
Abstract
Introduction
Migraine is a common neurologic disorder in children and adolescents. 1 The prevalence of pediatric migraine varies according to age, ranging from 3% in early childhood to 20% in adolescents. The prevalence is higher in boys than in girls prior to puberty. However, the condition is more prevalent in girls after age 11 years. 2 Pediatric migraine is a highly disabling condition in childhood as well as adolescence. 1 According to the pediatric migraine disability assessment scale (ped MIDAS), prophylactic therapy should be considered if a patient has 2 or more headache episodes per week or if the disability score is more than 20. 3 Indeed, there is no consensus regarding prophylaxis in pediatric migraine, even in recently published guidelines from the United States. 4 Complementary and integrative medicines have been increasingly used nowadays for treating diseases such as pediatric migraine. 5 Although many drugs can be used for prophylaxis and acute management of migraine in adults, the number of agents specifically indicated for prophylactic treatment of pediatric migraine is inadequate, and the use of alternative therapies is widespread, such as riboflavin, coenzyme Q10, magnesium, melatonin, polyunsaturated fatty acids, feverfew, butterbur, vitamin D, and ginkgolide B. 6 Recently, the US Food and Drug Administration (FDA) approved flunarizine and topiramate for migraine prophylaxis in children and adolescents. 7
Vitamin D is a neurosteroid with autocrine and paracrine properties. Vitamin D deficiency has been reported to be possibly involved in the etiopathology of autism, depression, schizophrenia, and diseases affecting the central nervous system, such as multiple sclerosis.8,9 Vitamin D plays a role in the secretion of chemical mediators in the central nervous system that are involved in the pathophysiology of migraine. Also, vitamin D has neuroprotective and antioxidant effects. These facts suggest that vitamin D and migraine may be related. 10 A few studies in adults found that vitamin D supplementation reduces the frequency of migraine attacks.11,12 In some studies,13,14 the supplementation reduced the frequency of migraine attacks. However, it is unclear whether vitamin D has a specific role in pediatric migraine prevention. Although a prospective study demonstrated that vitamin D supplementation to amitriptyline therapy reduced the number of migraine attacks, safety outcomes were not reported. 15 In a recent study of children with migraine headaches, the combination of topiramate and vitamin D3 showed a significant effect on the reduction of monthly headache frequency and disability score compared to topiramate alone. 16 In addition, a current meta-analysis study of vitamin D3 in migraine patients reported preliminary evidence of low serum levels of vitamin D3 in both adults and children. 17 Our study aimed to evaluate the effects and safety of vitamin D supplementation as adjuvant therapy to topiramate on children and adolescents with migraine.
Patients and Methods
This prospective, randomized, double-blind case-control study was conducted on 60 children and adolescents with migraine. However, 4 children did not complete the study. Following formal consent, the study was carried out from May 2020 to August 2021. Migraine patients were enrolled in the pediatric neurology outpatient clinic at Taif military hospitals in Saudi Arabia.
There were 34 females and 22 males, with ages ranging from 5 to 14 years (mean 10.6 ± 3.4 years). All participants were inhabitants of Taif City, with equal exposure to direct sunlight. The diagnosis of migraine was based on the International Classification of Headache Disorders–III (ICHD-III) diagnostic criteria that were published by the International Headache Society (IHS) in 2013. 18
The severity of the headache was determined according to the MIDAS scale as grade I: 0-5, grade II: 6-10, grade III: 11-20, and grade IV: 21. 19
A good response to treatment was defined as more than a 50% decrease in the monthly headache attack frequency during follow-up.
Children aged 5-14 years were diagnosed with migraine ICHD-III diagnostic criteria, 2 or more headache attacks per week, PedMIDAS score >20, normal hemoglobin (Hb) level, and mean corpuscular volume (Hb level >11.5 g/dL, mean corpuscular volume > 80 fL), normal vitamin D3 serum level (>30 ng/mL), no vitamin D3 supplements within the past 3 months, and not receiving any migraine preventive therapies other than topiramate.
