
Abstract
Objective
This study aimed to investigate calcitonin gene-related peptide (CGRP) levels in children and adolescents with primary headache.
Methods
All patients underwent blood sampling regardless of their headache state (ictal or interictal) on the day of examination. The patients were grouped based on their headache diagnosis (migraine, tension-type headache, or mixed).
Results
Ninety-two patients aged 5-18 years were included (29 diagnosed with migraine and 31 with tension-type headache). In the comparisons between the patients with migraine and the patients with tension-type headache, interictal CGRP levels in blood from the cubital vein showed no significant difference. Ictal samples were collected in the tension-type headache group only, and no significant difference was observed between the ictal and interictal phases. Variables such as headache diagnosis, sex, age, family history with primary headache, headache frequency, time since last headache, medication usage, and body mass index did not significantly influence CGRP levels.
Conclusion
No significant difference in interictal CGRP levels between patients with migraine and patients with tension-type headache were found. In patients with tension-type headache, there were no significant differences between CGRP levels in the ictal and interictal state. We were not able to draw conclusions about differences in ictal levels of CGRP in patients with migraine compared with patients with tension-type headache, or in differences between ictal and interictal levels in patients with migraine. Future studies should aim to replicate these results in a larger study cohort.
Headache disorders have been ranked as the second leading cause of disability as measured by disability-adjusted life years for individuals aged 10-24 years globally. 1 This highlights the substantial burden that headache disorders impose on the health of young people worldwide. Migraine, known for its debilitating nature, is linked to missed school days, curtailed social activities, and an overall diminished sense of well-being.2,3
The involvement of the trigeminovascular system in the onset of migraine headaches is well established. Activation of the trigeminal system by various triggers leads to the release of neuropeptides from nociceptive fibers that innervate cerebral and meningeal arteries. 4 One of the neuropeptides released is calcitonin gene–related peptide (CGRP), which is composed of 37 amino acids known to play a pivotal role in vasodilatation, neurogenic inflammation, and pain transmission. CGRP is expressed by almost 50% of trigeminal neurons. 5 Previous studies conducted on adults have yielded the following significant insights: (1) elevated plasma levels of CGRP have been associated with both migraine attacks 6 and the interictal period;5,7 (2) it has been observed that intravenous CGRP induces migraine-like headaches in migraine patients;8,9 and (3) CGRP antagonists have demonstrated efficacy in the acute management of migraine attacks. 10 Studies concerning CGRP levels in pediatric patients with migraine are much more limited, and results are thus forth contradictory.11–15
Studies investigating CGRP levels in children and adolescents with migraine are sparce. Two studies have found increased levels of CGRP in patients with migraine during a migraine attack,12,14 and two have found increased levels of CGRP both ictally and interictally.13,15 On the contrary, 1 study found neither any significant differences in CGRP level between patients with migraine and healthy control subjects nor between ictal and interictal measurements of CGRP in migraine patients (Table 1). 11
