
Abstract
Aim:
To evaluate the role of diffusion tensor imaging of the auditory pathway in patients with Crigler Najjar syndrome type I and its relation to auditory brainstem response.
Methods:
Prospective study was done including 12 patients with Crigler Najjar syndrome type I and 10 age- and sex-matched controls that underwent diffusion tensor imaging of brain. Mean diffusivity and fractional anisotropy at 4 regions of the brain and brainstem on each side were measured and correlated with the results of auditory brainstem response for patients.
Results:
There was significantly higher mean diffusivity of cochlear nucleus, superior olivary nucleus, inferior colliculus, and auditory cortex of patients versus controls on both sides for all regions (P = .001). The fractional anisotropy of cochlear nucleus, superior olivary nucleus, inferior colliculus, and auditory cortex of patients versus controls was significantly lower, with P values of, respectively, .001, .001, .003, and .001 on the right side and .001, .001, .003, and .001 on left side, respectively. Also, a negative correlation was found between the maximum bilirubin level and fractional anisotropy of the left superior olivary nucleus and inferior colliculus of both sides. A positive correlation was found between the mean diffusivity and auditory brainstem response wave latency of the right inferior colliculus and left cochlear nucleus. The fractional anisotropy and auditory brainstem response wave latency of the right superior olivary nucleus, left cochlear nucleus, and inferior colliculus of both sides were negatively correlated.
Conclusion:
Diffusion tensor imaging can detect microstructural changes in the auditory pathway in Crigler Najjar syndrome type I that can be correlated with auditory brainstem response.
Keywords
Crigler-Najjar syndrome is a rare genetic disorder in which there is an inability to convert unconjugated bilirubin to the conjugated form, which can be cleared from the body. This is attributed to the lack of the liver enzyme required to metabolize bilirubin leading to unconjugated hyperbilirubinemia. Two types of Crigler-Najjar syndrome are known: type I, in which there is a near-total lack of enzyme activity, and type II, with partial enzyme activity. Both forms are autosomal recessive and caused by errors or mutations of the uridine diphosphate glucuronosy1 transferase (UGT1A1) gene. 1,2 The risk of neurologic damage by hyperbilirubinemia is not always reversible, because of associated neuronal cell death even with use of daily phototherapy. It can occur at any age. 2 -5
One of the most common clinical presentations of Crigler-Najjar syndrome is hearing impairment. 3 -7 The auditory system is highly sensitive to bilirubin effects that can be just subtle hearing abnormalities up to complete deafness. It may occur at total serum bilirubin levels that were previously thought to be harmless. It can also occur in the absence of other signs of kernicterus. 8,9 Brainstem cochlear nuclei are the first structures affected by elevated total serum bilirubin levels, followed by the auditory nerve, with the higher neural centers involved last. 10 Permanent infantile hearing loss is an important public health problem. It not only affects language development but can also affect emotional, cognitive, and social development. 11
Auditory brainstem response provides an electrophysiologic means of assessing the ascending auditory pathway and localizing the lesions. 12 Auditory evoked potentials represent the response of the auditory pathway to an auditory stimulus that categorized based on the latency of the response following the auditory stimulus. They have been used to study the central auditory nervous system. They are objective tests, independent of an individual’s subjective response. 13,14 Auditory brainstem response includes a series of 5 to 7 peaks arising from the auditory nerve and brainstem structures occurring within 10 milliseconds (ms) of the onset of acoustic stimulus click or tone burst in an ontologically, audiologically, and neurologically intact individual. 15,16
One of the advanced magnetic resonance imaging (MRI) techniques that can quantitatively evaluate tissue microstructures is diffusion tensor imaging. It can study water molecules’ microscopic movements. The commonly used diffusion tensor imaging measurements are fractional anisotropy and mean diffusivity. 17 -20 Fractional anisotropy is an indicator of tissue microscopic criteria through the identification of their directional diffusion properties. Mean diffusivity is another parameter that measures the isotropic diffusion of water in multiple directions. Thus, diffusion tensor imaging is an MRI tool that can be used to investigate brain tissue structures in several diseases. 21 -24 Regarding the clinical utility of the current study, only a few studies have addressed the role of diffusion tensor imaging in pediatric patients 25,26 and the auditory pathway in the adult. 26 -29 Only 1 study discussed the role of diffusion tensor imaging of the gray and white matter of the brain in Crigler-Najjar syndrome type I without assessment of the cortical auditory pathway. 30 To our knowledge, there are no previous studies of the auditory pathway in patients with Crigler-Najjar syndrome type I.
The aim of this study was to evaluate the role of diffusion tensor imaging in assessing the microstructural integrity of the auditory pathways in children with Crigler-Najjar syndrome type I and its correlation with auditory brainstem response.
