
Abstract
We present an overview of the epidemiology and differential diagnosis of Marcus Gunn jaw-winking syndrome. We scrutinize various hypotheses regarding its etiology and pathogenesis, encompassing abnormal nerve connections, heredity factors, genetic variation, and the release hypothesis, as proposed in prior studies. Furthermore, we discuss the clinical manifestations of Marcus Gunn jaw-winking syndrome and highlight cases with exceptional clinical presentations or concurrent diseases. Moreover, we not only describe the existing surgical and nonsurgical treatments for Marcus Gunn jaw-winking syndrome but also delineate therapies for related conditions such as Meige syndrome, sequelae of facial paralysis, and other oculopalpebral and facial synkinesis. This comprehensive approach serves as a valuable reference for the holistic management of Marcus Gunn jaw-winking syndrome.
Preface
Robert Marcus Gunn, a Scottish ophthalmologist, was the first to identify and describe Marcus Gunn jaw-winking syndrome. In his report, he presented a case of a 15-year-old girl with unilateral ptosis and ipsilateral upper eyelid retraction. 1 Marcus Gunn jaw-winking syndrome is a congenital cranial dysinnervation disorder presenting as congenital ptosis. 2 Synkinetic movements of the upper eyelids with jaw movement and varying degrees of ptosis with masticatory muscles at rest are typical clinical manifestations of Marcus Gunn jaw-winking syndrome.2–4 The incidence is equal in both genders. 5 It is typically unilateral and more frequently occurs on the left side, although bilateral cases also exist. 6
We describe histopathologic changes in the muscle and aponeurosis of the levator palpebrae superioris of Marcus Gunn jaw-winking syndrome patients in a later section. Researchers have reported ocular and systemic associations of Marcus Gunn jaw-winking syndrome. Ocular concomitant symptoms include strabismus, anisometropia, paralysis of the superior rectus, paralysis of the double elevator, and amblyopia. 1 Amblyopia may occur secondary to anisometropia or strabismus. 1 Systemic associations mainly consist of genetic or nongenetic abnormal embryonic development, which we elaborate on in a later section. Individuals affected by Marcus Gunn jaw-winking syndrome experience ptosis from birth, which can potentially hinder visual development, leading to form deprivation amblyopia caused by visual occlusion. Although ocular examination results may appear normal, monocular or binocular vision can be affected, and binocular vision cannot exceed the lower limit of normal visual acuity for the corresponding age, even with corrective glasses. Furthermore, abnormal facial appearances may lead to inconvenience in establishing relationships with others and problems in psychological development in patients with Marcus Gunn jaw-winking syndrome. 7 Patients may experience long-term loneliness, lack of confidence, anxiety, or depression. 7 Therefore, proposing a comprehensive treatment for Marcus Gunn jaw-winking syndrome is both necessary and meaningful, but it also presents challenges.
Methods
This is a narrative review of Marcus Gunn jaw-winking syndrome. The literature search was performed using a PubMed search from 1939 through April 2024 for the terms marcus gunn jaw winking syndrome, marcus gunn syndrome, marcus gunn jaw-winking, jaw-winking ptosis, facial synkinesis, and congenital ptosis.
Etiology and Pathogenesis
Thorough research on the etiology and pathogenesis is helpful in formulating targeted treatment strategies and identifying therapeutic targets.
Abnormal Nerve Connection
The existing perspective is that Marcus Gunn jaw-winking syndrome is attributed to the abnormal connection between the motor branch of the trigeminal nerve (3 in Figure 1) that innervates the lateral pterygoid muscle (1 in Figure 1) and the superior division of the oculomotor nerve (9 in Figure 1) that innervates the levator palpebrae superioris (11 in Figure 1).2,8 The location of aberrant nerve connections may be categorized into central and peripheral. Central anomalous connection (12 in Figure 1) refers to subnuclear connections linking the trigeminal and oculomotor nerves. 9 The anomalous peripheral connection (13 in Figure 1) refers to a part of the trigeminal nerve fibers (13 in Figure 1) passing through the auriculotemporal nerve (10 in Figure 1). 9 Finally, it arrives at the levator palpebrae superioris (11 in Figure 1). 9 Figure 1, A and B, shows the contrast of normal and abnormal nerve connections.
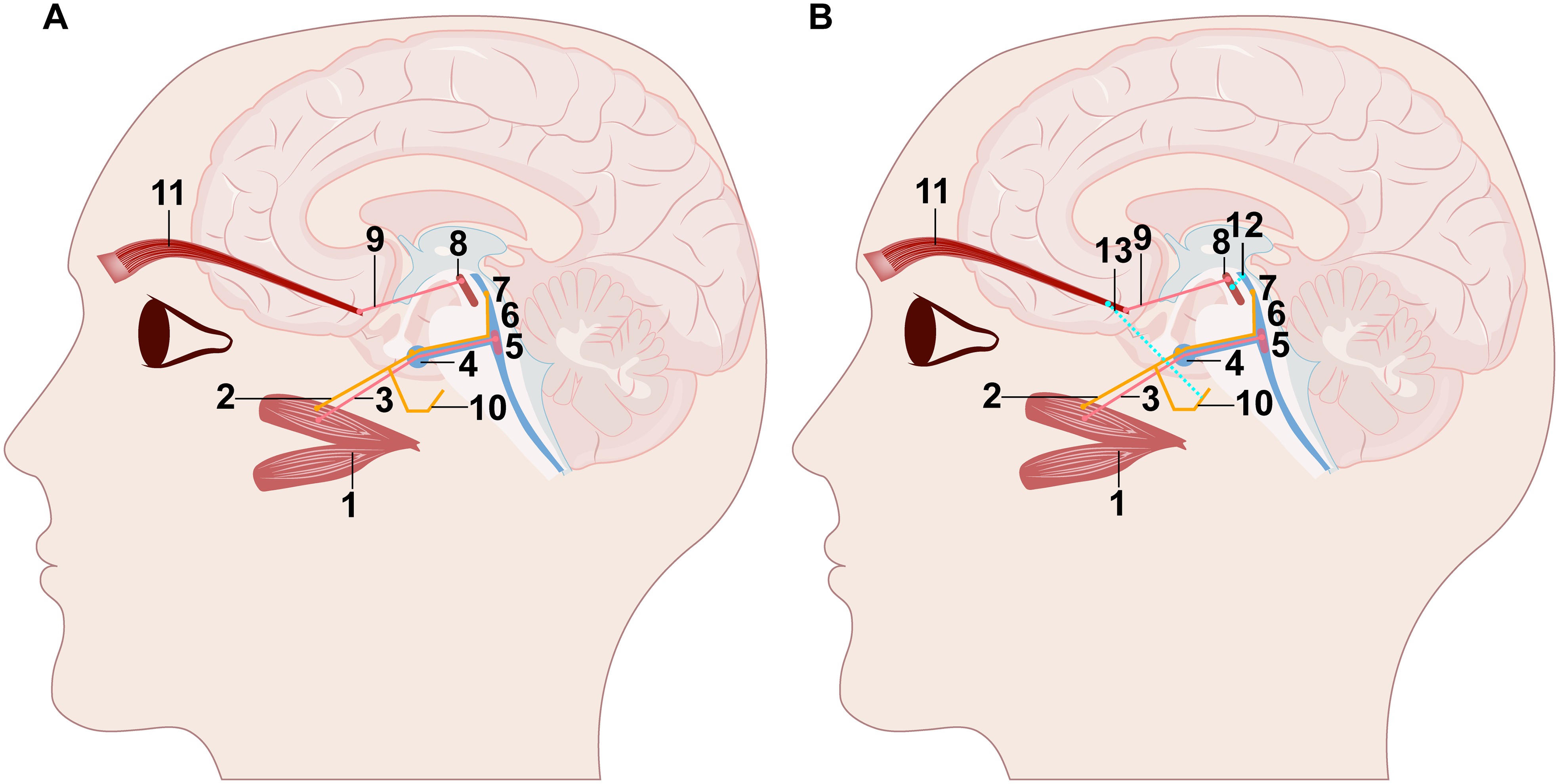
Schematic diagram of jaw-winking synkinesis. (A) Normal nerve innervation of the lateral pterygoid muscle and the LPS. (B) Central and peripheral abnormal nerve connection. We mark these abnormal connection points with dotted line (12 and 13). The central anomalous connection (12) refers to subnuclear connections linking the trigeminal and oculomotor nerves. The peripheral anomalous connection (13) refers to a part of the trigeminal nerve fibers reaching the LPS by passing through the auriculotemporal nerve. (1: lateral pterygoid muscle; 2: sensory branch of mandibular nerve; 3: motor branch of trigeminal nerve; 4: trigeminal ganglion; 5: motor nucleus of trigeminal nerve; 6: pontine nucleus of trigeminal nerve; 7: Vme; 8: oculomotor nucleus; 9: superior branch of oculomotor nerve; 10: auriculotemporal nerve; 11: LPS; 12: central abnormal connection; 13: peripheral abnormal connection). Abbreviations: Vme, mesencephalic nucleus of trigeminal nerve; LPS, levator palpebrae superioris.
