
Abstract
Seizures that occur between the ages of 6 and 60 months with a temperature of 38 °C or higher, that was not caused by a central nervous system infection or any metabolic imbalances, and who did not have a history of prior afebrile seizure are classified as febrile seizures. 1 Febrile seizures are the most prevalent form of seizure in the first 5 years of life, affecting 2% to 5% of the child population, globally. 2 The prevalence of febrile seizures varies greatly among nations, depending on the various risk factors involved. In Asia, it has been observed that 8% to 11% of children under the age of 5 years develop febrile seizures. 3 In addition, the total prevalence of febrile seizures in Indonesia has been shown to be 8.3%. 4 This demonstrates that the prevalence of febrile seizures in Asia is greater than the global prevalence, underlining an issue that needs to be addressed promptly.
Several studies have identified a number of risk factors for developing febrile seizures, including genetic factors, low socioeconomic factors, poor nutritional status, several infections, and some micronutrient deficiencies such as iron.5–7 Iron is an inorganic compound that serves as a cofactor for several enzymes in the body and is involved in the production and function of neurotransmitters, as well as various neurochemical reactions such as the formation of the myelin sheath, the metabolism of several neurotransmitters, and the formation of energy in brain cells. Iron deficiency is frequently linked to poor cognitive performance and has the potential to cause permanent brain cell damage. 8 Interestingly, the incidence of iron deficiency anemia and febrile seizures share the same prime age, and various research have led to the conclusion that iron deficiency plays a pivotal role in the development of febrile seizures. 9
Several investigations support the concept that the risk of febrile seizures is much greater in individuals with iron deficiency than in the control group.9–13 Other studies, on the other hand, have determined that the risk of febrile seizures in anemic children does not appear to be statistically significant when compared to children who do not have febrile convulsions.14–18 Nonetheless, iron deficiency anemia is a worldwide condition that requires intervention because it is a pervasive nutritional issue that may be avoided by screening and proper therapeutic interventions.
A recent meta-analysis conducted by Kwak et al 19 in 2017 demonstrated that iron deficiency anemia, low mean corpuscular volume, and low serum ferritin were associated with febrile seizures but not serum iron. Nonetheless, because of the limited number of studies included in its subgroup analysis, the lack of data on the relationship between total iron-binding capacity and febrile seizures, unexplained high interstudy heterogeneity, uncontrolled confounding factors, and the fact that this meta-analysis was performed in 2017, the association between these 2 aforementioned variables remains equivocal. Therefore, the present meta-analysis has 2 primary objectives: first, to evaluate the correlation between iron deficiency anemia, along with its indices (mean corpuscular volume, serum iron, total iron-binding capacity, ferritin) and febrile seizures; second, to estimate the sensitivity and specificity of each index through diagnostic-test accuracy analysis in order to increase the robustness of this research as well as to better understand which one is the better predictor of similar outcomes.
Methods
Protocol and Registration
This meta-analysis was recorded in the PROSPERO (International Prospective Register of Systematic Reviews) database under registration number CRD42022309491 and followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) standards. 20
Search Strategy
Two independent investigators searched PubMed, Europe PMC, and ScienceDirect from database inception up until November 30, 2022, with the search terms (“iron deficiency anemia” [MeSH Terms]) AND (“febrile seizure” [MeSH Terms]). We tailored each search term to the constraints of each database, and full-text publications were meticulously reviewed by both authors in case there was debate about whether research should be included based on its title or abstract. Our search followed the PRISMA guidelines, and the search and screening processes are depicted in Figure 1.
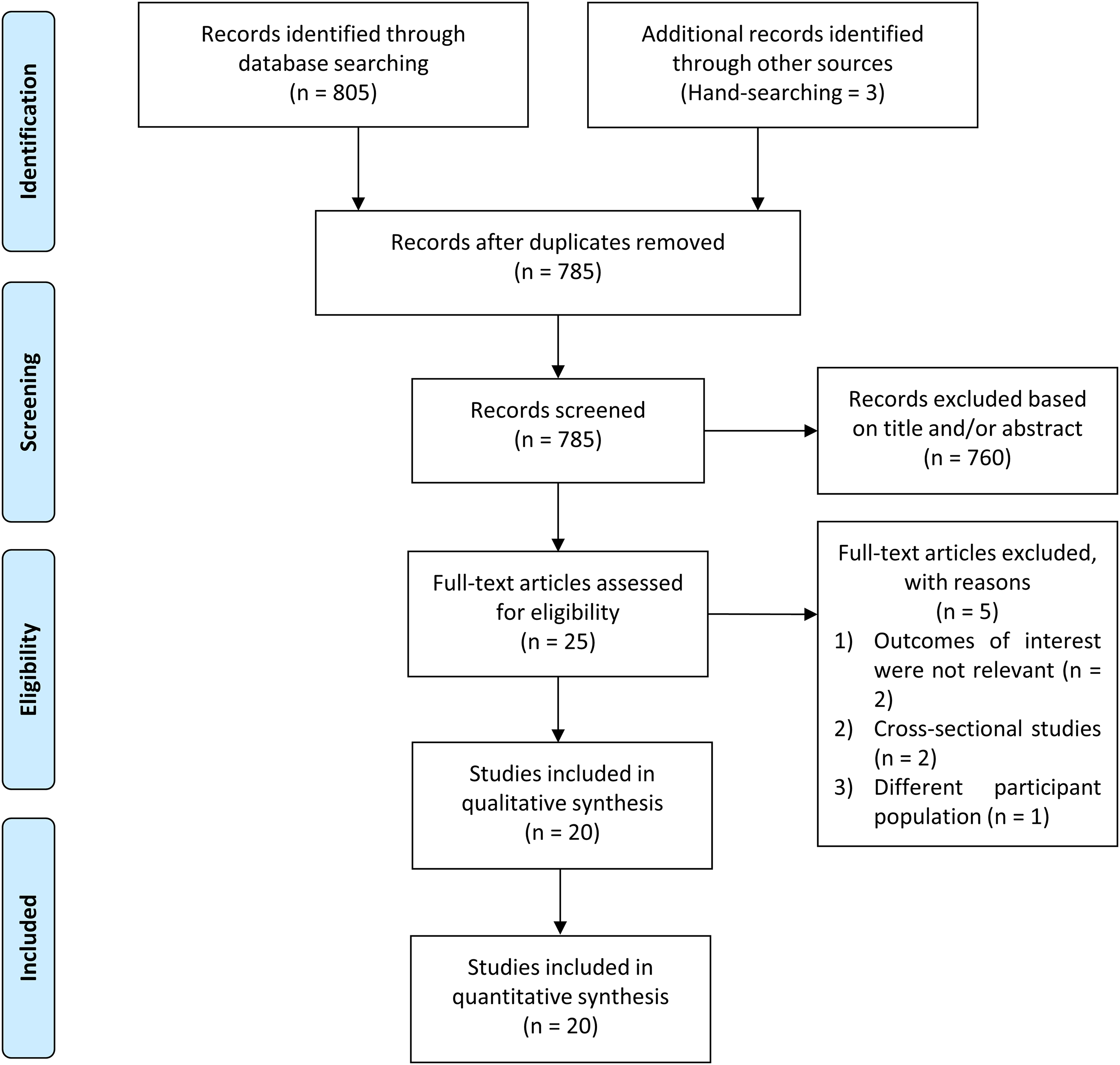
Flow chart of study selection.