Exclusion criteria included subjects with any neurologic diseases (mental retardation, seizure, epilepsy, etc), psychiatric problems, any systemic or autoimmune diseases, any drug use (steroids, immunosuppressants, vitamin D supplements, etc), acute or chronic infection, or hospitalization within the previous 4 weeks, headaches other than migraines or secondary headaches, excessive drug usage, discontinuation of drugs for more than 1 week, allergy to topiramate or vitamin D3, and a vitamin D3 serum level of 30 ng/mL or >80 ng/mL.
Group A (supplementation group) included 30 children with migraine on topiramate therapy who received vitamin D3 supplementation as an adjuvant therapy to the standard treatment.
Group B (placebo group) included 30 children with migraine who received topiramate therapy and a placebo without vitamin D3 supplementation.
Group A (supplementation group) was treated with topiramate tablets with a dose of 2 mg per kg of body weight in 2 divided doses daily in combination with vitamin D3 pearl supplementation with a dose of 5000 IU daily for 4 consecutive months.
Group B (placebo group) was treated with topiramate tablets with a dose of 2 mg per kg of body weight in 2 divided doses daily in combination with a placebo capsule. A placebo capsule was prepared by Abbott Pharmaceutical Company with an identical shape, color, and packaging to the vitamin D3 capsule and without any effective substances.
After selecting the patients for inclusion in our study and offering explanations to the parents, patients were randomly assigned in a double-blind fashion in a 1:1 ratio into either the vitamin D3 supplementation group (group A) or the placebo group (group B), and a code was assigned to them. Then, in a blind manner, without informing the patients or the physician about the medication content of group A or B, medications were given to the patients by the physician, and they were treated and followed up monthly for at least 4 months, and the severity, frequency, the PedMIDAS score, and duration of headache attacks as well as the efficacy and safety of medications were recorded. 20 The codes were unveiled after the completion of the treatment duration and the recording of patient information.
Before starting treatment, the demographic data, including age, genders, and clinical characteristics, were recorded. Also, routine laboratory screening evaluations, including vitamin D3 assays, were done.
The frequency of headache attacks before and after the treatment was recorded monthly through a parenteral questionnaire.
A pediatric Migraine Disability Assessment Score (PedMIDAS) was used to evaluate the severity of headaches before and after the treatment. According to the PedMIDAS questionnaire, the headache severity was divided into grades from the lowest to the highest, as follows: grade 1 (0-10), grade 2 (11-30), grade 3 (31-50), and grade 4 (greater than 50). 20 The questionnaire includes 7 questions that examine the impact of headaches on different levels of work, home, social, and leisure activities over the past 3 months. Questions 1 through 5 assess the migraine-related decline in performance. 20
In addition, at the end of the investigation, we asked the patients or parents to rate their overall clinical general impression using a 7-point Likert-type scale ranging from grade 1 (very dissatisfied) to grade 7 (quite satisfied). 21
During the interview, data were obtained and reported by reviewing self-reported diaries and daily notes of parents. Patients were revisited every 2 weeks for a further 2 months after the treatment, and the severity of migraine attacks was evaluated after the treatment.
During the study, if there was a change in the clinical condition of any patient, re-evaluation was done. If the diagnosis was changed, the patient was excluded from the study and replaced by another one according to inclusion and exclusion criteria. Also, analgesics (acetaminophen or ibuprofen) were allowed only for the symptomatic relief of moderate to severe attacks of headache.
Compliance to vitamin D3 supplementation and topiramate therapy was checked using a tablet count after 16 weeks of intervention. A participant was considered compliant if he consumed 80% of the supplements throughout the trial.
Additionally, compliance was stimulated by weekly telephone calls to use the supplements. Also, vitamin D3 status was evaluated at the end of the study to assess the compliance of patients in the intervention arm.
Patients were asked to report any side effects, minor or major adverse effects, that were likely to be associated with supplementation. Also, researchers had to be called immediately and promptly if serious adverse events occurred (such as refractory nausea or vomiting, severe anorexia and weight loss, drug rashes, severe abdominal pain, systemic symptoms, topiramate-related heatstroke, behavior changes, difficulties with concentration, lethargy, and disorientation).