In the last few years, certain researchers have partially validated the aforementioned hypothesis by studying selected Marcus Gunn jaw-winking syndrome patients. Conte et al 10 conducted a study using neurophysiological and neuroradiological methods on a pedigree with a multigenerational and autosomal dominant inheritance of Marcus Gunn jaw-winking syndrome. Neurophysiological examinations include electromyography, blink reflex, and the R2 component recovery cycle, Masseter inhibitory reflex, brainstem auditory evoked potentials, and motion analysis. 10 Neuroradiologic examinations comprise magnetic resonance imaging (MRI) and diffusion tensor imaging. 10 Their findings provided evidence of abnormal brainstem structure in individuals with familial Marcus Gunn jaw-winking syndrome. 10 The discovery corroborates the pathogenesis of abnormal differentiation of the axons of the motor branch of the trigeminal nerve to the levator palpebrae superioris. 10
Heredity Theory
Genetic predisposition is one of the etiologies of Marcus Gunn jaw-winking syndrome. Most cases of Marcus Gunn jaw-winking syndrome are sporadic, whereas familial ones are less common and may be irregularly autosomal dominant or autosomal recessive. 11 Investigators have reported more than 12 pedigrees in the past 74 years (see Table 1).
Summary Table for Familial Case Reports in the Past 74 Years.
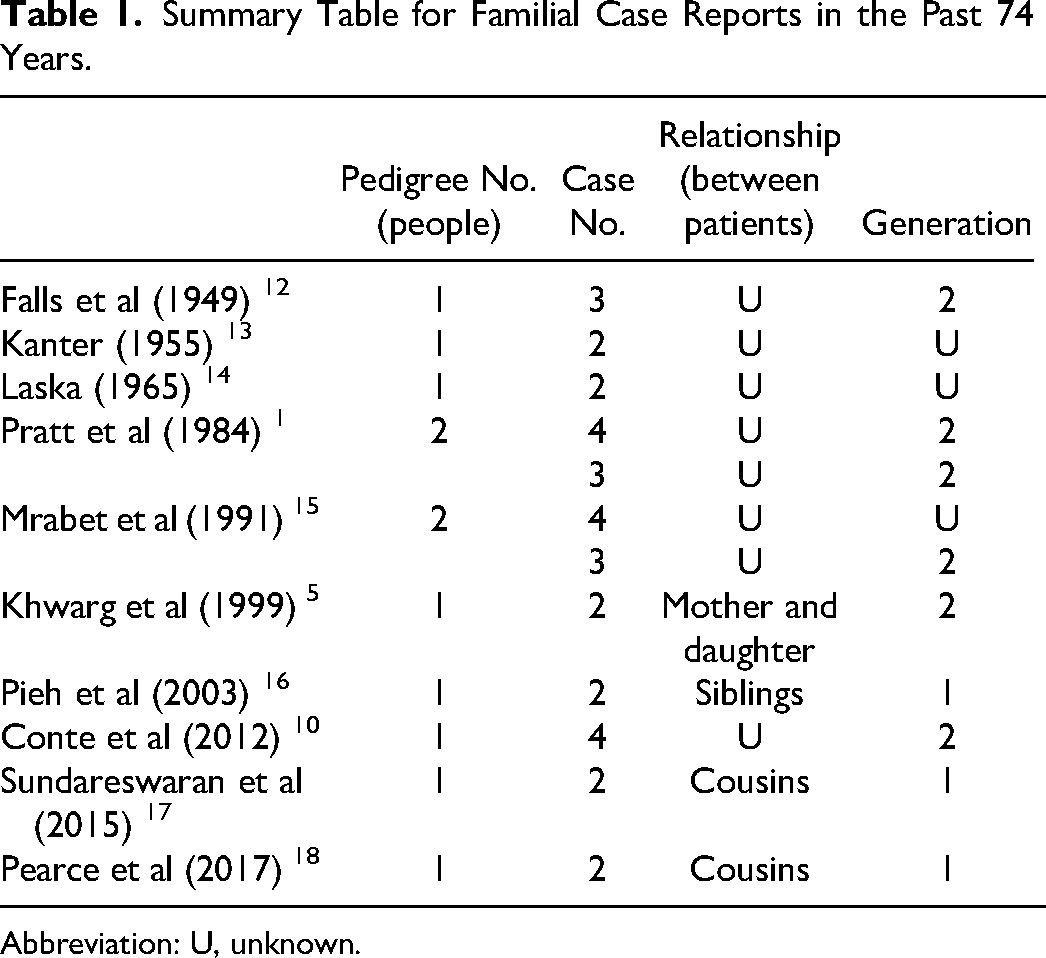
Abbreviation: U, unknown.
Genetic Variation
Marcus Gunn jaw-winking syndrome is a type of trigeminal oculomotor synkinesis. 19 Scholars have detected 7 trigeminal oculomotor synkinesis–related genetic variants, among which 2 genes, KIF21A and TUBB3, have been found in Marcus Gunn jaw-winking syndrome cases.19–22 However, all cases are individuals with congenital fibrosis of extraocular muscle (CFEOM) combined with Marcus Gunn jaw-winking syndrome, and CFEOM does not occur in most Marcus Gunn jaw-winking syndrome cases.19–22 Therefore, whether genetic variation is the primary direct cause of Marcus Gunn jaw-winking syndrome remains to be verified and explored. 19 Several studies have proposed or revealed that specific genetic variants are associated with other diseases by examining Marcus Gunn jaw-winking syndrome patients with other conditions.