Eligibility Criteria and Outcomes of Interest
This meta-analysis comprised prospective or retrospective comparative studies that explored the connection between iron deficiency anemia along with its indices (mean corpuscular volume, serum iron, total iron-binding capacity, ferritin) and febrile seizures. The study population included febrile seizure patients, who were defined as having a seizure between the ages of 6 and 60 months with a temperature of 38 °C or higher, that was not caused by a central nervous system infection or any metabolic imbalances, and who did not have a history of prior afebrile seizure. 1
The included articles had to delineate risk estimates with 95% confidence intervals (CIs) or sufficient data to calculate the effect size. To perform a diagnostic-test accuracy meta-analysis, the study must provide pertinent data on true positive and true negative rates to complete the statistical calculation related to the formula. Studies that did not report sufficient of the aforementioned data were omitted from our analysis. Review papers, editorials, comments, case reports/series, meta-analyses, and conference abstracts were excluded from our meta-analysis.
Data Extraction and Quality Assessment
Two separate authors then used a predesigned table to gather relevant data from the selected research. Extracted data comprised baseline and methodologic features of the studies involving the first author's name, the country in which the study was conducted, total participants, age, sex, iron deficiency anemia definition, iron deficiency anemia prevalence, iron deficiency anemia indices and their cutoff values, and family history of febrile seizures, along with duration of follow-up.
The Newcastle-Ottawa Scale (NOS) was used by 2 writers to independently assess the risk of bias in each study. 21 A study with a total score of 7 or higher is thought to have a low likelihood of bias. Otherwise, a study with a total score of 6 or less was judged to be biased and was removed from the study. Quality rating disagreements were resolved by discussion with a third reviewer.
Statistical Analysis
Stata (Software for Statistics and Data Science) software, version 17.0, was used to conduct statistical analysis. This meta-analysis’s effect size was expressed as odds ratios (ORs) with 95% CI. Restricted maximum likelihood method and random effects models were used to pool the overall effect size despite their heterogeneity. Mean differences were translated into effect sizes using the Cohen method and the random effects inverse variance model with DerSimonian-Laird estimate. The I2 index was used to assess inter-study heterogeneity, and an I2 statistic >50% or P value <.10 indicated substantial heterogeneity. We also used the potential covariates listed in the preceding subheading (eg, age, male sex, family history of febrile seizures) to run restricted maximum likelihood meta-regression in order to evaluate potential causes of heterogeneity among included studies. Furthermore, any statistically significant confounding factors will be included in the subgroup analysis and divided through median-split approach.
