
Abstract
Introduction
Epilepsy surgery is the most effective available treatment to eliminate or reduce seizure burden, decrease mortality rate, and improve quality of life in appropriately selected people living with drug-resistant epilepsy (DRE).1–3 Despite accumulating evidence for the benefits of surgery, people living with epilepsy (PWE) often fail to receive this care.4,5 According to one study, only approximately a quarter of Americans with DRE were evaluated in a comprehensive epilepsy center, and only about 1.5% to 3% of epilepsy surgery candidates ultimately underwent surgery. 6 Further, the small percentage of PWE who ultimately undergo epilepsy surgery experience extended delays with substantial variability.7,8 This unfortunate treatment gap in epilepsy surgery is secondary to a broad range of issues, including patients’ and families’ fear, anxiety, and misconceptions regarding epilepsy surgery - grounded in individual, family, and socioeconomic factors and further exacerbated by communication barriers with physicians. 9 Decision-making in epilepsy surgery involving children is further complicated as the primary decision-makers are caregivers and not the patients. 10 Many studies explored patient values that guide surgical decision-making, but a patient's decision to pursue epilepsy surgery is closely dependent on their physicians’ knowledge, attitude, and perception about surgical treatment.11–28
Understanding physician-patient communication about epilepsy surgery- a central and critical factor toward increasing surgery utilization- can be complex, as patients with DRE receive care from a wide range of health care professionals, including neurologists, epileptologists, and neurosurgeons. Physicians’ role in epilepsy surgery decision-making has not been adequately explored, and only a limited number of studies utilizing survey instruments report physician-specific barriers, which include identifying patients with DRE and referring promptly to a higher level of care, selecting appropriate candidates for surgery, discussing risks and benefits of various surgical options, and providing individualized counseling.29–36 As a result, we have a limited understanding regarding physicians’ approach to discussing surgical options for epilepsy, engaging patients and families in a complex conversation about surgical treatment, presenting risks and benefits of surgery, and fostering shared-decision making. Additionally, existing studies have not explored complex decision-making challenges physicians encounter when developing active collaboration with patients and families to arrive at the best treatment option, including epilepsy surgery, and none have qualitatively assessed differential perspectives of providers of the same specialty regarding epilepsy surgery.
To gain a deeper and refined version of physicians’ current counseling approach during the presurgical discussion regarding epilepsy surgery and understand the physicians’ perspectives behind the differential approaches to epilepsy surgery, we conducted detailed qualitative semi-structured interviews among physicians (neurologists, epileptologists, and a neurosurgeon) from a National Association of Epilepsy Centers Level 4 epilepsy center.
Methods
Design
We conducted qualitative semi-structured interviews for an in-depth assessment of the perspectives of physicians (regularly involved in the care of children with epilepsy) regarding presurgical discussion with patients and families.37–39 The University of Arkansas Medical Sciences (UAMS)IRB approved this study (Ref IRB 261387).
Setting
Physicians from the Arkansas Children's Hospital's (UAMS College of Medicine faculty members) comprehensive epilepsy center were selected for the study. The Arkansas Children's Hospital is the only pediatric healthcare system in Arkansas and a Level 4 epilepsy center.
Sample
We utilized purposive sampling with an aim for the diversity of the study population regarding experience managing children with epilepsy, conducting evaluations for epilepsy surgery, and having subspecialty exposure and training specifically for epilepsy. 40 Only academic clinicians were included, and data saturation was reached after 11 (5 neurologists, 5 epileptologists, and 1 neurosurgeon) interviews. 41 Characteristics of physicians are shown in Table 1.
Characteristics of Physicians.