Determination of Vitamin D Status
At the first visit and at the end of the trial, a venous blood sample of 3 mL was taken from each participant to assess the serum concentration of vitamin D3. Blood samples were centrifuged at 4 °C for 10 minutes to separate serum, which was then stored at −80 °C until analysis. Vitamin D3 levels in the form of serum 25OHD (S25OHD) were evaluated using the chemiluminescence immunoassay method. 22
Outcome Measures
The primary outcomes were a monthly frequency of headache attacks and a good response to intervention, as well as a reduction in migraine severity, duration, and disability before and after 4 months of treatment.
Statistical Analysis
The analysis of data and variables was done using SPSS, version 16.0 (Chicago, IL, USA). The quantitative data were presented as means ± standard deviation. A chi-square test was used to determine the significance of the data.-square test or Fisher exact test was used to compare categorical data. A Student t test was used to test differences in means, and the P value was considered significant whenever it was below .05.
Results
This case-control study was conducted on 60 children, 30 of whom were in the migraine cohort and 30 children in the control group. Seventy-six patients were screened for study inclusion, and 17 did not meet the inclusion criteria and were excluded. Of the 60 patients, 56 participants completed the study. The study found no difference in the attrition rates between the 2 arms, with 2 (6.6%) in the intervention group and 2 (6.6%) in the placebo group. The remaining participants, on the other hand, adhered to the rules to the letter.
Finally, 56 children completed the trial, 34 females (60.7%) and 22 males (39.3%), with ages ranging from 5 to 14 years (mean 10.6 ± 3.4 years).
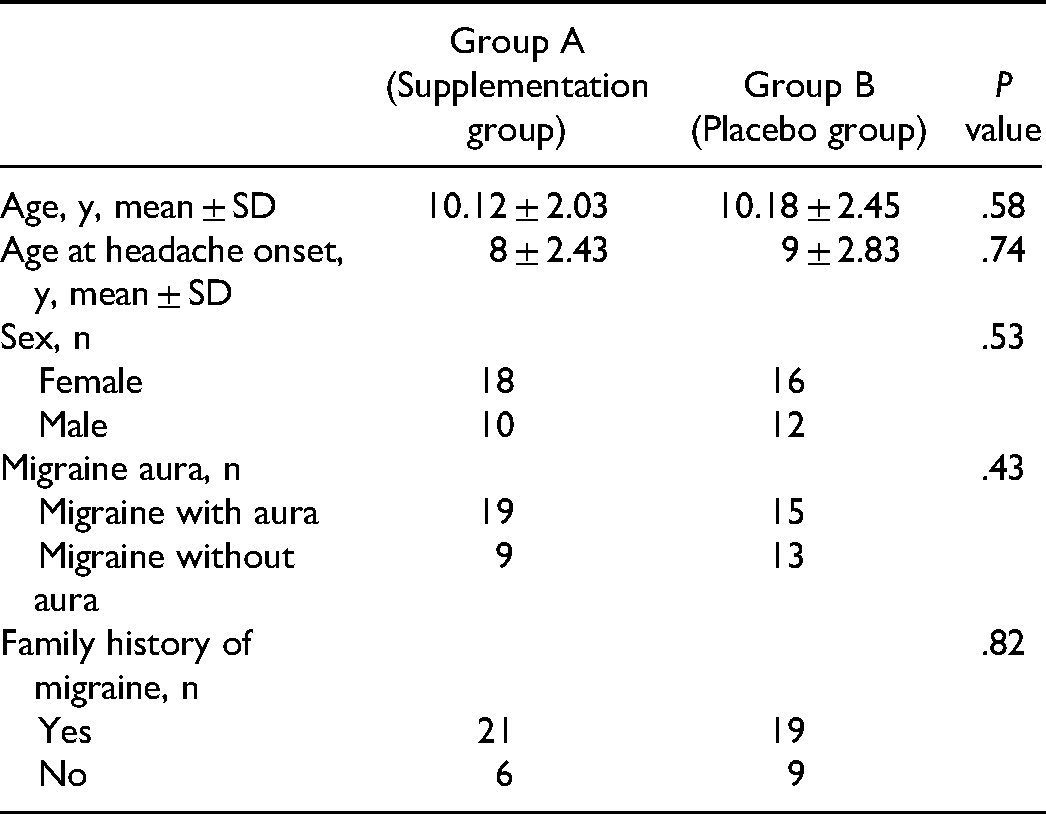
The results of the demographic data of the children in both groups are shown in Table 1, indicating that age and sex, as well as the type and positive family history of migraine, showed no significant difference between the 2 groups.