A diagnostic-test accuracy meta-analysis was also performed to calculate the sensitivity and specificity of each iron deficiency anemia index. A summary receiver operating characteristic curve was drawn to assess the overall diagnostic accuracy. The higher the area under curve value, the better the prognostic power. All statistical analyses were 2-sided, with a P value of <.05 indicating statistical significance.
Results
Study Selection and Baseline Characteristics
We identified 808 studies in our initial search, 3 of which were discovered via the hand-searching process, and 785 studies remained after duplicates were removed. Because we used the minimum keywords in order to maximize the search results, the number of research dropped dramatically from 785 studies to 25 studies. During this preinclusion screening, the majority of the eliminated studies comprised irrelevant titles, conference abstracts, unrelated laboratory parameters, and review studies. Conclusively, following a screening procedure based on predetermined inclusion criteria, 20 case-control studies with a total of 3856 participants were incorporated in this meta-analysis (Figure 1). The mean age of participants in the case group was older (23.2 months old) than in the control group (22.9 months old), and 52.4% of the participants were male, with a mean duration of follow-up 17.4 months. The prevalence of iron deficiency anemia in our study was also predominantly found in the case group (38.7%) rather than in the control group (24.3%). Baseline characteristics of the included studies are provided in Table 1.
Baseline Characteristics of the Included Studies (Case vs Control).
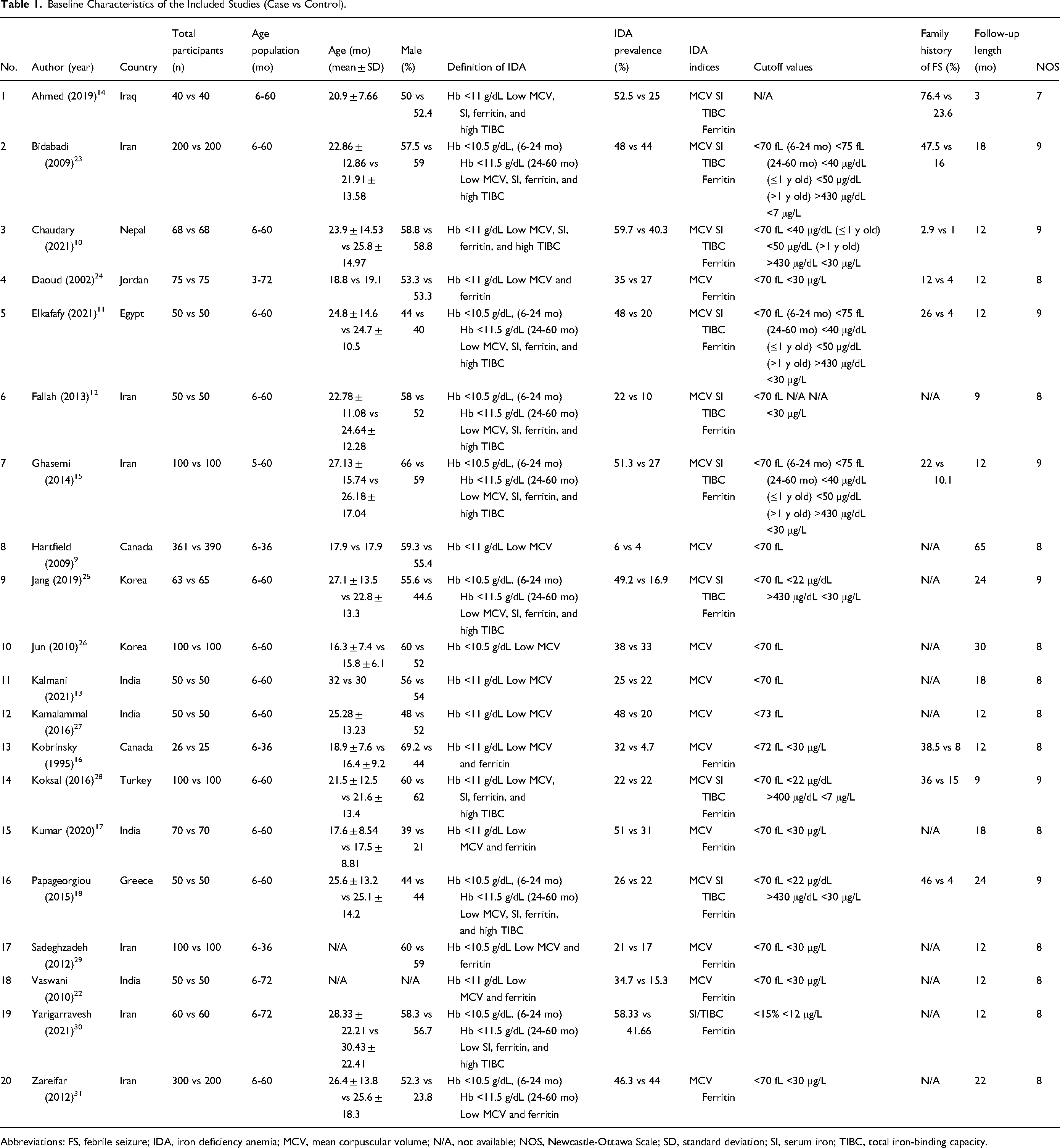
Abbreviations: FS, febrile seizure; IDA, iron deficiency anemia; MCV, mean corpuscular volume; N/A, not available; NOS, Newcastle-Ottawa Scale; SD, standard deviation; SI, serum iron; TIBC, total iron-binding capacity.
Iron Deficiency Anemia and Febrile Seizures
A total of 20 case-control studies evaluated the correlation between iron deficiency anemia and febrile seizures. We observed that patients who have iron deficiency anemia have a greater risk of febrile seizures (OR 1.33, 95% CI 1.18-1.50; P < .001; I2 = 77.1%, P-heterogeneity < .001). Significant heterogeneity was markedly observed in the risk estimates process. Further pooled research based on the country development status revealed the origin of heterogeneity derived from the developing countries studies (OR 1.33, 95% CI 1.14-1.56; P < .001; I2 = 84.2%, P-heterogeneity < .001) and demonstrated that the pooled OR in this aforementioned subgroup was greater than the pooled OR in the developed countries subgroup (OR 1.31, 95% CI 1.16-1.49; P < .001; I2 = 9.9%, P-heterogeneity = 0.353) (Figure 2).
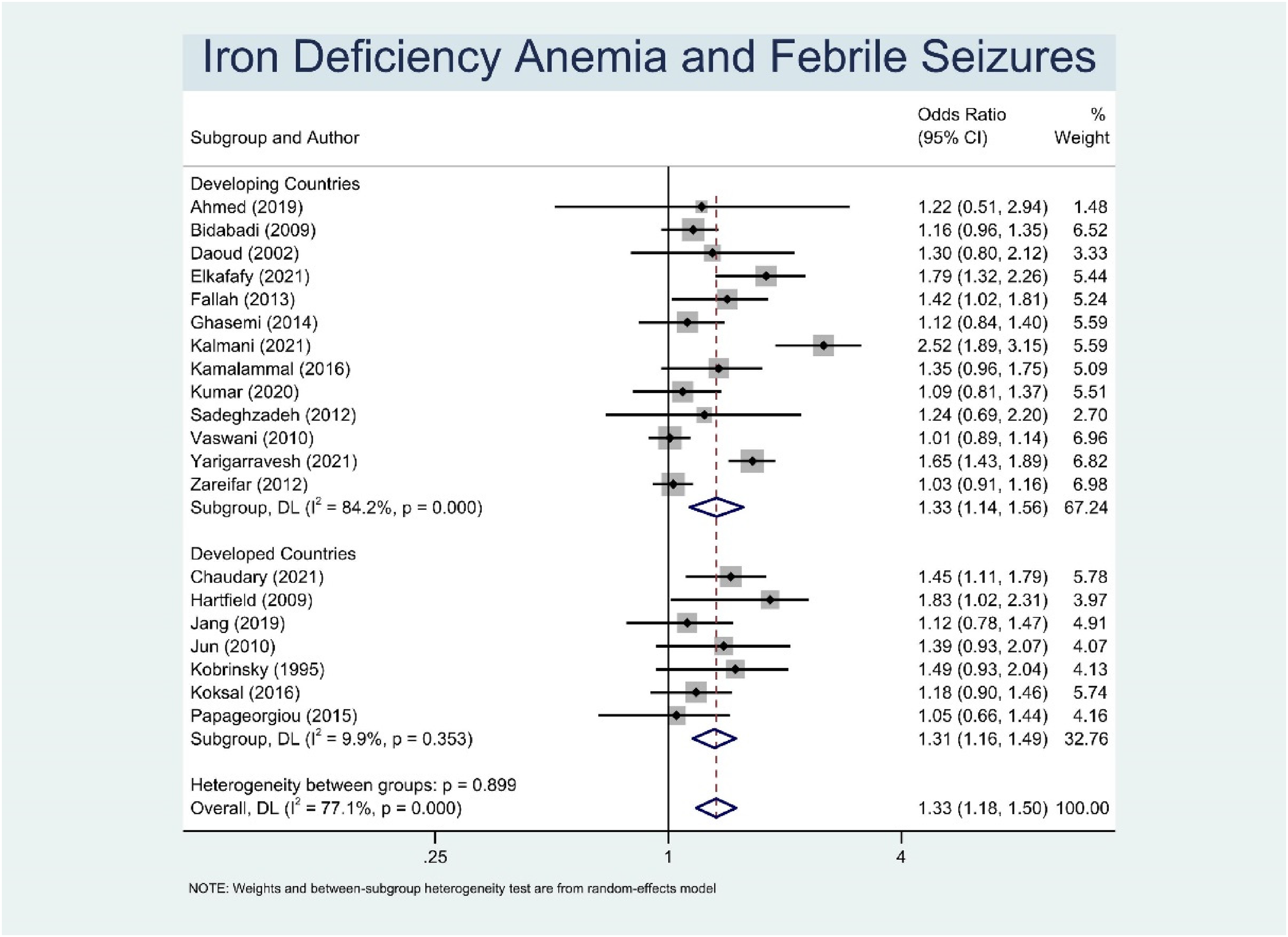
Pooled odds ratios for iron deficiency anemia (IDA) and febrile seizures (FS).