Atavism (Release Hypothesis)
According to a “release hypothesis,” Marcus Gunn jaw-winking syndrome is a primitive physiological reflex inhibited during the phylogeny of high-class creatures. 19 However, brain trauma or congenital diseases may release this primitive reflex. 19 Liang and Zhang 19 conducted neural tract tracing and electrophysiological studies in healthy rats. Their research showed that rapid and repeated mandibular stretching could induce Fos protein expression in the pre-oculomotor neurons of the oculomotor and trochlear nuclei. 19 These pre-oculomotor neurons were in the “interstitial nucleus of Cajal and Darkschewitsch nucleus (INC/DN) complex.” 19 They verified that mesencephalic trigeminal nucleus (Vme) neurons, which conduct proprioception and tactile pressure sensation, could project to the oculomotor, trochlear nuclei, and pre-oculomotor neurons of them. 19 Additionally, according to the clinical findings of Lehman et al, 23 stimulating the trigeminal nerve's motor branch could lead to eyelid retraction in the ordinary population. Thus, they hypothesized the mandibular-eyelid responding circuit associated with the Vme neurons, which might receive the afferent impulses of the jaw muscle. 19 As the pre-oculomotor neurons in the interstitial nucleus of Cajal and Darkschewitsch nucleus complex innervate vertical eye movement, such as eyelid collaboration, they further postulated the involvement of interstitial nucleus of Cajal and Darkschewitsch nucleus complex in Marcus Gunn jaw-winking syndrome.19,24,25 In addition, the inhibitory effect of interstitial nucleus of Cajal and Darkschewitsch nucleus complex on the oculomotor and trochlear nuclei may be essential for reduced afferents to them in healthy people.19,24,25 Hereditary factors may be determining factors in the phenotype and inhibitory effect of this primitive reflex to a certain degree. 19 Shi et al 26 conducted another neural tract–tracing study in healthy rats and found contacts of afferent Vme neurons from the eyelid and the masseter muscle (see Figure 2). Their finding further supported the release hypothesis. However, the researchers did not establish any Marcus Gunn jaw-winking syndrome animal model to test the hypothesis, which remains to be verified.
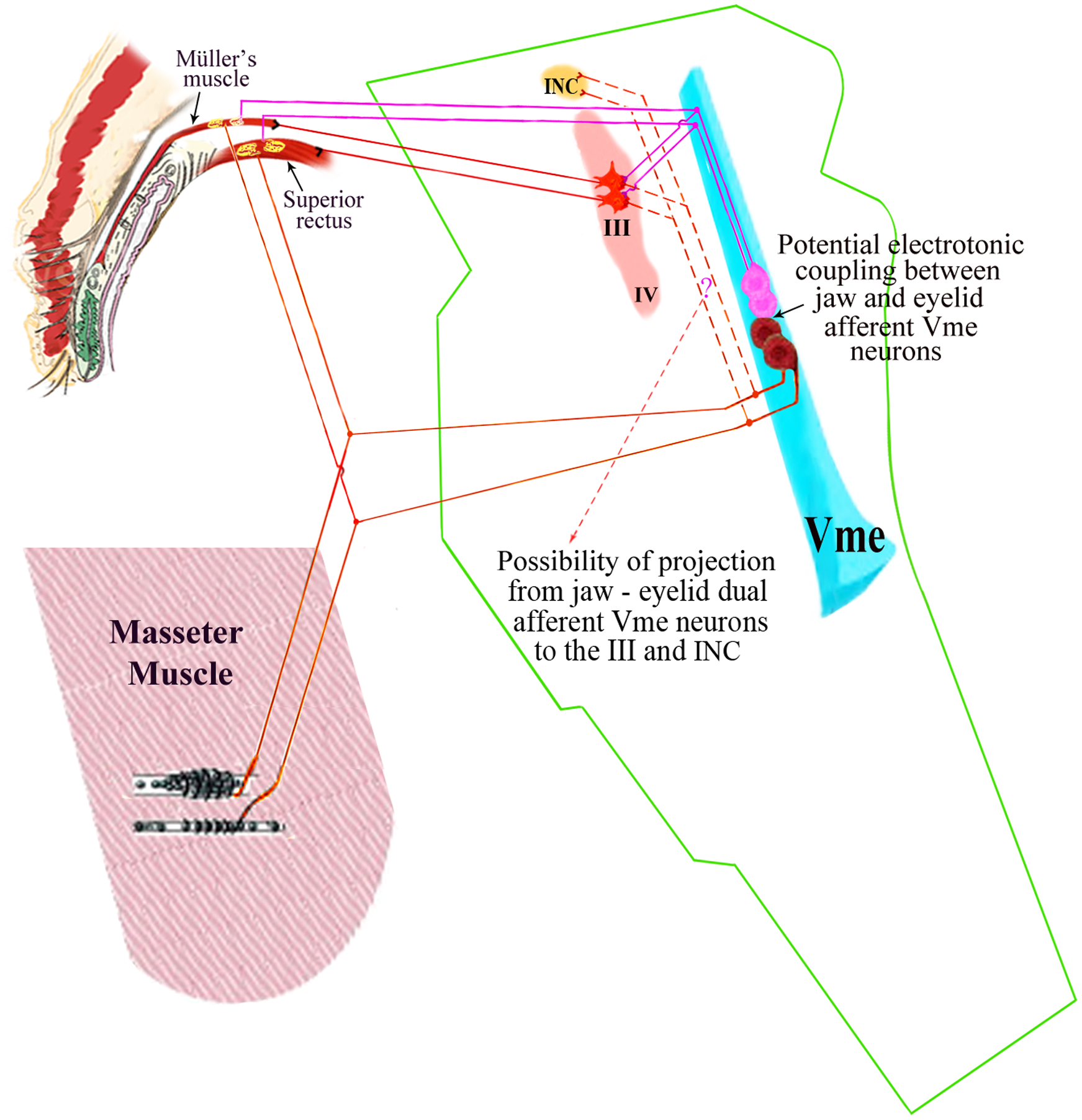
Schematic diagram of the electrotonic coupling of afferent Vme neurons according to the release hypothesis. Some masseter afferent Vme neurons may not project to the III/IV and INC straightforwardly (as if ignoring the dotted lines). There may be an electrotonic coupling of these masseter afferent Vme neurons with adjacent eyelid afferent Vme neurons (elucidation and arrow). When a jaw afferent Vme neuron (below) is highly activated by movement of the ipsilateral pterygoid muscle, the resting membrane potential of an adjacent eyelid afferent Vme neuron (above) may reach threshold through the electrotonic coupling, enabling the somatofugal action potential to discharge. (Reprint from Shi et al, 26 licensed under the terms of the Creative Commons Attribution License https://creativecommons.org/licenses/by/4.0/). Abbreviations: Vme, mesencephalic nucleus of trigeminal nerve; III/IV, the oculomotor and trochlear nuclei; INC, interstitial nucleus of Cajal.
The reflex arc of the jaw-winking reflex may be as follows. For jaw-winking synkinesis, the proprioceptor of the lateral pterygoid muscle is the origin of the impulse, and the involved nerve from the lateral pterygoid muscle innervated by the motor branch of the trigeminal nerve is the afferent nerve. 27 Vme may be the nerve center. The oculomotor nucleus and the superior branch of the oculomotor nerve serve as part of the efferent arc. The abnormal connection, the projection of Vme to the oculomotor nucleus, or an electrotonic coupling of afferent Vme neurons from the eyelid and the masseter muscle may also lead to the existence of the reflex arc.19,26 The transmission of nerve impulses makes the upper eyelid move synchronously during the mandibular masticatory movement. Common trigger conditions for the synkinesis include chewing, sucking, mandibular movement in all directions, contraction of the sternocleidomastoid muscle, Valsalva maneuver, smiling, tongue extension, and breathing, among which the extension of masticatory muscle spindles plays the most crucial role in triggering the synkinesis. 28 Furthermore, infrequent synkinesis exists, including the synkinesis between the medial pterygoid muscle and the levator palpebrae superioris. 29 As a result, patients’ upper eyelids retract when their mouths are closed, or they keep their teeth clenched. 29 Another example is the retraction of the upper eyelid when the patient assumes an upright position from a lying down position or raises the arm on the affected side. 30
Clinical Manifestations
The clinical presentation of Marcus Gunn jaw-winking syndrome may vary depending on individual patients and the course of the condition. Therefore, in the process of diagnosis and treatment, it is essential for doctors to consider patients’ symptoms and clinical manifestations comprehensively.