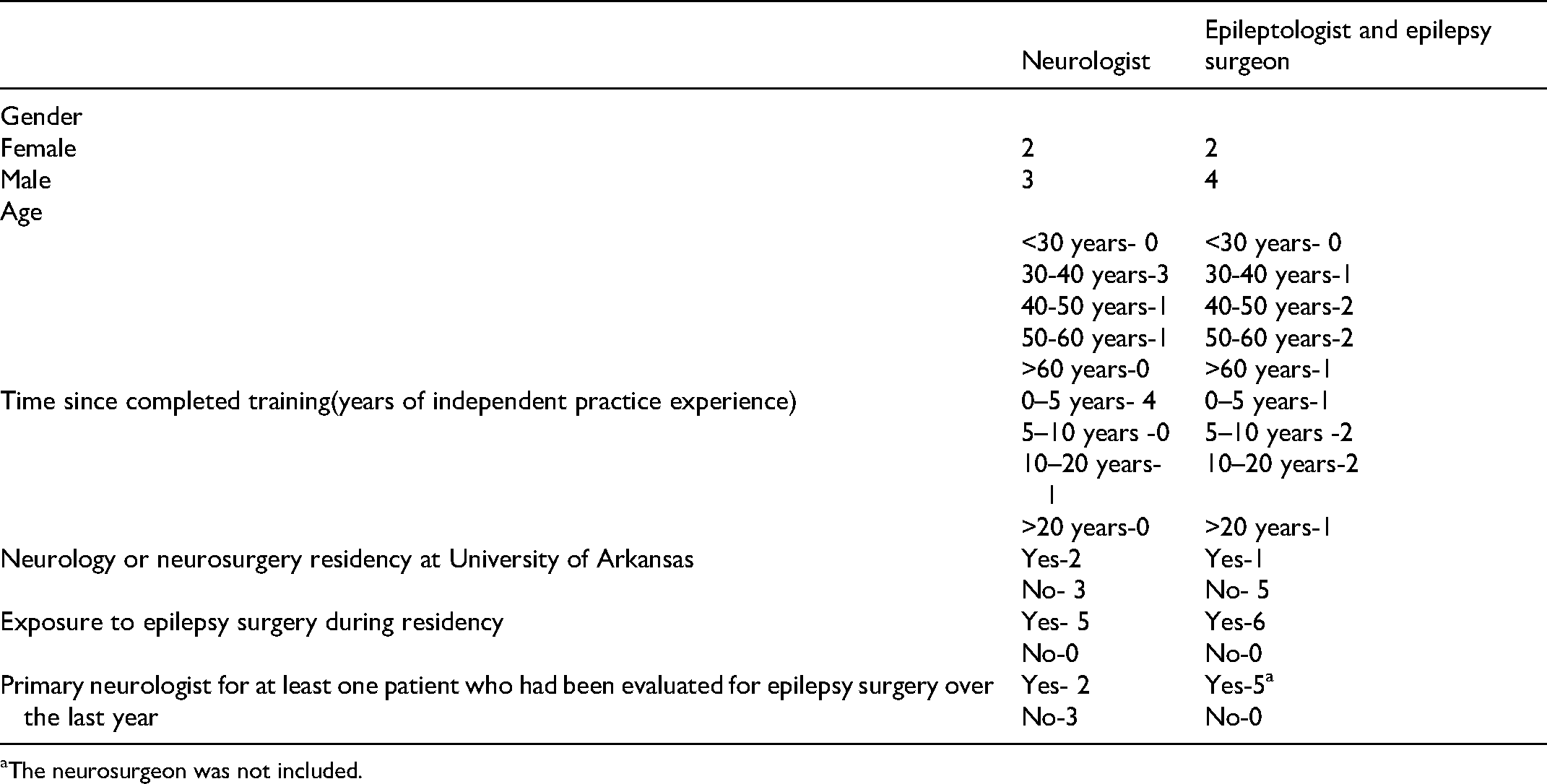
The neurosurgeon was not included.
Interview Guide
This study is part of a larger implementation research project to develop and tailor implementation strategies to reduce the epilepsy surgery treatment gap.42,43 The implementation study team developed the interview guide with further revision during the study period to explore emerging themes. 44 The interview guide was designed to explore how physicians communicate and pursue surgical decision-making in patients with DRE. Through open-ended questions with prompts, we interviewed clinicians about the surgical management for DRE based on multiple clinical examples to explore their willingness or reluctance to consider epilepsy surgery. The participants were also asked, “What are the potential benefits and risks of epilepsy surgery? When do you discuss epilepsy surgery with the patient? How do you discuss options in cases with uncertainty? How do you respond when families express a preference not aligned with your conclusion? Do you use any resources to help with shared decision-making and patient-and family education?”