Meta-regression Analysis
An additional meta-regression analysis was carried out to discover if there was a link between potential covariates and outcomes of interest in this study. Our findings revealed that the correlation between iron deficiency anemia and febrile seizures was affected by male sex (P < .05), but not age and family history of febrile seizures. Subgroup analysis for studies with a percentage of males >57.5% (median value) had higher OR for febrile seizures (OR 1.41, 95% CI 1.26-1.58; P < .001; I2 = 31.2%, P-heterogeneity = .169) compared to ≤57.5% (OR 1.32, 95% CI 1.08-1.60; P = .006; I2 = 81.5%, P-heterogeneity < .001). The effect of iron deficiency anemia in the occurrence of febrile seizures will increase as the number of males in the study increases, as illustrated in the bubble plot analysis. One research was omitted from the analysis owing to a lack of data on the number of male sex 22 (Figure 3).
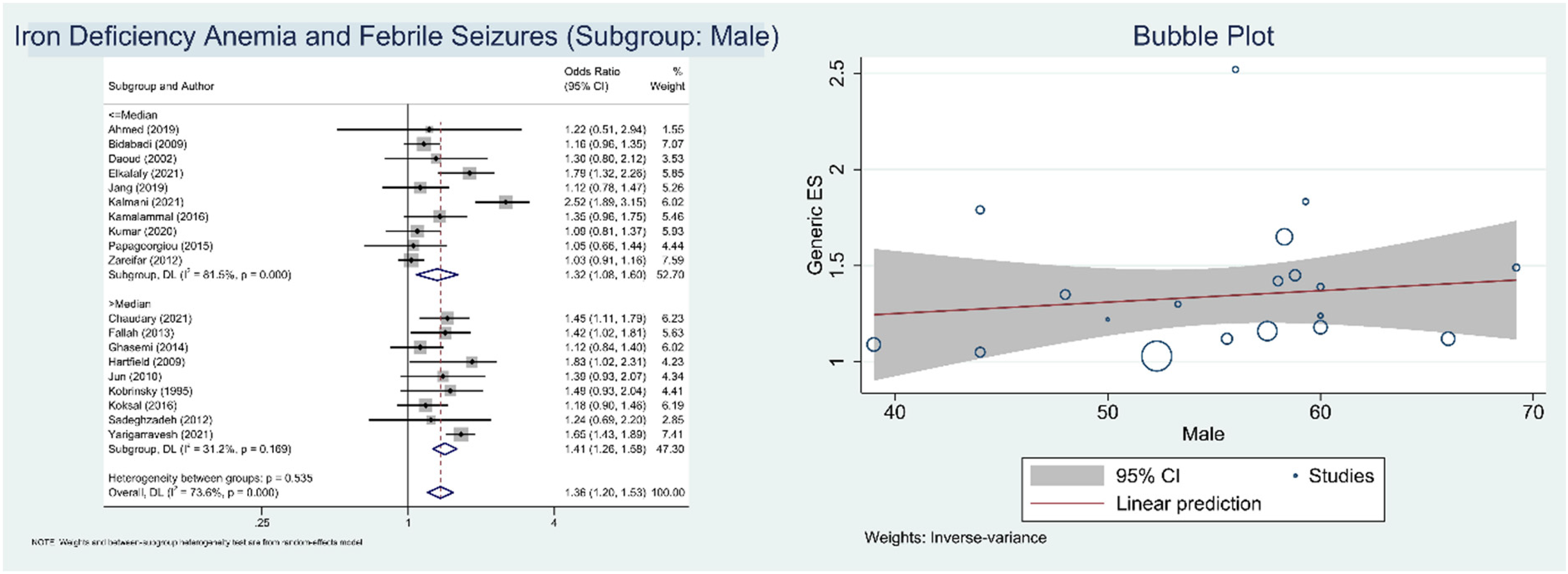
Pooled odds ratios and bubble plot for iron deficiency anemia (IDA) and febrile seizures (FS) based on male population subgroup.
Low Mean Corpuscular Volume and Febrile Seizures
The sum total of 19 studies were involved in regard to determining the correlation between low mean corpuscular volume and febrile seizures. Our pooled results suggest that population with low mean corpuscular volume had a significant increased risk of febrile seizures (OR 1.28, 95% CI 1.16-1.43; P < .001; I2 = 63.4%, P-heterogeneity < .001) when compared to the control subjects. Subgroup analysis based on country development status also disclosed the source of heterogeneity arising from the developing countries studies (OR 1.33, 95% CI 1.15-1.53; P < .001; I2 = 73.7%, P-heterogeneity < .001) and found that the pooled OR in this abovementioned subgroup was higher than the pooled OR in the developed countries subgroup (OR 1.23, 95% CI 1.09-1.39; P = .001; I2 = 0.0%, P-heterogeneity = .630). Furthermore, diagnostic-test accuracy meta-analysis results showed that low mean corpuscular volume had a sensitivity of 35% (95% CI 28%-43%), specificity of 76% (95% CI 70%-82%), and area under the curve of 0.61 (95% CI 0.57-0.65) in correlation with febrile seizures (Figure 4).