Comparison of Demographic Data of Children in the Studied Groups.
Before the intervention trial, the comparison of migraine characteristics between the 2 studied groups is shown in Table 2. There was no significant difference between the vitamin D3 supplementation group and the placebo group regarding the frequency of migraine attacks per month, severity, duration, and disability for migraines.
Comparison of Migraine Characteristics Before Treatment in the Studied Groups.
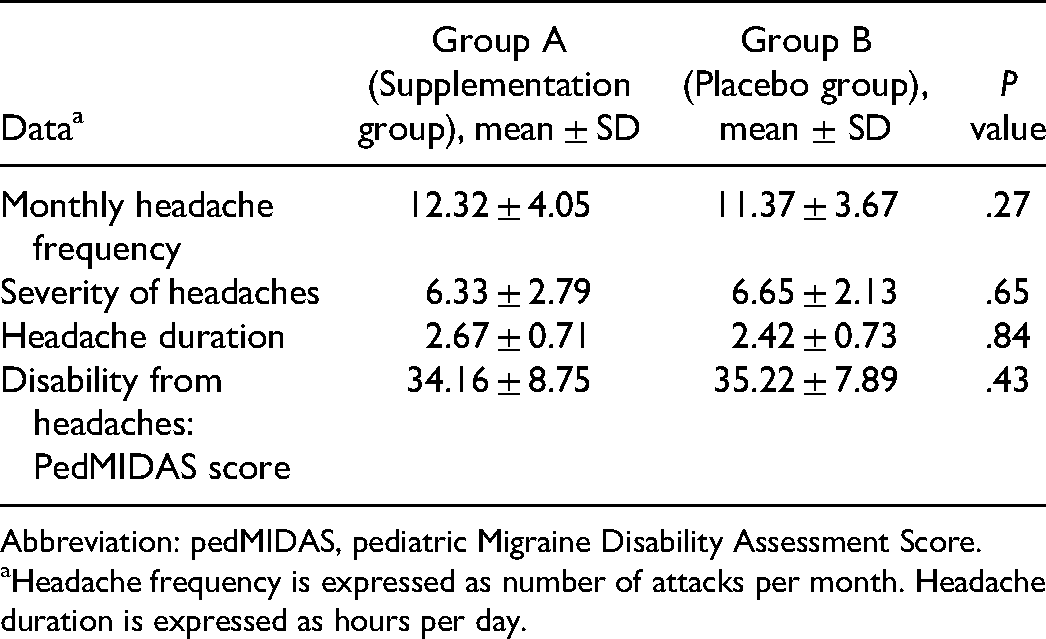
Abbreviation: pedMIDAS, pediatric Migraine Disability Assessment Score.
Headache frequency is expressed as number of attacks per month. Headache duration is expressed as hours per day.
Comparisons of migraine characteristics before and after intervention in the vitamin D3 supplementation group and placebo group are shown in Tables 3 and 4, showing that vitamin D3 supplementation to topiramate was more effective than the placebo group in the reduction of monthly frequency, severity, duration, and disability for migraines.
Comparison of Migraine Characteristics Before and After Treatment in the Supplementation Group.
