
Abstract
Objectives
To evaluate the demographic, clinical, laboratory, and prognostic data of children with acute disseminated encephalomyelitis with respect to anti-myelin oligodendrocyte glycoprotein (MOG) antibody status.
Methods
Acute disseminated encephalomyelitis patients (n = 245) from 24 centers followed up between 2010 and 2022 were evaluated retrospectively. The short- and long-term outcome characteristics (disease severity and course, clinical relapse, and recovery rates) were assessed. Incomplete clinical recovery was defined as modified Rankin Score ≥1 or the presence of epilepsy. Univariant and multivariant analysis were performed for outcome characteristics.
Results
The mean age at diagnosis was 6.3 ± 3.8 (0.5-17.7) years and the median follow-up was 22 (3-132) months. The outcome characteristics were evaluated in 180 of 245 patients (73.4%) with at least 12 months’ follow-up. Twenty-three patients (12.6%) relapsed. The multivariable logistic regression analysis revealed the following clinical parameters as predictors of relapse: sex, visual impairment, and ataxia at initial presentation. Incomplete clinical recovery (n = 42/180, 23.3%) was associated with the presence of seizures on admission and the need for an intensive care unit. Anti-MOG antibody positivity was not associated with an increased risk of relapse (25% vs 13.1%, P = .164) or incomplete clinical recovery (P = .511).
Conclusion
The nationwide cohort presented further supports the typically monophasic nature of acute disseminated encephalomyelitis, and a high rate of complete recovery. The presence of certain symptoms in the acute period may assist the clinician in estimating the outcome.
Acute disseminated encephalomyelitis (ADEM) is an immune-mediated, inflammatory demyelinating disorder of the central nervous system. It is characterized by encephalopathy and multifocal neurologic signs, often triggered by an infection or immunization.1,2 Acute disseminated encephalomyelitis is more common in males and children aged 5-8 years, with a prevalence of 0.3 to 0.6 per 100 000. 3 The diagnosis is based on clinical features and abnormal magnetic resonance imaging (MRI) findings typically showing diffuse, large, poorly defined white matter lesions on T2-weighted and fluid-attenuated inversion recovery sequences. Gray matter, particularly basal ganglia, may also be involved.4,5 Long-term follow-up reveals that most acute disseminated encephalomyelitis cases experience only 1 episode.4,6 The rate of recurrence ranges from 0% to 42% of all pediatric acute disseminated encephalomyelitis cases, with considerable variation among research groups.4,6-11
Demyelinating diseases of the central nervous system in childhood also include chronic recurrent conditions like multiple sclerosis and neuromyelitis optica spectrum disorder.1,2,6 These may initially present with an acute disseminated encephalomyelitis-like episode. Therefore, distinctive features will serve as diagnostic and prognostic biomarkers in the acute period. In recent years, myelin oligodendrocyte glycoprotein (MOG) antibody-associated disease (MOGAD) was recognized as a distinct inflammatory demyelinating disease of the central nervous system. It can present various clinical pictures like isolated optic neuritis, myelitis, multifocal acute disseminated encephalomyelitis-like demyelination, or cortical encephalitis; it is associated with antibodies against myelin oligodendrocyte glycoprotein (MOG) in the serum and has a pathogenesis distinct from multiple sclerosis. 12 While MOG antibody–associated disease may share features with neuromyelitis optica spectrum disorder, it also has distinct characteristics. The presence of anti-MOG antibodies has been associated with a higher risk of relapse, reported at around 50% in prior acute disseminated encephalomyelitis cohorts.10,11,13-17
Knowledge of factors related to relapse risk and prognosis affects clinical management. 18 The objectives of our study were to evaluate the demographic, clinical, laboratory, and outcome characteristics of acute disseminated encephalomyelitis in a large pediatric cohort. In particular, we aimed to investigate the impact of anti-MOG antibodies on the clinical and radiologic features of children who experience relapses following their initial presentation of acute disseminated encephalomyelitis.
Materials and Methods
Study Group
Patients <18 years of age from 24 tertiary referral centers in Turkey who were admitted during a first acute demyelinating event and discharged with the diagnosis of acute disseminated encephalomyelitis between 2010 and 2022 were evaluated (n = 245). The diagnosis of acute disseminated encephalomyelitis was based on both clinical (polyfocal central nervous system involvement along with encephalopathy that cannot be explained by fever, systemic illness, or postictal symptoms) and radiologic findings in accordance with the guidelines outlined by the International Pediatric Multiple Sclerosis Study Group (IPMSSG) in 2013. 19 Patients with the encephalitic form of MOG antibody–associated disease were excluded. The clinical features and outcomes of the series were reviewed, and the patients who had a serum anti-MOG antibody test result were also evaluated separately.