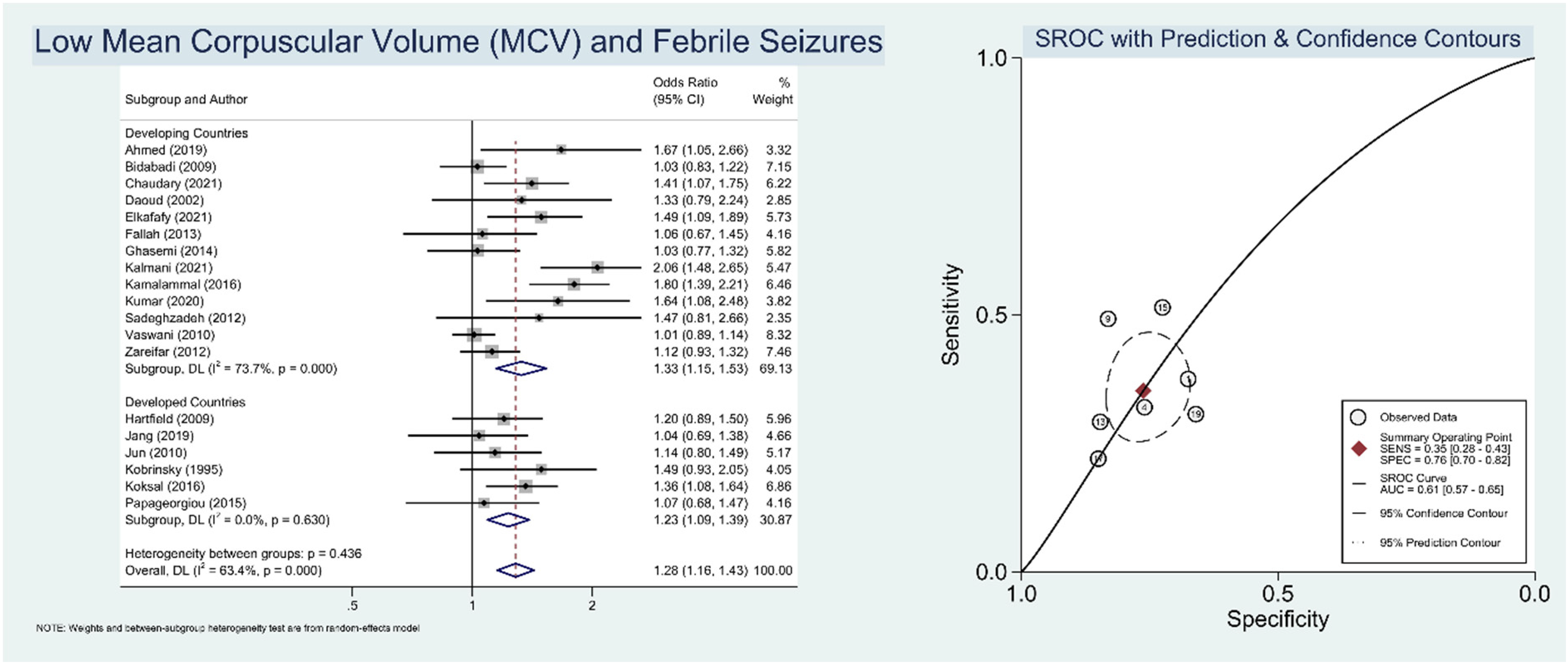
Pooled odds ratios and summary of receiver operating characteristic (SROC) curve for low mean corpuscular volume (MCV) and febrile seizures (FS).
Low Serum Iron and Febrile Seizures
Our merged analysis of 10 case-control studies revealed that low serum iron was significantly associated with febrile seizures (OR 1.31, 95% CI 1.17-1.48; P < .001; I2 = 69.1%, P-heterogeneity = .001). Additionally, subgroup analysis based on country development status in the developing countries showed a higher increment in the risk of febrile seizures (OR 1.32, 95% CI 1.08-1.68; P = .006; I2 = 81.3%, P-heterogeneity < .001) than in the developed countries subgroup (OR 1.31, 95% CI 1.19-1.43; P < .001; I2 = 0.0%, P-heterogeneity = .703), and was deemed as the source of inter-study heterogeneity. Pooling research based on the prognostic performance showed that low serum iron had a sensitivity of 52% (95% CI 29%-74%), specificity of 75% (95% CI 55%-88%), and area under the curve of 0.69 (95% CI 0.65-0.73) (Figure 5).
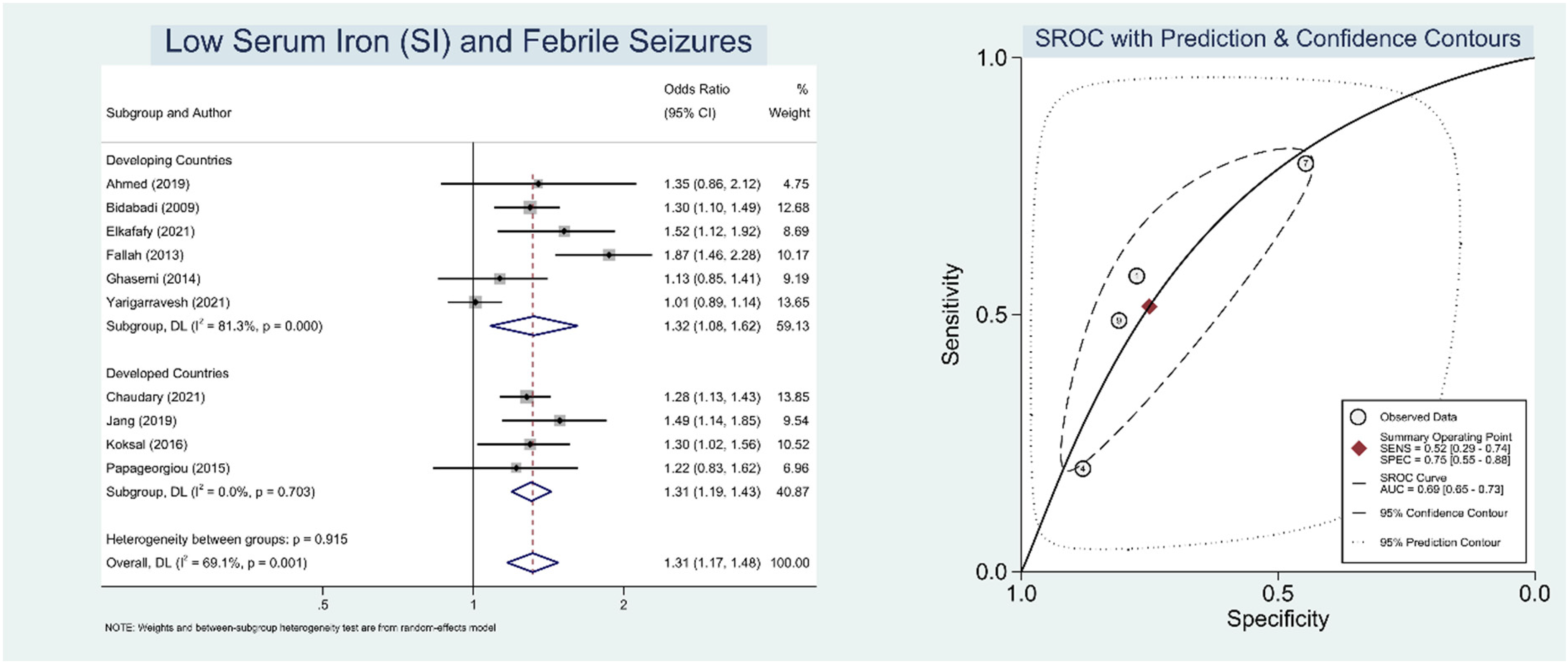
Pooled odds ratios and summary of receiver operating characteristic (SROC) curve for low serum iron (SI) and febrile seizures (FS).
