
Abstract
Background
This study aimed to investigate the effects of Video-Based Action Observation Training and Live Action Observation Training on motor function, activity participation, and secondary outcome measures in children with spastic diparetic cerebral palsy (CP).
Materials and Methods
Thirty-nine children with spastic diparetic cerebral palsy, aged 5-14 years, with Gross Motor Function Classification System I-III, were distributed in equal numbers to any of the Video-Based Action Observation Training (conventional physiotherapy + Video-Based Action Observation Training), Live Action Observation Training (conventional physiotherapy + Live Action Observation Training), and control (conventional physiotherapy) groups through stratified randomization. For 8 weeks, action observation training groups received 20 minutes of conventional physiotherapy followed by 20 minutes of action observation training, and the control group received 40 minutes of conventional physiotherapy. Primary outcome measures were Gross Motor Function Measurement and Child and Adolescent Scale of Participation, secondary outcome measures were Pediatric Berg Balance Scale, timed-up-and-go test, five times sit-to-stand test (FTSST), Gillette Functional Assessment Questionnaire (GFAQ), and 1-minute walk test (1MWT).
Results
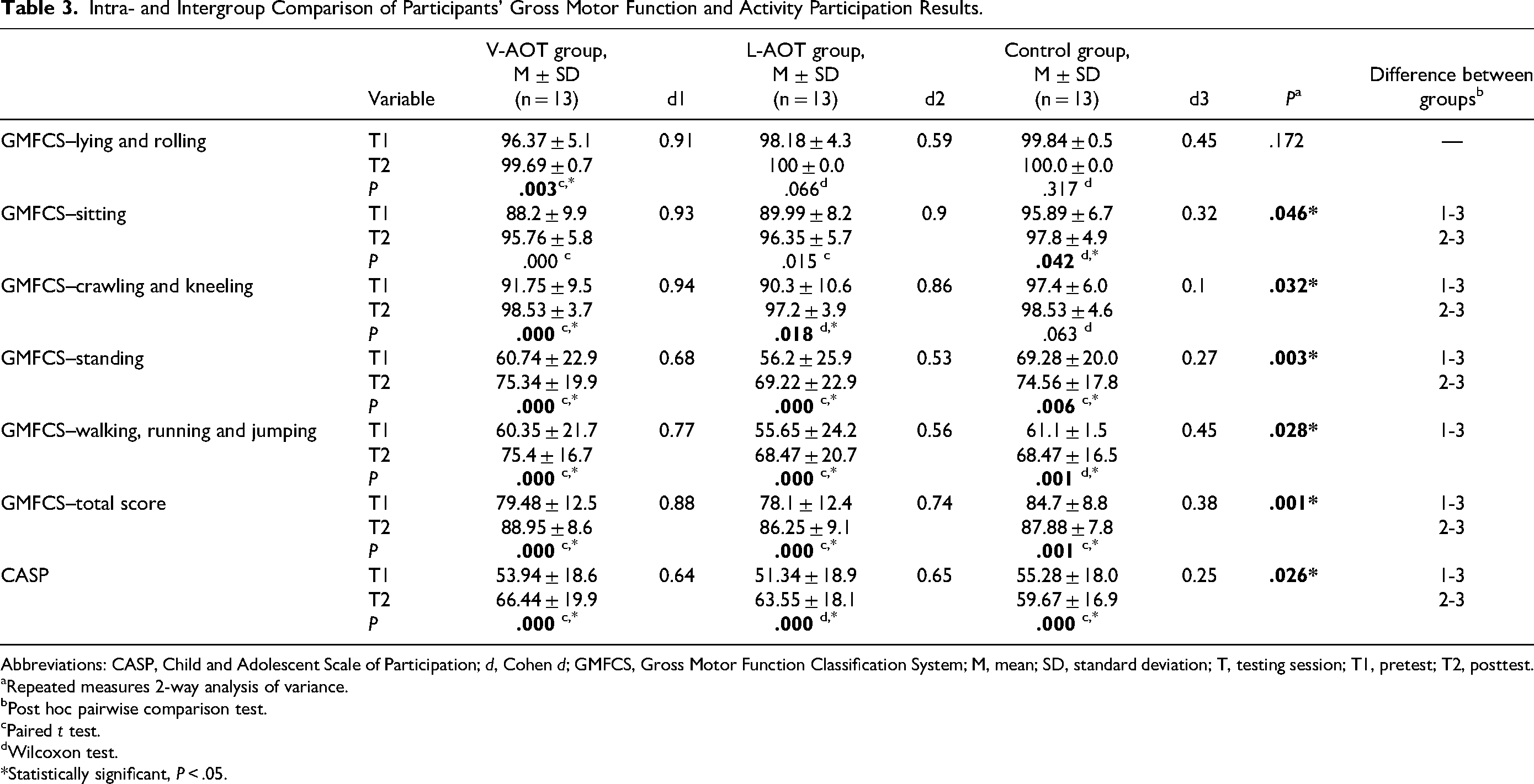
Improvements were observed in all other evaluation parameters of the groups except Gross Motor Function Measurement–lying and rolling (P = .066) in the Live Action Observation Training Group, and lying and rolling (P = .317) and crawling and kneeling (P = .063) motor subtests and Gillette Functional Assessment Questionnaire–walking scale (P = .513) in the control group. Comparisons of the increases in all other measurements between the groups, except for the dimensions of Gross Motor Function Measurement–lying and rolling (P = .172), were statistically significant (P < .05) and this difference was in favor of action observation training.
Conclusion
It was found that 2 different AOTs applied in addition to conventional physiotherapy in children with spastic diparetic cerebral palsy were more effective on all outcomes than was conventional physiotherapy alone.