Comparison of the Studies Reporting on CGRP and Primary Headache in the Pediatric Population.
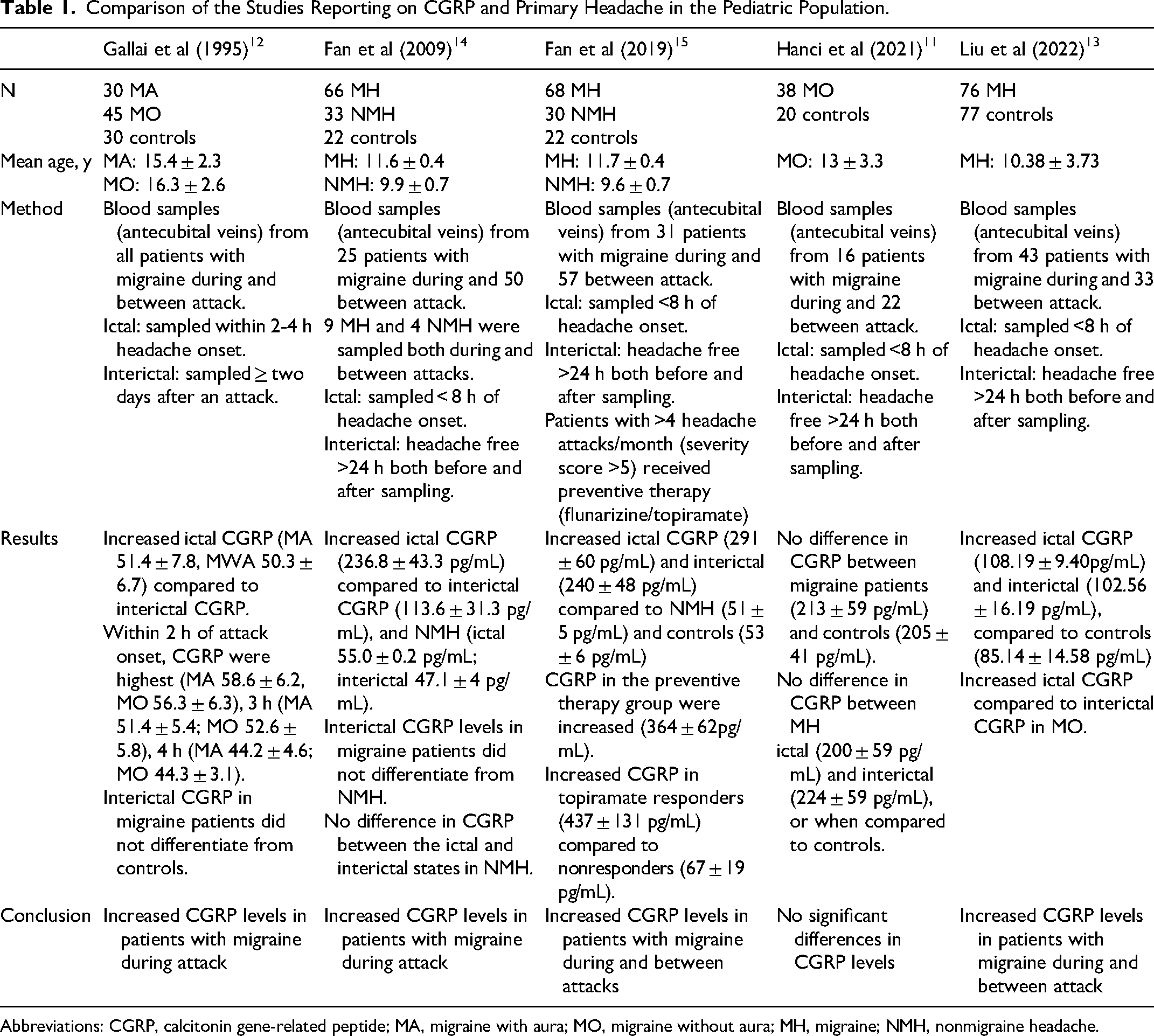
Abbreviations: CGRP, calcitonin gene-related peptide; MA, migraine with aura; MO, migraine without aura; MH, migraine; NMH, nonmigraine headache.
Diagnosing migraine in pediatric patients is often difficult. Young patients often face challenges in articulating or recalling specific details of their headache attacks, which complicates reliance on symptom-based diagnostic criteria such as those outlined in the International Classification of Headache Disorders (ICHD).13,16,17 Furthermore, pediatric migraine exhibits distinct features from its adult counterpart, 18 and many pharmacologic treatments have not proven to be more effective than placebo in relieving symptoms of pediatric migraine. 19 More objective measures, such as biomarkers to distinguish migraines from other primary headache disorders, could be beneficial.
For decades, studies have delved into the continuum theory, which proposes that migraine and tension-type headache are points on a spectrum of severity.20–22 Notably, in a study involving patients with chronic tension-type headache, it was observed that interictal plasma CGRP concentrations were elevated in those experiencing pulsating pain. 23 This observation, supported by prior research linking CGRP levels to migraines, may imply a potential pathophysiological connection between these headache types. Nerve fibers containing CGRP are found in extracranial cutaneous and perivascular tissue, also accompanying the small blood vessels running through the muscle bundles of the temporal and occipital regions. 24 Because of the prominent role that extracranial myofascial regions seem to play in the activation of the trigeminal system and the initiation of tension-type headache, we hypothesized that CGRP might be involved in tension-type headache. Furthermore, there appears to be a considerable shift from migraine to tension-type headache and vice versa in pediatric patients, with approximately 20% to 25% undergoing this transition within a matter of years. 25 This observation further supports the notion of a continuum.
Only a few studies have compared levels of CGRP in patients with tension-type headache with levels in patients with migraine. Gupta et al 26 did not find any statistically significant differences in plasma CGRP between patients with migraine, tension-type headache, and healthy controls. Ashina et al 23 found no difference in interictal plasma CGRP levels between patients with chronic tension-type headache compared with healthy control subjects.
All of the above-mentioned research affirms the need for ongoing research into CGRP as a biomarker, particularly because CGRP, if indeed implicated in the pathophysiology of pediatric primary headaches, could represent a promising therapeutic target.
In the present study, we aim to investigate CGRP levels in a Danish clinical cohort of children and adolescents with the most frequent primary headache forms, migraine and tension-type headache. We hypothesized that CGRP was involved in tension-type headache and therefore expected no significant differences between the patients with migraine and the patients with tension-type headache. We also expected ictal levels of CGRP to be higher than interictal levels in patients with tension-type headache.