Recruitment and Data Collection
All clinicians that were approached agreed to participate in the discussions. No monetary incentive was offered. We conducted the interviews face-to-face in a private setting convenient for the participants, between July 21, 2020, to August 21, 2020. The average duration of the 11 interviews was 45 min (range 20-95 min). The discussions were audio-recorded and then transcribed verbatim. Identifying information was deleted from the transcripts.
Data Analysis
To begin, we used deductive qualitative content analysis to answer our research questions about presurgical discussion, shared decision-making, and instruments to facilitate discussions, based on a few set codes identified from prior studies. 45 Next, we implemented inductive thematic analysis to identify and report patterns outside of our a priori determined codes to ensure we capture the full breadth of physicians’ perspectives. 45 Data were coded independently by three researchers (DS, VE, and MH), who met regularly to discuss/refine emerging analyzes. Two research team members (DS and MH) reviewed each transcript to ensure a consistent coding process. Initial disagreements in coding were resolved at a series of team meetings. Open coding was followed by axial and sequential coding, in which the initial list of codes was reviewed, grouped, and refined with multiple iterations. 46 Significant statements attached to the themes were included for robust characterization of perceived patterns in the words of the participants. Analytic impressions were presented to the participating clinicians for a member check-in. To further expand the validation and generalizability of the data and interpretations, a group of experts of the surgical subgroup of the Pediatric Epilepsy Research Consortium (PERC; a national collaboration of more than 40 pediatric epilepsy programs in the United States) was consulted for feedback regarding the agreement with the themes applicable in diverse settings.
Results
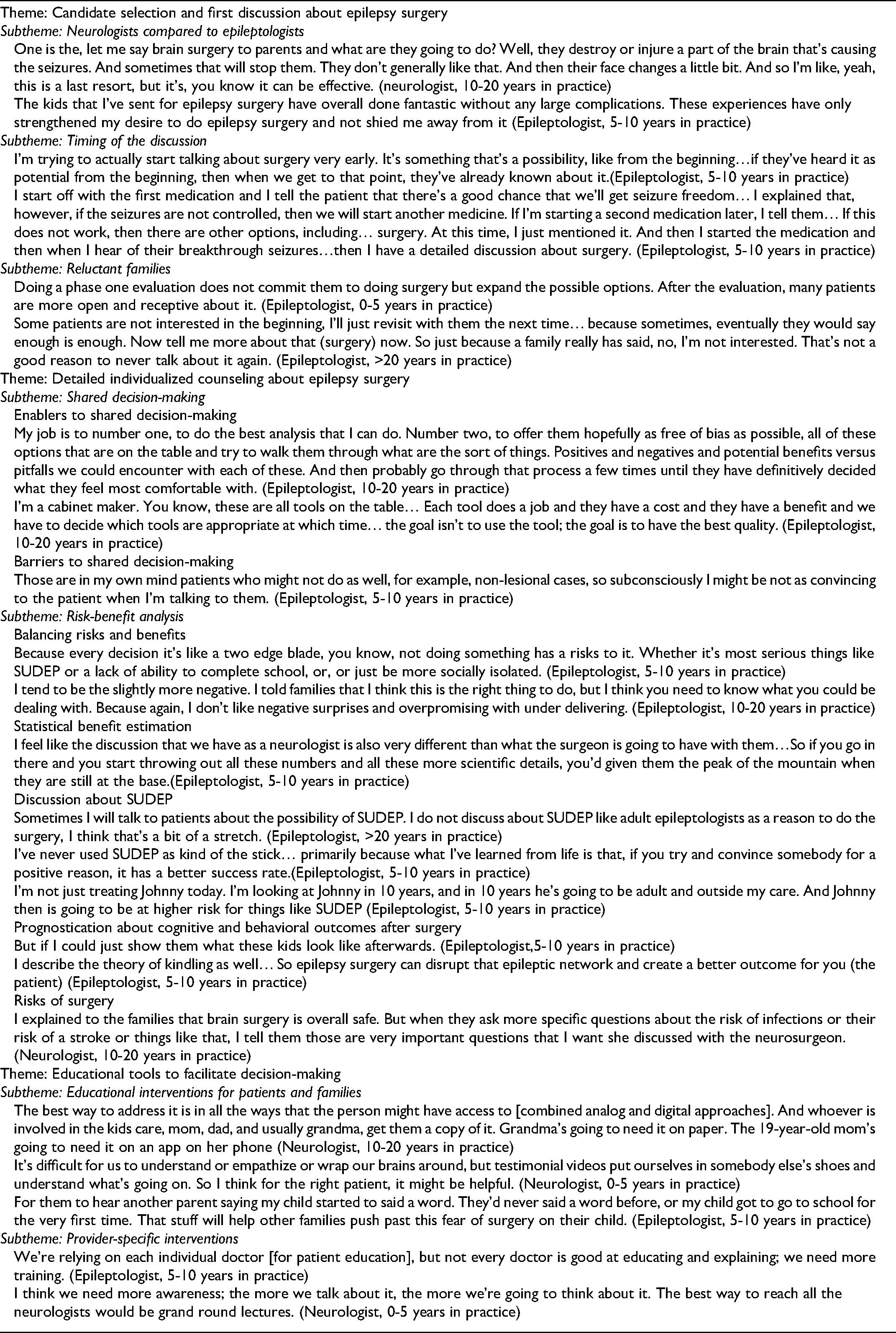
Three themes (noted in
Physician Reported Themes with Exemplars on Presurgical Discussion and Shared Decision-Making in Epilepsy Surgery (N = 11).