High Total Iron-Binding Capacity and Febrile Seizures
The summary ORs of high total iron-binding capacity in the occurrence of febrile seizures was (OR 1.24, 95% CI 1.10-1.40; P < .001; I2 = 61.6%, P-heterogeneity = .005). The risk estimation procedure revealed significant heterogeneity. Pooled research based on country development status identifying the source of heterogeneity came from developing countries studies (OR 1.26, 95% CI 1.05-1.50; P = .011; I2 = 71.8%, P-heterogeneity = .003) and confirmed that the pooled OR in this aforesaid subgroup was larger than the pooled OR in the developed countries subgroup as well (OR 1.21, 95% CI 1.03-1.43; P = .020; I2 = 45.0%, P-heterogeneity = .142). Pertaining to its prognostic value, it was revealed that high total iron-binding capacity had a sensitivity of 58% (95% CI 48%-67%), specificity of 68% (95% CI 68%-76%), and AUC of 0.67 (95% CI 0.63-0.71) (Figure 6).
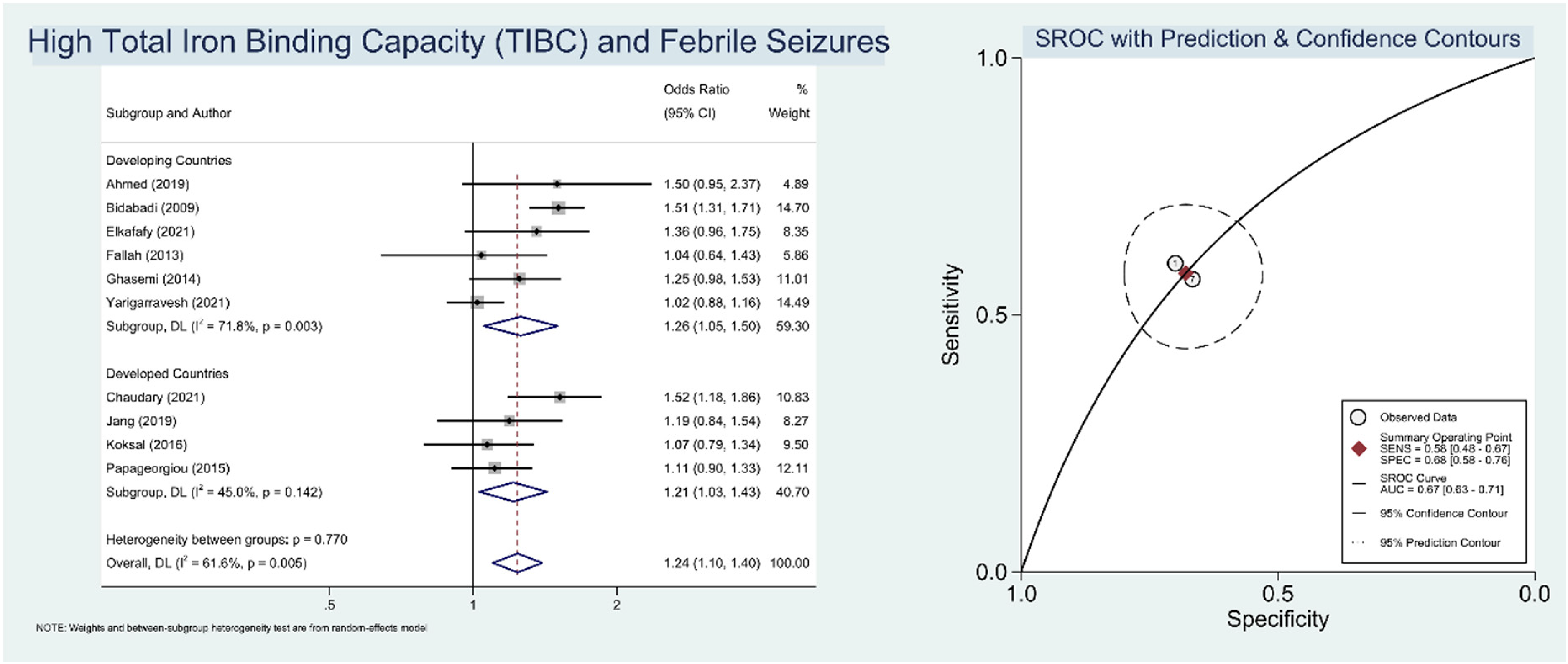
Pooled odds ratios and summary of receiver operating characteristic (SROC) curve for high total iron-binding capacity (TIBC) and febrile seizures (FS).
Low Ferritin and Febrile Seizures
In this meta-analysis, a substantial increase in the risk of febrile seizures in those who had low ferritin level was disclosed (OR 1.59, 95% CI 1.36-1.72; P < .001; I2 = 73.5%, P-heterogeneity < .001). Furthermore, subgroup analysis based on nation development status in developing countries revealed a greater increase in the risk of febrile seizures (OR 1.63, 95% CI 1.36-1.94; P < .001; I2 = 80.9%, P-heterogeneity < .001) than in the developed countries subgroup (OR 1.53, 95% CI 1.36-1.72; P < .001; I2 = 0.0%, P-heterogeneity = .534), a result that was attributed to the source of interstudy heterogeneity. The pooled sensitivity and specificity were 57% (95% CI 31%-80%) and 82% (95% CI 74%-88%), respectively. The area under the curve of the low ferritin level was 0.82 (95% CI 0.78-0.85), indicating the highest prognostic value among the other iron deficiency anemia indices (Figure 7).
