
Abstract
Objective:
To explore perspectives of pediatric neurologists regarding sexual and reproductive health care for adolescent women with epilepsy (WWE) and intellectual disability.
Methods:
We interviewed pediatric neurologists regarding sexual and reproductive health for WWE with intellectual disability. We audio-recorded and transcribed interviews and conducted qualitative analysis.
Results:
16 pediatric neurologists participated. Themes included the following: (1) Pediatric neurologists have differing perspectives about how intellectual disability affects WWE’s sexual and reproductive health needs, (2) pediatric neurologists provide sexual and reproductive health counseling variable in content and frequency to this population, (3) pediatric neurologists tend to recommend longer-term methods of contraception for this population, and (4) pediatric neurologists are asked to be involved in decision-making around sterilization, yet express ethico-legal reservations.
Conclusion:
Our findings suggest pediatric neurologists provide variable, often suboptimal, sexual and reproductive health care for WWE and intellectual disability. Themes reveal ethical concerns among neurologists about sexual and reproductive health practices including sterilization. More tailored clinical guidelines and provider training on sexual and reproductive health for this population may be beneficial.
Epilepsy and intellectual disability commonly co-occur. Nearly 20% of people with intellectual disability have epilepsy, and nearly 25% of people with epilepsy have intellectual disability. 1 -6 Adolescent and young adult women with epilepsy (WWE) and intellectual disability experience sexual and reproductive health disparities. While adolescent and young adult women with intellectual disability have similar fertility rates as peers with typical development, they experience a disproportionately higher burden of sexually transmitted infections and sexual abuse. 7 -9 Women with intellectual disability and epilepsy face additional challenges such as antiseizure medications with teratogenic effects or drug interactions with contraceptives. 10
Adolescent and young adult WWE with intellectual disability may benefit from sexual and reproductive health counseling about contraception, sexually transmitted infections, pregnancy, menstruation, folic acid supplementation, relationship violence, sexual abuse, and teratogenesis. However, prior research has suggested that health care professionals provide suboptimal sexual and reproductive health care to adolescent and young adult WWE and/or intellectual disability. Adolescent and young adult WWE have reported receiving inadequate contraceptive information from health care providers. 11 Pediatric neurologists have reported performing limited sexual and reproductive health counseling with adolescent and young adult WWE. 12 Primary care pediatricians disproportionately omit provision of sexual and reproductive health care to adolescent and young adult women with intellectual disability compared with patients without disabilities. 13
Despite sexual and reproductive health concerns faced by WWE with intellectual disability, there are no previous studies of sexual and reproductive health care specific to this population. As adolescents and young adults with chronic conditions often perceive their subspecialist as their primary medical provider, understanding sexual and reproductive health care provision in pediatric neurology is critical for understanding how these patients’ sexual and reproductive health care needs are addressed. 14 The attitudes and practices of pediatric neurologists regarding sexual and reproductive health care for adolescent and young adult WWE with intellectual disability have not previously been investigated. Regarding sexual and reproductive health care for WWE with typical development, we previously found that neurologists reported challenges in providing sexual and reproductive healthcare occasionally omitting this care. 12
In this study, we explore the attitudes and practices of pediatric neurologists concerning sexual and reproductive healthcare for adolescent and young adult WWE, including the impact of patients’ intellectual disability on sexual and reproductive health care provision. To elicit a heterogeneity of perspectives including personal attitudes and practices that may contribute to gaps in sexual and reproductive health care for this population, we conducted qualitative, anonymous interviews with pediatric neurologists and epileptologists.
Methods
We used purposive sampling to recruit pediatric neurologists (including general neurologists and epileptologists) by e-mail to participate in individual semistructured interviews by telephone. We invited participants to ensure diversity of gender, location within the United States, institution, and years in practice. Prior to the interviews, the lead author developed an interview guide consisting of questions and probes. Although we did not formally pilot test the interview guide, it was adapted from one previously used to research pulmonologists’ sexual and reproductive health care for patients with cystic fibrosis. 15 Participants provided verbal informed consent. The lead author is a female pediatric neurologist with experience conducting qualitative research. She had no prior relationship with participants. Participants were made aware that she is a pediatric neurologist studying sexual and reproductive health for WWE. She conducted all interviews in private. Participants were interviewed from settings of their choosing. Interviews occurred from May to July 2019. The lead author conducted, audio-recorded, and transcribed all interviews and took field notes. There were no repeat interviews. The interviews addressed sexual and reproductive health for adolescent and young adult WWE. Certain questions and probes addressed whether and how a patient’s intellectual disability would influence participants’ sexual and reproductive health care practices. Interviews lasted between 30 and 60 minutes. We did not return transcripts to participants for comments.
