
Abstract
The COVID-19 pandemic has seen an explosion in the use of telemedicine in neurology.1,2 Although telemedicine is noted to be safe, effective, and a valuable means of patient care when combined with in-person visits,1,3 it was implemented across health care in large part as a “crisis standard of care” during a global pandemic. There are some inherent limits to epilepsy care that can be provided with the current technology. These include, for example, the inability to perform electroencephalographies (EEGs) and altered management of conditions like epileptic spasms.4,5 In addition, evaluation of neurostimulation devices for epilepsy patients is a challenge. In all other respects, however, a telemedicine visit for epilepsy should be similar to an in-person visit. This also means that the same best practices that are implemented in an in-person visit should be implemented in a synchronous (real-time audiovisual) telemedicine visit. Because there are many gaps in the quality of care provided, performance measures are established to easily measure whether specific activities are carried out during an encounter. 6 The purpose of the current study was to determine if Epilepsy Quality Measures (EQM), guidelines, and best practices are followed when patients are seen for epilepsy or seizure related care via a telemedicine visit.
Methods
This was a cross-sectional, retrospective, multicenter study. Three level 4 National Association of Epilepsy Centers pediatric epilepsy centers participated. This study was approved by the institutional review board at each center and data sharing use agreements were executed where necessary. An electronic medical record (Epic, Verona, WI) data extraction was performed using the key terms “new patient, spells/ seizures/ epilepsy” between January or February 2020 to December 2020 in 2 centers while at the third center an initial cohort (time frame March-June 2020) that had been analyzed for safety and quality of telemedicine 1 was searched for all new patient, spells, seizure, and epilepsy encounters. Only outpatient clinic visits were accessed. Variables extracted included demographic variables (age, gender, race, ethnicity, payor type, location), provider variables (physician, advance practice providers, nurse [RN]), specialty (epilepsy, general child neurology); encounter specifics: vitals, seizure/ spell specifics (frequency, description, last event, seizure and epilepsy syndrome diagnosis per ILAE), details of examination including number of systems examined, assessment, and plan (medications reviewed, controlled substance/s prescription/s, adverse effect discussion, testing ordered if any), counseling regarding seizure safety, driving, mood, sudden unexplained death in epilepsy (SUDEP), pregnancy-related counseling, and coordination of care. The terms above in italics form variables that are important epilepsy quality metrics, best practices, and or guidelines. Because there was no uniform/standardized method of charting across the 3 level 4 National Association of Epilepsy Centers–accredited centers, if any mention of the above italicized items was made in the history, discussion, plan, prescriptions, or after-visit summary for the said telemedicine encounter, it was considered that the action had been performed.
A total of 242 patients met criteria for this cohort as “new encounters.” Their charts were then manually reviewed. Any patient that had been previously seen in the emergency department (ED) at the same facility for the presenting complaint or seen by a different team within the same group (patient seen by ketogenic diet team for example) was excluded.
Statistics
Means and standard deviations summarized continuous variables while counts and percentages summarized categorical data. Logistic regression was performed to identify variables associated with implementation of quality metrics. All P values were based on 2-sided tests and P values less than .05 were considered significant. All statistical analyses were performed using SAS, version 9.4 (SAS Institute Inc, Cary, NC).