Histopathologic Changes
In a prospective observational study, researchers examined the levator palpebrae superioris in 77 patients with congenital ptosis, including 12 eyelids with Marcus Gunn jaw-winking syndrome, through light microscopy, enzyme histochemistry, immunohistochemistry, and electron microscopy. 31 They found fibrosis in most Marcus Gunn jaw-winking syndrome eyelids. 31 There were more fibers in the patients with moderate ptosis than those with severe ptosis. 31 The fibers were of unequal sizes, and fibrotic microstructures and degrees of hypertrophy were different (see Figure 3A). 31 An electron microscope detected abnormal muscle fiber in 4 Marcus Gunn jaw-winking syndrome eyelids (see Figure 3B). 31 Lyness et al 32 conducted a histologic observation on the levator palpebrae superioris of 12 Marcus Gunn jaw-winking syndrome patients through immunohistochemical and morphometric methods. They found that the bilateral levator palpebrae superioris fiber density decreased, overall atrophy occurred, and there were hypertrophied or atrophied muscle fiber groups in the levator palpebrae superioris of Marcus Gunn jaw-winking syndrome patients (see Figure 3C). 32 The manifestation was consistent with neurogenic atrophy, and the lesion also occurred on the clinically normal side, indicating that the causative lesion was located in the central nervous system. 32 However, the studies’ small sample size did not draw universal conclusions. Therefore, it is still necessary to further explore whether there are abnormalities in the muscle and aponeurosis of the levator palpebrae superioris of Marcus Gunn jaw-winking syndrome patients.
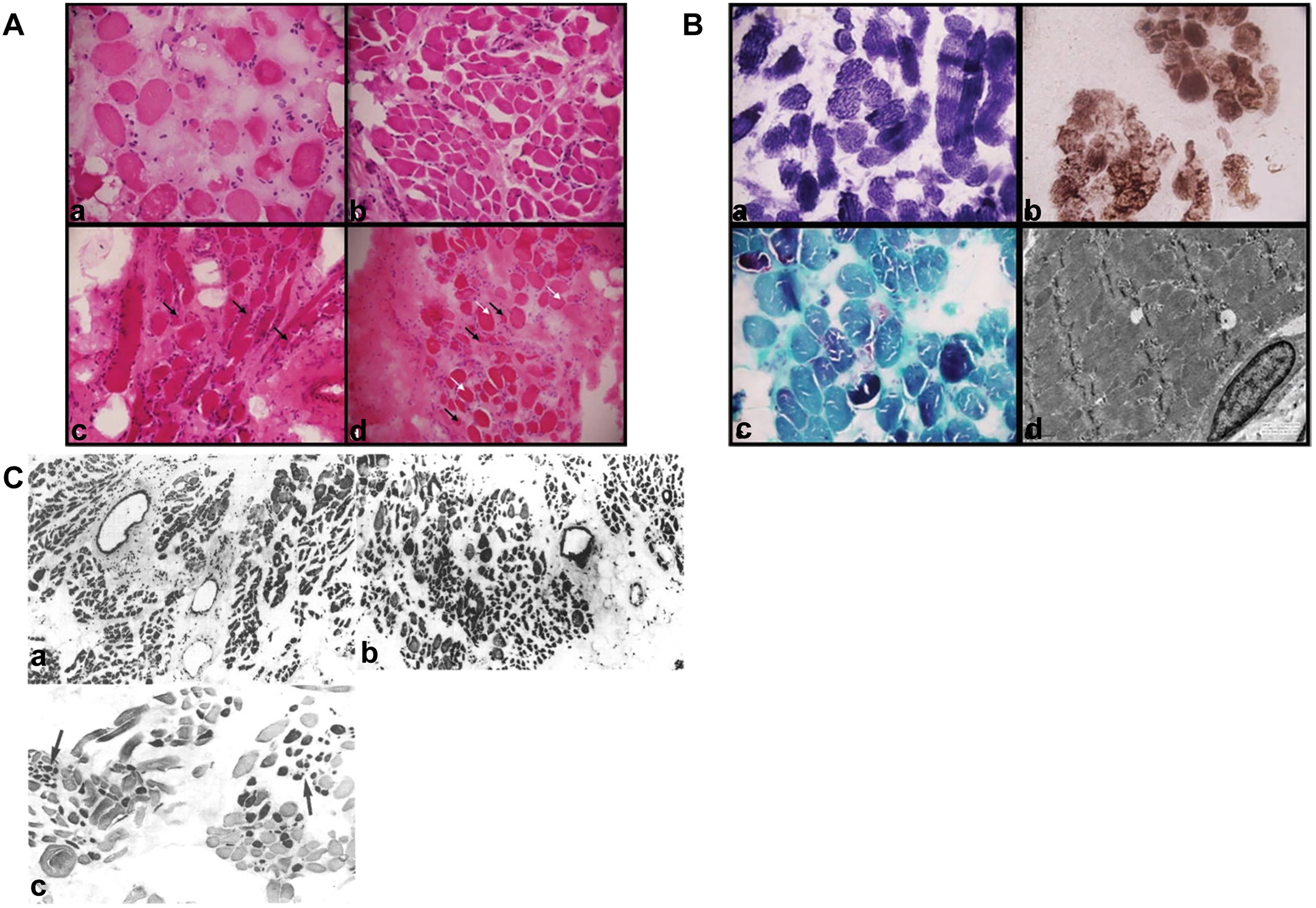
Histopathologic changes of levator of MGJWS and other types of congenital ptosis. (A) Histologic section of levator of congenital ptosis (hematoxylin-eosin [H&E]): (a) levator of BPES showing fibers of unequal sizes (×200); (b) levator of simple ptosis showing mild variation in size of fiber (×100); (c) levator of MGJWS showing nuclei internalization (arrow) (×200); (d) levator of MGJWS showing hypertrophic and atrophic fibers (arrow; ×200) (Reprint from Surve et al, 31 with permission from Springer Nature and the Copyright Clearance Center's RightsLink service; license number 5784100130498). (B) Histologic section of levator of simple ptosis and MGJWS: (a) NADH-TR staining of the levator of simple ptosis showing irregular results (×200); (b) COX staining of the levator of simple ptosis showing irregular results (×200); (c) MGT staining of the levator of simple ptosis showing ragged red fibers (×200); (d) ultrastructural examination of the levator of MGJWS showing myofibrillar disruption (reprint from, 31 with permission from Springer Nature and the Copyright Clearance Center's RightsLink service; license number 5784100130498). (C) Histologic section of levator of MGJWS: (a) H&E staining of levator of the affected side showing decreased muscle fiber density and remaining muscle fiber of unequal sizes; (b) H&E staining of levator of the clinically normal side showing decreased muscle fiber density and remaining muscle fiber of unequal sizes; (c) ATPase staining preincubated at pH 4.3 of levator of the affected side showing hypertrophied or atrophied muscle fiber groups (arrow). (Reprint from Lyness et al, 32 licensed under the Copyright Clearance Center's RightsLink service. License number 5782920097954.) Abbreviations: BPES, blepharophimosis, ptosis, and epicanthus inversus syndrome; MGJWS, Marcus Gunn jaw-winking syndrome.