Methods
Study Population
Participants were recruited from the Pediatric Headache Outpatient Clinic at the Pediatric Department of Herlev and Gentofte Hospital, Denmark, between April 2019 and April 2021. Inclusion criteria for the study required individuals to be between 5 and 18 years of age and diagnosed with a primary headache disorder. In our clinic, patients are referred to adult departments after the age of 18 years, but before the age of 19 years. Diagnoses were assigned manually after chart review using the International Classification of Headache Disorders 3rd edition (ICHD-3) 17 by trained research staff supervised by senior child neurologists with many years of experience in diagnosing headache disorders in children and adolescents. If there was any doubt about the patient's diagnosis, clinical consensus was reached via a multidisciplinary conference. The patients were divided into groups depending on their headache diagnosis, resulting in a group with migraine, another with tension-type headache, and a third group formed by patients diagnosed with both migraine and tension-type headache, referred to as the mixed group. All patients were summoned for blood sampling in consecutive order, independent of whether headache was present or absent on the day of examination. Consequently, some patients underwent blood sampling during a headache attack (ictally), whereas others were tested in the period between headache attacks (interictally). Several factors that might have an influence on CGRP levels were also reported: age, sex, body mass index, age of onset of headaches, family history of primary headaches, frequency of headache, duration of headache attacks, time since last headache attack, visual analog scale (VAS) during headache attack, and medication usage within the last 7 days. The data were obtained by reviewing medical records and conducting interviews on the day of examination. Headache frequency was categorized based on the number of headache days past month into daily (≥15 days per month), weekly (4-14 days per month), monthly (1-3 days per month), and less than monthly. A consistent frequency measure across all groups was necessary to enable comparison of the effect of headache frequency on CGRP levels. This generalized categorization was adopted instead of using the established frequency categories in ICHD-3, as the data available quantified headaches in the last months, whereas ICHD-3 categorizes based on a longer time frame. However, the cutoff of ≥15 days past month corresponds to a diagnosis of chronic headache according to the ICHD-3. Headache duration was determined by calculating the mean of the maximum and minimum recorded headache durations in minutes. Some patients reported experiencing persisting headaches around the clock, which we refer to as constant headache. The duration of headache disorder was derived by calculating the time in years from debut of first headache to the day of blood sampling.
Plasma CGRP Measurement
A volume of 20 mL of blood was drawn from the antecubital vein in an EDTA-containing tube and promptly centrifuged within 1 hour at 3000 rpm for 10 minutes at 4° C. The resulting plasma was collected into cryotubes and stored at −20° C for a maximum of 1 hour while examination of the patient was completed. Subsequently, the samples were transferred to a storage freezer at −80° C until being assayed for CGRP using the radioimmunoassay (RIA) method as previously described. 27 The RIA assay was chosen as it has been shown to be highly sensitive and specific to both a-CGRP and b-CGRP, but without cross-reactivity for calcitonin; cholecystokinin fragment 26-33 amide, nonsulfated; and gastrin I. Moreover, we have used this assay for many studies, and it is one of the most well-characterized assays 27 with quality specifications superior to most commercially available ELISA assays. 28 Samples were labeled using patient IDs. CGRP determinations were assayed blindly with regard to headache diagnosis and state (ictal vs interictal). CGRP analysis was performed between October 14, 2021, and October 28, 2021, by the Department of Clinical Biochemistry at Glostrup Hospital. The blood analyses were double-checked to ensure accurate processing in the laboratory.
Statistical Analysis
Continuous variables showing a Gaussian distribution were compared using the Welch t test and presented as means with accompanying standard deviation (SD). Non-Gaussian distributed variables were assessed with a Mann-Whitney U test and expressed as the median along with the interquartile range (IQR). To ascertain the normality of continuous data, both the Shapiro-Wilk test and the Q-Q plot were employed. Categorical variables were compared using the χ2 test. Statistical significance was set at P < .05. In our statistical analyses, we aimed to identify significant differences between the migraine and tension-type headache groups. When comparing these 2 groups, data from the mixed group were not included. Baseline cohort characteristics were conducted for the 3 groups (migraine, tension-type headache, and mixed) separately. Univariate linear regression was used to analyze the correlation between CGRP and headache diagnosis as well as the correlation between CGRP and all other relevant clinical variables. Studies have indicated that several factors can exert an influence on CGRP. Higher levels of CGRP are seen in women as compared to men and in patients with obesity or high body mass index. 29 Furthermore, levels of CGRP may decrease with age and may be correlated with severity of headache, medication use, and time since headache attack.30,31 Factors such as consumption of high-fat meals and physical activity may also impact CGRP levels. 32 Therefore, we examined these factors and adjusted the multivariate model for the following confounders: age, sex, family history of primary headaches, headache frequency, time elapsed since last headache attack, and medication usage within the last 7 days. It was not possible to perform a power analysis before the study because of missing data in the literature regarding expected differences between CGRP levels among children and adolescents with migraine compared to tension-type headache and between ictal and interictal levels of CGRP in patients with tension-type headache. All analyses were conducted using R statistical software (version 4.3.2).
Results
Study Population
Ninety-three patients initially met the inclusion criteria. Following the withdrawal of consent from 1 patient, the final study cohort consisted of 92 patients, aged 5-18 years, all diagnosed with a primary headache disorder. Of the 92 patients, 29 (31.5%) were diagnosed with migraine, 31 (33.7%) were diagnosed with tension-type headache, and 32 (34.8%) were diagnosed with both migraine and tension-type headache, forming the mixed group. The migraine group had a mean age of 12.6 years (± 2.9), whereas the tension-type headache group had a significantly higher mean age of 15.2 years ± 2.5 (P < .001). A skewed gender distribution was observed, with 26 (83.9%) of the patients in the tension-type headache group being female, compared with 10 (34.5%) in the migraine group (P < .001). The patients in the mixed group had a mean age of 13.9 years (±3.2), and 50% were female. The migraine patients started experiencing headaches at a median age of 7 years (IQR: 6-10), compared with 11.5 years (IQR: 10-13.8) in the tension-type headache group (P = .001). Regarding headache frequency, patients in the tension-type headache group were more likely to experience daily headaches, with 20 (64.5%) reporting daily attacks, compared with 1 (3.5%) in the migraine group (P < .001). Conversely, in the migraine group, 17 (58.6%) reported being more prone to monthly attacks, as opposed to 1 (3.2%) in the tension-type headache group (P < .001). Family history of primary headache disorders was more prevalent among the migraine group, with 26 cases (89.7%) compared with 11 (35.5%) in the tension-type headache group (P < .001). The baseline characteristics are shown in Table 2.