Patients and Methods
Patients
Twelve patients without clinically detectable hearing loss proved to be Crigler-Najjar syndrome type I (diagnosed based on persistently elevated unconjugated serum bilirubin levels greater than 20-50 mg/dL in the absence of hemolysis or other liver diseases; they did not contain more than traces of bilirubin conjugates). Regarding Crigler-Najjar syndrome type II, bilirubin does not exceed 20 mg/dL and can be lowered by phenobarbital therapy by at least 25%. The bile of these patients contains bilirubin monoconjugates and traces of deconjugates. In addition, 10 age- and sex-matched controls with normal hearing, proved by the absence of a clinical complaint of hearing loss or previous history of ear disease added to the normal routine tympanogram done for all patients and control groups (who were undergoing MRI examinations for other reasons not related to the auditory disease), were enrolled in this prospective, case-control study. Ethical approval from the institutional review board was obtained and informed consent was taken from the parents/guardians of the patients and controls before enrollment in the study. The patients were 5 boys and 7 girls with mean age 8.01±4.9 years, and the controls were 5 boys and 5 girls with mean age 6.19 ± 4.1 years. Serial serum bilirubin level was done for all patients, and the highest level was used for analysis. The auditory assessment with auditory brainstem response was done for all patients, and diffusion tensor imaging of the brain was performed for both patients and controls.
MRI Imaging
MRI of the brain and brainstem was done for all patients and controls. Oral chloral hydrate in a dose of 70 to 80 mg/kg of body weight was used to sedate 4 patients and 5 controls. The MR examination was performed using a 1.5-tesla scanner (Ingenia; Philips, Best, Netherlands). Head neck coil with 20 channels was used. Routine sequences were obtained first; T1-weighted (time to response [TR] / time to echo [TE] = 620/20 ms), T2-weighted image (TR/ TE = 5430/95 ms), and fluid-attenuated inversion recovery (TR/TE/TI = 10500/120/2800 ms) with matrix = 80 × 80, field of view = 240 × 220 mm and slice thickness = 5 mm. The diffusion tensor imaging was also done with a single-shot echo-planar sequence (TR/TE=3118/93 ms). Then diffusion gradients were applied along 32 axes, using a b-value of (0 and 1000 s/mm2). Field of view = 240 × 220 mm2 and data matrix = 92 × 88 were used, leading to voxel dimensions (2.43 × 2.54 × 2.5 mm). Slice thickness of 2.5 mm, no gap, and the total scan time = 7-8 minutes.
Auditory Brainstem Response
Auditory brainstem response was analyzed for all patients. Oral chloral hydrate in a dose of 70 to 80 mg/kg of body weight was used to sedate 4 patients and 5 controls. Auditory brainstem response evaluations have been performed with the Bio-Logic Systems Corp’s Navigator devise. In the auditory brainstem response evaluations, 21.1 rates click stimulus, 10 msn analysis time, 1500 sweep in averaging, and 100 to 3000 Hz filtration was used. The high forehead was used as the non-inverting electrode. The mastoid ipsilateral to the stimulus was used as the inverting electrode site and the mastoid contralateral to the stimulus was used as the ground electrode. All impedances were less than 5 kΩ. The analysis of the auditory brainstem response waveforms consisted of peak latency for waves I, III, and V. The 2 waveforms were overlapped on the computer screen, and a cursor was used to obtain measurements. Peak latencies for waves I and III were measured at the highest peak. Peak latency for wave V was measured at the highest peak if there was a clearly identifiable wave IV. If waves IV and V were complex, wave V was measured at the farthest excursion before the trough of the complex.
Image Analysis
A pediatric neuroradiologist did an analysis of the obtained MR images. He was blinded to the clinical and laboratory data. The single-pixel seed isotropic region of interest was placed in 4 regions (cochlear nucleus [CN], superior olivary complex [SOC], inferior colliculus [IC], and auditory cortex [AC]) on each side (Figure 1). The fractional anisotropy and mean diffusivity readings were registered in an Excel sheet and used for statistical analysis.