Clinical Evaluation
The prodromal and clinical symptoms that appeared both before and during the hospitalization period were recorded. Prodromal symptoms included headache, fever, fatigue, nausea, and vomiting. Clinical symptoms and signs on admission included altered state of consciousness, meningeal irritation, emotional and behavioral symptoms, motor or sensory deficit, movement disorders, sphincter dysfunction, ataxia, visual impairment, diplopia, cranial nerve palsy, seizures, aphasia, and papilledema. The severity of the first attack of acute disseminated encephalomyelitis was assessed based on the following variables: Glasgow Coma Scale score (<6, 6-10, >10), the need for intensive care unit (ICU) admission, duration of ICU admission, and need for mechanical ventilation. If present, characteristics of seizures, antiseizure medications, and the development of post–acute disseminated encephalomyelitis epilepsy as defined below, were also recorded.
Neuroimaging
Cranial and all available spinal MRI scans performed at disease onset were assessed. Follow-up neuroimaging had been obtained between 3 and 24 months after the initial scan. The principal investigators (S.K., S.Y.) categorized the MRI findings according to the reports provided by neuroradiologists of the participating centers. Lesions were defined based on hyperintensities observed on T2-weighted and T2–fluid-attenuated inversion recovery sequences in line with established radiologic criteria for acute disseminated encephalomyelitis and classified by location: subcortical and central white matter, corpus callosum, cortical and deep gray matter, basal ganglia, thalami, brain stem, cerebellum, spinal cord, periventricular area, and optic nerve involvement. Additionally, the contrast enhancement of the lesions was recorded.
Biomarkers
All patients underwent serum biochemical analysis and 83.2% also had cerebrospinal fluid testing. White blood cell and platelet counts, erythrocyte sedimentation rate, and cerebrospinal fluid analysis (pleocytosis, oligoclonal band test, immunoglobulin G [IgG] index) results were recorded. Oligoclonal bands were considered positive if they were present only in the cerebrospinal fluid (type 2) or if they were detected in both the cerebrospinal fluid and serum, with additional distinct bands observed exclusively in the cerebrospinal fluid (type 3). Because anti-MOG antibody testing became available in our country in 2016, anti-MOG antibody analysis could be performed in cases that presented subsequent to this date. Anti-MOG antibodies were analyzed using a serum fixed cell-based assay, and titers greater than 1:100 were considered as clear positive, titers between 1:10 and 1:100 as low positive. The diagnosis of MOG antibody–associated disease in patients with low positive titers was according to the recently published criteria based on the presence of one of 3 supportive clinical or MRI features: optic neuritis, myelitis, or a brain, brainstem, or cerebral syndrome compatible with MOG antibody–associated disease. 8 Only patients meeting these criteria were included in the anti–MOG-positive group.
Treatment Modalities
The immunotherapy regimens and additional treatments for each patient were documented. Immunotherapy included steroids, intravenous immunoglobulin (IVIg), plasma exchange, and rituximab. The time between the onset of symptoms and the initiation of appropriate treatment was noted as treatment lag (first day, 2-7 days, and ≥7 days).
Outcome
Long-term Outcome
The long-term outcome was examined in patients who had been followed for at least 1 year. Outcome measures included neurologic disability and epilepsy at the end of 1 year. The modified Rankin Score for functional outcome was scored as follows: 0 = no residual symptoms; 1 = no significant disability despite symptoms; 2 = modest disability; 3 = moderate disability requiring external support; 4 = fairly severe disability restricting walk; 5 = severe disability necessitating ongoing care; and 6 = death. Complete clinical recovery was defined as the absence of any deficits or epilepsy. Incomplete clinical recovery was defined as modified Rankin Score ≥1 or the presence of epilepsy.