Jaw-Winking Reflex
During movement of the ipsilateral pterygoid muscle, the upper eyelid retracts and then quickly goes back to a lower position. 28 The blink is more prominent when the patient looks down. 28 In a few cases, the patients do not present with ptosis.
Reported Cases With Special Associations
Associations of Marcus Gunn jaw-winking syndrome include ocular associations and coexisting systemic diseases, which may be hereditary or sporadic. We summarize the essential information and clinical characteristics of 142 Marcus Gunn jaw-winking syndrome patients with particular associations or other illnesses reported in the past 43 years (see Table 2). According to 44 cases in which the age was recorded, the average patient age was 10.0 ± 2.1 years (range, 3 weeks-76 years). According to 37 cases in which the gender was recorded, there were 23 (62%) males and 14 (38%) females. Among 39 patients with a known side of the affected eye, the right side, the left side, and both sides were involved in 19 (49%), 16 (41%), and 4 (10%) patients, respectively. Several visual symptoms commonly observed in patients include strabismus (77 patients), paralysis of extraocular muscles (15 patients), and conditions such as Duane retraction syndrome (9 patients) and CFEOM (8 patients). There were 38 patients with amblyopia or severe visual impairment. In addition, some ocular associations are infrequent, such as nystagmus (1 patient), morning glory disc anomaly (1 patient), Marin-Amat syndrome (1 patient), eyelid myokymia (5 patients), abnormal tears (1 patient), etc. Other systemic diseases associated with Marcus Gunn jaw-winking syndrome are relatively complex to see, mainly including abnormal embryonic development, which are genetic, nongenetic, or whose etiologies are unclear. Several genetic diseases that affect multiple organ systems throughout the body are unfamiliar. These diseases include 22q11.2 microduplication (1 patient), CHARGE (1 patient), Waardenburg (1 patient), congenital central hypoventilation (2 patients), Townes-Brocks (1 patient), and Williams-Beuren syndrome (1 patient). Möbius sequence was found in 2 patients. Other systemic associations include developmental nervous system disorders (4 patients), facial deformities (1 patient), and congenital heart disease (3 patients). Some patients have both ocular associations and systemic diseases. Other findings such as genetic variation mainly include KIF21A genetic variant (6 patients), 22q11.2 microduplication (1 patient), ZC4H2 genetic variant (1 patient), CHD7 genetic variant (1 patient), heterozygous for a PHOX2B gene polyalanine expansion variant (1 patient), heterozygous SALL1 nonsense variant c.826C.T (1 patient), 7q11.23 gene deletion (1 patient), and pure de novo direct duplication dup (12) (q24.1→q24.2) (1 patient). Treatments mainly include frontalis suspension (55 patients), strabismus surgery and other extraocular muscle surgeries (27 patients), levator resection, and botulinum toxin injection (1 patient).
MGJWS Cases With Particular Associations or Other Illnesses in the Past 43 Years.
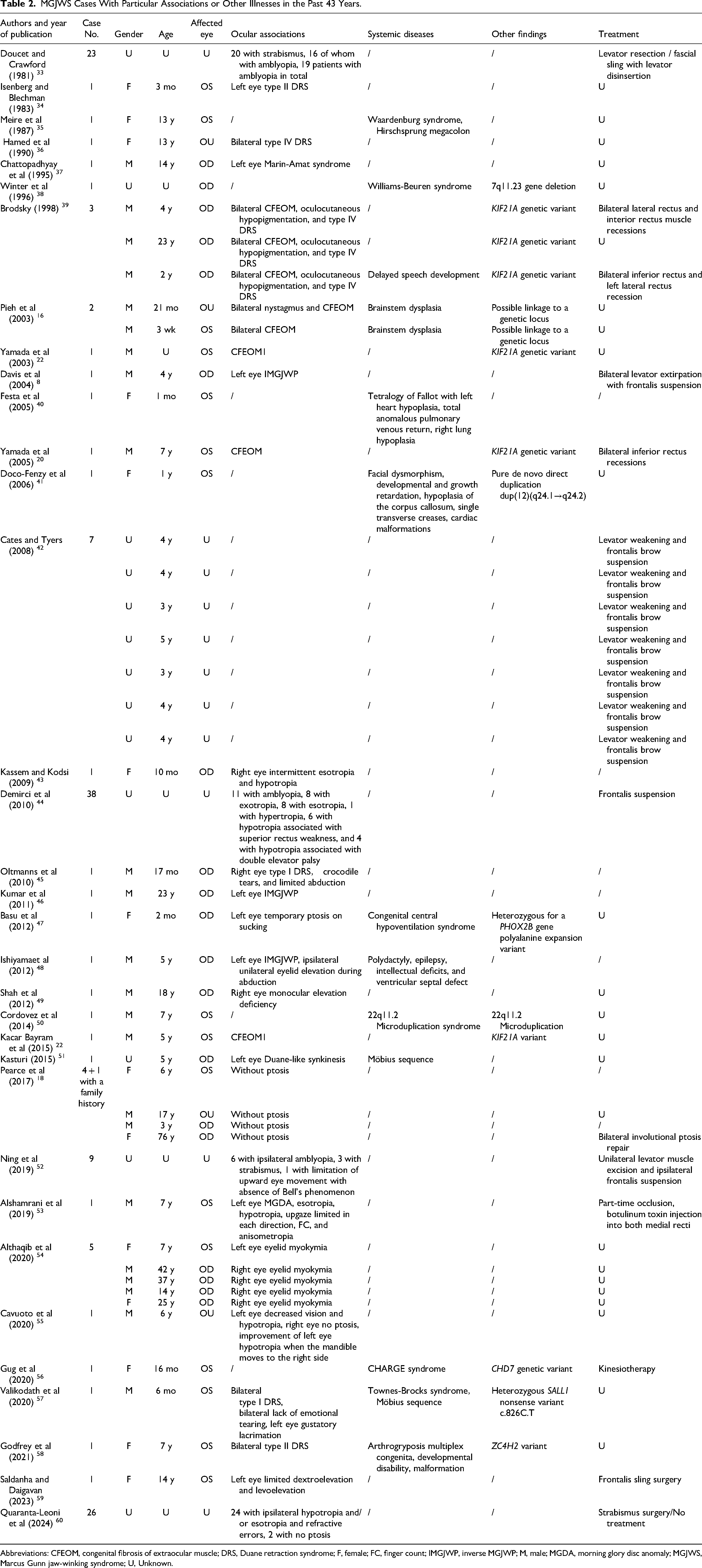
Abbreviations: CFEOM, congenital fibrosis of extraocular muscle; DRS, Duane retraction syndrome; F, female; FC, finger count; IMGJWP, inverse MGJWP; M, male; MGDA, morning glory disc anomaly; MGJWS, Marcus Gunn jaw-winking syndrome; U, Unknown.
Differential Diagnosis
Other Oculo-palpebral and Facial Synkinesis
Marin-Amat syndrome
This acquired facial synkinesis results from peripheral facial palsy, where an aberrant neural pathway forms between the trigeminal nerve and the frontal zygomatic branch of the facial nerve, which innervates the orbicularis oculi muscle.61,62 Its primary clinical manifestation is involuntary eye closure instead of upper eyelid elevation caused by blepharospasm when the patient smiles or opens the mouth.61–63
Meige syndrome
This disease is primary or secondary focal dystonia, the mean onset age of which is 60 to 70 years old.64–66 The major cause of primary Meige syndrome may be genetic variation. 67 In contrast, secondary Meige syndrome occurs due to tardive dystonia, potential neurologic diseases, or long-term use of antineuropathic drugs or other medications.67,68 Initially, the disease presents with blepharospasm or oral-mandibular dystonia.64,69,70 Subsequently, other muscles may become involved, including those in the neck, respiratory system, or upper limbs, resulting in dystonic tremors. 71 Marcus Gunn jaw-winking syndrome is a congenital disease that usually presents with symptoms in childhood, and there is no abnormal movement, such as involuntary oral-mandibular dystonia or systemic dystonic tremors.