Neurologists Compared to Epileptologists
Both neurologists and epileptologists had a general agreement about the diagnosis of DRE following the ILAE definition. 47 However, they had distinctive perspectives in selecting candidates for surgical evaluation. Neurologists primarily considered patients with lesional intractable epilepsy as candidates for surgery and were ambivalent about nonlesional patients. Epileptologists appraised a broader pool of patients suitable for presurgical workup, including extratemporal epilepsy, nonlesional epilepsy, hemispheric epilepsy, as well as palliative surgeries for generalized epilepsy. Few epileptologists also considered surgical options for multifocal epilepsy after quantifying seizures with a determination of predominant focus. However, epileptologists also highlighted that they would only consider surgical options in complex cases if noninvasive diagnostic modalities generate a reasonable surgical hypothesis. Epileptologists and the neurosurgeon were open to exploring surgical options for epilepsy even if the epileptogenic focus overlaps the eloquent cortex, except involvement of the critical language area. However, they expressed less enthusiasm about surgery in children with severe intellectual disabilities.
Both neurologists and epileptologists reported difficulty initiating discussions with families about epilepsy surgery. Neurologists disclosed experiencing more resistance from families during conversations related to surgery, forcing them to continue medical therapy. Some neurologists had a more ambivalent attitude about epilepsy surgery and were concerned if epilepsy surgery is sometimes ‘oversold.’ They also struggled to bring up surgical options consistently. Many of them had prior experience referring patients for surgery or caring for them afterward, but they were not involved in the complete evaluation process. Thus, the neurologists preferred families to discuss surgery with epileptologists and neurosurgeons. However, the neurologists felt difficult conversations related to epilepsy surgery are not unique and gave examples of challenging interactions from their subspecialty field.
Epileptologists reported more confidence discussing epilepsy surgery and hold a more favorable attitude toward surgery. They were more willing to discuss the curative potential of surgical therapy and expressed understanding that detailed discussion regarding surgery might be difficult for neurologists. The decision-making process was streamlined when patients were specifically referred for surgical considerations. However, some epileptologists encountered ‘shocked and upset’ families during the initial conversation as surgical options were not discussed previously by the treating neurologist(s). The epileptologists reported ‘being on the same page’ regarding the content of their counseling but reported differences in styles and assertiveness. However, several experts felt frustrated that an aggressive approach to presurgical workups had not ‘dramatically moved the numbers’ and mentioned the importance of not narrowly focusing on epilepsy surgery but instead to ‘push people toward the therapy with the highest possibility of improving the outcomes’. Several epileptologists were also concerned that they might not be as effective in discussing surgical options if they had a preconceived bias for less than the optimum outcome for an individual patient based on patient or epilepsy characteristics (multifocal or nonlesional epilepsy).