Baseline Characteristics. a
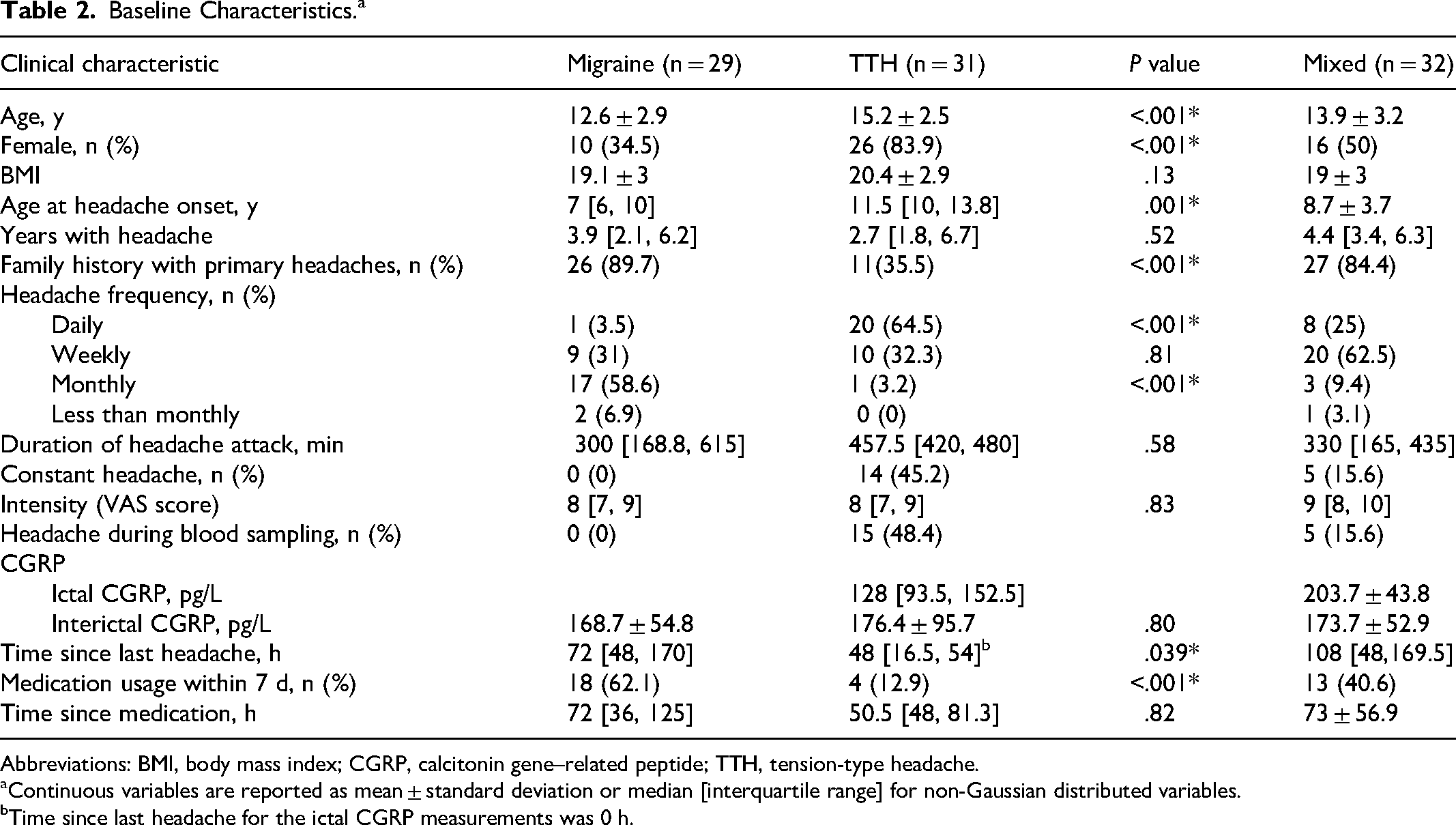
Abbreviations: BMI, body mass index; CGRP, calcitonin gene–related peptide; TTH, tension-type headache.
Continuous variables are reported as mean ± standard deviation or median [interquartile range] for non-Gaussian distributed variables.
Time since last headache for the ictal CGRP measurements was 0 h.
CGRP
All 29 migraine patients underwent blood sampling in the interictal period. In the tension-type headache group, 16 (51.6%) of the patients were sampled in the interictal period, whereas 15 (48.4%) were sampled during a headache attack. The mean level of interictal CGRP was 168.7 pmol/L (±54.8) in the migraine group and 176.4 pmol/L (±95.7) in the tension-type headache group. No statistically significant difference was observed between the 2 groups (P = .8; Figure 1). Migraine patients had a statistically significantly longer median time since their last headache before blood sampling of 72 hours (IQR: 48-170) compared with 48 hours (IQR: 16.5-54) in the tension-type headache patients (P = .039). Among patients with migraine, 18 (62.1%) reported using medication for a headache attack within the last 7 days before blood sampling, whereas only 4 (12.9%) reported similar usage in the tension-type headache group (P < .001).