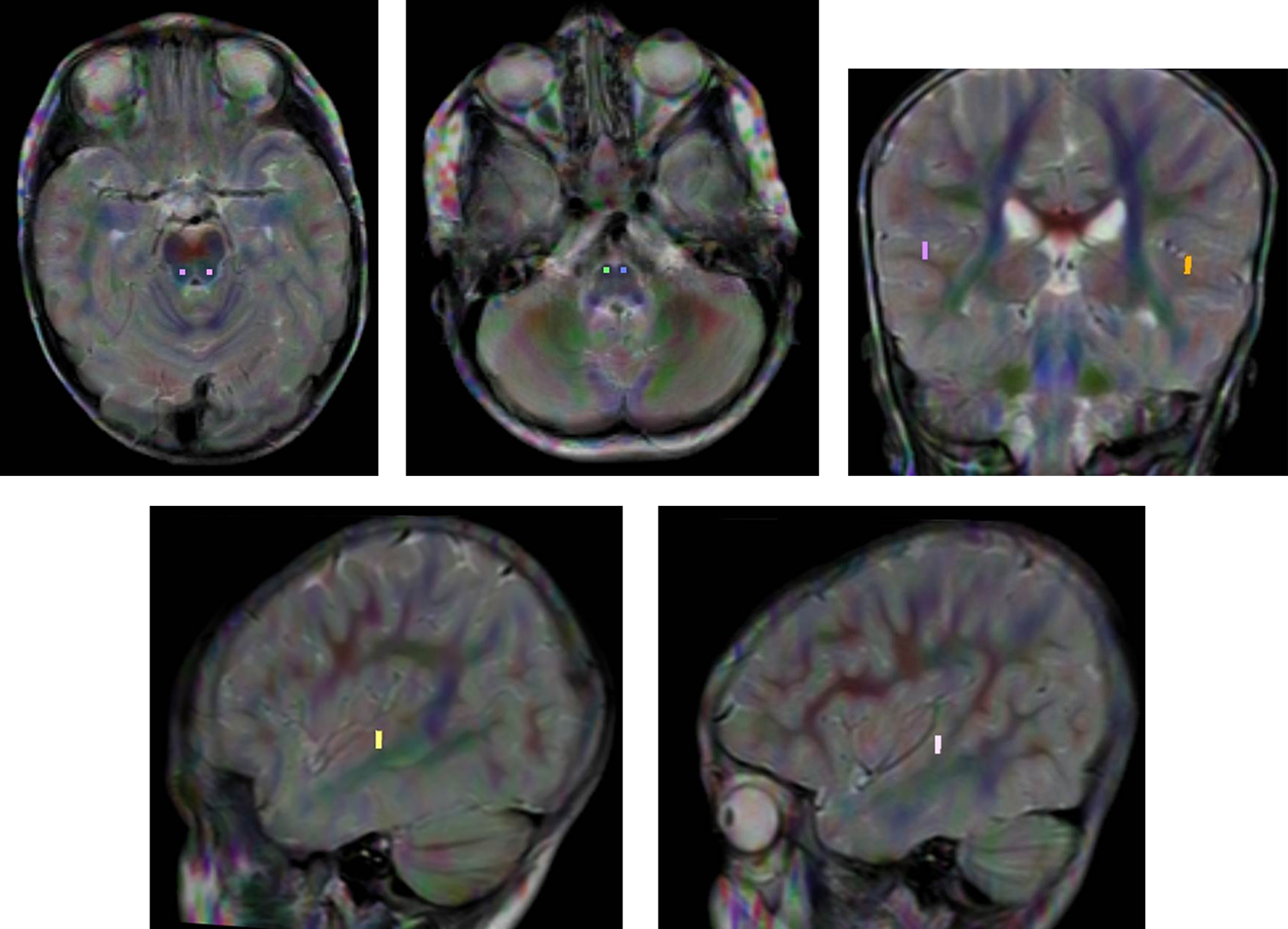
Regions of interest localization: single pixel seed isotropic region of interest was placed in 4 regions on each side—cochlear nucleus, superior olivary complex, inferior colliculus, and auditory cortex.
Statistical Analysis
Statistical analyses were done using Statistical Package for Social Sciences version 25 (SPSS, Chicago, IL). Quantitative data were presented as mean and standard deviation (SD). The mean and standard deviation of the fractional anisotropy and mean diffusivity of the selected regions on each side in the patients and controls were calculated. Normally distributed data were compared between the 2 groups using independent samples t test. Data that violated the normality assumptions were compared using the Mann-Whitney test. Probability values less than .05 were considered statistically significant. Pearson correlation test was performed to correlate the fractional anisotropy and ADC of the auditory pathway with auditory brainstem response results. The correlation coefficient r and P value were calculated.
Results
On conventional brain MRI examinations, no abnormality could be detected in any of the patients or controls.