Timing of the Discussion
Participating clinicians did not have a consensus on when to broach the concept of epilepsy surgery. Some physicians wanted to broadly discuss different treatment options-including epilepsy surgery- after a confirmed diagnosis of epilepsy or during the first anti-seizure medication (ASM) initiation. Epileptologists were more willing to discuss epilepsy surgery earlier in the disease course. However, these physicians were also concerned whether discussion about surgery would induce more anxieties for the families. To mitigate unnecessary stress, these physicians included epilepsy surgery as one of the many treatment options to consider in the future if epilepsy becomes intractable to medical therapy. Several physicians reported avoiding epilepsy surgery discussion until the failure of the first ASM, especially if the patients did not have a form of epilepsy likely to be pharmacoresistant. All physicians agreed about a detailed conversation about epilepsy surgery after the failure of two appropriate treatment trials.
Reluctant Families
Physicians noted that some families were initially resistant to the concept of epilepsy surgery. They had not noticed any particular racial/ethnic distribution among reluctant families but hypothesized lower socioeconomic and educational status might be associated with more resistance toward surgery. Physicians were empathetic about commonly noted fear and anxiety linked with brain surgery among patients and caregivers and willing to offer other treatment options. If families did not want to pursue surgery, the physicians were hesitant to discuss surgical options. They were concerned that ‘pushing too hard’ might backfire and make families more resistant to surgery. Instead, they emphasized building trust and rapport with the family to understand families’ values and priorities better. None of the physicians reported utilizing motivational interviewing techniques; however, most physicians successfully negotiated with families to complete the presurgical workup. They noted that many families became more open and receptive later and decided to pursue surgical therapy. They also remarked on the importance of ‘revisiting surgical options’ with these families as many families reconsidered surgical options when seizures remained uncontrolled or worsened.
On the other hand, they noted that some families continued to have unfounded expectations about newer ASMs, alternative nonsurgical therapies, or experimental treatment options available in research trials. One epileptologist underscored the importance of counseling families about possible recurrence and reconsidering surgery if the patient with DRE enjoyed better seizure control for some time due to the dynamic nature of the disease. Some physicians also reported that many families were resistant to undergo the complicated process of presurgical diagnostic workup and required significant explanation of the utility of going through a long and complex process. Most epileptologists were confident in their ability to persuade most families to undertake diagnostic testing. They did notice, however, that reticent families were more likely to abandon the workup by failing to show up for appointments or leaving the monitoring unit before seizures were recorded.
Shared Decision-Making
Enablers to shared decision-making
Primarily the epilepsy surgeon and epileptologists discussed shared decision-making processes for surgical therapy and were noted to have a robust supportive attitude for collaborative decision-making. They indicated the importance of a detailed conversation about ‘positives and negatives and potential benefits versus pitfalls of surgery and other alternative treatments’ due to the preference-sensitive nature of the elective surgical treatment. The specialists also reported ‘probably going through that process a few times until they have definitely decided what they feel most comfortable with.’ Several specialists highlighted physician-family partnerships, with physicians bringing expertize in discussing diagnosis and treatment options (including surgery), defining risks and benefits of each option, and counseling regarding prognosis. In contrast, children and caregivers become experts in values, risk tolerance, preferences, and social contexts during collaborative decision-making. Some reported utilizing option listing for patients and families to compare various options through the lens of their values and goals rather than pushing for epilepsy surgery. Several epileptologists wanted to involve the older children in the decision-making process.
Barriers to shared decision-making
Most participants expressed the importance of providing clear, accurate, and unbiased medical evidence about all the options. Still, some disclosed the need for additional expertize and training in communicating and tailoring that evidence to the patients and families. Some epileptologists acknowledged that they might be biased while providing treatment options based on the intuitive assessment of an individual's epilepsy. Some experts used ‘framing and refocusing’ of the possibilities when they repeated the benefits of surgery at the end (that they would personally opt for) to reinforce the benefits of surgery. Some participants were concerned that providing too much information may overwhelm or confuse families. Some clinicians adopted a paternalistic role or modified conversations to facilitate decision-making. Another neurologist noted that some families want to be informed about options but leave decision-making to the physicians “if it was your child, what would you do"? None of the participants discussed team-based discussions (utilizing nurses, care coordinators, social workers) or formal online or phone-based counseling in the shared decision-making process.