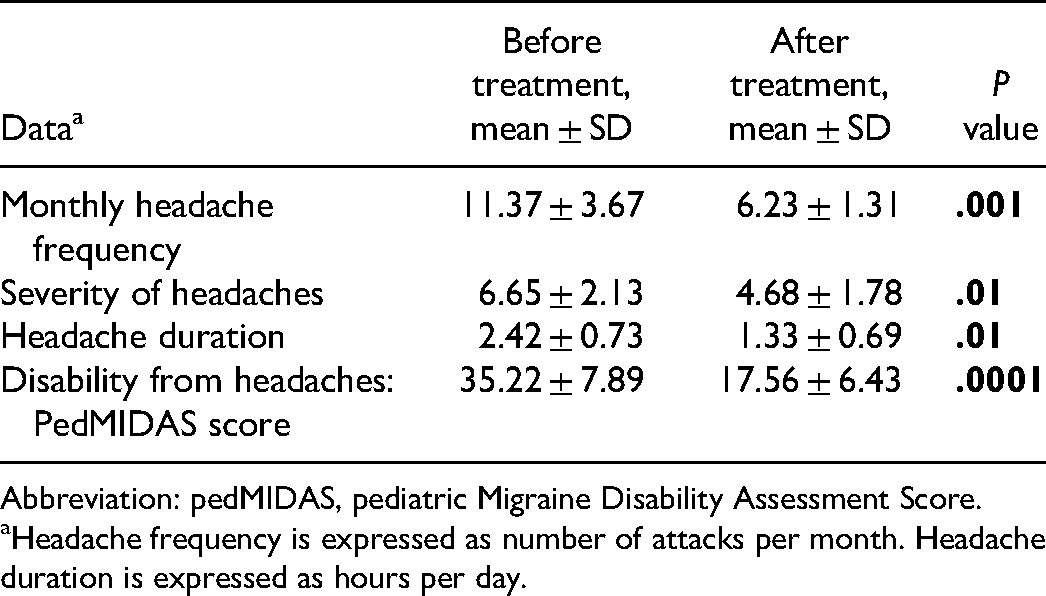
Abbreviation: pedMIDAS, pediatric Migraine Disability Assessment Score.
Headache frequency is expressed as number of attacks per month. Headache duration is expressed as hours per day.
Comparison of Migraine Characteristics Before and After Treatment in the Placebo Group.
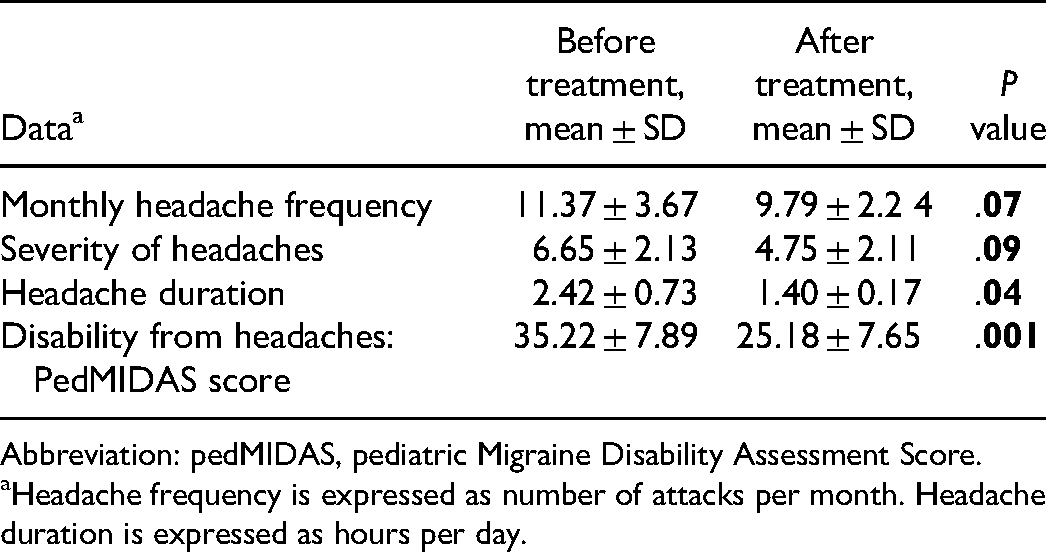
Abbreviation: pedMIDAS, pediatric Migraine Disability Assessment Score.
Headache frequency is expressed as number of attacks per month. Headache duration is expressed as hours per day.
