, acquisition, analysis and interpretation of the work and drafting and critical revision of the the manuscript. SF, JF, SS, AO, and FB contributed to acquisition, analysis and interpretation of data and critical revision of the manuscript. IM, TM, VB, and DN contributed to interpretation of the work and critical revision of the manuscript. All authors provided final approval of the version to be published and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This work was approved by the Phoenix Children’s Hospital Institutional Review Board (IRB #20-040).