Risk-Benefit Analysis
Balancing risks and benefits
The best-individualized decision is less specific in many cases of pediatric epilepsy: clinical equipoise of risks and benefits of surgery and decision-making requires balancing a different set of values and goals for each patient. One epileptologist described showing a pathway for the family to optimize quality of life. Another participant emphasized the importance of setting up realistic expectations of surgery. Both neurologists and epileptologists discussed with families about several potential benefits of epilepsy surgery: seizure freedom, seizure reduction, reduction of medicines. Experts were conservative about ASM withdrawal after surgery but sensitive to the information that weaning of ASM or dose reduction may improve the child's cognitive development - a significant motivation for surgery for many caregivers. Several participants highlighted knowing family well and tailoring the discussion according to family's education and interest. The cumulative risk of conservative therapy was expressed more by specialists compared to neurologists.
Statistical benefit estimation
Epileptologists discussed using statistics of seizure-freedom to discuss surgical benefits, primarily citing data from adult temporal lobe surgical series. Most epileptologists were aware of randomized control studies regarding temporal lobe surgery in adults, but none used pediatric epilepsy-surgery-specific statistics during counseling. They were also mindful of the problem of translating adult-specific data for children, who have a higher incidence of extratemporal and hemispheric epilepsies. However, some stressed the importance of not focusing on the numbers with the family early on, which may overwhelm the family and deter them from seeking further evaluation. They instead wanted to have the surgeon discuss those numbers with the family. One participant also noted many families wanted to know about the change in functional ability more than these statistics.
Discussion about sudden unexpected death in epilepsy (SUDEP)
Epileptologists did not discuss SUDEP in the context of epilepsy surgery; however, some discussed SUDEP to improve medication adherence. Some physicians were uncomfortable bringing up SUDEP in the discussion for fear of frightening the family. One specialist remarked discussing SUDEP as a reason for doing epilepsy surgery might be a ‘bit of a stretch.’ One pediatric epileptologist reported that his adult colleagues might discuss this more with their patients to motivate them for surgery. Another subject remarked with a metaphor of “carrot and stick” that convincing somebody with a potentially positive effect may have a better success rate (improving quality of life rather than reducing the risk of dying). However, one specialist discussed SUDEP prevention in the future (when the patient becomes an adult) as a provoking factor to motivate families for epilepsy surgery.
Prognostication about cognitive and behavioral outcomes after surgery
All epileptologists and some neurologists reported the need for an extensive discussion about cognitive and behavioral outcomes(both positive and negative) of surgery. Epileptologists expressed frustration due to the inability to provide precise prognostication related to cognitive outcomes, which can be a primary motivator for many caregivers to proceed to surgery. Experts were disappointed that published studies about cognition following surgery were not directly applicable in most situations due to heterogeneous patient populations and various factors unique to each patient. They noted that rather than scores (commonly reported in studies), parents wanted to have information regarding improvement in meaningful daily living skills. Many epileptologists discussed their practice of discussing potential progress in cognitive development following surgery ‘by disrupting the epileptic network’ in patients with epileptic encephalopathy secondary to a focal brain lesion.
Similar to cognitive outcomes, physicians frequently faced questions regarding behavioral prognosis following surgery. Physicians expressed understanding that often, behavioral difficulties associated with autism spectrum disorders, disruptive behaviors, attention-deficit hyperactivity disorder, depression, anxiety, psychosis are more intimately related to health-related quality of life rather than seizures by themselves. However, they felt not having much evidence to provide quality presurgical counseling regarding behavioral changes following surgery. They also noted that behavioral difficulties might be unmasked after successful epilepsy surgery causing challenges. Additionally, some families may have problems adjusting to life after surgery as chronic disability changes to sudden wellness.
Risks of surgery
Both neurologists and epileptologists agreed that epilepsy surgery is an ‘overall safe procedure’ with a risk of major complications being about 1% to 2%. Some epileptologists discussed the risk of neurological deficits with families based on the potential epileptogenic zone overlapping with nearby eloquent cortex but mostly wanted the neurosurgeon to discuss other possible major and minor complications associated with any epilepsy surgery. The neurosurgeon reported comprehensive discussions - including numerical probabilities of various complication rates - with patients and families. The neurosurgeon also noted that families appreciated information regarding the expected recovery period, including rehabilitation. He also stressed the importance of comprehensively answering all questions (some of which might be perceived as trivial for the context, such as how much hair to be shaved or the appearance of the incision afterward) prior to surgery.