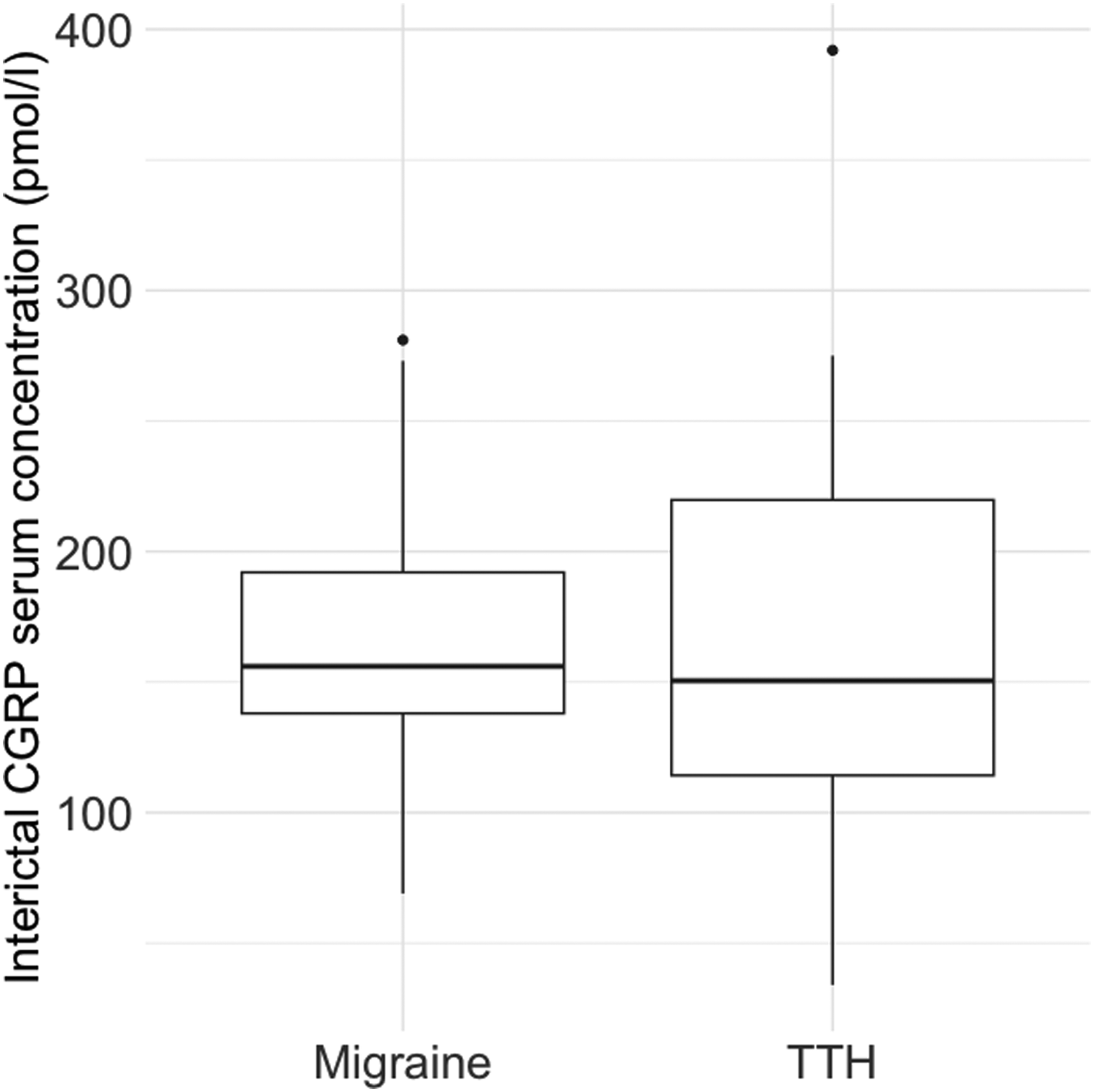
Box-and-whisker plot (median, first and third percentiles, range) of the interictal CGRP level in the migraine and TTH group. CGRP, calcitonin gene-related peptide; TTH, tension-type headache.
Among the 15 tension-type headache patients who underwent blood sampling during the ictal phase, their headache attack had been ongoing for a median of 4 hours (IQR: 2.25-6.50). The median value of CGRP in this group was 128 pmol/L (IQR: 93.5-152.5) (Table 1). Headache duration had no significant impact on CGRP levels during the ictal phase (P = .99). Although there was a difference in plasma CGRP levels in tension-type headache patients during the ictal (128 pmol/L) and the interictal (176.4 pmol/L) phase, this difference did not reach statistical significance (P = .27) (Figure 2). There was no difference in the ictal CGRP levels between the children with episodic and chronic headache (P = .9).