There was a significantly higher mean diffusivity value (P = .001) of the cochlear nucleus, superior olivary nucleus, inferior colliculus, and auditory cortex on both sides in patients compared with controls. The mean diffusivity of the cochlear nucleus, superior olivary nucleus, inferior colliculus, and auditory cortex in patients were (0.87 ± 0.08, 0.85 ± 0.11, 0.74 ± 0.07, and 0.9 ± 0.09 ×10–3 mm2/s) and of the controls were (0.72 ± 0.02, 0.67 ± 0.03, 0.62 ± 0.03, and 0.75 ± 0.04 ×10–3 mm2/s), respectively. The mean diffusivity for the patients were (0.85 ± 0.06, 0.86 ± 0.14, 0.78 ± 0.06, and 0.89 ± 0.06 ×10–3 mm2/s) and for controls were (0.75 ± 0.04, 0.67 ± 0.03, 0.64 ± 0.06, and 0.79 ± 0.02 ×10–3 mm2/s), respectively (Table 1).
Mean, Standard Deviation, Minimum and Maximum Mean Diffusivity Values of the Selected Regions on Each Side in Patients and Control Groups.
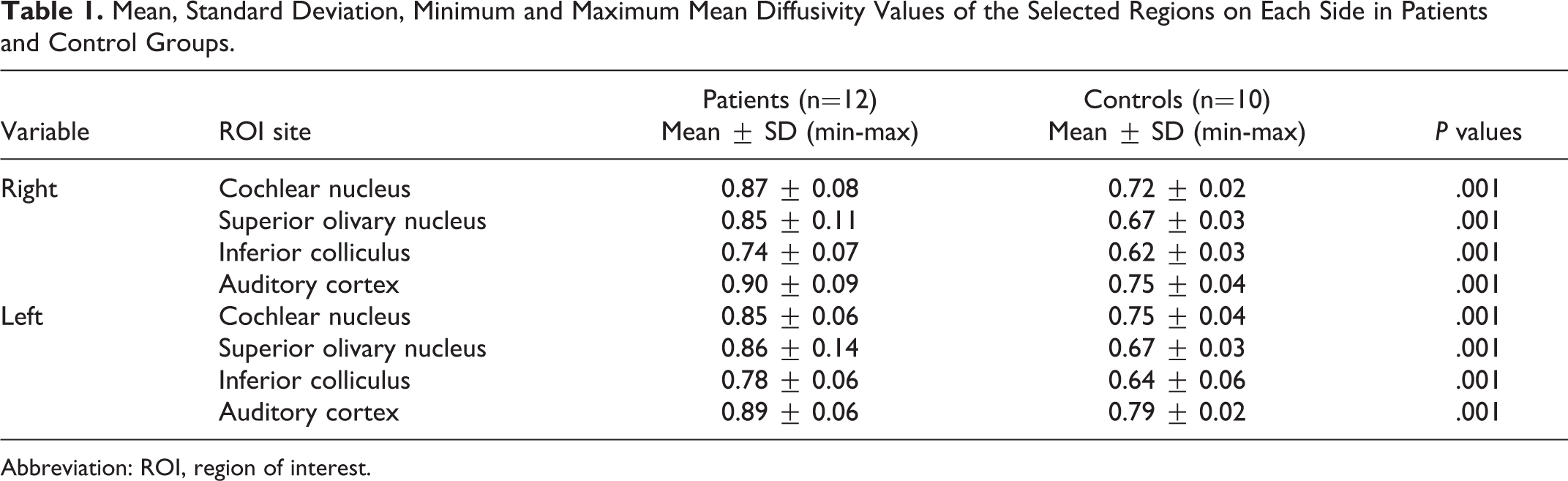
Abbreviation: ROI, region of interest.
There was significantly lower fractional anisotropy of the cochlear nucleus, superior olivary nucleus, inferior colliculus, and auditory cortex on both sides in patients compared with control groups. The fractional anisotropy values of the cochlear nucleus, superior olivary nucleus, inferior colliculus, and auditory cortex in patients were (0.46 ± 0.15, 0.5 ± 0.13, 0.55 ± 0.08, and 0.15 ± 0.05) and of the controls were (0.62 ± 0.04, 0.67 ± 0.04, 0.65 ± 0.07, and 0.23 ± 0.03) with significant difference (P = .001, .001, .003, and .001), respectively. The fractional anisotropy values of the cochlear nucleus, superior olivary nucleus, inferior colliculus, and auditory cortex for the patients were 0.39 ± 0.16, 0.48 ± 0.14, 0.54 ± 0.09, and 0.15 ± 0.05, respectively, and that of the controls were 0.61 ± 0.04, 0.67 ± 0.04, 0.66 ± 0.07, and 0.23 ± 0.03, with significant difference (P = .001, .001, .003, and .001), respectively (Table 2).
Mean, Standard Deviation, and Minimum and Maximum Fractional Anisotropy Values of the Selected Regions on Each Side in Patients and Control Groups.