Results
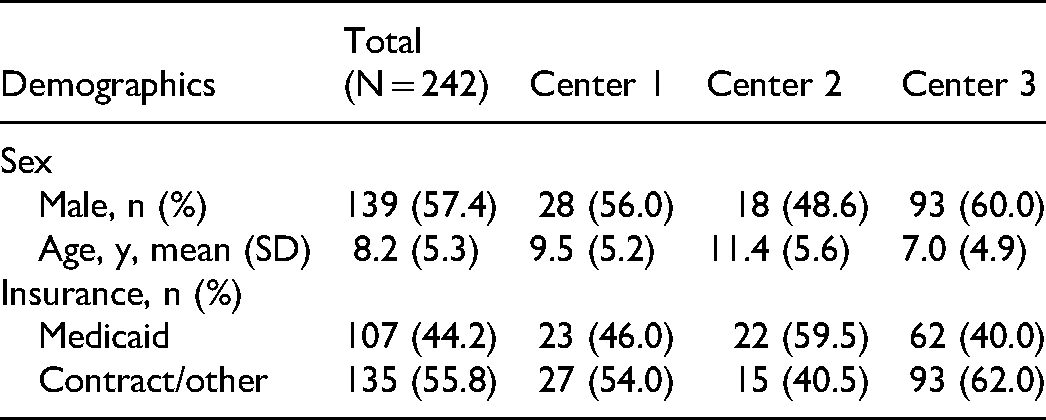
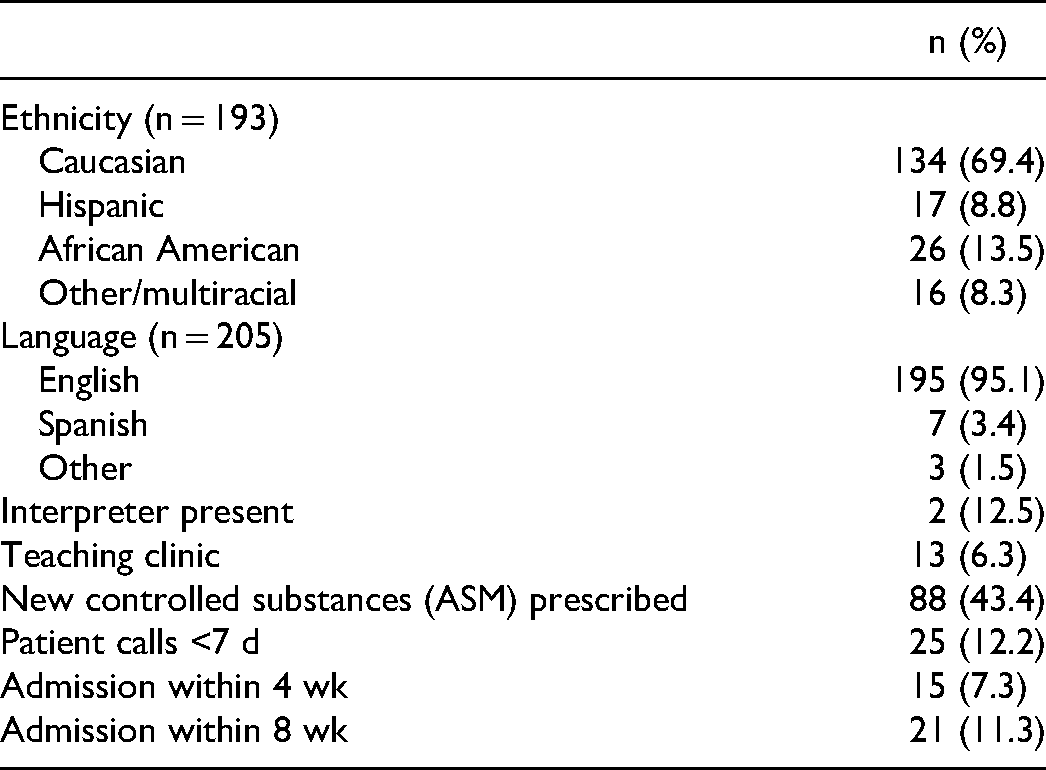
A total of 242 patients met the inclusion criteria. Of these, 160 patients were diagnosed with epilepsy and were included for analysis of EQM, quality measures, and best practices in epilepsy. Demographic details and other relevant visit details are reported in Tables 1 and 2, respectively. There were 50, 37, and 155 patients who satisfied inclusion criteria at centers 1, 2, and 3, respectively. The 3 centers did not differ in patient characteristics with respect to gender, average age at time of appointment, or insurance type. Eighty-four percent patients were seen by physicians (33% epileptologists and 67% generalists) and 16% by midlevel providers. Entry complaint was spells in 81% (vs seizures in 19%). Ultimately, epilepsy was diagnosed in 66% (n = 160). Seizure characteristics were described in 95% patients, whereas frequency of seizures was described in only 67%. Last seizure was reported in 81%. Epilepsy syndrome was mentioned in 67%, whereas epilepsy diagnosis per International League Against Epilepsy (ILAE) was described in 78%. Quality of life was discussed or mentioned in only 3%. Anticipatory guidance related to seizure safety (examples include height safety and water safety) was described in 57%; transition was discussed in 5% (if >14 years) and 30% (if >18 years), anxiety or mood was discussed in 27%; driving in 47%; SUDEP was discussed in only 11%; vitamin D discussion occurred in 19%; and pregnancy and folic acid discussions occurred in just 4% and 10%, respectively in eligible patients (defined as females aged >14 years for this study). Seizure action plan for school was provided in only 46%. There was no difference between an epileptologist or generalist for discussion of SUDEP, pregnancy, or water safety. Epileptologists were 4 times as likely as generalists to discuss driving safety (OR 3.93, 95% CI 1.7-8.9; P = .001) if all ages were considered. However, if only patients aged >14 years at visit date were assessed, this difference was not significant. Cause-specific admission was 7.3% within 4 weeks and 11.3% within 8 weeks; there was 1 SUDEP in the entire cohort. There was no statistical correlation of cause-specific admission rates and encounters with low documentation of EQM variables like discussion around rescue medications, adverse effects, seizure and frequency details, safety discussion or counseling related to SUDEP, driving, folic acid, pregnancy, or vitamin D. Additionally there was not any statistically significant correlation with factors like race or primary language with the above measures.