Comparisons of migraine characteristics after vitamin D3 supplementation are shown in Table 5, showing that vitamin D3 supplementation to topiramate was more effective than the placebo group in the reduction of monthly frequency and disability score. However, the severity and duration of migraines were not significantly different between the 2 groups.
Comparison of Migraine Characteristics and Patients’ Satisfaction After Treatment in the Study Groups.
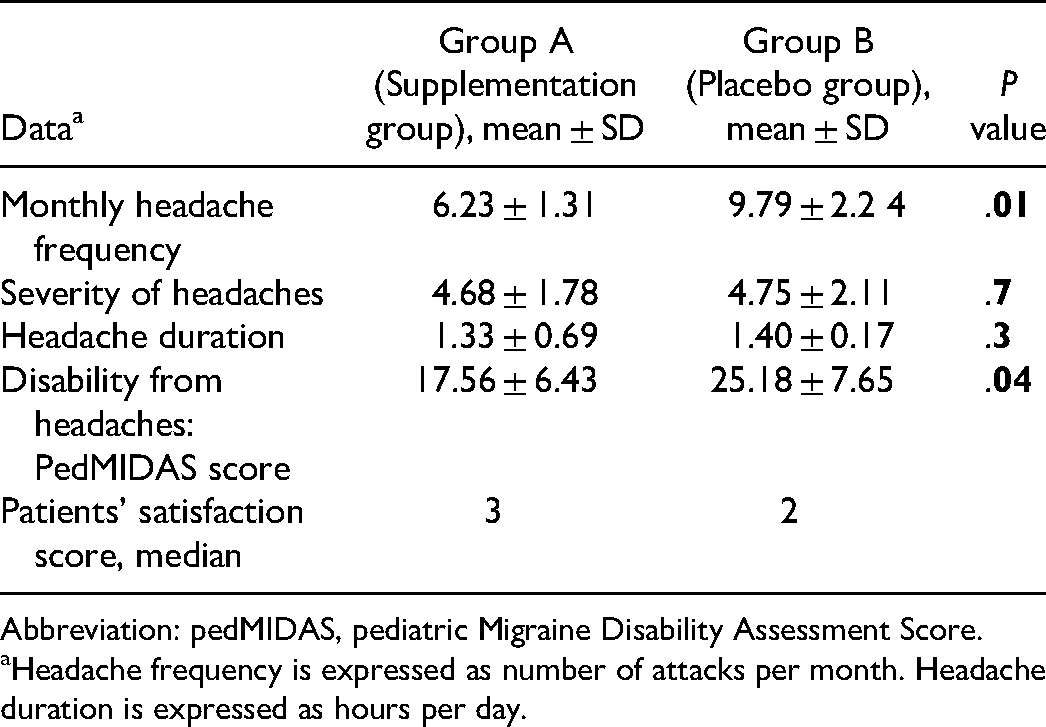
Abbreviation: pedMIDAS, pediatric Migraine Disability Assessment Score.
Headache frequency is expressed as number of attacks per month. Headache duration is expressed as hours per day.
Regarding migraine disability, there were no significant differences in baseline MIDAS scores in the vitamin D3 supplementation and placebo groups (mean values of 34.16 ± 8.75 and 35.22 ± 7.89, respectively).
After 16 weeks of vitamin D3 supplementation in the intervention group, it resulted in a significant improvement in MIDAS (mean value of 17.56 ± 6.43) compared to placebo (mean value of 25.18 ± 7.65) (P = .05). Within the vitamin D3 supplementation group, comparisons before and after intervention revealed a significant reduction in the MIDAS (mean values of 35.22 ± 7.89 and 17.56 ± 6.43, respectively; P = .0001) before and after intervention, respectively.
After 16 weeks of vitamin D3 supplementation, a good response (more than 50% reduction in the frequency of the monthly migraine attacks) was observed in 15 patients in the placebo group (53.5%, 95% CI 40.65%) and 21 patients in the vitamin D3 supplementation group (75%, 95% CI 58.23%) and vitamin D3 supplementation was significantly more effective than placebo (P = .01). We recorded 4 patients (13.3%) in the intervention group, with side effects in the form of abdominal pain in 2, anorexia in 1, and nausea and vomiting in 1 child.