Educational Interventions for Patients and Families
Both neurologists and epileptologists discussed patient-facing educational interventions to improve surgical counseling and decision-making. The majority of the participants wanted to have combined analog (written information in the physician's office, handouts, large charts in the examination and waiting rooms) and digital tools (downloadable apps or URLs of relevant websites, webinars, podcasts) for patient education. All participants agreed that patient testimonial videos would be the most effective method for easing family worry, especially if the video included the treating team discussing the patient's journey to epilepsy surgery. Several physicians also recommended judicious use of social media posts to provide support, information, and resources for potential patients and families. Although many clinicians discussed option-listing for offering patients various choices, none of the participants mentioned using a decisional aid to facilitate shared decision-making.
Provider-and Organization-Specific Interventions
All physicians endorsed further physician-specific education and training in effective communication, shared decision-making, and care planning. Some commented that not all physicians are good communicators and would benefit from patient-centered communication training. Some physicians wished to learn more about epilepsy surgery by attending lectures and case presentations that detailed the patient's disease course, surgery, and outcome. Some also reported that they preferred learning from clinical experience rather than via lectures. Most participants were interested in learning about online decision-support tools to identify surgical candidates or using statistical tools such as nomogram or scoring algorithms to estimate the likelihood of seizure freedom or complication after surgery, but none were using these in their practice due to practical problems, including the non-user-friendly interface of various tools. Similarly, participants were interested in having specific toolkits designed within the electronic health records (EHRs) to facilitate structured clinical documentation and support clinical decision making but remained doubtful about the successful implementation of these tools. According to both neurologists and epileptologists, effective communication between the two groups, accelerated referral processes through a specialized interdisciplinary surgery clinic, and the availability of an epilepsy care coordinator can aid with the decision-making process.
Discussion
We highlight several differences in approach to epilepsy surgery counseling between general neurologists and epileptologists. Most physicians are cautious about discussing surgical options and deliberate significantly about the best timing to initiate talks to prevent causing stress in families. Despite general agreement about the diagnostic criteria of DRE, awareness of the benefit of surgery in appropriate patients, and supportive attitude for collaborative decision-making for surgery, the neurologists consider surgery for a narrower pool of candidates with lesional epilepsy, hold a more ambivalent attitude toward surgery, struggle to bring up surgical discussion consistently, and face greater resistance from families after suggesting surgical options. Conversely, epileptologists were concerned about static surgical outcomes despite the availability of newer diagnostic tools, preconceived bias in selecting surgical candidates, and challenges associated with cognitive and behavioral outcome prediction following surgery.
Although no previous studies explored the physicians’ perspectives behind the differential approaches to epilepsy surgery and complex challenges associated with shared decision-making, a limited number of studies utilizing survey instruments report physician-specific barriers related to epilepsy surgery.29–36 Previous studies showed that neurologists were more likely to refer lesional temporal lobe epilepsy patients than nonlesional and presumed extratemporal onset patients.32,33 Prior studies also showed only half to three-quarters of neurologists had sufficient knowledge regarding the role of epilepsy surgery.29,30 A study among Canadian neurologists reported that only 43.4% of participants correctly identified the need for referral in DRE with ongoing seizures, and 54.1% recognized the need to refer these patients promptly. 34 Regarding attitudes toward epilepsy surgery, an Italian study demonstrated that neurologists had a neutral attitude compared to epileptologists who had a more positive and unified approach toward epilepsy surgery. 36 A Swedish study also reported that epileptologists had a favorable attitude toward surgery except in patients with severe intellectual disability. 35 Positive attitudes may be related to increased knowledge about epilepsy surgery, as noted in a study among neurologists in Saudi Arabia. 29 Other physician-specific factors correlated with a positive attitude toward epilepsy surgery are exposure to a higher volume of patients with epilepsy, previous experience of surgical referral, training in specialized programs with exposure to epilepsy surgery, and formal instruction in epilepsy subspecialty.30,34,36 However, a separate study showed that epileptologists might also have a significant implicit bias in selecting surgical candidates. 48 Besides variability of knowledge and attitude among clinicians, previous studies also reported challenges associated with shared decision-making, including deficient communication practices between physicians and patients, including discussion regarding the risks and benefits of the surgery. 9 For example, a study in Michigan, USA, reported that 41% of neurologists did not provide surgical outcome information to patients, more commonly in patients with extratemporal lobe epilepsy. 32
There are limitations to our study. Interviews provided physicians’ perspectives only without direct field observation of physician-patient communication during clinical encounters. The other major limitation of the study is it recruited neurologists and epileptologists from a single pediatric epilepsy center from a primarily rural, southern state in the USA. In comparison to the epileptologists in the study, the neurologists were younger and had less clinical experience. Additionally, all participants were academic clinicians and part of a comprehensive epilepsy program. Therefore, the study findings may not reflect views of private practice neurologists or academic neurologists not attached to an epilepsy center. Additionally, this study represented a small sample (as is the practice in qualitative research). 49 For a more comprehensive assessment of healthcare professionals’ challenges and views about epilepsy surgery, recruiting physicians of broader backgrounds (including primary care physicians) and diverse experience beyond one epilepsy center could be beneficial. However, we consulted a group of epilepsy experts from various settings (members of the surgical subgroup of the PERC) to confirm the generalizability of the themes of our study in different contexts.