Cerebral palsy (CP) is a permanent but nonprogressive disorder that occurs when the immature brain is affected by various reasons. 1 It has been reported that the most common subtype of cerebral palsy is spastic cerebral palsy (77%), whereas the most common subtype in the spastic group is bilateral spastic cerebral palsy (70%). 2 In diparetic type cerebral palsy, muscle weakness is evident in postural, antigravity, and core muscles, and muscle tone is increased in the lower extremities. 3 Insufficiency in movement experiences, and disruption of the agonist-antagonist muscle relationship, causes insufficiency in postural control, balance, and walking problems. 4 In children with cerebral palsy, the use of the upper extremities as a compensation mechanism increases with balance effects, and this is followed by limitation of movement of the extremities. This can cause limitations in performance and learning activities in activities of daily living, problems in movement, and limitations in social roles and participation in society. 5 Additionally, the abnormal trunk patterns they create to compensate while walking also negatively affect their functional skills and activation skills. 6
Various treatment methods are used to rehabilitate children with cerebral palsy. One of these, Action Observation Training (AOT), has recently been applied as a cognitive intervention method to improve motor skills in the rehabilitation of children with cerebral palsy. 7 Based on the mirror neuron system, action observation training is characterized by systematically repeated observation of actions and then reenacting the observed actions on demand. 7 Action observation training can be applied by showing previously recorded video recordings or images, or by repeating the actions live in front of the observer. 8 Action observation training is cognitively simpler than simply communicating verbal information and instinctive imitation can be elicited when patients closely observe the detailed limb coordination involved in performing the exercise. 8 Observing another person's movements causes activation in the sensorimotor system, resulting in behavioral changes and plasticity in these areas. 9 In addition, the fact that making the patients’ habitual motor control target-oriented provides some benefits and increases the retention effect indicates that the selection of actions to be shown during action observation training is important in the effectiveness of this approach. 10
There are studies demonstrating the positive effects of action observation training in the field of rehabilitation. Positive effects of action observation training in improving motor function have been reported mostly in stroke patients. 11 Studies show that action observation training is useful in the rehabilitation of children with cerebral palsy, but these studies mostly focused on the functional rehabilitation of the upper extremities in children with cerebral palsy. 7 There are limited studies investigating the effectiveness of action observation training in children with diparetic cerebral palsy. 12 Studies examining gross motor function, balance, and gait in the relevant population are insufficient.12,13 However, to our knowledge, no study has evaluated activity participation, functional muscle strength, and functional mobility and examined the effectiveness of 2 different AOTs.
In light of this information, our study aimed to examine the effects of 2 different AOTs on motor function, activity participation, balance, functional mobility, functional muscle strength, and walking ability in children with diparetic cerebral palsy by monitoring and repeating task-oriented actions and to compare them with conventional treatment.
Materials and Methods
Study Design
This study was planned as a single-blind and randomized controlled study to examine the effects of action observation training applied in different ways on motor function, activity participation, and secondary outcome measures in children with spastic diparetic cerebral palsy.
Participants
The inclusion criteria were as follows: (1) between the ages of 5 and 14 years, (2) a diagnosis of spastic diplegic cerebral palsy, (3) gross motor function levels ranging from I to III according to the Gross Motor Function Classification System, (4) havng the cognitive ability to follow the instructions given by researchers, (5) an Intelligence Quotient >70 (accessed from patient files), and (6) children without severe restrictions on joint movement. The exclusion criteria of the study were (1) presence of joint contracture, (2) presence of visual field defect and visual impairment, (3) having had a seizure in the past 6 months or uncontrolled seizure, and (4) presence of any orthopedic surgery and botulinum toxin injection in the past 6 months. Those who refused to participate in the study, could not comply with the treatment program, and left the treatment unfinished for various reasons were excluded from the study.
Sample Size and Randomization
NCSS PASS 13 program was used to calculate the sample size of the study. In this context, assuming that the difference in Gross Motor Function Measure (GMFM) value was 5.12 units with α=0.05 and 1 – β (power) = 0.80 in a previous study, 12 it was calculated that a total of 39 diparetic children with cerebral palsy should be included, with at least 13 children in each group.
The population of the research consisted of children with spastic diparetic cerebral palsy in all special education and rehabilitation centers in Bingöl province between the data collection dates. Children who agreed to participate in the study and met the inclusion criteria were assigned to groups (Video-Based Action Observation Training [V-AOT], Live Action Observation Training [L-AOT], or control) with an equal number of children by stratified randomization method according to Gross Motor Function Classification System. Which case with the same Gross Motor Function Classification System level was selected to which group was made according to the simple random sampling method.
Interventions
All participants received treatment for 40 minutes, 2 days a week for 8 weeks. Experimental groups received 20 minutes of action observation training following a 20-minute conventional physiotherapy program in each session. The control group received only conventional physiotherapy. All patients were given an additional weekly home program and the home program was followed via WhatsApp. The children in the groups did not receive any treatment program other than this program.
Video-Based Action Observation Training (Group 1)
Participants were asked to watch the actions shown in the video on a 17-inch laptop screen from a distance of 50 cm and not to perform the actions while watching. To ensure clear movement, the model was shot from the closest distance, including the whole body. The videos were watched in a quiet environment, with the child sitting on a chair in the most comfortable position. They were instructed to concentrate on the video at 1-minute intervals to increase attention span, and all experiments were performed by the same researcher from the beginning to the end of the experiment. During action observation training, another physical therapist stood next to/behind the patient to ensure their safety.
There is no specific protocol for action observation training content in children with diparetic cerebral palsy. In terms of action observation training standardization, a general action observation training protocol and videos of physiotherapy-oriented training models prepared within the scope of this protocol were created by the physiotherapist treating the child, accompanied by current literature.12–14 However, taking into account the functional levels and functional disabilities of children with cerebral palsy, individual-specific protocols were created within the general protocol, including task-oriented functional movements of increasing difficulty level and variety, to maintain functional equivalence and adapt to learning.
The action observation training protocol was created in 4 main parts:
Part 1: Activities to improve balance in a sitting position Part 2: Sitting to standing activities Part 3: Activities to improve balance and weight bearing in a standing position Part 4: Walking activities
The movement was recorded from the front, side, and back to ensure the child understood the movement correctly. Considering that the same movement had to be repeated several times, 4 movements were determined for each video recording and a duration of 3 minutes for each movement. After 3 minutes of repeated observation of each activity, children were asked to carry out what they observed for 1 minute and then take a 1-minute break. It was said that the quality of the imitations was not the goal of rehabilitation. Video of each step was watched all week long. Each episode was performed over 2 weeks (Figure 1).