Relapse
Based on the 2013 criteria established by the International Pediatric Multiple Sclerosis Study Group (IPMSSG), a relapse is defined as the emergence of new symptoms at least 3 months following the initial attack of acute disseminated encephalomyelitis, regardless of the use of steroids. 19 The patients with relapses were classified into following diagnostic categories: (1) multiphasic acute disseminated encephalomyelitis is defined as a new acute disseminated encephalomyelitis episode that occurs three months or more after the initial event and involves new clinical and MRI abnormalities, or the recurrence of previous clinical and MRI findings; (2) acute disseminated encephalomyelitis–optic neuritis refers to acute disseminated encephalomyelitis or multiphasic acute disseminated encephalomyelitis followed by episodes of optic neuritis; 12 and (3) multiple sclerosis is defined as a second demyelinating event with no encephalopathy occurring 3 months or longer after the initial episode with new lesions on brain MRI consistent with multiple sclerosis, or, for patients ≥12 years, fulfilling the revised McDonald 2010 criteria. 20 Risk factors for recurrent disease were evaluated in patients who experienced relapses and were followed for at least 1 year. Statistical analyses concerning relapse were conducted only for the first relapse after the initial event. Multiple relapses were assessed solely to determine any changes in the diagnosis of acute disseminated encephalomyelitis.
Prognostic Factors
The following prognostic factors were evaluated: age, sex, preceding event, clinical features in the acute phase of the disease (seizures at onset, Glasgow Coma Scale score, and modified Rankin Score on admission), biomarkers (white blood cell and platelet counts, erythrocyte sedimentation rate, cerebrospinal fluid analysis, and anti-MOG antibody status), treatment lag, the use of single or multiple treatment modalities (steroids, IVIg, plasmapheresis), the need for and the duration of ICU admission, and mechanical ventilation. These variables were in relation with the outcome parameters: (1) the long-term neurologic status and (2) relapse.
Statistical Analysis
Data set was analyzed using IBM SPSS, version 25 (IBM Corp, Armonk, NY). Descriptive statistics were presented as the mean and standard deviation (SD) for continuous variables when the data followed a normal distribution; otherwise, the median (minimum-maximum) was reported. The normality of the data was assessed using the Shapiro-Wilk and Kolmogorov-Smirnov tests. Independent t test was used for parametric data, and the results were given as mean ± SD. Mann-Whitney U test was used for nonparametric data, and the results were given as the median (minimum-maximum). Categorical variables were tested using Pearson χ2 or Fisher exact test according to number of variables, and the findings were presented using marginal and contingency tables. Independent variables with P values below .20 in bivariate analysis were selected for inclusion in the model. The Backward LR method of logistic regression was used to assess the relationship between the dependent (long-term outcomes and relapse) and independent variables (risk factors). Odds ratios (ORs) and their 95% confidence intervals (CIs) were computed, with P values less than .05 indicating statistical significance. The study was approved by the Ege University Medical Research Ethics Committee (project No.: 22-1.1 T/5).
Results
Demographic and Clinical Landscape of the Cohort
The male-to-female ratio was 1.66:1. The mean age at diagnosis was 6.3 ± 3.8 (0.5-17.7) years, and the median follow-up duration was 22 (3-132) months. The most common symptoms on admission besides encephalopathy (81.6%) were motor deficit (58.8%), fatigue (57.1%), and headache (40.4%) (Table 1).
Clinical Characteristics of the Whole Cohort With the Initial Diagnosis of Acute Disseminated Encephalomyelitis (n = 245).
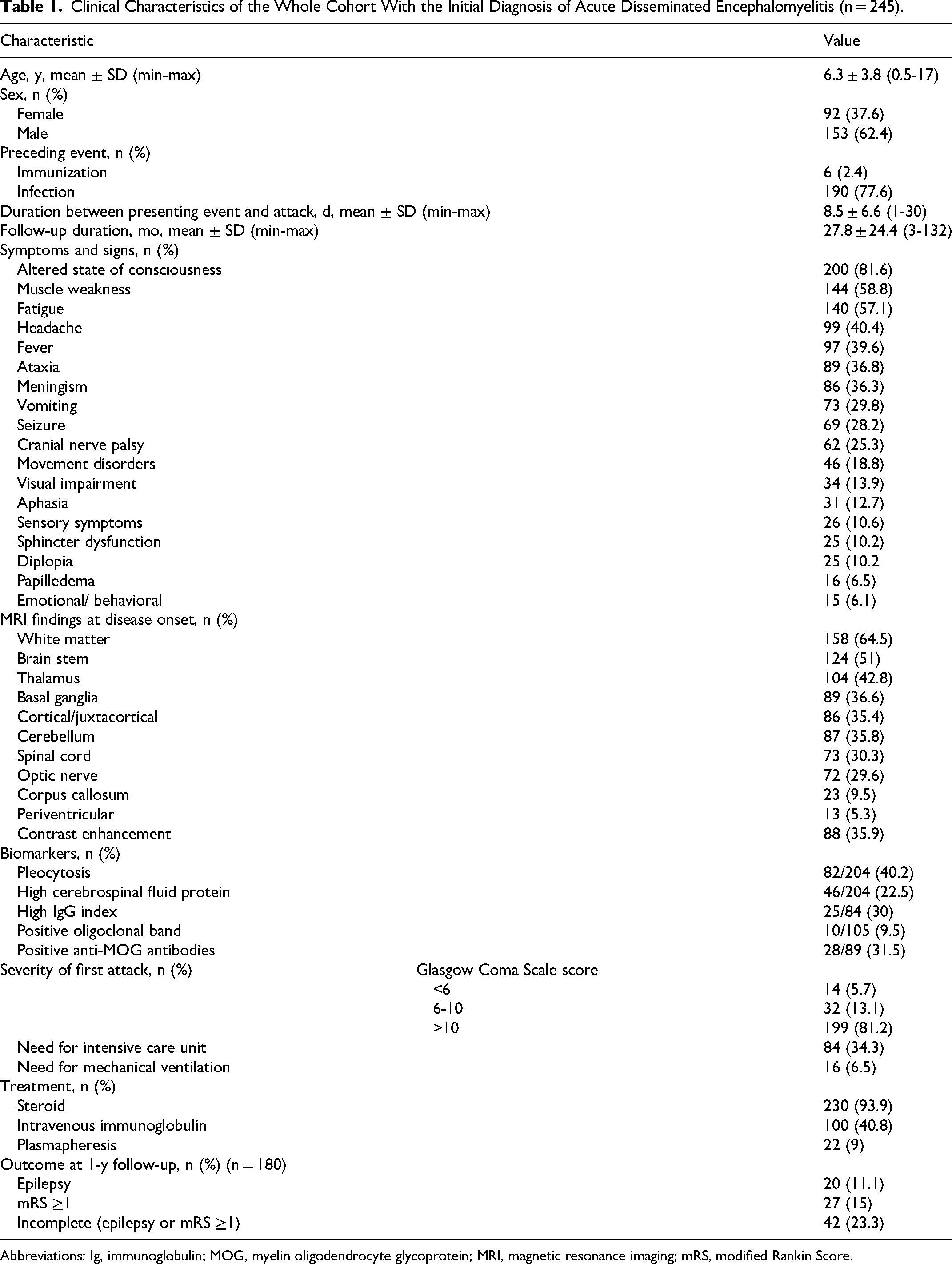
Abbreviations: Ig, immunoglobulin; MOG, myelin oligodendrocyte glycoprotein; MRI, magnetic resonance imaging; mRS, modified Rankin Score.
Sixty-nine patients (28.2%) presented with seizures. Of these, 55% had generalized, 31.8% had focal, and 13% had focal to bilateral seizures. No antiseizure medication was initiated after acute seizure treatment in 6 patients. Nonconvulsive status epilepticus developed in 1 patient. Monotherapy was successful for seizure control in 74% of patients with seizures, whereas 4 patients (5.8%) required more than 1 antiseizure medication. Levetiracetam (46.1%) and phenytoin (30%) were the most frequently used antiseizure medications in the acute phase.
Cerebrospinal fluid pleocytosis was observed in 40.2% (82 of 204) patients. Cerebrospinal fluid protein was increased in 22.5%, IgG index was elevated in 30%, and oligoclonal band were positive (type 2 pattern n = 8, type 3 pattern n = 2) in 9.5%. Serum anti-MOG antibodies were tested in 89 of 245 patients (36%); 28 (31.5%) of them resulted positive (Table 2). This group was younger than the seronegative group (5.1 ± 2.7 vs 7.1 ± 3.4, P = .006). The clinical features of anti-MOG antibody positive and negative acute disseminated encephalomyelitis patients were similar, as were their laboratory markers except higher white blood cell counts in the antibody-positive group (P = .05; Table 2).
Clinical Characteristics and Outcomes of the Patients With Respect to Anti-MOG Antibody Serostatus (n = 89).