However, 6 patients (20%) in the placebo group had side effects in the form of constipation in 2, anorexia in 2, and nausea and vomiting in 2 children. None of our patients developed serious adverse drug reactions. Drug safety showed no significant difference between the 2 groups (P = .5). All adverse effects were mild, transient, and disappeared within 10 days. None of our patients required discontinuation of medications because of side effects.
Patients’ satisfaction with the trial was significantly higher among the vitamin D3 supplementation group (median = 3) than the placebo group (median = 2) (P value = .04).
Discussion
Recently, the relationship between vitamin D and migraines in children and adolescents has been the focus of interest for many investigators. To our knowledge, this is the first double-blind therapeutic trial that examined the impact of vitamin D supplementation at a dose of 5000 IU daily for 16 weeks in children and adolescents with migraine and without vitamin D3 insufficiency.
Vitamin D deficiency is a global public health problem. There is growing but conflicting evidence of a possible association between vitamin D and chronic or recurrent painful conditions such as migraine. 8 Migraine is a common hereditary chronic neurovascular disorder characterized by dysfunction of the autonomic nervous system and may be accompanied by nausea and vomiting with phonophobia, photophobia, and osmophobia. Many drugs are used in the prophylactic treatment of migraine in children and adolescents. 9 It was observed that migraine attacks increase in the winter and autumn seasons as well as higher latitudes, which may be attributed to lower vitamin D serum levels. 23 Treatment with vitamin D and calcium dramatically reduces the frequency and severity of migraine in patients with migraine.24,25 In previous studies, 26 the link between vitamin D and headache has been suggested. Vitamin D deficiency and/or insufficiency were found in about 44% of migraine patients. A negative correlation was found between serum vitamin D concentrations and the frequency of migraine attacks. 26
It was reported that vitamin D supplementation at a dose of 2000 IU/d could reduce the frequency of monthly headache attacks, decrease the need for analgesics, and attenuate the severity and duration of headaches. 23
The present study aimed to detect the efficacy and safety of vitamin D supplementation as an adjunctive therapy to topiramate in pediatric migraine prophylaxis in children and adolescents (5-14 years old) without vitamin D3 deficiency. In our study, there was a significant decrease in the monthly frequency of migraine attacks and disability score in the vitamin D3 supplementation group starting treatment with vitamin D3 in addition to topiramate compared with the placebo group receiving topiramate without vitamin D3 supplementation.
Vitamin D has a neuroprotective effect on the central nervous system. The mechanisms beyond these effects include antioxidative, neuronal calcium modulation, and detoxification mechanisms.27,28
Although many studies have reported a positive link between pain-associated conditions and vitamin D status, no causal relationship has been established. 29 It was found that vitamin D3 supplementation may result in pain relief, especially among patients who had vitamin D insufficiency.29–33
The mechanisms that explain the beneficial effects of vitamin D on migraine characteristics and associated disability include significant increments in serum vitamin D3 and a reduction in serum calcitonin gene–related peptide (CGRP) levels.
CGRP is thought to be the primary mediator of migraine pain. 34 Vitamin D has antiinflammatory effects on migraineurs via lowering the levels of inducible nitric oxide synthase and interleukin-6. 35 CGRP levels were significantly elevated in migraine patients, particularly during pain attacks.36,37 For migraine pain, CGRP stimulates the production of nitric oxide (NO), resulting in neuro-inflammation and vasodilation.34,37
The effects of vitamin D in improving the features of migraine and reducing CGRP levels are attributed to the antinociceptive properties and NO pathway to trigger nociceptive neurons and neuro-inflammation, especially in the trigeminovascular system.29–31
Previous randomized controlled trials found that taking vitamin D at a dose of 2000 IU/d for 12 weeks resulted in significantly fewer headache days and a lower frequency of migraine attacks. 35
A Turkish study found that combining 400 IU of vitamin D3 daily with 1 mg/kg amitriptyline produced significant results.