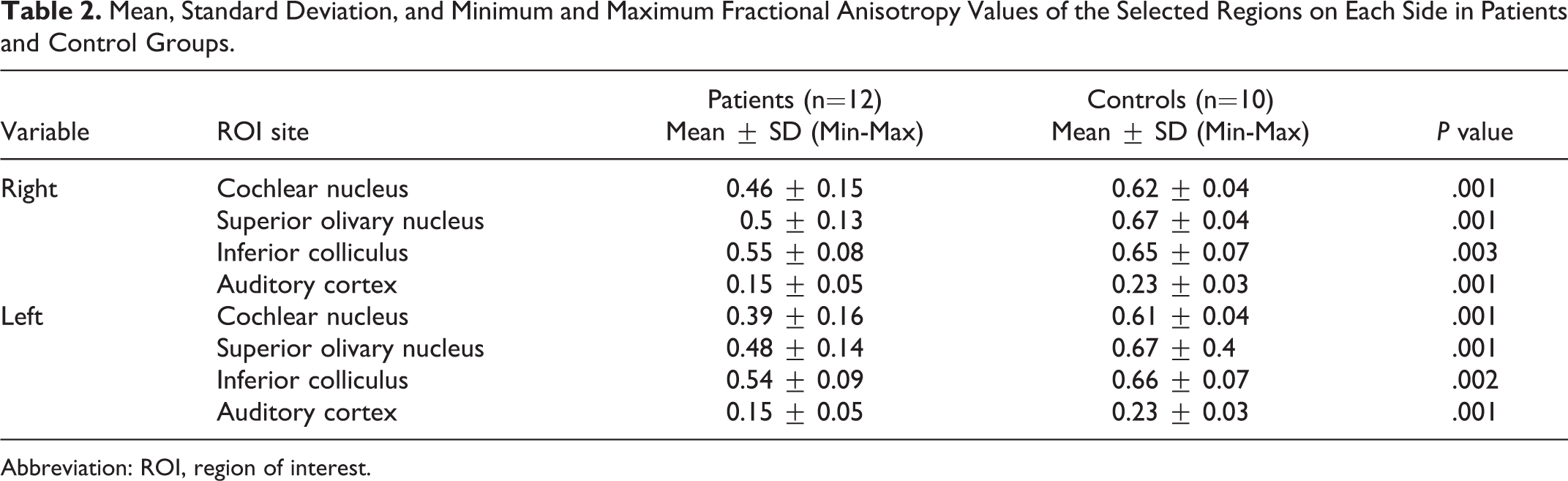
Abbreviation: ROI, region of interest.
There was negative correlation between the maximum bilirubin level and fractional anisotropy of the left superior olivary nucleus (r = –0.67, P = .04) and inferior colliculus (r = –0.7, P = .02) on both sides. There was positive correlation between the mean diffusivity and auditory brainstem response wave latency of the right inferior colliculus (r = 0.93, P = .001) and left cochlear nucleus (r = 0.64, P = .05). There was negative correlation between fractional anisotropy and auditory brainstem response wave latency of the right superior olivary nucleus (r = –0.78, P = .008), left cochlear nucleus (r = –0.77, P = .009) and the inferior colliculus on both sides (r = –0.94, P = .001) and (r = –0.92, P = .001), respectively. Figure (2) shows auditory brainstem response of controls and Figure (3) shows auditory brainstem response of child with Crigler-Najjar syndrome type I.
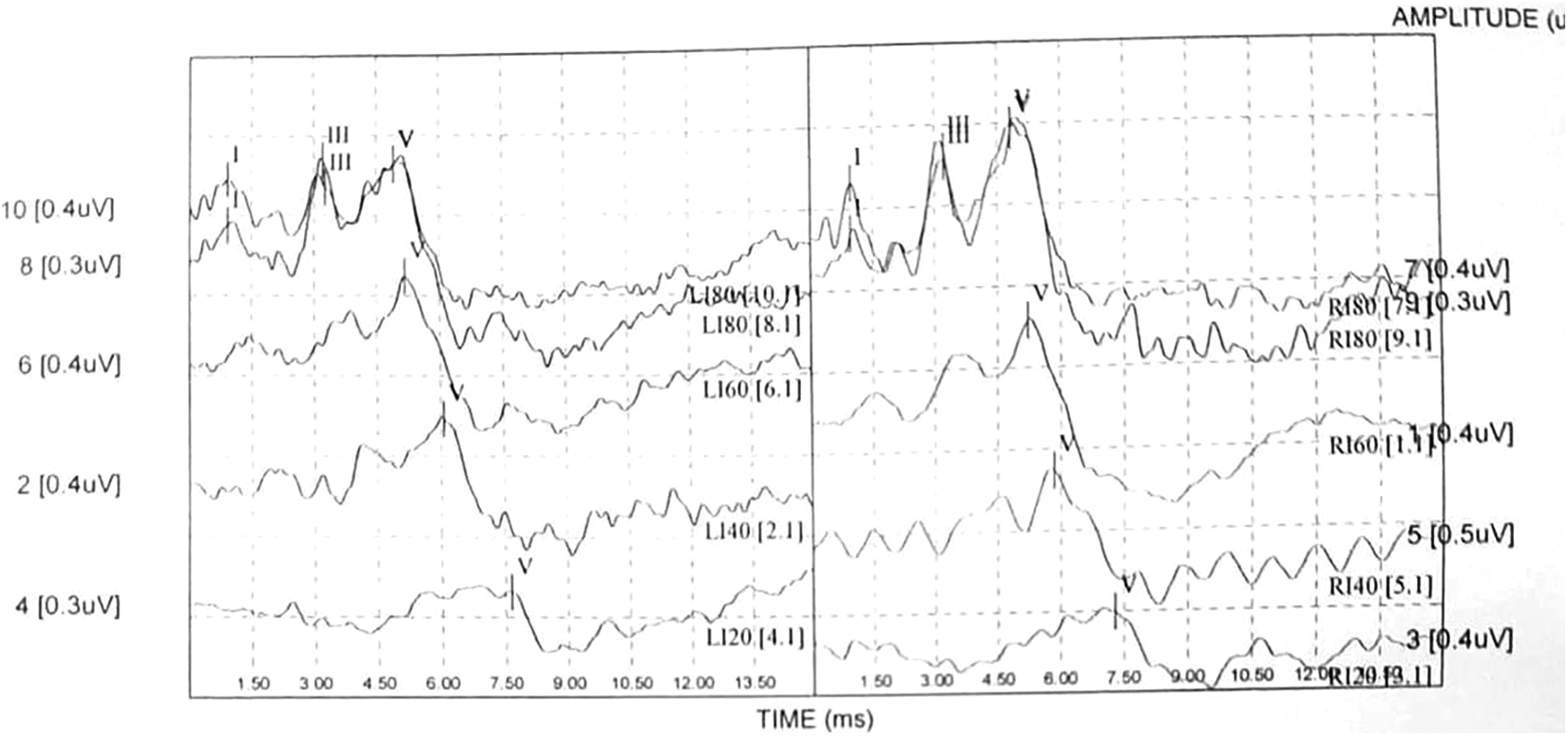
ABR of controls: ABR shows normal waves I, III, and V, and wave V can be traced down to 20 dBnHL. Abbreviations: ABR, auditory brainstem response; dBnHL, decibels above normal adult hearing level.
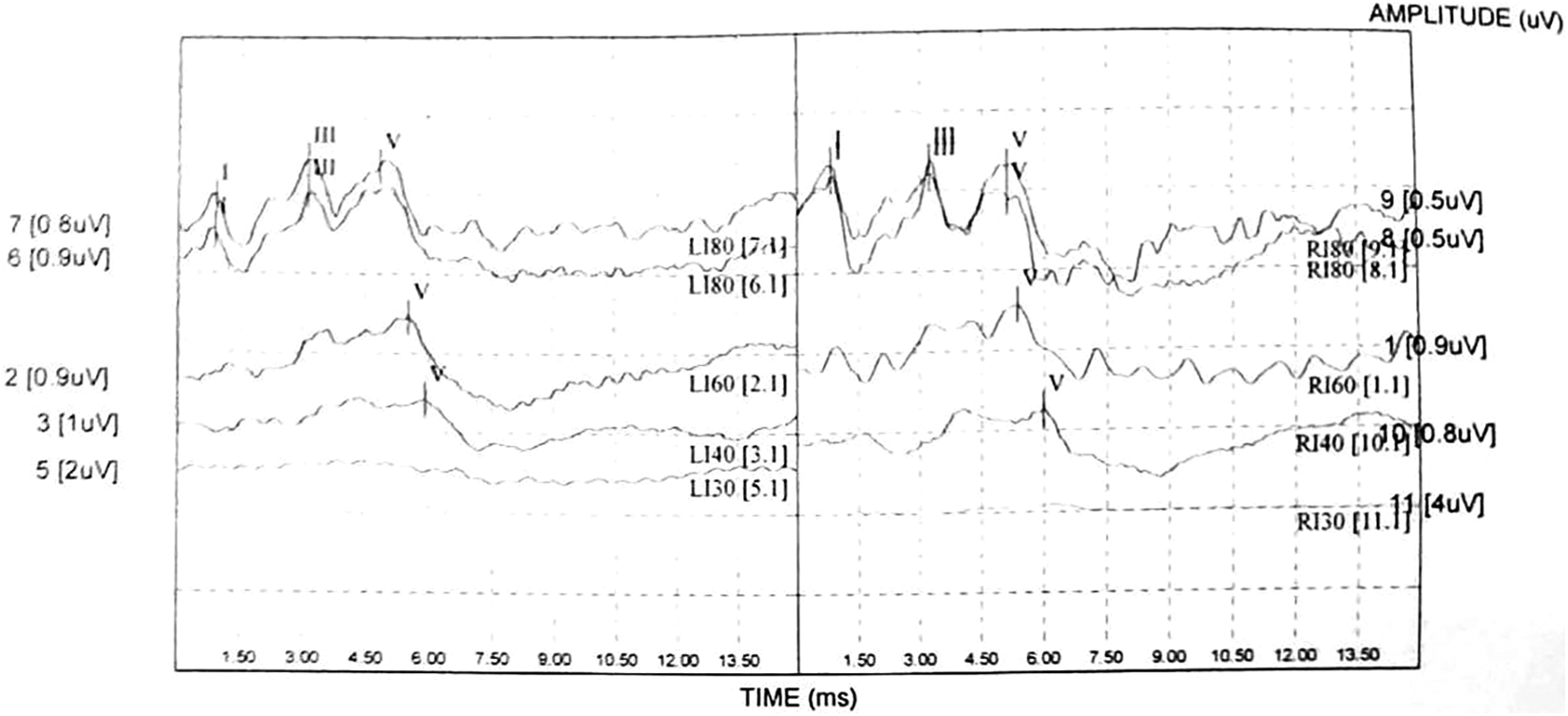
ABR of CNS-I: ABR shows mild hearing loss with wave V can be traced down to 30 dBnHL. Abbreviations: ABR, auditory brainstem response; CNS-I, Crigler-Najjar syndrome type I; dB nHL, decibels above normal adult hearing level.
Discussion
Crigler-Najjar syndrome is a rare genetic disorder that presents with unconjugated hyperbilirubinemia. Hearing impairment is one of the common clinical presentations because the auditory system is highly sensitive to bilirubin effects that can range from subtle hearing abnormalities up to complete deafness. It may occur at a low total serum bilirubin levels. 4 -9
The main findings in this study are the significantly higher mean diffusivity and lower fractional anisotropy value of the selected regions of the auditory pathway (cochlear nucleus, superior olivary complex, inferior colliculus, and auditory cortex) on both sides. These changes are correlated with auditory brainstem response results. We did not find any abnormal signal intensity on T2-weighted