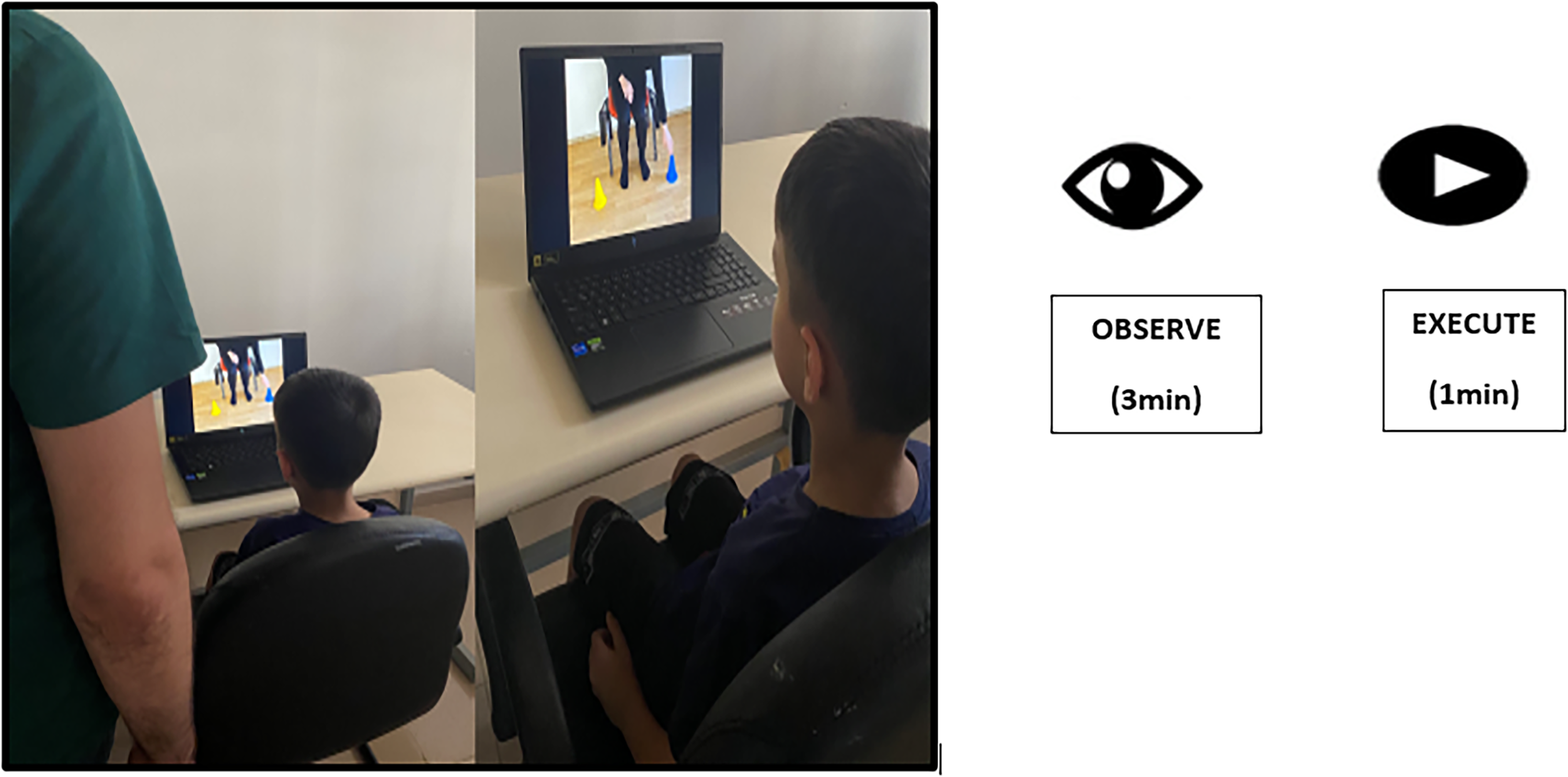
Experimental set-up for the video-based action observation training group.
Live Action Observation Training (Group 2)
Repeating the actions in the video, the same researcher sat facing the child and performed the tasks while the child watched. Subsequent experimental procedures were the same as for the Video-Based Action Observation Training group.
Conventional Physiotherapy (Group 3)
Conventional physiotherapy practice was created as a result of a literature review and our clinical experience. The content consisted of stretching and strengthening lower extremity muscles, strengthening upper extremity muscles, sitting and standing, trunk strengthening, standing weight bearing, walking, going up and down stairs, and balance exercises. The content consisted of stretching and strengthening lower extremity muscles, strengthening upper extremity muscles and trunk, sitting and standing, standing weight bearing, walking, going up and down stairs, postural control, and balance exercises. Stretching exercises were applied to the adductors, hamstrings, quadriceps, and calf muscles of both limbs. Additionally, active/passive range of motion exercises were performed for both lower limbs in a sitting and supine position. Strengthening exercises included the core muscles, hip abductors, hip extensors, hamstrings, and quadriceps. Postural control and balance exercises incorporated walking in all directions, as well as challenging stability in various positions such as kneeling, half-kneeling, standing on uneven and soft surfaces, stepping, standing, standing on one leg, and walking. Walking exercises included tandem walking, walking on different surfaces, and walking between obstacles.
Outcome Measures
The content of the survey form prepared in line with the literature is as follows: gender, age (years), weight (kg), height (cm), body mass index (BMI), prenatal-natal-postnatal history, botulinum toxin A history, assistive device use, presence of medication use, and how long physical therapy has been received. Evaluations were made by a physiotherapist with pediatric rehabilitation experience immediately before the study and at the end of the 8-week rehabilitation period.