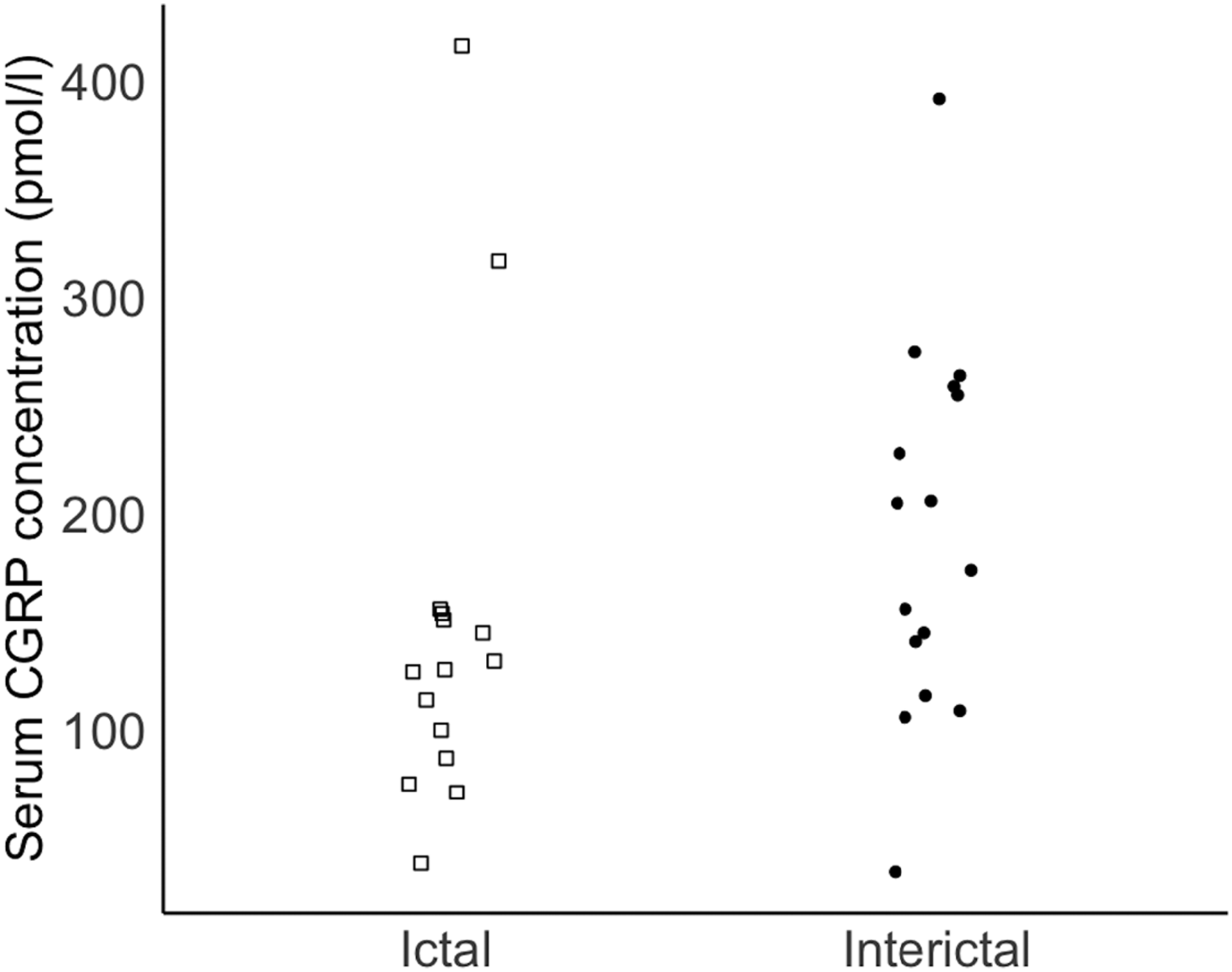
Ictal and interictal plasma CGRP in the TTH group. The open squares represent individual values of ictal CGRP, and the black dots represent individual values of the interictal CGRP. CGRP, calcitonin gene-related peptide; TTH, tension-type headache.
Mean interictal CGRP level in the patients in the mixed group was 173 pmol/L (±52.9). Five patients in the mixed group underwent blood sampling during the ictal phase, and the mean ictal CGRP level was 203.7 pmol/L (±43.8). These patients had either migraine, tension-type headache, or a combination of both at the time the blood sample was taken.
Correlation of CGRP Levels With Clinical Characteristics
We found no correlation between CGRP and headache diagnosis in univariate regression analyses (r2 = 0.0006, P = .8) or in multivariable regression analysis with correction for the possible confounders sex, age, family history of primary headaches, headache frequency, time elapsed since last headache attack, and medication usage within 7 days. Furthermore, in individual analyses, CGRP levels were determined to be independent of sex, age, family history with primary headaches, headache frequency, time since last headache, medication usage, and body mass index.
Discussion
In this study, we examined the levels of CGRP in children afflicted with migraine and tension-type headache. We found no statistically significant difference in interictal plasma CGRP levels between the 2 groups. In the tension-type headache group, although the ictal CGRP levels were lower than the interictal CGRP, this difference did not reach significance. As all migraine patients underwent blood sampling between headache attacks, we were unable to conduct a similar analysis in this group.
There were some statistically significant differences between the migraine and tension-type headache groups. Age of included patients in the tension-type headache group was higher, there were more females, age at headache onset was later, more participants had daily headache, and fewer had a family history with primary headache than in the migraine group. This is consistent with the natural course of migraine and tension-type headache. 22
We observed that CGRP levels did not correlate with headache diagnosis, sex, age, family history of primary headaches, headache frequency, time elapsed since last headache attack, medication usage, and body mass index. Several studies have previously reported on CGRP in migraine patients. However, to the authors’ knowledge, this is the first study to shed light specifically on CGRP levels within a pediatric population diagnosed with tension-type headache. Previous research has included tension-type headache in a combined non-migraine headache group, but has not analyzed the tension-type headache patients’ data separately, making our study a unique contribution to the understanding of CGRP in pediatric tension-type headache.