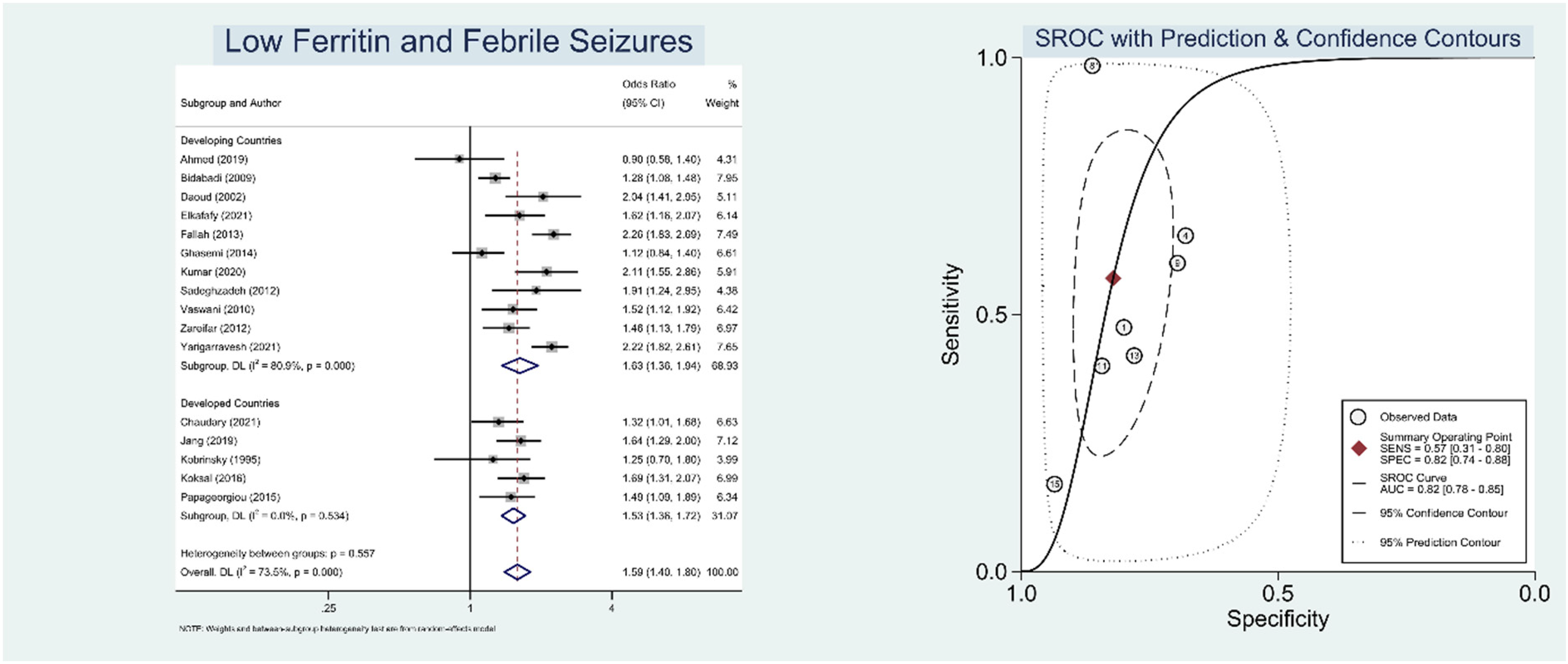
Pooled odds ratios and summary of receiver operating characteristic (SROC) curve for low ferritin level and febrile seizures (FS).
Table 2 presents the overall diagnostic-test accuracy meta-analysis findings of several iron deficiency anemia indices in relation with febrile seizures.
Summary Results of Diagnostic-Test Accuracy Meta-analysis.
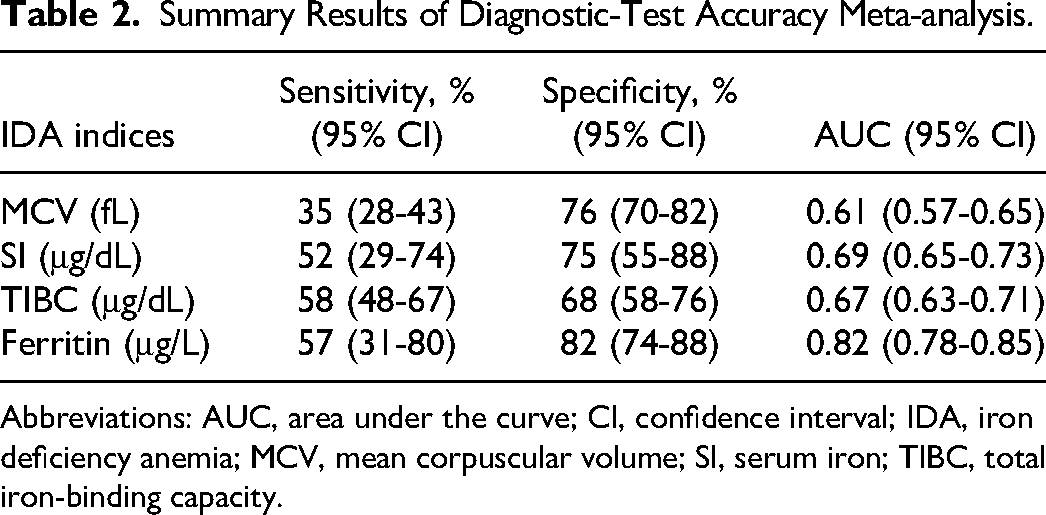
Abbreviations: AUC, area under the curve; CI, confidence interval; IDA, iron deficiency anemia; MCV, mean corpuscular volume; SI, serum iron; TIBC, total iron-binding capacity.
Discussion
This present study is a contemporary and comprehensive systematic review and meta-analysis of case-control studies aimed at determining the association between iron deficiency anemia and its indices, along with febrile seizures in child population. The following are the main findings of this meta-analysis. To commence, our study found that patients with febrile seizures were more likely to have higher prevalence of iron deficiency anemia in comparison to the control group. Second, iron deficiency anemia significantly raised the likelihood of developing febrile seizures. Eventually, our meta-analysis based on iron deficiency anemia indices demonstrated a significant relationship between low mean corpuscular volume, low serum iron, high total iron-binding capacity, and low ferritin and febrile seizures.
Several hypotheses have been proposed to elucidate why iron deficiency in children may increase the risk of developing febrile seizures. For starters, iron status has been linked to children's overall health in terms of nutrition, neurodevelopmental growth, and immunity. Iron deficiency is related with growth disruption, neurodevelopmental delay, and may impair the enzymatic activities involved in deoxyribonucleic acid (DNA), ribonucleic acid (RNA), monoamine metabolism, and neurotransmitter generation and function. These disruptions may be associated to several consequences of iron deficiency in the developing brain including disrupted development of nerve cells, impeded energy metabolism, and delayed development of myelin sheath. Changes in synaptic neurotransmitter systems such as norepinephrine, dopamine, serotonin, glutamate, and γ-aminobutyric acid (GABA) have also been linked to iron deficiency. Dopamine metabolism alterations appear to have a role in increased neuronal excitability, which may increase the likelihood of initiating a seizure event.25,26,32,33
In terms of immunity, iron deficiency impairs the ability to mount an adequate immune response. Iron has a core role in immunosurveillance, because of its growth-promoting and differentiation-inducing features for immune cells and its interference with cell-mediated immunologic cascades and cytokines activities.34,35 Recent experimental and clinical findings done by Brock and Mulero 36 and Kuvibidila and Porretta, 37 demonstrate that fever exacerbates the negative effects of iron deficiency on the brain, implying that iron-deficient children may have a lower seizure threshold and an increased risk of subsequent brain damage.