Primary Outcomes
Gross motor function was assessed with the Gross Motor Function Measurement (GMFM). The scale consists of 5 parts: A, Lying and rolling (17), B: Sitting(20), C, Crawling and kneeling (14), D: Standing (13) and E: Walking, running and jumping (24). Maximum total score is 264. 15
The Child and Adolescent Scale of Participation was used to measure activity participation. The Child and Adolescent Scale of Participation is a valid outcome measure for individuals with acute cerebral injury or other disability. A high score indicates a high level of participation. 16
Secondary Outcomes
The Pediatric Berg Balance Scale was used to assess balance function. A higher score indicates better balance. The Pediatric Berg Balance Scale is used as a scale with high reliability and validity in the pediatric population. 17
A timed-up-and-go test (TUG) was used to evaluate functional mobility. The child was seated in a chair without arm support but with back support, 3 m away from the wall, with the hip and knee joints in a 90° flexion position. The child was asked to get up from the chair, walk at his normal pace, touch the sign on the wall, and then come back and sit down, and the elapsed time was noted. The average of 3 trials was taken and the duration was recorded in seconds. Walking aid users were evaluated with walking aids. 18
Five times sit-to-stand test (FTSST) was used to evaluate functional muscle strength. Participants sat in a height-adjustable chair with their arms, right hand over the left shoulder, and left hand over the right shoulder. The starting position was standardized at hip 90° flexion and knee 105° flexion. 19 They were then asked to stand up and sit down five times as quickly as possible and the time was recorded with a stopwatch (seconds). 19 Subjects classified as Gross Motor Function Classification System III were allowed to use assistive devices during testing. Three repetitions of the test were conducted, and data analysis was done using the average result.
Gillette Functional Assessment Questionnaire (GFAQ) and 1-minute walk test were used to evaluate functional walking. Gillette Functional Assessment Questionnaire includes the Walking Scale, which classifies a person's ambulation ability into 10 levels, and the 22-item skill subtests that measure functional locomotor activity. 20 In the Gillette Functional Assessment Questionnaire–walking subscale, each score corresponds to a functional level: 1 is the lowest functional score and means that the child cannot take a step; 10 means that the child can walk and run without difficulty. In the FAQ-Skill Test, answers are given according to a Likert-type answer scale (easy, somewhat difficult, very difficult, not at all possible, and too small for the activity). For the 1-minute walk test, children were evaluated using walking aids, if any. The child was asked to walk as fast as he could without running for 1 minute. The test was repeated 3 times in a row and their average (meters) was taken. 21
Statistical Analysis
Statistical analyses were performed using SPSS program version 25. Descriptive statistics were summarized using mean ± standard deviation for normally distributed variables, and numbers, ratios, and percentages for categorical (ordinal and nominal) variables. The suitability of the data to normal distribution was examined using analytical (Shapiro Wilk) and visual (probability and histogram graphs) methods. Baseline clinical and demographic characteristics between groups were analyzed by 1-way analysis of variance and Kruskal-Wallis tests. Changes within the group after treatment were determined using the Student t test and the Wilcoxon test. Possible differences between the increases in the measured values of the groups before and after physiotherapy were determined using 2-way analysis of variance in repeated measurements (Group × Time). Mauchly sphericity test was used for the basic assumptions of 2-way analysis of variance. When the P value of this test was greater than .05, it was decided that the data was homogeneously distributed. If not, Greenhouse-Geisser or Huynh Feldt corrections were used. A post hoc test was applied for pairwise group comparison of the measurements that showed differences. The Mann-Whitney U test was used for paired comparisons between groups for nominal data. Finally, the effect of the interventions was calculated using Cohen d formula. Cohen d was interpreted as large (>0.8), moderate (0.5-0.8), small (0.2-0.5), or insignificant (<0.2). Statistics were considered significant when P < .05.
Results
A total of 39 children, 9 children in each group, were included in the analysis (Figure 2). Participants did not report any negative situations regarding treatment compliance throughout the study.
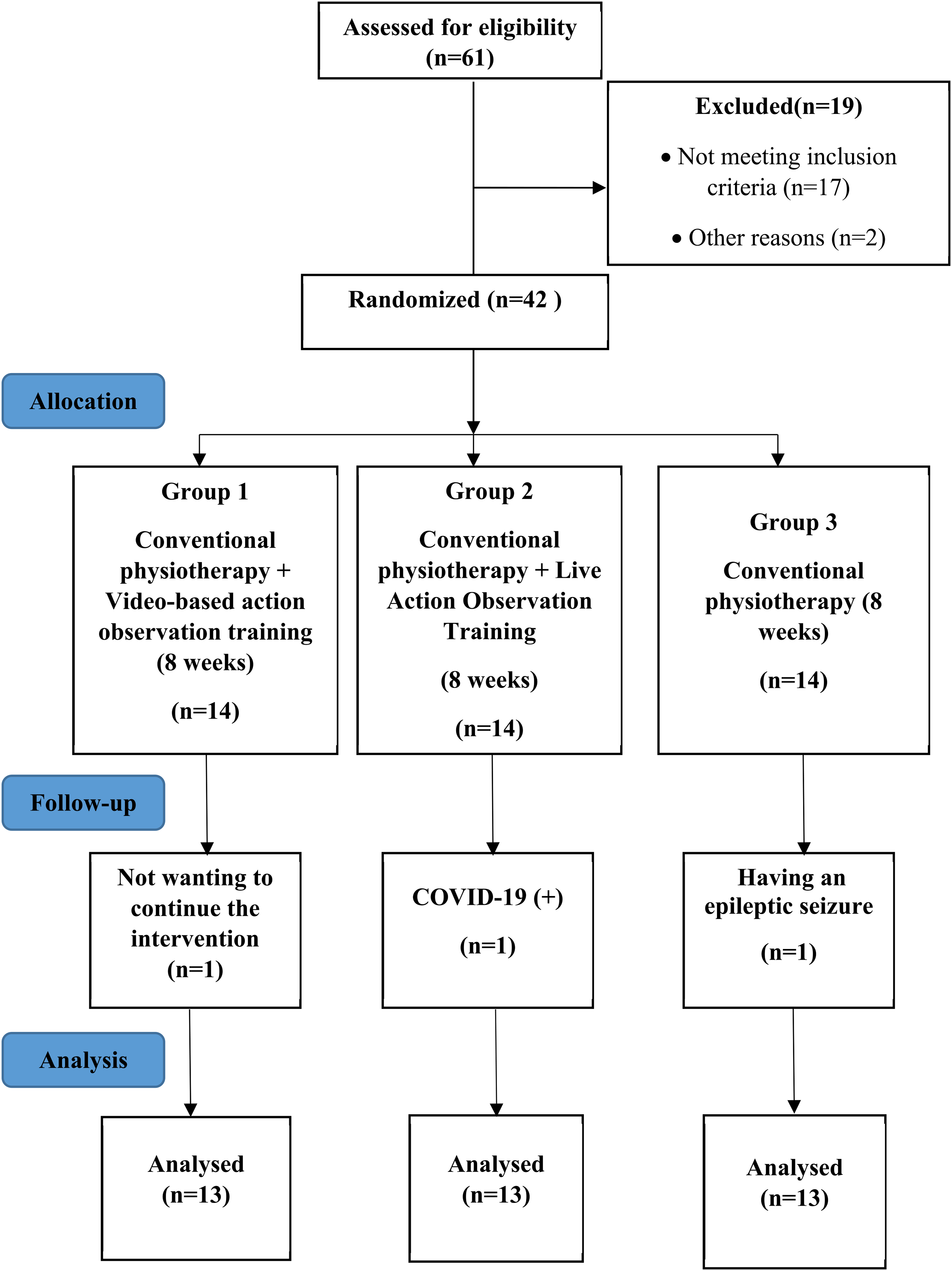
Flow chart (CONSORT flow diagram).