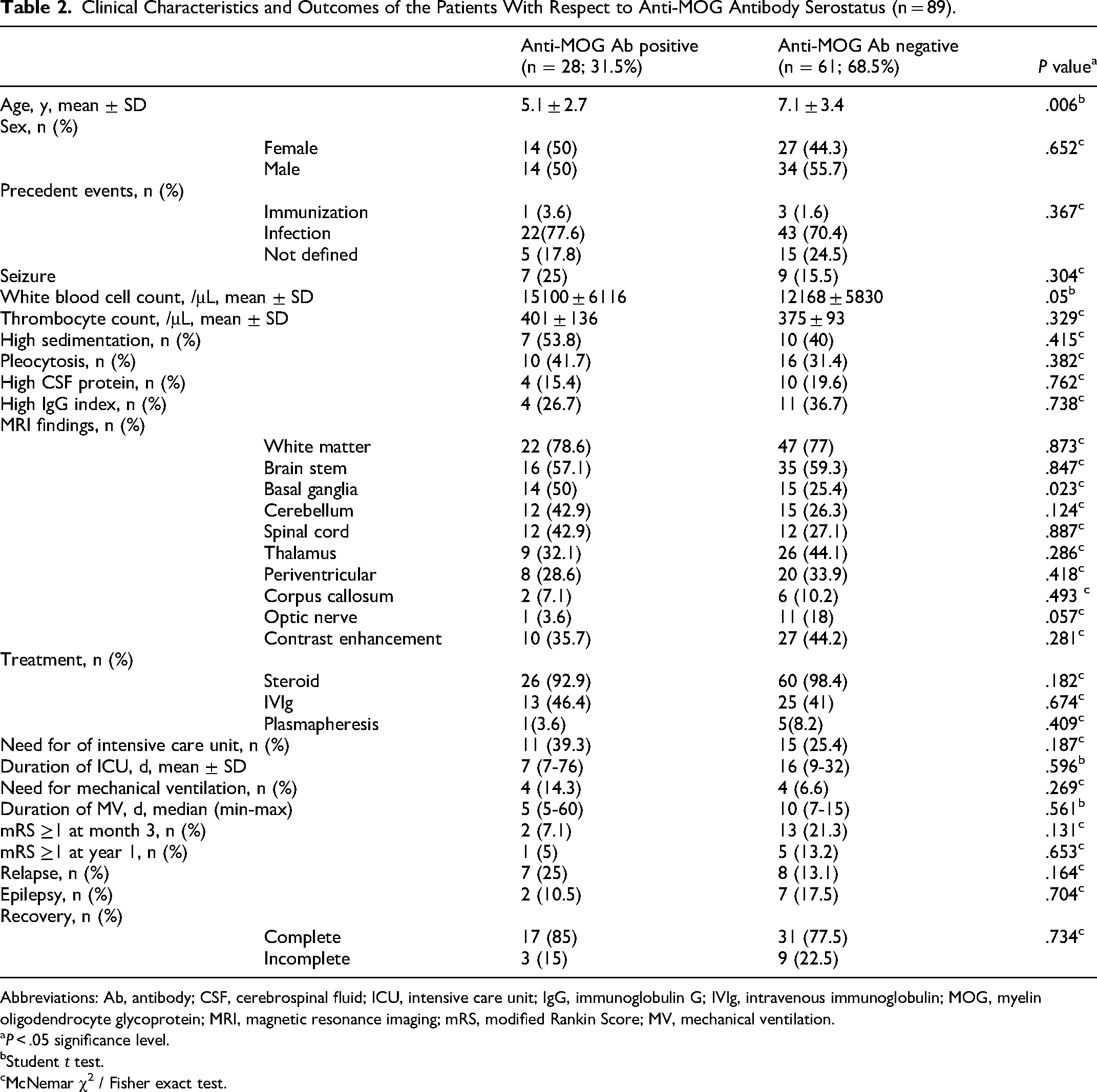
Abbreviations: Ab, antibody; CSF, cerebrospinal fluid; ICU, intensive care unit; IgG, immunoglobulin G; IVIg, intravenous immunoglobulin; MOG, myelin oligodendrocyte glycoprotein; MRI, magnetic resonance imaging; mRS, modified Rankin Score; MV, mechanical ventilation.
P < .05 significance level.
Student t test.
cMcNemar χ2 / Fisher exact test.
MRI Characteristics
The distribution of affected areas at the time of initial diagnosis is presented in Table 1. The most commonly involved regions were the white matter (64.5%), brainstem (51%), and thalamus (42.8%), followed by the basal ganglia (36.6%), cerebellum (35.8%), cortical-juxtacortical regions (35.4%), and the spinal cord, which was affected in 44 of 145 patients (30.3%). Contrast enhancement was present in 84 of 235 patients (35.9%).
The radiologic findings of acute disseminated encephalomyelitis patients with and without anti-MOG antibodies are shown in Table 2. Children with anti-MOG antibodies had significantly higher basal ganglia involvement compared to those without anti-MOG antibodies (50% vs 25.4%, P = .023). They also had more spinal cord involvement (42.9%) than the seronegative patients (26.3%), but the difference was not significant (P = .124).