Following Braun and Clarke’s thematic analysis approach, 16 2 independent coders (L.K., A.C.) used NVivo 12 software (QSR International, Melbourne) to code transcribed interviews, conduct thematic analysis, elucidate themes, and select illustrative quotations. After developing a preliminary codebook, the coders applied it to transcripts using consensus coding while creating additional codes as needed. The coders met repeatedly to review their work, discuss differences, and identify and define any new codes, proceeding iteratively until no new codes were developed. A senior coinvestigator (T.M.K.) was available to review discrepancies. We used the final codebook to analyze all transcripts and evaluate themes. We identified illustrative quotations for each theme. Participants did not provide feedback on the findings.
Results
Sixteen physicians, including 6 general pediatric neurologists and 10 epileptologists, completed the interview (44% male). Three additional candidates declined interviews for unstated reasons. Participants ranged in years in practice from 1 to 45, with a median of 11, were located across the United States, and practiced in academic and private settings (15 total institutions or practices). Although we attained thematic saturation after 12 interviews, we continued recruitment to increase diversity of perspectives by geography and discipline, and analyzed data from all 16 interviews. Several themes that emerged concerning pediatric neurologists’ attitudes and practices regarding sexual and reproductive health for adolescent and young adult WWE with intellectual disability are summarized below with additional representative statements that further demonstrate each theme presented in Table 1.
Sample Statements Reflecting Themes Regarding Pediatric Neurologists’ Attitudes and Practices Concerning SRH for WWE With ID.
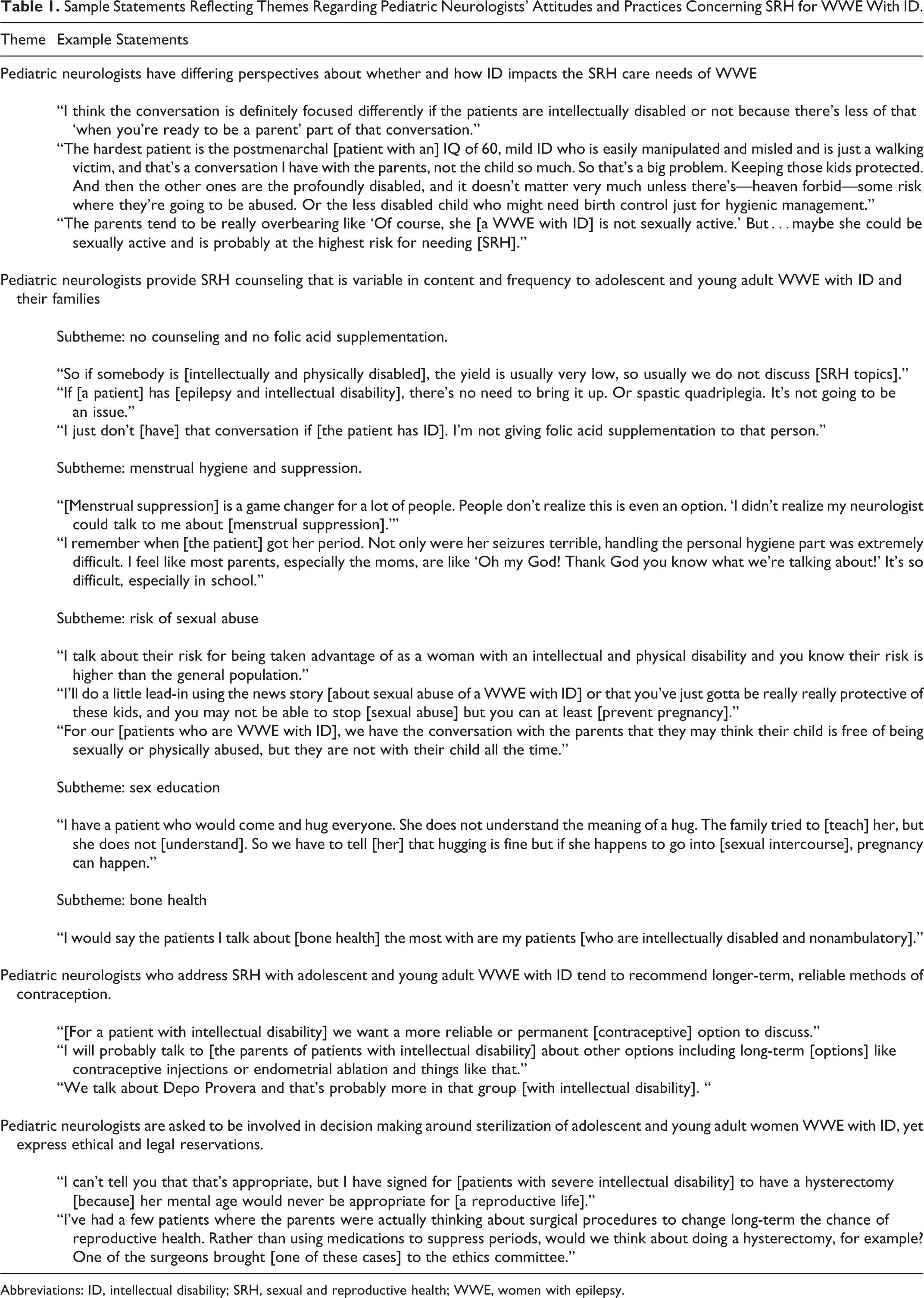
Abbreviations: ID, intellectual disability; SRH, sexual and reproductive health; WWE, women with epilepsy.
Theme 1. Pediatric neurologists have differing perspectives about whether and how intellectual disability impacts the sexual and reproductive health care needs of WWE.
Participants expressed conflicting perspectives regarding whether adolescent and young adult WWE with intellectual disability are capable of engaging in sexual relationships and parenting because of their cognitive status. Participants’ perceptions of their patient’s capabilities influenced whether and how they would provide sexual and reproductive health care. As one said, “If you know that the patient is significantly delayed where they’re not going to have a reproductive life, you do not touch on [SRH] with those families.” Another said, “There’s less preparation for the ‘When they will get pregnant?’ We know that she’s not going to be a parent, so we can change the medicines that we would think about using [referring to teratogens].”