Baseline Comparisons
The demographic and clinical characteristics of the individuals and the comparison of these characteristics between the groups are summarized in Tables 1 and 2.
Comparison of Demographic and Physical Characteristics of Participants in Groups.
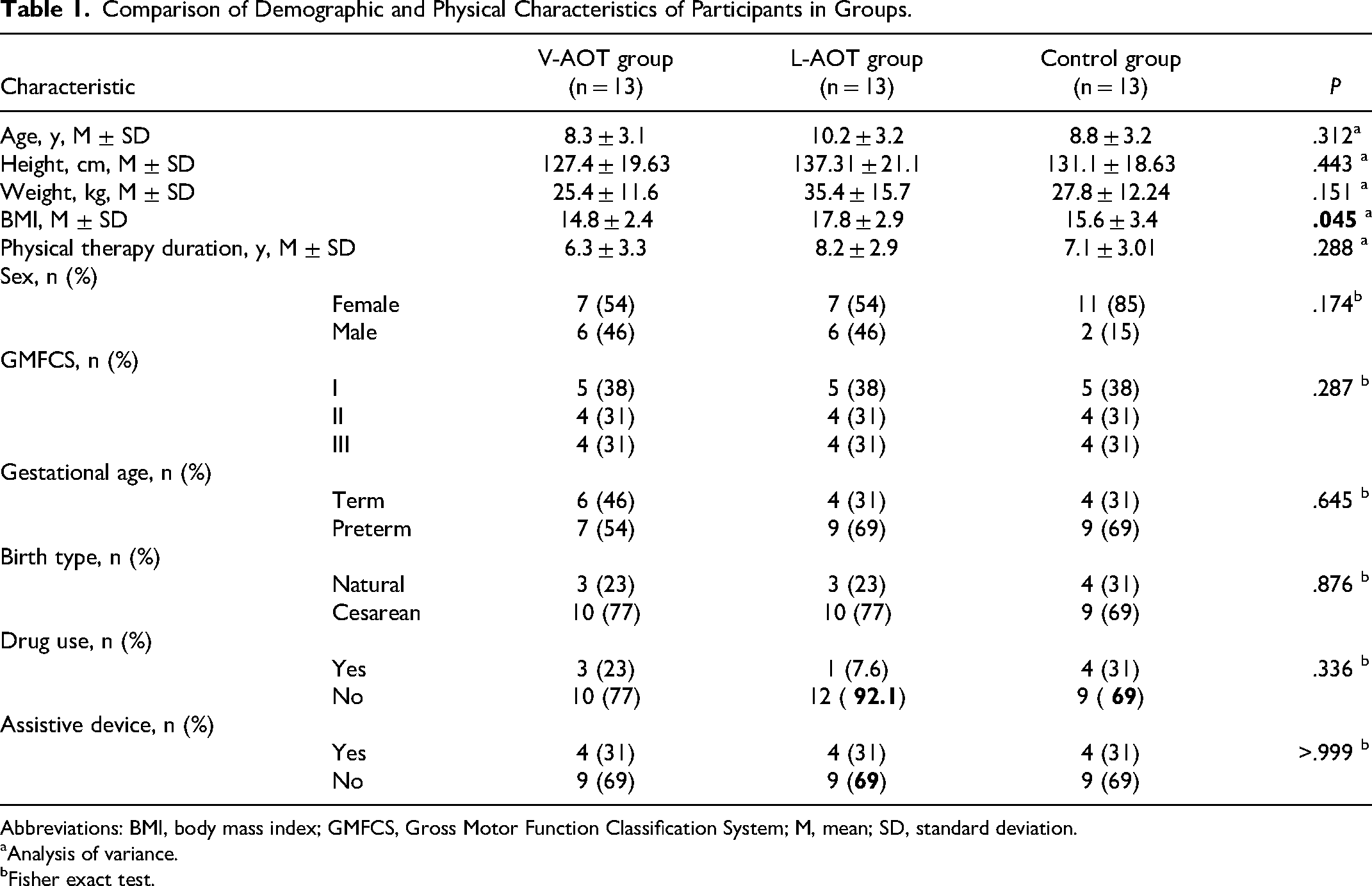
Abbreviations: BMI, body mass index; GMFCS, Gross Motor Function Classification System; M, mean; SD, standard deviation.
Analysis of variance.
Fisher exact test.
Comparison of Baseline Characteristics of Participants in the Groups as Determined by Measurement.