Inverse Marcus Gunn Jaw-Winking phenomenon
This disease may be attributed to an unusual connection between the oculomotor and trigeminal nerves. 61 The abnormal connection mode is opposite to that of Marcus Gunn jaw-winking syndrome, and the fundamental clinical manifestation is ptosis instead of upper eyelid elevation induced by mouth opening or aggravated when opening the mouth.61,72
Other Nonsimple Ptosis
Progressive external ophthalmoplegia
Progressive external ophthalmoplegia is a mitochondrial myopathy characterized by progressive bilateral ptosis and diffuse decreased ocular movement, usually accompanied by other symptoms of mitochondrial dysfunction, and also seen in individuals with systemic mitochondrial cell disease. 73 When a patient shows only ocular signs, it is called “chronic progressive external ophthalmoplegia.” 73 Orbital CT imaging, MRI, postexercise blood lactic acid level tests, electromyography, genetic testing, and muscle biopsy can help diagnose progressive external ophthalmoplegia. 73 Progressive external ophthalmoplegia patients do not exhibit upper eyelid elevation during chewing.
CFEOM
CFEOM is a genetic congenital cranial dysinnervation disorder associated with abnormal oculomotor nerve and nucleus development, with 3 main phenotypes: CFEOM 1, CFEOM 2, and CFEOM 3.74,75 CFEOM 1, caused mainly by KIF21A genetic variants, presents as relatively symmetrical bilateral ptosis and severely limited eye movement, with fixed eyes, exotropia, and depression.74,76 CFEOM 2 is passed on through a recessive gene. 74 Its characteristics are bilateral miosis, asthenocoria, ptosis, and the eyeballs’ limited movement. 74 The primary cause of CFEOM 3 is TUBB3 genetic variant.21,74 Its clinical manifestations are heterogeneous, possibly including unilateral or asymmetrical ptosis and limited eye movement, often associated with other neurodevelopmental abnormalities, mental retardation, or social disability.21,74 CFEOM patients without Marcus Gunn jaw-winking syndrome do not exhibit upper eyelid elevation during chewing. Muscle biopsy shows fibrous tissue and collagen replace most affected muscle tissue. 74 A traction test can also help with diagnosis.
Pediatric myasthenia gravis
Myasthenia gravis is an autoimmune disease that occurs in adults but can also exist in neonates and adolescents. In individuals with myasthenia gravis, neuromuscular junction transmission disorder results in skeletal muscle myasthenia. Ptosis is usually the first symptom of myasthenia gravis. Other clinical manifestations may include dysphagia, dysmasesia, and dysarthria; severe patients may have dyspnea. The fatigue of the affected muscle group worsens as the day goes on.
There are 3 types of myasthenia gravis affecting children: transient neonatal myasthenia gravis, juvenile myasthenia gravis, and congenital myasthenia gravis syndrome. 77 The etiology of transient neonatal myasthenia gravis is the entry of autoantibodies from the mother with autoimmune myasthenia gravis into the fetus through the placenta. 77 The patient may present with extraocular muscle weakness, systemic hypotonia, respiratory distress, weak crying, and poor sucking.77,78 Autoantibody testing is usually positive. 77 This disease is transient and self-limiting. 77 Juvenile myasthenia gravis is an autoimmune disease characterized by the promotion of postsynaptic membrane lysis, direct inhibition of activity, and receptor degradation by autoantibodies, leading to a decrease in acetylcholine receptor activity, which can affect any skeletal muscle.77,79–81 Among them, patients with ocular myasthenia gravis subtype may exhibit eyelid retraction in the morning in the early stage, followed by upper eyelid ptosis becoming more severe at night. 77 Autoantibody testing is helpful for diagnosis, and some researchers have proposed using B cell activation factors as markers of juvenile myasthenia gravis disease activity.77,82,83 Congenital myasthenia gravis syndrome is mainly caused by abnormal acetylcholine receptor structure, possibly related to genetic variation. 77 The affected child may exhibit ptosis in the eyes alone, or other skeletal muscles throughout the body may be affected, leading to fatigue. 77 Congenital myasthenia gravis syndrome patients have negative autoantibody tests, and genetic testing is also helpful for typing and differential diagnosis. 77 Children with myasthenia gravis have the characteristic of upper eyelid ptosis, which is mild in the morning and heavy in the evening and does not show upper eyelid elevation during chewing. Autoantibody tests may be positive. Children with Marcus Gunn jaw-winking syndrome show upper eyelid elevation during chewing, and the degree of ptosis usually does not vary with the masticatory at rest. Autoantibody tests are negative.
Duane retraction syndrome
Duane retraction syndrome is caused by abnormal nerve innervation of the external rectus muscle on the affected side of the eye by the axon that should have innervated the internal rectus muscle. 84 Duane retraction syndrome is divided into 4 types with different clinical manifestations: type I (abduction dysfunction, normal or mild adduction dysfunction), type II (normal abduction function or mild abduction dysfunction, adduction dysfunction), type III (both abduction and adduction dysfunction), and type IV (synergistic divergence, exotropia, abduction when attempting adduction in affected eyes, abduction when staring at the healthy side with the affected eye, narrow eyelid fission).85–87 Duane retraction syndrome is primarily diagnosed based on clinical manifestations and electromyographic examination. 85 The enlargement or reduction of eyelid fissures in Duane retraction syndrome patients is associated with the outward and inward rotation of the affected eye and is unrelated to mandibular movement. In contrast, the elevation of upper eyelid of Marcus Gunn jaw-winking syndrome patients is related to mandibular movement.
Congenital Horner Syndrome
Congenital Horner syndrome may be caused by damage to any part of the sympathetic nervous system or present as one of the clinical manifestations of primary thoracic neuroblastoma. 87 This condition is characterized by reduced pupil size, drooping upper eyelid, asymmetrical facial flushing, and common accompanying symptoms such as iris heterochromia.87–89 Patients with congenital Horner syndrome do not exhibit upper eyelid elevation during chewing, whereas Marcus Gunn jaw-winking syndrome patients have normal pupil size, no asymmetrical facial flushing, and no sweating on the affected side of the face. Diagnostic criteria and methods include medical history, clinical manifestations, physical examination, pharmacologic testing, etc. 87 Imaging examinations such as CT and MRI can help diagnose and locate the primary disease. 87
Congenital third cranial nerve palsy
Congenital oculomotor nerve paralysis can be caused by adverse intrauterine events, postnatal trauma, congenital absence of the oculomotor nucleus, or septo-optic dysplasia.90,91 Clinical manifestations include ptosis, strabismus, and unequal pupil size in both eyes.90,91 Patients do not exhibit upper eyelid elevation during chewing. Medical history, clinical manifestations, ophthalmic examination, high-resolution MRI, and other imaging examinations can help in clarifying the diagnosis. 92
Infant botulism
Infant botulism is caused by ingestion of food or dust contaminated with botulinum toxin spores. 93 The onset of the disease is typically preceded by constipation, and other clinical manifestations include drowsiness, poor feeding, weak crying, decreased muscle tone, and ptosis.93,94 Subsequently, it may develop into descending bilateral symmetrical paralysis.93,94 Ultimately, it can lead to paralysis of respiratory and diaphragmatic muscles, resulting in respiratory failure.93,94 Diagnostic methods include clinical manifestations, fecal or serum botulinum toxin testing, etc.93,94 Patients with infant botulism do not exhibit upper eyelid elevation during chewing, and their botulinum toxin test results are positive.