Although most participants endorsed this viewpoint, a minority expressed a different perspective. One reflected that he might be erroneously assuming that WWE with intellectual disability are not capable of volitional sexual activity: “It’s not to say that somebody with intellectual disability couldn’t make a conscious decision to become sexually active. Of course they could. I probably don’t talk about that in the ways that I could. I probably focus a little bit more on the issue of being taken advantage of but maybe that’s another area where I could improve.”
Theme 2. Pediatric neurologists provide sexual and reproductive health counseling that is variable in content and frequency to adolescent and young adult WWE with intellectual disability and their families.
Compared with their practices with typically developing WWE, several participants reported that they do not ever provide sexual and reproductive health care to WWE with intellectual disability. As one said, “There’s no need to bring [SRH] up. It’s not going to be an issue.” Another said, “I just don’t [have] that conversation if [the patient has ID]. I’m not giving folic acid supplementation to that person.”
Other participants, in contrast, described with great enthusiasm providing counseling about sexual and reproductive health to this patient population on many topics that they do not usually discuss with typically developing WWE. When asked how often such conversations occur, some participants reported that they discuss sexual and reproductive health at every health care visit. Several participants discussed menstrual hygiene as a critical area to discuss with this population. As one physician said, “I had a patient who wasn’t even going to school for the entire week that she had her period because she had heavy periods and she has an IQ of 40. She just didn’t handle the whole personal hygiene part well. So I’m like, ‘No, this is not acceptable. No girl should be missing school because she has her period.’”
Some participants noted the importance of providing anticipatory guidance about the risk of sexual abuse faced by WWE with intellectual disability. As one neurologist said, “I try to get a sense of how much of the day the kid is unsupervised. There are children who get taken advantage of…I really do want to know how often they are with responsible adults and how much time they spend alone with their classmates.” Another emphasized the challenge of addressing this topic with families: “Parents don’t want to hear the ugly bad things that could happen if you have a nonverbal adolescent living in a group home or taken care of by someone during the day.”
Several participants incorporated basic teaching points on sex education into their counseling on sexual and reproductive health for WWE with intellectual disability. As one neurologist said, “This may sound a little maternalistic.…But I’ll ask them if they have a boyfriend. And if they say yes…I have said, ‘Do you and your boyfriend want to have babies, and do you know how babies are made?’ And then if the answer is no, then I say, ‘Then I think you probably need to have some talking with your mom.’”