Treatment Modalities
Immunotherapy was initiated on the first day in 24.5%, between 2 and 7 days in 56.7%, and after day 7 in 16.3% of patients. There was no statistically significant association between the first-year outcome and the treatment lag (P = .105) (Table 3). For first-line treatment, the majority of the patients (93.9%, n = 230) received steroids, whereas 6.1% (n = 9) received IVIg. Among those initially treated with steroids, 38.5% (91/236) required additional IVIg, and only 9% (22/236) required plasmapheresis. Sixty-one percent of patients were administered a single treatment modality, whereas 38.8% of the cohort were administered multiple treatment modalities. The administration of single or multiple therapy modalities during the early stages of disease did not have any influence on recovery or relapse (P > .05). First-line therapy was initiated with pulse methylprednisolone at a dosage of 30 mg/kg/d in 90%, and 20 mg/kg/d in 10% of the patients. The duration of pulse methylprednisolone treatment varied from 3 to 10 days (5 days in 70%, 3 days in 15%, and 7 days in 11%). The maintenance steroid dose ranged between 1 and 2 mg/kg/d prednisolone. A total of 22 patients (9%) underwent plasmapheresis consisting of 5 to 10 cycles (5 cycles in 50%, 7 cycles in 35%, and 10 cycles in 1 patient).
The Relation Between the 1-Year Outcome and Certain Clinical and Laboratory Parameters in Patients With Initial Diagnosis of Acute Disseminated Encephalomyelitis.
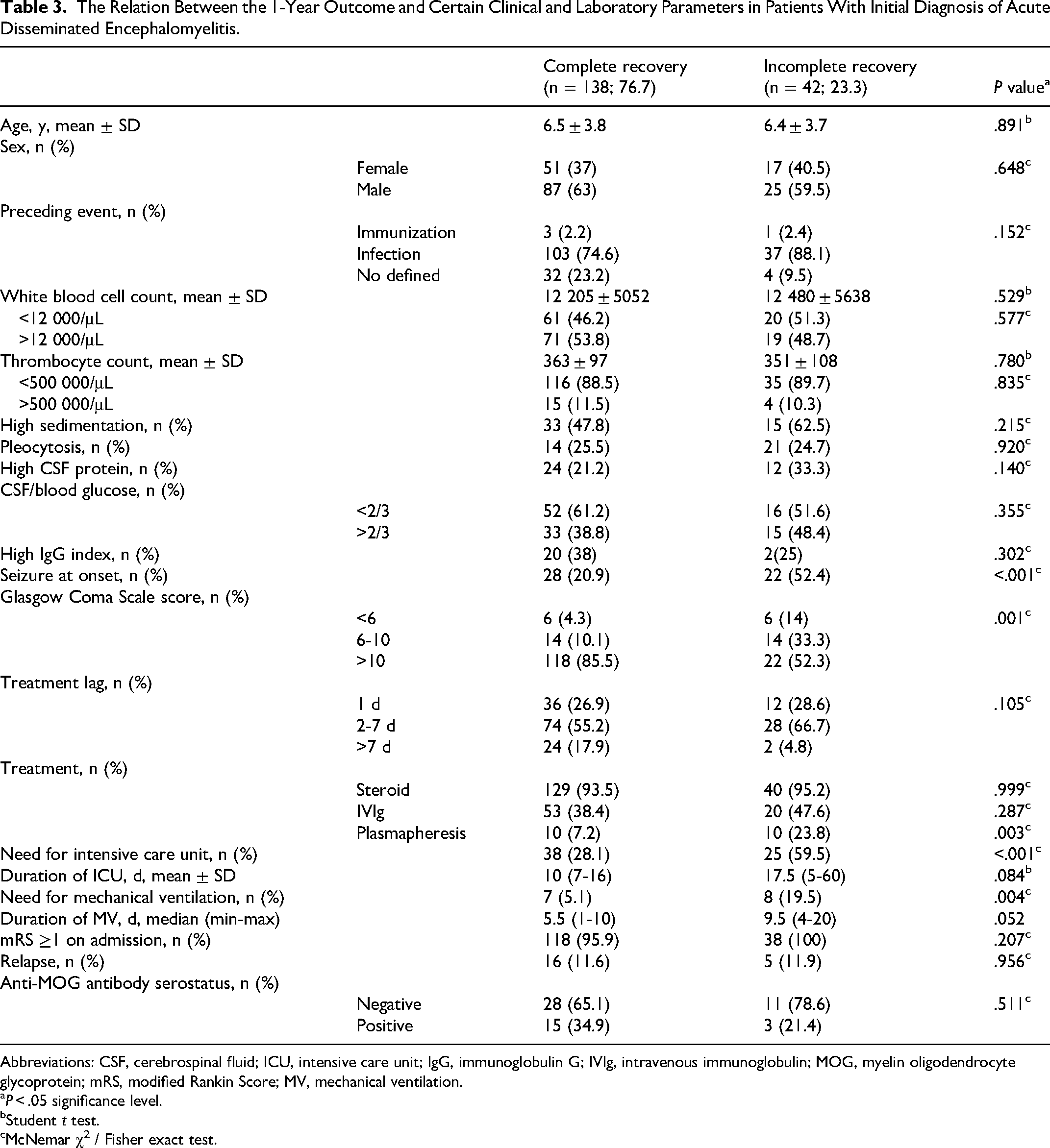
Abbreviations: CSF, cerebrospinal fluid; ICU, intensive care unit; IgG, immunoglobulin G; IVIg, intravenous immunoglobulin; MOG, myelin oligodendrocyte glycoprotein; mRS, modified Rankin Score; MV, mechanical ventilation.