image or fluid-attenuated inversion recovery images in the selected regions along the auditory pathway, while on diffusion tensor imaging abnormalities were detected. This could be related to the minimal changes and damage in the selected regions that could be under the minimum level to be detected by conventional MRI. Also, diffusion tensor imaging parameters become abnormal before the detection of morphologic changes on conventional MR because of its sensitivity to microstructural changes. So, diffusion tensor imaging improved sensitivity and objectivity in the early detection of minor developmental and long-term changes along specific anatomic pathways that could be missed by the relatively subjective conventional MRI. 21 -23
In this study, there is a statistically significant higher mean diffusivity and lower fractional anisotropy of selected regions of patients. This effect could be related to chronic exposure to high levels of unconjugated bilirubin, resulting in cell death with subsequent increased extracellular spaces with free diffusion and increased mean diffusivity values. 24 -30 The cell death resulting from the toxic effect of the unconjugated hyperbilirubinemia is also associated with demyelination, and because myelin is the most important factor in the presence of anisotropy; thus, changes in the anisotropy and lower fractional anisotropy values appear. 26 -30 The fractional anisotropy and mean diffusivity may vary independently because the damaged brain tissue has glial and neuronal cells and the changes of the mean diffusivity are related to the mainly isotropic nature of gray matter. 21 -25
Bilirubin-induced neuronal damage can be explained by different mechanisms. First unconjugated bilirubin can diffuse passively through cell membranes and the blood-brain barrier and accumulate within the cytoplasm and become toxic. This effect is augmented by the neuronal supporting cells, which when exposed to bilirubin, secrete inflammatory markers leading to increased permeability of the blood-brain barrier and thus more bilirubin cell loading and more toxic effect. 31,32 Hyperbilirubinemia also causes impairment of calcium homeostasis, which is an important mechanism in neuronal toxicity. 33