Many participants who reported conducting more extensive sexual and reproductive health counseling with this population also counseled on decreased bone density, particularly with patients with reduced mobility. As one said, “I’ll mention [bone health and] I’m much more aggressive talking about [it] in the non-ambulatory patients.”
Implicit throughout interviews with pediatric neurologists who both do and do not discuss sexual and reproductive health with this population was a sense of discomfort in broaching sexual and reproductive health topics during clinical visits with WWE with intellectual disability, and a concern that caregivers might be uncomfortable as well.
Theme 3. Pediatric neurologists who address sexual and reproductive health with adolescent and young adult WWE with intellectual disability tend to recommend longer-term, reliable methods of contraception.
For WWE with intellectual disability, participants most commonly discussed contraception for menstrual hygiene, though also occasionally for pregnancy prevention. As one participant said, “I usually discuss [contraception], like how well they’re able to take care of their period…and in case of any mishappening and they get pregnant.”
When discussing contraception for this population, many participants expressed that they recommend longer-term, reliable methods. By contrast, in our broader study, participants more frequently reported discussing oral contraceptive pills with WWE with typical development. 12 In particular, depot medroxyprogesterone acetate (Depo-Provera injection) was the most preferred method for several participants for WWE with intellectual disability. As one said, in a perspective echoed by many participants, “I usually talk to [children with intellectual disability] about the Depo shot.”
Some participants preferred long-acting reversible contraception (LARC) for these patients, such as the intrauterine device (IUD) or intradermal implant. As one said, “The first thing [I bring up with this population] is Nexplanon.…Nexplanon is pretty easy to use and works pretty well.” However, others expressed ethical reservations about LARC: “Generally, I think putting an IUD in a [child with intellectual disability] who might not be able to consent is a little gray.” None discussed considering concerns about hormonal methods or interactions with antiseizure medications in recommending a contraceptive method.
Theme 4. Pediatric neurologists are asked to be involved in decision-making around sterilization of adolescent and young adult WWE with intellectual disability, yet express ethical and legal reservations.
Several participants brought up that they had been asked to be involved in decision making around potential sterilization via hysterectomy for WWE with intellectual disability, ranging from being asked their opinion to being asked to facilitate the process or sign legal documentation approving sterilization. However, when the topic of sterilization arose, participants invariably expressed ethical and legal concerns. As one said, “I’ve been part of the signature to the juvenile court that it’s appropriate for this woman to have a hysterectomy.…The courts want [signatures] from multiple physicians because they don’t want it blowing back in their face that here they are sterilizing [women with intellectual disability].” Another said, “Parents [have asked], ‘Would we think about doing a hysterectomy?’ […] I’ve had one patient who was [under 18 years old] and whose parents brought the issue up and we actually ended up discussing it as part of the ethics committee.” Another participant expressed their concerns about sterilization thusly: “That started a whole ethical issue for us as neurologists. Could we support that or not?”
Discussion
Pediatric neurologists have reported challenges with sexual and reproductive health care provision for adolescent and young adult WWE with typical development. 12 This study reveals that their attitudes and practices regarding sexual and reproductive health care for WWE are further complicated when their patients also have intellectual disability. Pediatric neurologists reported wide-ranging, conflicting opinions and practices regarding sexual and reproductive health care for adolescent and young adult WWE with intellectual disability. They were conflicted regarding (1) whether these individuals are capable of volitional sexual activity and parenting, and whether they even have sexual and reproductive health care needs; (2) whether and how much to counsel this patient population about sexual and reproductive health; (3) the most appropriate and ethical contraceptive method for this population; and (4) whether or not it is appropriate for pediatric neurologists to be involved in decision making around sterilization, with some having already participated in this process. Our research group recently also conducted a survey of child neurologists subsequent to this qualitative study. Findings supported provision of suboptimal sexual and reproductive health care to both WWE with and without intellectual disability, and generally lower rates of provision of sexual and reproductive health care to WWE with intellectual disability compared to WWE without intellectual disability. 17
Several participants tied their perception of a patient’s capacity for a volitional “reproductive life” to their sexual and reproductive health care needs, which ignores many potential concerns. The legal standard for capacity for sexual consent is controversial, and women with milder intellectual disability may meet the standard for capacity for sexual consent in some US states. 18 Consequently, some women with milder intellectual disability could engage in legally consensual sexual relationships and childbearing. However, women with intellectual disability are also at increased risk of sexual abuse and therefore unintended pregnancy. 9 As pediatric neurologists treat a large population of WWE with intellectual disability, they might benefit from clinical guidelines and additional training around the sexual and reproductive health care needs of this population.