Migraine
Over the past decade, there has been notable advancement in our understanding of migraine pathophysiology, particularly in recognizing the important role played by CGRP.
In prior research within the pediatric population, the findings have been contradictory (Table 2). A study by Gallai et al 12 observed increased CGRP levels in plasma during migraine attacks in comparison to the period between attacks. A study by Fan et al 15 revealed elevated plasma CGRP levels in patients with migraine both during and between attacks, also confirmed in a recent study from 2022. 13 However, Hanci and colleagues 11 could not replicate the findings of increased CGRP levels in pediatric migraine patients. Their study revealed no change in plasma CGRP levels during or between attacks. Another study by Fan et al 14 reported elevated plasma CGRP levels during attack in children aged 4-18 years with migraine compared to children experiencing nonmigraine headaches (tension-type headache, epileptic headache, and headache secondary to sinusitis) and nonheadache patients. In this study, 9 of the migraine patients were blood sampled both during and between attack. Intriguingly, it was discovered that CGRP levels from 2 of the 9 patients with migraine were not significantly elevated ictally when compared with the interictal state. Furthermore, mean interictal CGRP did not significantly differ between the migraine and the nonmigraine group. When taking these findings into consideration, this might suggest the possibility of a subgroup within the pediatric migraine population that is CGRP-independent. 14 Given that different CGRP receptor antagonists have been shown to have a response rate of only between 50% and 80% in adults in various studies,10,33–38 it seems likely that there exists a CGRP-independent pathway for migraine. In the first mentioned study by Fan and colleagues, it was found that topiramate responders had higher plasma CGRP levels than topiramate nonresponders. 15 Based both on previous research and in the light of our own findings, we therefore suggest that CGRP may serve as a valuable biomarker in the guidance of pediatric migraine treatment, but that it may not be sufficient as a biomarker for migraine diagnosis. As seen in Table 1, only 2 of the mentioned studies found the baseline (interictal) CGRP to be elevated in pediatric migraine patients. As in Fan et al,14 we did not find differences in interictal CGRP levels between migraine and nonmigraine, but we did not find elevated interictal levels in patients with migraine. This discrepancy might be explained by differences in methods (Table 1) or the included patient groups (eg, as with regard to headache severity or frequency). 28
Tension-Type Headache
The role of CGRP in tension-type headache is only sparsely investigated.26,39 Gupta et al 25 included 3 groups: adult patients with migraine, adult patients with tension-type headache, and healthy controls. There were no statistically significant differences in plasma CGRP between the groups. 25 In another study conducted on adults, it was found that there was no difference in interictal plasma CGRP levels between those with chronic tension-type headache and healthy control subjects. 23 In an exploratory analysis, Ashina and colleagues 23 discovered that 8 chronic tension-type headache patients whose usual headache quality was pulsating had significantly higher levels of plasma CGRP. In studies concerning the pediatric population, to the authors’ knowledge, tension-type headache has only been included as part of nonmigraine groups alongside other headache diagnoses, but not as a separate tension-type headache-group. In the previously mentioned study by Fan et al, there was no significant difference in the CGRP levels of nonmigraine headache patients between ictal and interictal periods. In our study, ictal CGRP levels were lower than interictal levels. Although the difference was not statistically significant, the finding is unexpected. The difference could potentially be attributed to the small sample size, where individual variations may have had a greater influence on the observed outcome. This finding highlights the need for future, larger studies that include patients with tension-type headache and incorporate detailed headache characteristics (eg, pulsating quality) to explore this further.
The pathophysiology of tension-type headache involves a complex interplay of genetic, peripheral (including myofascial and vascular), and central factors. 40 Although cranial hemodynamics do play a role in tension-type headache, their influence is less pronounced as compared to in migraine. 41 However, it is possible that the emergence of pulsating pain in some tension-type headache patients may be linked to their increased levels of CGRP, which is known to be a potent vasodilator. Studies have consistently reported normal CGRP concentrations in the average adult tension-type headache patient. As mentioned in the introduction, the involvement of the trigeminal system plays a key role in both tension-type headache and migraine, pointing toward shared pathologic features.42–45 Although the continuum theory has faced counterarguments, such as the varying responses to triptans between the 2 groups, 20 it raises an intriguing question of whether tension-type headache patients with elevated CGRP levels potentially could find relief through triptan treatment, given its capacity to block CGRP release. 46 As stated earlier, it is not unusual for children to transition between headache diagnoses. In children, there is a higher degree of overlap between the diagnosis of migraine and tension-type headache than in adults. 16 We do not have data on the prevalence of pulsating headaches among the tension-type headache patients in our study, but investigating this aspect in future studies could be interesting.