When the neuronal cells become exposed to bilirubin, there will be an increase in the oxidative stress and decreased neuronal proliferation together with presynaptic neurodegeneration at the central glutaminergic synapses. The hyperbilirubinemia results in smaller spiral ganglion cell bodies with decreased cellular density and selective loss of large cranial nerve VIII myelinated fibers. 2,34,35 Another study added that when bilirubin was applied to cultured auditory neurons taken from brainstem cochlear nuclei, it resulted in hyperexcitability and excitotoxicity. 36
In our study, there was a negative correlation between the maximum bilirubin levels and fractional anisotropy values of the left superior olivary nucleus and inferior colliculus on both sides. One study reported that serum bilirubin level is used only in the assessment of the severity of hyperbilirubinemia in the newborn, especially preterm, but it is unhelpful in the detection of the neurologic outcome. 37
Assessment of the ascending auditory pathway with lesions localization can be obtained from the auditory brainstem response. The electric field generated by the compound firing of neurons permits tracking of the auditory signal as it travels from the cochlea through each of the brainstem nuclei in sequence. 38,39 Auditory brainstem response is considered the test of choice in hearing screening to detect auditory damage in children with hyperbilirubinemia. It is a sensitive test to the earliest manifestations of neurotoxicity that can be resolved with phototherapy and exchange transfusion, but it can take about 1 hour or more to get the results. 40 -43 In our study, a negative correlation is detected between fractional anisotropy values and auditory brainstem response wave latency of the right superior olivary nucleus and left cochlear nucleus together with the inferior colliculus on both sides. In addition, a positive correlation could be detected between mean diffusivity values and auditory brainstem response wave latency of the right inferior colliculus and left cochlear nucleus. This established the value of diffusion tensor imaging in the evaluation of the auditory pathway, which takes less time for patient examination by MRI machine.