Our findings raise questions regarding the scope of practice of a pediatric neurologist for adolescent and young adult WWE with intellectual disability regarding sexual and reproductive health. Although refraining from any sexual and reproductive health counseling is potentially insufficient, it is not clear that all pediatric neurologists would agree that the extensive counseling offered by some participants, such as discussion of menstrual hygiene, sexual abuse prevention, sex education, and bone health, is within their scope of practice. Better systems of collaboration between neurologists, primary care physicians, and women’s health providers may ensure that patients’ comprehensive needs are met.
One caveat to collaboration with other specialties is that primary care pediatricians have also been shown to provide suboptimal sexual and reproductive health care to adolescent women with intellectual disability. 13 Although there are no existing data on how women’s health providers serve adolescent and young adult women with intellectual disability, obstetrician-gynecologists have reported feeling poorly trained and providing disparate services to adult women with intellectual disability. 19 More training in sexual and reproductive health care for women with intellectual disability is needed for other subspecialties as well.
Controversy exists as to what extent pediatric neurologists should be involved in contraceptive decision making. Participants reported recommending contraception for WWE with intellectual disability for pregnancy prevention and menstrual hygiene. There are ethical issues regarding menstrual manipulation in patients with intellectual disability who cannot consent. The American Academy of Pediatrics cautions against menstrual manipulation for caregiver convenience or hygiene as opposed to dysmenorrhea or heavy bleeding. 20 However, the American College of Obstetrician-Gynecologists (ACOG) expresses that the reasons for menstrual manipulation should be evaluated on a case-by-case basis. 21
The most prescribed method of contraception for menstrual suppression for adolescents with disabilities is oral contraceptive pills. 22 This method was less common among our sample, as more expressed a preference for depot medroxyprogesterone acetate (Depo-Provera injection), consistent with reports that women with intellectual disability are prescribed this method at significantly higher rates than the general population. 22 -24 The reasons for this preference are unclear but may relate to greater convenience than daily medication and desire to achieve amenorrhea. 20 Guidelines regarding women with intellectual disability recommend caution with this method given concerns about bone health and weight gain for patients with limited mobility. 20,21
LARC is less frequently provided to women with intellectual disability, though the reasons are unclear. 22 Some providers expressed a preference for LARC for WWE with intellectual disability. IUDs have been shown to be effective and well tolerated in adolescents with disabilities. 25 However, a minority expressed ethical reservations about LARC placement in women who cannot consent. There are currently no guidelines from national or international medical organizations that caution against LARC use in women with intellectual disability. 20,21
Several neurologists mentioned that their opinion or legal signature was sought regarding sterilization of WWE with intellectual disability. In the United States in the nineteenth and twentieth centuries during the eugenics movement, people with intellectual disability were forcibly sterilized. 26 The World Health Organization and United Nations have identified forced sterilization of people with disabilities as discriminatory and unethical. 26 Presently, there are legal safeguards in multiple US states regarding the sterilization of minors and people without capacity to consent. 20,26 ACOG recommends that sterilization should only be considered if standard indications are met and reasonable alternatives have been attempted. 21 However, some authors have argued that sterilization should still be considered as first-line in women with intellectual disability. 27,28 Rates of sterilization of women with intellectual disability remain higher than peers’, and sterilization occurs at younger ages compared with peers. 29 No practice guidelines are available to pediatric neurologists regarding sterilization, contributing to the lack of clarity about the neurologist’s role.
Clinical practice guidelines might clarify the scope of practice of pediatric neurologists regarding sexual and reproductive health care for adolescent and young adult WWE with intellectual disability. The conflicting opinions and practices expressed in these interviews suggest that pediatric neurologists might benefit from guidelines on sexual and reproductive health care for WWE that are tailored to patients’ ages and development. The Child Neurology Foundation advises annual anticipatory guidance on sexual health by pediatric neurologists for adolescents appropriate to age and developmental status. 30 These recommendations provide no specific guidance by disease or intellectual capacity. 30 The American Academy of Neurology provides a quality measure regarding WWE of childbearing age regardless of neurodevelopmental status. 31 Our interviews suggest that a more tailored guideline addressing developmental stage, disease, and cognitive status might be needed.