Demographic Data of Our Cohort.
Additional Data Related to Patient and Clinic Characteristics.
Discussion
The use of telemedicine increased quickly during the early phases of the COVID-19 pandemic. Most of the infrastructure changes that helped make this transition are likely to remain in place and be used more frequently as clinicians become increasingly comfortable with telemedicine. In a telehealth model that incorporates synchronous audiovisual visits for care delivery (“telemedicine” in our study), opportunities to ensure high quality of care and implementation of EQM, guidelines, and best practices exist. Our study is the first to evaluate these end points in new pediatric encounters.
Quality measures were created for epilepsy care by the American Academy of Neurology (AAN-EQM) with the first set published in 2009. 6 The quality measure sets are periodically reviewed and revised to help providers offer care that is consistent with current medical knowledge. 7 Additionally, the American Epilepsy Society has published guidelines and practice parameters to guide best practices in epilepsy. 8 Quality measures and best practices should be applicable across all models of care in epilepsy—whether these occur in person or via telemedicine.
Because no such data exist to compare quality measures in telemedicine to date, we make comparisons with historically published data from in-person visits in the following discussion.
History Regarding Seizures and Classification
In our study, seizure frequency, description of events, last seizure, and epilepsy classification per ILAE was documented in >60% of the telemedicine visits. This information was obtained during the clinic encounter. A previous study in adults using patient surveys to study EQM evaluated baseline seizure frequency, adherence to medication, and issues around driving and found that patient-reported quality of care measures (history regarding seizures, for example) directly affected patient-reported outcomes. 9 Our centers did not uniformly use patient surveys prior to clinic appointments. Patient-reported data in the form of standardized intake forms, filled out before an appointment, could save time and help to further increase compliance with some EQM measures.
Counseling for Key Education Measures: Driving, Pregnancy, SUDEP, Transition, Seizure Action Plan
Counseling for key education measures like SUDEP, driving, and pregnancy-related outcomes was performed in fewer than 20% of eligible patients in our study. In relation to counseling women with epilepsy, a survey of child neurologists showed that although 95% respondents reported that counseling was performed at some point in time, only a third of the respondents reported counseling on a regular basis. 10
Epileptologists were statistically more likely to discuss issues related to driving than nonepileptologists at any visit not analyzed by age. However, when only patients >14 years of age were analyzed, the odds ratio of epileptologists discussing driving were still higher than general neurologists and clinically significant although not reaching statistical significance. One explanation for this finding could be that it is common for epilepsy providers to be asked to advise on driving clearance and fill the DMV forms for their patients; therefore, epileptologists habitually discuss driving regulations in all patients. Additionally, the goal of seizure freedom is identified prior to driving age, and thus discussion is more likely to start even before the age of 14 years.
In this cohort, transition-related discussion occurred in 5% of patients aged >14 years and 30% if aged >18 years. Discussion of transition-related issues is important, and it is recommended that this should begin as early as age 14 years, but is not common in practice. (https://www.gottransition.org/) In a community-based study of young adults, 11 only a third of young adults with epilepsy reported having transition-related discussions with health care providers before age 18 years. It is possible that in our study, the virtual environment and lack of familiarity with a patient and their family in the new patient setting were barriers for these discussions to occur.