P < .05 significance level.
Student t test.
cMcNemar χ2 / Fisher exact test.
Outcome Characteristics
In the cohort, 34.3% (84/245) required ICU admission and 6.5% (16/245) necessitated mechanical ventilation during their initial episode. Anti-MOG seropositivity did not impact the need for ICU admission, mechanical ventilation, or the duration of these interventions (Tables 1-3).
Long-term Outcome
The long-term outcome of 180 of the 245 patients (73.4%) with at least 12 months’ follow-up was evaluated (Table 3). The majority of patients (n = 138, 76.7%) had complete clinical recovery. The remaining 42 (23.3%) patients had incomplete clinical recovery: 27 with modified Rankin Score ≥1, 20 with post–acute disseminated encephalomyelitis epilepsy, and 5 had both. The spectrum of modified Rankin Score ≥1 comprised 4 in 2 patients, 3 in 1 patient, 3 in 6 patients, and 1 in 18 patients. Post–acute disseminated encephalomyelitis epilepsy was not associated with the presence of seizures on admission, anti-MOG antibody status, or the occurrence of relapse. The following 5 factors were related to incomplete clinical recovery: a Glasgow Coma Scale score <10 on admission (P = .001), the presence of seizures on admission (P < .001), the need for ICU (P < .001), the need for mechanical ventilation (P = .004), and treatment with plasmapheresis (P = .003).
The long-term overall outcome was not significantly impacted by anti-MOG serostatus (P = .511). The univariate analysis revealed 4 clinical parameters related to incomplete recovery: the presence of seizures on admission (odds ratio [OR] 4.164, 95% CI 1.997-8.684, P = .010), the need for ICU admission (OR 3.754, 95% CI 1.188-11.872, P = .025), the need for mechanical ventilation (OR 4.052, 95% CI 1.523-10.310, P = .005), and plasmapheresis (OR 4, 95% CI 1.534-10.429, P = .005) (Table 4).
Univariate and Multivariate Logistic Regression Analysis of 1-Year Outcome and Relapse.
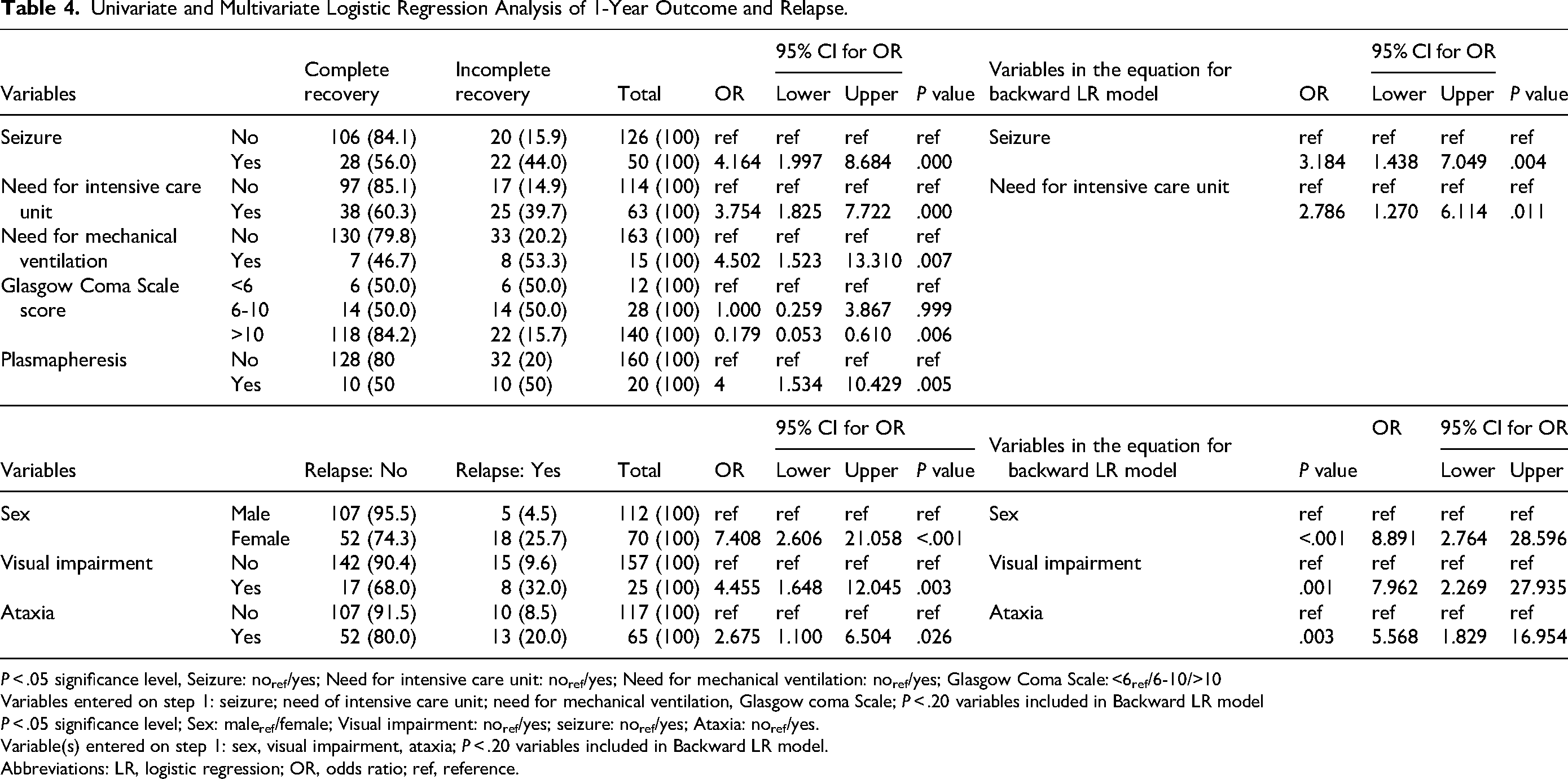