We believe optimal sexual and reproductive health care for adolescent and young adult WWE with and without intellectual disability would be tailored to the individual’s age, neurodevelopment, and cognitive status. In addition, providers should incorporate confidential care with patients cognitively able to engage in private discussions. The content of sexual and reproductive health discussions should encompass the topics advised in the American Academy of Neurology guideline and add consideration of sexual abuse prevention and prevention of sexually transmitted infections particularly for people with intellectual disability. Ideally, sexual and reproductive health care for this population should also involve active coordination between the neurologist and (where applicable) the primary care physician and/or reproductive health provider. We would also advise caution regarding neurologist involvement in providing medico-legal permission for sterilization of people with intellectual disability. We would recommend doing so only after thorough discussion about risks and benefits with the patient (where feasible) and/or caregivers, as well as the reproductive health provider performing the procedure.
This study has several limitations. First, qualitative research cannot provide information about the prevalence of participants’ practices, and instead aims to elicit a heterogeneity of perspectives. However, quantitative information about practices can be found elsewhere. 17 Second, participants most interested in this topic may have agreed to be interviewed. However, given that participants often endorsed suboptimal sexual and reproductive health provision, participation bias may not have compromised these findings.
Future research could quantify provider attitudes and practices through retrospective studies of medical record documentation, in addition to the aforementioned survey that relies on self-report. 17 Additional studies could better delineate differences in care for subsets of WWE with intellectual disability, such as WWE with mild vs moderate to severe intellectual disability, or with and without physical disabilities. Such research could examine differences between subgroups of pediatric neurologists (eg, by gender or between physicians and advanced practice providers), or between pediatric neurologists and adult neurologists who care for WWE with intellectual disability into adulthood and later in life. Although this study focused on health care professionals, future studies should also focus on the experiences and preferences of young WWE with intellectual disability and their caregivers regarding sexual and reproductive health to ensure optimally patient-centered sexual and reproductive health care delivery.
Conclusion
Pediatric neurologists have differing perspectives on whether and how intellectual disability affects the sexual and reproductive health needs of WWE, and report providing counseling variable in frequency and content to adolescent WWE with intellectual disability that is at times suboptimal. They also report ethical reservations about certain sexual and reproductive health practices such as sterilization. Better understanding of sexual and reproductive health care provision for WWE with intellectual disability would facilitate the development of clinical guidelines regarding best practices as well as interventions to improve comprehensive, patient-centered sexual and reproductive health care for this population.
Supplemental Material
Supplemental Material, sj-pdf-1-jcn-10.1177_08830738211041824 - Pediatric Neurologists’ Perspectives on Sexual and Reproductive Health Care for Adolescent and Young Adult Women With Epilepsy and Intellectual Disability
Supplemental Material, sj-pdf-1-jcn-10.1177_08830738211041824 for Pediatric Neurologists’ Perspectives on Sexual and Reproductive Health Care for Adolescent and Young Adult Women With Epilepsy and Intellectual Disability by Laura Kirkpatrick, Amy Collins, Elizabeth Harrison, Elizabeth Miller, Christina Patterson, Yoshimi Sogawa, Anne C. Van Cott and Traci M. Kazmerski in Journal of Child Neurology
Footnotes
Acknowledgments
We would like to acknowledge Miya Asato and Patricia K. Crumrine with assistance with recruitment for this study. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contributions
Laura Kirkpatrick contributed to study design, data collection, data analysis, interpretation, drafting and revision of the manuscript, and approved the final version of the manuscript Amy Collins contributed to data analysis, interpretation and revision of the manuscript, and approved the final version of the manuscript Elizabeth Harrison contributed to data interpretation and revision of the manuscript, and approved the final version of the manuscript Elizabeth Miller contributed to data interpretation and revision of the manuscript, and approved the final version of the manuscript Christina Patterson contributed to data interpretation and revision of the manuscript, and approved the final version of the manuscript Yoshimi Sogawa contributed to study design, data collection, data interpretation, drafting and revision of the manuscript, and approved the final version of the manuscript Anne C. Van Cott contributed to data interpretation and revision of the manuscript, and approved the final version of the manuscript Traci M. Kazmerski contributed to study design, data analysis and interpretation, drafting and revision of the manuscript, and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Ethical Approval
The University of Pittsburgh Institutional Review Board deemed this study exempt (no. 19040356).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.