Despite its positive findings and plausible explanations between these 2 prior-mentioned variables, there are a few key points to consider before drawing any conclusions from our study. Theoretically, age <1 year, male sex, and family history of febrile seizures can also contribute to increase the risk of febrile seizures in such populations. 5 Therefore, meta-regression analysis for possible confounders was also performed to ensure the true direct effect regarding the aforementioned variables. Our meta-regression showed that the association between iron deficiency anemia and febrile seizures was influenced by male sex but not age and family history of febrile seizures. The omission of age as a covariate in the relationship between these 2 variables within our study is due to the fact that the mean age amid our included studies is older than the risk factor listed above (23.8 months old). Furthermore, the paucity of information regarding family history of febrile seizures in some included studies is likely to have an influence on this covariate's negligible significance. The percentage of male sex, on the other hand, was directly proportionate to the effect of iron deficiency anemia on febrile seizures. In other words, the estimated effect of iron deficiency anemia on febrile seizures was greater in male-dominated populations. It was hypothesized that the presence of more prominent voltage-gated channels in men may contribute to the susceptibility to enhanced depolarization activity, which might also trigger a seizure event. Hence, the total risk in male populations is expected to be higher (Figure 3).38,39
Iron indices, as previously discussed, have been strongly linked to children's overall nutritional health. We exclusively conduct a meta-analysis in a subgroup manner based on the country's development status (as categorized by the United Nations 40 ), which is directly linked to the nation's socioeconomic level and so may indirectly represent children's nutritional health. Children are more prone to illnesses when they have poor dietary and socioeconomic status. These repeated illnesses have a severe impact on their physical and immune systems, trapping them in a vicious cycle. Limited living standards and high prevalence of infectious illnesses, all of which may contribute to the disastrous effects of iron deficiency, making this population more prone to febrile seizures.36,41 Our findings corroborate this evidence, indicating that the overall pooled ORs for the relationship between iron deficiency anemia and its indices along with febrile seizures were higher in the developing countries subgroup than in the developed countries subgroup (Figures 2 and 4-7). Fortunately, implementing a meta-analysis based on the above-mentioned subgroup markedly reduced the moderately high heterogeneity between each included study. The conceivable rationale is that most studies done in underdeveloped countries had a broad range of cutoff values for iron deficiency anemia indices and diverse statements in defining iron deficiency anemia.12,23,24,30 Nevertheless, most importantly, conducting a meta-analysis using this subgroup did not modify the overall effect sizes on any independent variables and preserved the statistical robustness of the interplay relationships across variables within.
To our knowledge, this is the first meta-analysis of diagnostic-test accuracy that has specifically studied the predictive values of each iron deficiency anemia index (mean corpuscular volume, serum iron, total iron-binding capacity, ferritin) in connection to febrile seizures. It is important to note that odds ratios cannot be used to evaluate the prognostic performance of prognostic indicators when identifying the best parameter for forecasting an event. For assessing and reporting a marker's diagnostic or prognostic potential, appropriate statistical methodologies such as sensitivity, specificity, and area under the curve are necessary. In this investigation, we observed that low ferritin levels had the greatest area under the curve value among the other iron deficiency anemia indices. Mean corpuscular volume is an unspecified laboratory value that only measures the average size and volume of a red blood cell. Serum iron and total iron-binding capacity fluctuate during the day and are affected by oral iron supplements and the quantity of iron in the food. To reduce variation, serum iron and total iron-binding capacity should be tested in the morning on an empty stomach.42,43 In addition to physiological changes, the World Health Organization (WHO) cannot establish the fixed cutoff values for these 2 indices because of a degree of interassay variability for serum iron and total iron-binding capacity measurements, for which transferrin saturation calculation seems to be the solution for deciphering this issue. Ferritin levels, on the other hand, are the most commonly deployed indicator for determining iron deficiency, as low ferritin concentrations directly reflect a state of iron depletion. However, it should be noted that ferritin is also an acute phase reactant, and serum concentration is increased in conditions of inflammation, which was primarily found in febrile seizures patients. Providentially, the WHO already assists in the interpretation of serum ferritin interpretations when an inflammatory condition occurs. To account for the rise in ferritin values induced by inflammation, one method is to elevate the cutoff value that identifies deficiency, commonly to 30 μg/L instead of 12 μg/L.44,45 It is fortunate that the majority of our included studies used a 30-μg/L cutoff to define iron deficiency anemia.10–12,15–18,22,24,25,29,31 This meta-analysis indicates that ferritin levels have a poor sensitivity but a good specificity in accordance with the diagnostic test accuracy meta-analysis. Thus, it is better utilized to rule in rather than rule out the probability of the aforementioned outcome of interest. As a result of our research findings, we can fairly infer that serum ferritin is indeed a reliable index in predicting febrile seizures.
This study has a number of advantages over prior meta-analyses. First, meta-regression analysis was used in this meta-analysis to confirm the actual direct impact regarding our variables of interest. Second, our study contained a sufficient number of studies to perform the subgroup analysis; thus, the results were able to explain the cause of the moderately high interstudy heterogeneity in the previous meta-analysis. Lastly, we also conducted a diagnostic-test accuracy meta-analysis in order to increase the robustness over previous studies related to this topic.
Several limitations still warrant consideration in this meta-analysis. First, all of the included research were retrospective studies; hence, it increases the likelihood of recall and selection bias. Second, significant heterogeneity was discovered in the analysis as a result of various cutoff values and diverse definitions of iron deficiency anemia. Fortunately, after we conducted subgroup analysis, the heterogeneity was significantly reduced, possibly because of more distinct conditions in the developing countries subgroup. Third, further observational studies with a multivariable-adjusted analyses and analyses of each febrile seizures subtype are expectantly to be pursued in fervor to better understand the association between iron deficiency anemia and febrile seizures.
Conclusion
In conclusion, this meta-analysis found that iron deficiency anemia and its indices are associated with the increased risk of febrile seizures in children. Moreover, low ferritin concentrations were denoted as a significant indicator for predicting febrile seizures. Further prospective observational studies evaluating the predictive value of iron deficiency anemia that implement iron supplementation and follow these patients to determine the expected course of recurrence of febrile seizures are needed to augment the findings of this meta-analysis.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738231170333 - Supplemental material for Anemia and Poor Iron Indices Are Associated With Susceptibility to Febrile Seizures in Children: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-jcn-10.1177_08830738231170333 for Anemia and Poor Iron Indices Are Associated With Susceptibility to Febrile Seizures in Children: A Systematic Review and Meta-analysis by Rini Sulviani, William Kamarullah, Sherly Dermawan and Helen Susanto in Journal of Child Neurology
Footnotes
Author Contributions
RS and WK conceived and designed the study. WK, SD, and HS performed study selection, data extraction, and interpreted the data. RS, WK, SD, and HS performed extensive search of relevant topics. WK performed statistical analysis. RS reviewed and extensively edited the manuscript. All authors contributed significantly to the writing of the manuscript. All authors approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.