Assessment and Surgical Treatment
The visual acuity of the affected eye and its difference from that of the opposite eye need to be evaluated before a patient's vision correction treatment and help determine the need for surgical treatment. Prior to any surgical procedure, it is standard practice to conduct various examinations, including a blood routine test, coagulation function test, electrocardiogram, and chest radiography. Considering the development of binocular and palpebral structure, as well as visual function, and assessing the tolerance and safety of general anesthesia, surgery, and postoperative medication in children, surgical treatment is typically performed after age 3 years. 7 The primary indications for surgery include visual dysfunction of the affected eye with evident differences in bilateral visual function and ptosis with or without levator dysfunction. The optimal treatment goals encompass correcting ptosis and weakening or possibly eliminating synkinesis.
There is yet to be a unified surgical plan for the treatment of Marcus Gunn jaw-winking syndrome in clinical practice. The surgical procedure varies according to the severity of the ptosis. 28 Standard external levator resection and advancement and Fasanella-Servat surgery are feasible options to correct mild ptosis. 28 Levator resection and advancement involves exposing the upper eyelid crease incision and extending it downwards to the levator aponeurosis. 2 Then, the levator aponeurosis is folded or removed and reconnected to the front surface of the tarsus using nonabsorbable sutures. 2 This type of surgery offers advantages such as short duration, fast recovery, and reduced requirement for additional surgery. 2 Fasanella and Servat 95 first introduced a surgical method for correcting mild ptosis, which includes removing 3-mm-long superior tarsus, Müller muscle, conjunctiva, and levator palpebrae superioris. 2 This technique is suitable only for cases where the levator palpebrae superioris function is good and the ptosis is less than 3 mm. 2 Additionally, this surgical procedure removes the meibomian plate, affecting the eyelids’ stability and reconstruction function. 2 Correcting moderate to severe ptosis often requires levator disabling/excision and bilateral/ipsilateral frontalis suspension/flap.44,60 Levator disabling and bilateral/ipsilateral frontalis suspension is performed as follows. Through an eyelid crease incision, the surgeon identifies and separates the levator aponeurosis beneath the preaponeurosis orbital fat, extending it upward to the Whitnall ligament. The aponeurosis is then transected, and the proximal end of the levator is attached to the arcus marginalis. 44 Then, the frontalis suspension is performed using the autologous fascia lata sling, with the eyelid crease incision used to pass through the fascia lata in the pretarsal plane. 44 For patients undergoing bilateral surgery, a fascia lata frontalis sling is separately placed on the normal side with similar tension. 44 In levator excision surgery, at least 10 mm of the levator muscle is excised. 60 A frontalis flap procedure requires no autologous fascia lata sling but involves an L-shaped incision. 60 The strength of the frontalis muscle is directly used to elevate the eyelid.
Currently, there is no practical solution for Marcus Gunn jaw-winking syndrome synkinesis. Existing levator resection and advancement surgery primarily removes or folds a segment of the aponeurosis connected to the tarsal plate. The levator and the zone of the fornix (a part of the aponeurosis below the Whitnall ligament) remain intact. Theoretically, synkinesis persists and becomes permanent after simple frontalis muscle surgery. Doucet and Crawford 33 reported that all patients who underwent unilateral maximum levator resection failed to eliminate jaw-winking synkinesis, and eyelid lagophthalmos occurred in 82% of the patients. Quaranta-Leoni et al 60 conducted a retrospective study and concluded that levator resection and advancement aggravated synkinesis, and that levator resection was ineffective in cases of severe ptosis. Fasanella-Servat surgery is unsuitable for most patients and unable to eliminate synkinetic movements. 33
The combination of levator disabling and bilateral/ipsilateral frontalis suspension surgery, as reported by Dermirci et al, 44 can eliminate 97% of patients’ synkinesis. Similarly, levator excision with bilateral frontalis sling or unilateral frontalis flap, as reported by Quaranta-Leoni et al, 60 can eliminate synkinesis with a reoccurrence rate of 17.6%. However, this surgery is more time-consuming and difficult. 44 Additionally, bilateral frontalis suspension surgery damages the healthy eyelid, causing the levator to detach and leaving the severed end open, potentially leading to recurrence if it heals in situ. There is also a potential risk of ocular surface complications caused by eyelid elevation dysfunction. Levator aponeurosis resection and ipsilateral frontalis suspension, as reported by Ning et al, 52 was observed during the 6-month follow-up period after surgery. However, the levator still exists; theoretically, the synkinesis cannot be completely suppressed. Moreover, the short follow-up period is insufficient to prove this surgical method's effectiveness in eliminating synkinesis. 52 In summary, the existing surgical methods may not effectively suppress synkinesis or may cause inconvenience to both the patient and the surgeon, and are not ideal treatment methods for Marcus Gunn jaw-winking syndrome.
Therefore, we aim to summarize existing surgical methods, detailing their names, introduction years, indications, advantages, and disadvantages. Our goal is to identify areas for improvement and propose more optimal surgical techniques in the future, addressing current limitations and ultimately benefiting patients (see Table 3).
Existing Surgical Methods for MGJWS.
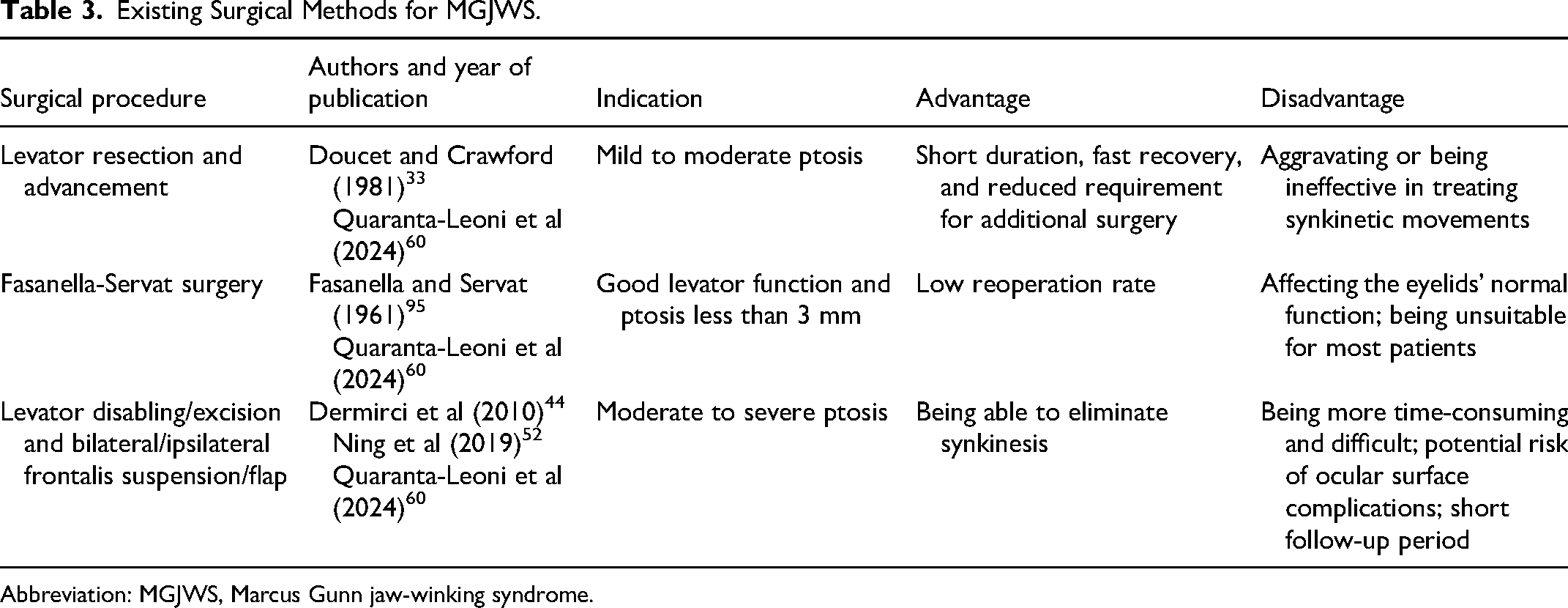
Abbreviation: MGJWS, Marcus Gunn jaw-winking syndrome.