There are a few limitations to this study. First, no gene testing or identification of the pathogenic mutation were done because of limited resources of the study, so further studies with gene testing and pathogenic mutation detection should be done. Second, only 1 reader for region of interest placement was included in this study, which may affect the values of fractional anisotropy and mean diffusivity, so further studies should be done with 2 readers for region of interest placement independently for accuracy. Third, the number of patients included in the study was relatively small; therefore, multicenter studies on a larger number of patients are recommended to confirm the results. Fourth, the study used diffusion tensor imaging on a 1.5-tesla scanner using regions of interest, so further studies are needed with multiparametric MR imaging of proton MR spectroscopy using higher tesla scanners 43 -47 with application of advanced postprocessing and machine learning 46 -48 to improve the results. Fifth, there is no serial follow-up with diffusion tensor imaging of these patients, so further studies with serial follow-up with diffusion tensor imaging are recommended for better evaluation.
Conclusion
Diffusion tensor imaging can detect microstructural changes of the auditory pathway in patients with Crigler-Najjar syndrome type I that well correlated with auditory brainstem response results.
Supplemental Material
Supplemental Material, sj-pdf-1-jcn-10.1177_08830738211025865 - Diffusion Tensor Imaging of Auditory Pathway in Patients With Crigler-Najjar Syndrome Type I: Correlation With Auditory Brainstem Response
Supplemental Material, sj-pdf-1-jcn-10.1177_08830738211025865 for Diffusion Tensor Imaging of Auditory Pathway in Patients With Crigler-Najjar Syndrome Type I: Correlation With Auditory Brainstem Response by Ahmed Abdel Khalek Abdel Razek, Mohamed Ezz El Regal, Mortada El-Shabrawi, Mohamed Moustafa Abdeltawwab, Ahmed Megahed, Sherine Elzeny, Noha El Tantawi and Saher Ebrahiem Taman in Journal of Child Neurology
Footnotes
Author Contributions
Ahmed Abdel Khalek Abdel Razek: Choosing the title of the study, putting study framework, doing MRI examinations, participating in statistical data preparation together with manuscript reviewing and submission.
Mohamed Ezz El Regal: Performing clinical examinations, collecting laboratory results, participating in full history taking, collecting clinical and Demographic data together with statistical data preparation.
Mortada El-Shabrawi: Performing clinical examinations, collecting laboratory results, participating in full history taking, collecting clinical and Demographic data together with statistical data preparation.
Mohamed Moustafa Abdeltawwab: Performing ABER examinations, participating in full history taking, collecting ENT clinical data together with statistical data preparation.
Ahmed Megahed: Performing clinical examinations, collecting laboratory results, participating in full history taking, collecting clinical and Demographic data together with statistical data preparation.
Sherine Elzeny: Performing clinical examinations, collecting laboratory results, participating in full history taking, collecting clinical and Demographic data together with statistical data preparation.
Noha El Tantawi: Performing clinical neurological examinations, participating in full history taking, collecting clinical and Demographic data together with statistical data preparation.
Saher Ebrahiem Taman: Doing MRI examinations, reviewing and preparing images for processing, performing images processing and registering DTI readings, statistical data preparation together with manuscript writing and preparation for submission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Institutional Review Board, Mansoura Faculty of Medicine, Mansoura University, IRB approval number (R/18.05.197). Informed consent was obtained from guardians of the children.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.