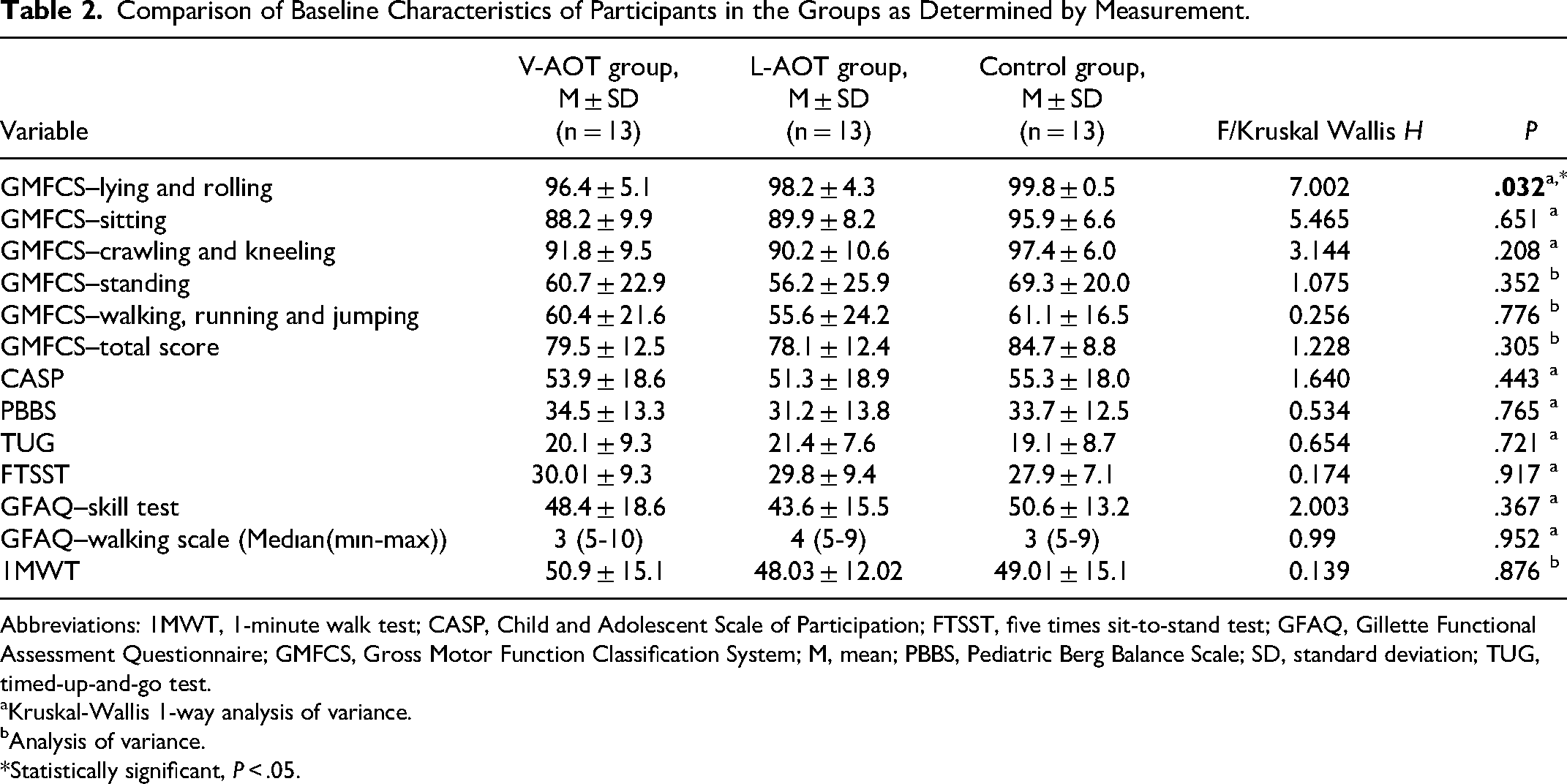
Abbreviations: 1MWT, 1-minute walk test; CASP, Child and Adolescent Scale of Participation; FTSST, five times sit-to-stand test; GFAQ, Gillette Functional Assessment Questionnaire; GMFCS, Gross Motor Function Classification System; M, mean; PBBS, Pediatric Berg Balance Scale; SD, standard deviation; TUG, timed-up-and-go test.
Kruskal-Wallis 1-way analysis of variance.
Analysis of variance.
Statistically significant, P < .05.
Primary Outcomes
A comparison of the participant's gross motor function and activity participation results within and between groups is shown in Table 3.
Intra- and Intergroup Comparison of Participants’ Gross Motor Function and Activity Participation Results.
Abbreviations: CASP, Child and Adolescent Scale of Participation; d, Cohen d; GMFCS, Gross Motor Function Classification System; M, mean; SD, standard deviation; T, testing session; T1, pretest; T2, posttest.
Repeated measures 2-way analysis of variance.
Post hoc pairwise comparison test.
Paired t test.
Wilcoxon test.
Statistically significant, P < .05.