Despite these limitations, the study highlights the nuanced perspectives of the pediatric epilepsy providers regarding surgical counseling for epilepsy, presenting risks and benefits of surgery, overcoming resistance to surgery, and fostering shared decision-making with patients and families. Our results also provide evidence that physicians, including epileptologists, do not agree on when to broach the concept of epilepsy surgery and how to pursue surgical options for reluctant patients and families. The physicians in our study recommended patient and physician-focused education, training, and tools (decision aids) to facilitate shared decision-making and presurgical risk-benefit analysis. Physicians should start receiving epilepsy surgery-specific education during residency training. A competency-based educational curriculum (for example, EpiEd curriculum, which has seven competencies and seven learning objectives specific to epilepsy surgery) and hands-on training for neurology residents could help raise awareness about identifying, counseling, and referring patients with DRE for epilepsy surgery. Residents should be strongly encouraged to attend epilepsy surgery conferences at their facility in order to gain a better understanding of the reasoning behind the patient selection, testing options, and, ultimately, prognostication. Beyond residency, independent practitioners may benefit from the ILAE (a virtual campus and teaching academy built around the EpiEd curriculum) and other relevant national organizations’ interactive, web-based online education resources. In-person training, such as the J. Kiffin Penry Epilepsy Education seminars or mini fellowships to expose practitioners to epilepsy surgery, may also be beneficial to some professionals.
Besides physician education, we need to develop clinical practice guidelines and practical decision models focused on presurgical counseling to reduce existing practice variations. 50 For example, the Three-talk model framework can be standardized for presurgical discussion and shared decision making. 51 Additionally, a practical risk-benefit analysis model needs to be developed and evaluated to allow objective decision-making. The suitable model may help families avoid overreliance on physicians, avert overestimation of ‘high-magnitude, low-probability events’ (e.g., death from epilepsy surgery), and comprehend the cumulative risk of conservative therapy, such as the cumulative risk of SUDEP over a lifetime and the possibility of reversibility with better seizure control after surgery. 52 Lastly, a formal team-based presurgical counseling approach(involving nurses, care coordinators, and social workers), with or without the use of telehealth services, may be more time-sensitive and sustainable in a busy clinical practice without causing clinician burnout.53,54
Conclusion
This study contributes to understanding epilepsy providers’ experiences and views on challenges and barriers in the presurgical conversations for epilepsy surgery. Our findings support the need to develop clinical practice guidelines and a shared decision-making model (including a practical risk-benefit analysis framework) to achieve a more positive patient and family experience toward epilepsy surgery.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738221089472 - Supplemental material for Physicians’ Perspectives on Presurgical Discussion and Shared Decision-Making in Pediatric Epilepsy Surgery
Supplemental material, sj-docx-1-jcn-10.1177_08830738221089472 for Physicians’ Perspectives on Presurgical Discussion and Shared Decision-Making in Pediatric Epilepsy Surgery by Debopam Samanta, Adam P Ostendorf, Rani Singh, Satyanarayana Gedela, Vimala Elumalai, Megan Leigh Hoyt, M. Scott Perry, Luca Bartolini and Geoffrey M Curran in Journal of Child Neurology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Debopam Samanta is supported by the Translational Research Institute (TRI), grant UL1 TR003107 through the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. Megan Hoyt is supported by the ACRI/ABI Nursing and Allied Health Grant.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.