Prospects
To weaken or even eliminate synkinesis while correcting ptosis, it is necessary to develop Marcus Gunn jaw-winking syndrome treatment methods with minimal damage, simplicity, and fewer complications in the future. Using treatments for other diseases with similar clinical manifestations as a reference may be a feasible approach. In clinical practice, the ocular-palpebral and facial synkinesis of Marcus Gunn jaw-winking syndrome refers to the involuntary elevation of the affected upper eyelid during autonomous movements such as chewing. Synkinesis, by definition, involves muscles participating in movements they normally would not during autonomous activities. There are similar ocular-palpebral and facial synkinesis in clinical practice, such as Meige syndrome and sequelae of facial paralysis. Meige syndrome is characterized by involuntary movement in multiple face regions, similar to the clinical manifestations of facial synkinesis. Facial synkinesis, one of the most common sequelae of facial paralysis, refers to the involuntary movement of other areas of the face when a specific area moves autonomously. The clinical manifestations of Marcus Gunn jaw-winking syndrome align with the definition of facial-associated movement clinical manifestations. Additionally, skull base tumors may compress the cranial nerves, leading to abnormal nerve innervation and function, resulting in similar symptoms. From a pathogenesis perspective, abnormal muscle movement is associated with congenital or acquired dysfunction of the nervous system. In summary, these diseases share similarities in clinical manifestations and pathogenesis. Whether considering symptomatic or etiologic treatment, there may be similarities and correlations in the treatments. Using treatments for these diseases as a reference can be a reasonable approach for selecting therapies to address synkinesis in Marcus Gunn jaw-winking syndrome and similar conditions.
Meige Syndrome
Traditional treatments for blepharospasm or oral-mandibular dystonia include drugs and botulinum toxin A injection. 67 Drugs targeting pathogenesis include anticholinergic drugs, dopamine antagonists, γ-aminobutyric acid (GABA) receptor agonists, psychoactive drugs, and antiepileptics. 66 Medications and botulinum toxin are more effective in treating blepharospasm than oral-mandibular dystonia, regardless of whether blepharospasm exists alone or is associated with oral-mandibular dystonia. 67 The effectiveness of simultaneously eliminating symptoms in different regions requires further exploration.
Sequelae of Facial Paralysis
Facial synkinesis secondary to facial paralysis can be treated through nonsurgical methods. Surgical treatment can relieve symptoms and is suitable for patients with severe and persistent synkinesis. 96 Surgical procedures include selective myectomy, selective neurectomy, selective neurolysis, direct brow lift combined with eyelid skin grafts, orthodromic temporalis muscle flap combined with cross-face nerve grafts, and nerve or free muscle transfer.96–98 The current surgical method for eliminating the synkinesis of Marin-Amat syndrome, secondary to facial paralysis, is the excision of the orbicularis oculi muscle of the upper or lower orbital septum. 99 Nonsurgical methods include neuromuscular retraining and chemo-denervation with botulinum toxin. 96 In addition, the “Mirror Effect Plus Protocol (MEPP)” reported by Martineau et al, 100 which combined motor imagery, manipulations, and facial mirror therapy, could be used to improve facial symmetry and reduce synkinesis in patients with acute Bell's palsy.
In recent years, with the development of information technology and artificial intelligence, some researchers have tried to apply deep learning and facial recognition technology to the physical training of facial muscles of patients with facial synkinesis and other facial muscle dysfunctions secondary to facial paralysis, to help patients form new muscle memory. Wang et al 101 invented a facial paralysis rehabilitation training method assessing the facial symmetry of the patient through facial images and a facial coordinate system. It provides training tasks of facial paralysis rehabilitation to the patient. 101 Then, it uses animation images to guide the expression training and gives the patient feedback on the quality of training. 101 Through comprehensive study and drawing from existing knowledge, targeted muscle training methods may be proposed in the future for patients with Marcus Gunn jaw-winking syndrome.
Oculo-palpebral and Facial Synkinesis Associated With Ptosis
Ben Rayana et al 102 reported a surgical method of levator palpebrae superioris resection through the orbital floor to ensure the disappearance of the synkinesis. Although this procedure might result in complete ptosis, it can be treated by frontalis muscle suspension. 102 However, it can still cause binocular asymmetry during blinking, and when performed only on the affected side, it can cause upper eyelid hysteresis. 102
Facial Muscle and Autonomic Nerve Synkinesis in Response to Carbamazepine
Lavrador et al 103 encountered a 41-year-old woman with left facial palsy, myokymia, and Bell's palsy in childhood who developed abnormal left eye lacrimation while eating. The symptom disappeared after carbamazepine treatment. 103 We cannot exclude the possibility that carbamazepine is effective for other facial synkinesis.
Malignant Skull Base Tumors
In patients with post–facial paralysis synkinesis secondary to these disorders, modified selective neurectomy isolating and transecting the specific nerves resulting in aberrant movements is available for facial nerve management.104,105
Conclusions
The existing studies on the pathogenesis of Marcus Gunn jaw-winking syndrome are limited. In some exceptional cases, patients often exhibit other ocular or systemic diseases or abnormal manifestations since childhood, which may significantly impact their physical health and social adaptation. When available and compared with other studies, genetic testing, neurophysiology, and imaging examination may provide more insight into the etiology of Marcus Gunn jaw-winking syndrome itself and its association with other diseases. Through future research, a more thorough understanding of the pathogenesis of Marcus Gunn jaw-winking syndrome in terms of anatomy, genetics, and physiology will be achieved. For instance, further evidence of abnormal nerve connections in patients, genes directly related to the pathogenesis of Marcus Gunn jaw-winking syndrome, or additional support for the release hypothesis can be discovered. In terms of treatment, in the past, surgery, botulinum toxin injection, and other methods were mainly used to alleviate ptosis. However, surgical treatment may not permanently eliminate synkinesis. Drawing from treatments for other oculo-palpebral and facial synkinesis, the most cost-effective and beneficial interventions can be developed for long-term patient care. Nonetheless, there is scope for exploring and developing more practical and diversified treatment methods.
Footnotes
Author Contributions
SZ and QQ contributed to data acquisition, analysis, and interpretation and drafted the manuscript. All authors contributed to study conception and design, critically revised the manuscript, approved the final version and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
No ethical approval was needed for the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was supported by the National Nature Science Foundation of China (Grant no. 81870688), the Funding of Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine (Grant no. JYLJ202008), Shanghai Key Clinical Specialty, Shanghai Eye Disease Research Center (Grant no. 2022ZZ01003), and China Scholarship Council (award no. 202306230291).