In terms of migraine frequency, the addition of 400 IU daily vitamin D3 to amitriptyline was more effective than amitriptyline alone after 6 months in 6- to 18-year-old children and adolescents with normal serum 25-OH vitamin D3 levels (>20 ng/mL). 15
Our findings are consistent with a recently published Iranian blind randomized controlled trial in which supplementation of vitamin D3 in a dose of 500 000 IU of vitamin D3 weekly for 2 months in conjunction with topiramate was more effective than topiramate alone in reducing the monthly frequency and disability score of migraine in children and adolescents (5- to 15-year-old) who did not have vitamin D3 deficiency (serum 25-OH vitamin D3 > 30 ng/mL). 16 However, this study has limitations that included lack of placebo, short duration of treatment, and lack of follow-up after discontinuation.
Also, in a recent meta-analysis study that included 6 randomized controlled trials and 301 patients, it was concluded that vitamin D supplementation could significantly decrease monthly headache attacks, headache days per month, and MIDAS score in patients with pediatric migraine. 38
However, this meta-analysis study has some limitations; it was based on only 6 randomized controlled trials, with a small sample of patients in each study and significant heterogeneity, which may be derived from different protocols and combinations of vitamin D and type and severity of migraine.
In an adult study, vitamin D3 supplementation at a dose of 100 g/d for 12 weeks was found to be more effective than placebo in decreasing frequency and daily headache episodes, with significant elevations in vitamin D3 serum levels. 11 It was observed that vitamin D3 supplementation is more effective in pediatric migraine patients than in adult patients. In addition, vitamin D supplementation had a low risk of side effects.39,40 The adverse events of vitamin D3 were well tolerated. 11 On the other hand, the association between migraine and vitamin D3 was not observed by other authors.10,12,13
In our study, we did not report any significant differences between the groups with regard to the number of patients who developed adverse effects all over the study period. We recorded 4 patients (13.3%) in the intervention group and 6 patients (20%) in the placebo group with mild gastrointestinal complaints.
No serious adverse reactions were reported. So, the therapeutic trial of vitamin D3 supplementation was well-tolerated and safe.
The limitations of the present study were the small sample of patients, the short duration of treatment, a lack of comparison of serum levels of vitamin D3 between cases and controls, and the lack of follow-up after discontinuation of vitamin D3 supplementation. Also, vitamin D3 levels were not investigated over all 4 seasons, and patients’ dietary habits were not examined. However, the strengths of this study are the prospective, double-blind, placebo-controlled design, using a safe daily dosage of vitamin D.
Conclusions
Accordingly, vitamin D3 supplementation may improve pediatric migraine prophylaxis. Therefore, daily administration of vitamin D 5000 IU as an adjuvant therapy to topiramate could be considered a well-tolerated, safe, and effective strategy in the improvement of pediatric migraine prophylaxis.
Further randomized controlled trials with a larger sample size and a longer duration of follow-up are recommended, taking into consideration altitude control and seasonal differences to determine the optimal dose of vitamin D3 supplementation for the prevention of pediatric migraine.
Footnotes
Author Contributions
Moustafa Kotb Elmala: Conceived the study, provided key technical guidance, drafted the manuscript. Hany Abdelaziz Suliman: Participated in its design and coordination, drafted the manuscript. Ashraf Hamed Al-shokary: Participated in its design and coordination, drafted the manuscript. Asmaa Obada Ibrahim: Participated in its design and coordination, critically revised the manuscript for important intellectual content. Naglaa M. Kamal: Participated in its design and coordination, critically revised the manuscript for important intellectual content. Hatem Hamed Elshorbagy: Conceived the study, provided key technical guidance, drafted the manuscript, critically revised the manuscript for important intellectual content. Khaled Amin Nasef: Participated in its design and coordination, drafted the manuscript. Mohamed Gamal El Din Fathallah: Participated in its design and coordination, drafted the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Before the study was conducted, the study protocol was reviewed and approved by an independent research board. All ethical guidelines in the 1964 Declaration of Helsinki and its later amendments were considered.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.