In our study, 46% of patients received a seizure action plan. These plans are important, can improve comfort with seizure care, 12 and help with clinic appointment attendance.12,13 A previous publication describes improved performance on ensuring that patients receive a seizure action plan in the outpatient clinic for in-person visits from 0% to 58.1% using quality improvement methodology. The patients who received a seizure action plan demonstrated improved knowledge about seizures. 14
Published studies show an overall lower trend toward discussion of measures related to patient education. In a national survey of adults done through the VA system, only 38% patients were counseled about driving. 15 In another survey on knowledge and experience of neurology trainees about SUDEP, only 6.8% of respondents reported discussing SUDEP with all their patients and 11% never did. 16 In a survey directed at child neurologists, 12% were reported as discussing SUDEP in all patients. 17 Lack of time and discomfort with discussing a topic that could provoke anxiety were reported reasons for the lack of adherence to SUDEP practice guidelines. We chose a new patient encounter to study these parameters because most new patient encounters allow for more time and hence time constraint is less likely to be a cofactor in play for suboptimal adherence to discussion around EQM in our cohort. Discomfort and unfamiliarity in discussion of a difficult topic in a non–face-to-face encounter could be a potential barrier and could account for the low numbers seen in our study.
Discussion around pregnancy and folic acid was the least documented (4%) in our study for eligible (defined as >14 years of age for purposes of this study) female epilepsy patients. In a survey of child neurologists, even though between 70% and 90% felt that they should be responsible for doing the counseling around topics related to pregnancy, contraception, drug interaction, and folic acid, but fewer felt confident in performing the actual education themselves, for example, drug-drug interactions (65%) and contraception (47%-64%). 10
Study Limitations
Limitations of our study are that this was a retrospective, cross-sectional chart review and that we did not compare the implementation of quality measures for patients seen in each of the centers during an in-person clinic visit during the pandemic. It is possible that performance with quality measures decreased overall, not solely in telemedicine visits, because of all the stressors of the pandemic. 18 We relied on documentation within the telemedicine clinic encounter to assess whether an EQM, best practice guideline was followed. We are limited in our ability to judge “how much discussion” occurred surrounding these topics or “how complete” this discussion was but feel that we would have had the same limitation whether we were assessing an in-person encounter or a telemedicine encounter. We are also limited by the possibility of “if it was not documented it was not done” as a corollary to the above limitation discussing “how much” was discussed. Although our numbers were too small to determine any signal of disparities in EQM and guideline adherence for patients considered vulnerable (low socioeconomic status, non-native English speakers, non-White race, and non-Caucasian ethnicity), this could certainly be a topic for future exploration with telehealth visits.
Are there ways to improve EQM, quality measure adherence?
In a recent study by Moura et al, the authors describe quality improvement interventions to improve documentation of EQM. They started their efforts in the pre-COVID time frame. Adherence to EQM fell during the pandemic telemedicine visits but later saw an improvement with implementation of smart phrases and frequent plan-do-study-act (PDSA) cycle methodology. 18 However, this publication has chiefly targeted an adult “follow-up” epilepsy population where the authors targeted only seizure descriptors as a single quality measure. 18 Nevertheless, this study shows that with repeated interventions and standardization of note templates, EQM adherence can be improved even in telemedicine visits. In another study using Extension for Community Healthcare Outcomes (ECHO), implementation of EQM in pediatric epilepsy improved over 8 months in a community health care setting after periodic quality improvement sessions. 19 Although the quality improvement sessions were held using telehealth technology, the patients encounters where documentation of better EQM implementation occurred were seen in face-to-face encounters in a pre-COVID time frame. Although some authors are of the opinion that new patients or existing patients with new health problems should not be seen in telemedicine clinics 20 ; in a chronic condition like epilepsy, the use of quality improvement sessions and standardization of note templates are reasonable next steps to consider for centers to improve their EQM implementation.
Conclusion
This is the first study that describes adherence to EQM, guidelines, and best practices in a pediatric telemedicine visit. We found that although adherence to factors related to direct medical management were comparable to historical data for in-person visits, there are certainly opportunities to improve discussions around other education-related topics in a telemedicine visit. Additional research is needed to study contributing factors into why some EQM, best practice quality measure implementation is lacking in telemedicine visits. Greater provider education to ensure that telemedicine care aligns with EQM implementation that models best practices in epilepsy care is also necessary.
Footnotes
Acknowledgments
The authors would like to thank Evelyn Wentzel, RN, for her assistance with IRB submission, data collection, and data review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.