Interestingly, in our study, ictal levels of CGRP in the patients in the mixed group were elevated in comparison to interictal levels. The interictal CGRP levels in this group were comparable with those in the migraine and tension-type headache groups. Because there was a tendency toward nonelevated ictal CGRP levels in the tension-type headache group, we suggest that this difference between ictal and interictal levels in the mixed group could be caused by migraine. As we have not included ictal CGRP measurements in the migraine group in our study, we cannot confirm the findings of prior studies that have found elevated ictal CGRP levels in migraine patients. We suggest that in future studies both ictal and interictal levels should be examined in tension-type headache, migraine, and mixed groups.
The levels of CGRP in both the tension-type headache group and the mixed group in our study are higher than levels previously measured in nonmigraine headache populations and healthy controls (Table 1). As described previously, assay choice and many other factors can influence the measured level of CGRP. However, these elevated levels could also be discussed in the light of the continuum theory.20–22
Although ICHD criteria try to differentiate headache diagnoses based on clinical characteristics, there are challenges associated with distinguishing tension-type headache from migraine, as evidenced by various common epidemiologic, clinical, and pharmacologic features22,47 that support the previously mentioned continuum theory.20–22 Revising the classification system in order to fit the possible common underlying pathophysiology could be considered.
A variety of variables (headache diagnosis, sex, age, family history of primary headaches, headache frequency, time elapsed since last headache attack, medication usage, and body mass index) did not correlate with CGRP levels in our study. Another study has likewise not found a significant correlation between sex and CGRP level. 15 On the other hand, Liu et al found that low headache frequency (<15 per month) had a marginally significant inverse correlation with interictal plasma CGRP level in patients with migraine (P = .05). 13 We were not able to reproduce these findings in our own study. The most notable distinction between this study and our own lies in the size of their study population: 76 children with migraine vs 21 children with migraine in our study population, and their categorizing of frequency in 0 to 15, 15 to 30, and 30 to 60 times per month, where we categorized frequency as <1, 1 to 3, 4 to 14, and >15 times per month.
Limitations
Some limitations of this study need to be addressed. First, our cohort consisted of a limited number of patients, which could signify that the study lacks statistical power to detect genuine differences between the groups. Second, unlike most prior studies, our protocol did not require the study population to be free of headaches for a minimum of 24 hours before blood sampling. Consequently, our interictal CGRP may be more closely timed with recently experienced headache attacks and may not have returned to baseline. There was a longer median time since last headache in patients with migraine compared to patients with tension-type headache, and these differences in sampling time might limit the interpretation of differences in interictal level between the groups. However, we did not identify a correlation between CGRP levels and the time elapsed since last headache attack. Third, blood was collected from the ictal tension-type headache patients at any time within 170 hours of headache onset, as long as their headache was still ongoing. CGRP levels have previously been shown to peak within 2 hours of onset of migraine headache attacks, followed by a gradual decrease. 12 The timing of blood sampling could thus potentially influence the measured CGRP in patients with ongoing tension-type headache if CGRP concentration (as in patients with migraine) decreases over time after headache onset. Fourth, our sampling approach resulted in a lack of ictal blood samples within the migraine group. It is important to acknowledge the difficulties in procuring ictal blood samples from children and adolescents within the migraine group. These participants may find it difficult to physically attend hospital visits for blood sample collection during a migraine attack. Fifth, we identified some outliers with high levels of CGRP (Figure 2), emphasizing the interindividual variation of CGRP levels. As stated in the introduction, it is important to consider that factors such as consumption of high-fat meals and physical activity may impact CGRP levels. 32 We did not inquire of the patients’ dietary intake or if they had exercised before blood sampling. This could potentially help in understanding the presence of outliers and should be considered in future research on CGRP levels. Sixth, there could be a bias due to our inclusion of a clinical cohort that might not be representative of the general population of patients with primary headaches. Approximately one-third of the included patients had tension-type headache, although most patients with tension-type headache may never consult a doctor. Median pain intensity for our tension-type headache patients was 8/10, which is higher than expected for patients with tension-type headache, who by definition have mild-moderate intensity, although these criteria can be difficult to use in the pediatric population.16,17 Therefore, participants with more severe headache than in a population-based cohort might have been included in our cohort. Our migraine group was predominantly male, although prevalence of migraine in adults is higher in females than in males. 48 The mean age of the patients in the migraine group was 12.6 years, and migraine is more prevalent in males than females until puberty, where incidence in the female population rapidly increases. 49
Conclusion
This study did not find a significant difference in interictal CGRP levels between patients with migraine and patients with tension-type headache. In patients with tension-type headache, there was no significant difference between CGRP levels in the ictal and interictal state. CGRP levels were not correlated with sex, age, family history of primary headaches, headache frequency, time since last headache, medication usage, or body mass index. We were not able to draw conclusions about differences in ictal CGRP levels in patients with migraine compared with patients with tension-type headache, or in differences between ictal and interictal levels in patients with migraine. Future studies should aim to replicate these results in a larger study cohort.
Footnotes
Acknowledgements
Christian Bach Vase, Josefine Lund, Merve Colak, Stefni Ravichandran.
Author Contributions
MMF contributed to analysis and interpretation. AABU contributed to acquisition and interpretation. AFS contributed to acquisition and interpretation. NRJ contributed to analysis and interpretation. NMMD contributed to acquisition, analysis, and interpretation.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Regional Scientific Ethics Committee (reference number: H-19003374) and the Danish Data Protection agency (reference number: VD-2019-222). Prior to participation, signed, informed consent was obtained from all adults with parental custody.