Secondary Outcomes
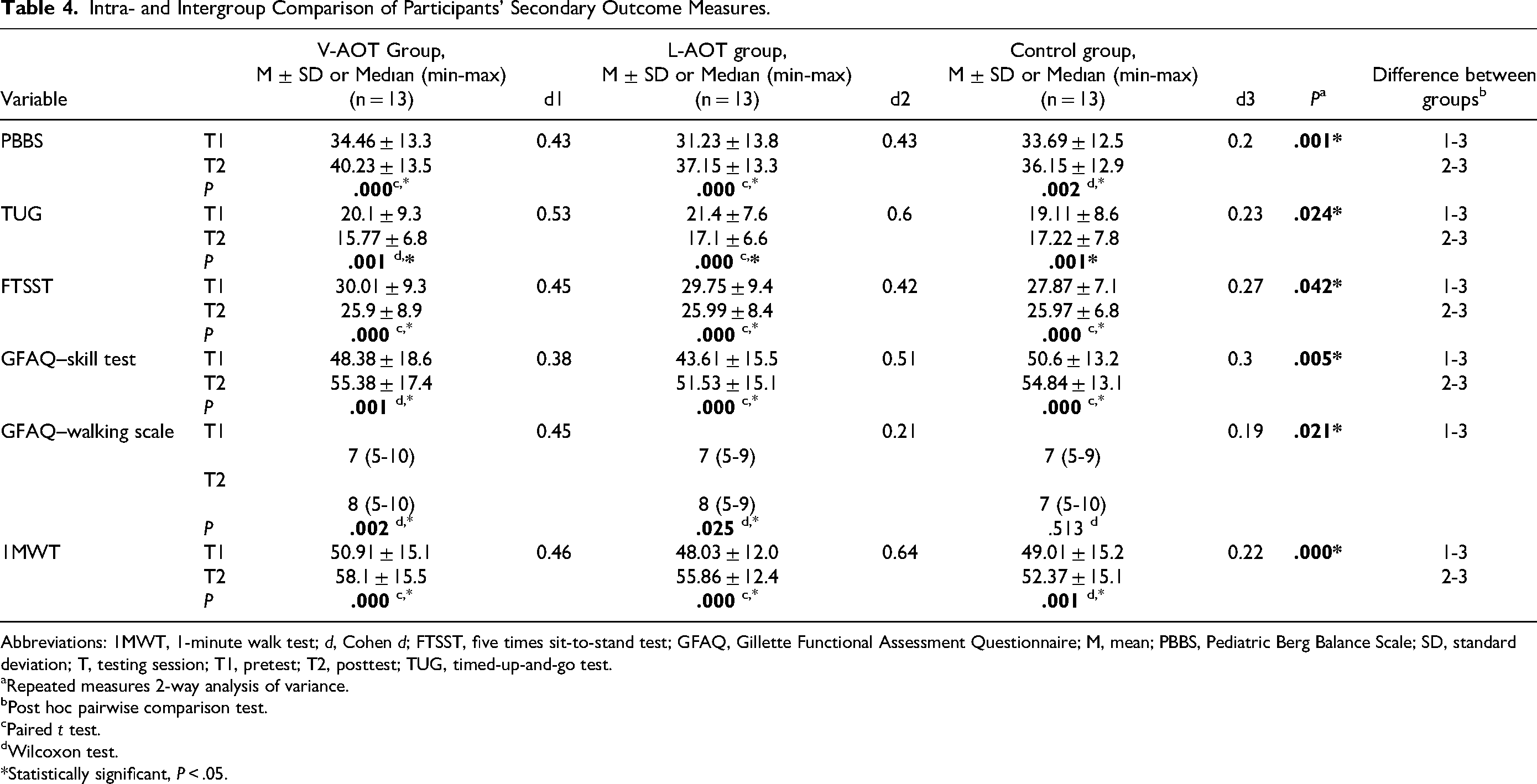
A comparison of the participants’ secondary outcome measures within and between groups is shown in Table 4.
Intra- and Intergroup Comparison of Participants’ Secondary Outcome Measures.
Abbreviations: 1MWT, 1-minute walk test; d, Cohen d; FTSST, five times sit-to-stand test; GFAQ, Gillette Functional Assessment Questionnaire; M, mean; PBBS, Pediatric Berg Balance Scale; SD, standard deviation; T, testing session; T1, pretest; T2, posttest; TUG, timed-up-and-go test.
Repeated measures 2-way analysis of variance.
Post hoc pairwise comparison test.
Paired t test.
Wilcoxon test.
Statistically significant, P < .05.
Discussion
This study aimed to see the functional results of action observation training applied in different ways by taking advantage of the changes caused by watching the actions in children with diparetic cerebral palsy. Action observation training applied in addition to conventional physiotherapy has been shown to produce better results than conventional physiotherapy alone on gross motor function, activity participation, and secondary outcome measures. Although Video-Based Action Observation Training was effective on gross motor function and Live Action Observation Training was effective on functional mobility, the effects of action observation training on walking ability were found to be variable, but it was observed that 2 different action observation trainings provided similar improvements in activity participation, functional balance, and functional muscle strength.
One of the main objectives of interventions for children with cerebral palsy is to improve motor functions and increase the performance of gross motor functions. 22 Studies on the effect of action observation training, one of the methods used for this purpose, on functional results in diparetic cerebral palsy are insufficient. No studies have been found that measure all Gross Motor Function Measurement substeps in the relevant population, and conflicting results have been revealed in existing studies.12,13,25 In a study, it was found that action observation training provided improvements in the motor function of children with diparetic cerebral palsy, but only in the standing substep, it revealed superior improvement than conventional physiotherapy. 12 Sritipsukho et al reported that action observation training in children with diparetic cerebral palsy revealed significant improvements in all dimensions except the lying and rolling dimension compared to the pretreatment period. Additionally, they showed that the mean change in Gross Motor Function Measurement scores was higher in the action observation training than in the Bobat concept, but did not reach statistical significance. 12 In our study, it was action observation training that provided significant improvements in all motor function subtests in the Live Action Observation Training group, except for the lying down and rolling over subtest. The lack of a significant increase in the relevant subtest can be attributed to the fact that the initial score of the groups for the subtest in question is close to the full score. Overall, our gross motor function results showed that there were no significant differences between action observation training groups, showing that they were superior to conventional physiotherapy, but Video-Based Action Observation Training was relatively more effective. This can be considered as an alternative treatment option for children who have problems accessing traditional physiotherapy. The results confirm that action observation training showed positive effects in improving gross motor function, as well as an increase in participants’ mobility and ability to perform activities of daily living. With its direct multisensory impact, action observation training helps the patient visualize the exact position for each exercise. 24 Our results confirmed this. Although performed in a relatively short period, repeated viewing of videos of sitting, standing, and walking sideways may have increased the learning effects of the exercise by making it easier to understand the specific positions for each action and their sequence. We think that our study, to our knowledge, contributes to the literature as the first study examining all Gross Motor Function Measurement subparameters.
It has been reported that the participation level of individuals with cerebral palsy decreases compared to the normal population and that participation decreases as the functional status worsens. 25 This shows the importance of adding different rehabilitation strategies to the treatment protocol to increase participation in daily life and physical activity in children with cerebral palsy. In our study where we examined the effect of action observation training on activity participation, participation results were positively affected in all 3 groups. However, the effects of Video-Based Action Observation Training and Live Action Observation Training were close to each other and superior to conventional physiotherapy. In our study, this effect of action observation training on activity participation and on brain activity in the primary motor area may be interpreted as resulting from the activation of cognitive activities related to motor memory formation and understanding other children's behavior through imitation. Action observation training may cause the patient to make a greater effort to maintain concentration and produce movement. Therefore, we believe that action observation training will be a method that can be used to create functional movements and provide somatic sensation, as well as to overcome the limitations in active participation in repetitive active training during the treatment process because of problems in motor abilities. Additionally, the inclusion of exercises that are task-oriented and integrated with daily life in our action observation training program may have increased children's activity participation. In a study, it was observed that gait parameters were related to the ability to perform activities without fear of falling, physical activity level, and balance. 26 In this context, the decrease in the fear of falling due to repeated observation and performance of task-oriented balance and walking exercises, which are frequently used in daily life and included in action observation training, may also explain the improvement in activity participation results.
Two studies examining the effects of action observation training on balance function in children with cerebral palsy showed that action observation training was more effective than conventional physiotherapy in improving balance function.12,23 Consistent with the action observation training studies conducted in the literature on children with diparetic cerebral palsy, in our study, more improvement was seen in the action observation training groups than in the control group. It can be thought that action observation training improves balance function by contributing to uniform weight bearing, postural adaptation, and direction-changing ability. In addition, in our study, which was the first time to our knowledge that Video-Based Action Observation Training and Live Action Observation Training were compared on children with diparetic cerebral palsy, their effects were found to be the same.
Only Jung et al 23 examined the effectiveness of action observation training or other rehabilitative methods that activate mirror neurons on timed-up-and-go test in children with cerebral palsy, and mobility scores in the action observation training group increased compared with the pretreatment, and superior results were obtained compared to the control group. This result is compatible with the results of our study regarding the superiority of action observation training over conventional treatment on mobility function. In our study, Live Action Observation Training was found to be more effective than Video-Based Action Observation Training. Considering that the improvements in mentally simulated tasks during action observation training were better, the explanation for the improvement in mobility function in our study may be the goal-oriented exercises in the standing and walking sections. However, in our study, Live Action Observation Training was relatively more effective; It may be related to the fact that live demonstration of relevant training simultaneously stimulates sensory elements, has a strong positive effect in promoting motor learning and movements, and further facilitates plasticity in the central nervous system.
Functional muscle strength improved significantly in all 3 groups. The effects of these improvements were similar in the action observation training groups and greater than that in the control group. In a study consistent with our results, it was shown that action observation training improved functional muscle strength in children with diparetic cerebral palsy more than the control group. 23 It has been reported that the movement from sit to stand is both a training task and an outcome measure regarding the functional mobility level, lower extremity muscle strength, and balance of children with cerebral palsy. 27 Task-specific activity practices have been proven to provide optimal recovery in functional movement in children with cerebral palsy. 28 Sit-to-stand exercise is also one of the effective task-specific elements for children with cerebral palsy. 28 In this context, the presence of task-specific, repetitive sit-and-stand movements in the action observation training content of our study showed that it was a more optimal training program that included the application of functional movements in daily life activities by motor learning principles.
The 1-minute walk test results of our study showed more improvement in the action observation training groups than in the control group, and the improvement was in favor of Live Action Observation Training. Considering that there is a direct relationship between lower extremity weight-bearing movements, standing symmetrical weight-bearing ability, and functional walking ability, 29 the results of our study regarding walking will be better understood. The fact that it provides useful information in determining the efficiency of walking in children with diparetic cerebral palsy and long-term walking tests complicate the evaluation process and cause cooperation problems, 30 especially in the pediatric group, explaining why the 1-minute walk test was used in our study. Gillette Functional Assessment Questionnaire results also showed significant improvements in all 3 groups. Although Live Action Observation Training was more effective in the Gillette Functional Assessment Questionnaire–skills test, Video-Based Action Observation Training was more effective on the Gillette Functional Assessment Questionnaire–walking scale. We think that such a result may have arisen between the subsections because the Gillette Functional Assessment Questionnaire–walking scale classifies walking in 10 items and the change that occurs takes longer to reflect on the function. For this reason, it may be necessary to apply it for a longer period to ensure clarity of results. Only Jung et al examined the effect of action observation training on walking in the cerebral palsy group and used stair climbing, 10-m walk, and 6-minute walk tests to measure walking function. Action observation training showed significant improvements in all outcome measures, but only the results of the stair climbing and 6-minute walk tests were superior in the action observation training group. 13 Based on the observation of walking movements to help participants walk efficiently in real environments may have provided participants with future experience and preparation. In other words, videos recorded from various angles or watched live directly in front of children, which can enable children to observe and learn walking skills accurately and repeatedly, may also explain this superiority.
Our study has some limitations. The lack of follow-up evaluation in our study prevented the determination of the duration of the effectiveness of action observation training. In addition, the inclusion of cases with GMFS I to III in our study to minimize heterogeneous distribution prevented the generalization of the results to children with severe cerebral palsy. Considering this situation, future studies are needed to include larger-scale and long-term follow-up evaluations.
The most powerful aspect of our study is that it comprehensively demonstrates the effect of a partially new treatment program based on the mirror neuron system on gross motor function, activity participation, balance, functional mobility, functional muscle strength, and walking ability in children with diparetic cerebral palsy. Our study is the first study comparing different application methods of action observation training in children with diparetic cerebral palsy.
Conclusion
As a result, our study showed that action observation training is a feasible and useful method in improving various motor functions and increasing activity participation in children with spastic diparetic cerebral palsy. We also think that our study may create differences in the perspective of treatment programs and evaluation methods for physiotherapists working in this field.
Footnotes
Author Contributions
Dilan Demirtas Karaoba: Writing and manuscript preparation; Burcu Talu: Writing and manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The research was approved by Inonu University Malatya Non-invasive Clinical Research Ethics Committee (approval number: 2021/2663) and Clinical Trial registration was made (registration number: NCT05209282). Written permissions were obtained from the Governorship and Provincial Directorate of National Education to collect the data of the study in Special Education and Rehabilitation Centers (governor's approval numbered 48605746-44-E.32792794). Written informed consent was obtained from the participants and their families. This study was conducted between January 2022 and October 2022 and in accordance with the Declaration of Helsinki.