P < .05 significance level, Seizure: noref/yes; Need for intensive care unit: noref/yes; Need for mechanical ventilation: noref/yes; Glasgow Coma Scale: <6ref/6-10/>10
Variables entered on step 1: seizure; need of intensive care unit; need for mechanical ventilation, Glasgow coma Scale; P < .20 variables included in Backward LR model
P < .05 significance level; Sex: maleref/female; Visual impairment: noref/yes; seizure: noref/yes; Ataxia: noref/yes.
Variable(s) entered on step 1: sex, visual impairment, ataxia; P < .20 variables included in Backward LR model.
Abbreviations: LR, logistic regression; OR, odds ratio; ref, reference.
However, the multivariable logistic regression analysis identified only 2 clinical parameters significantly associated with the overall outcome: the presence of seizures on admission (OR 3.184, 95% CI 1.438-7.049, P = .004) and the need for ICU admission (OR 2.786, 95% CI 1.270-6.114, P = .011) (Table 4).
Relapse Rates of the Whole Cohort
Among the 180 patients with a one-year follow-up, 21 experienced relapses. Additionally, 2 patients with a follow-up period of less than 1 year also had relapses. The relapse rate was 12.6% (23/182). The median time to first relapse was 12 (4-72) months. Of all relapses, 56.5% occurred within the first year, 21.7% between 13 and 24 months, 17.4% between 25 and 48 months, and 4.3% beyond 49 months.
The multivariate logistic regression analysis identified significant associations between relapse and the following factors: female sex (OR 8.89, 95% CI 2.764-28.596, P < .001), presence of ataxia (OR 5.568, 95% CI 1.829-16.954, P = .003), and visual impairment at admission (OR 7.962, 95% CI 2.269-27.935, P = .001) (Table 4).
Of the 89 individuals tested for anti-MOG antibodies, the relapse rate was 25% (7/28) in seropositive and 13% (8/61) in seronegative patients (P = .164) (Table 2). Among patients who had serological testing and a 1-year follow-up, the relapse rate was 35% (7/20) in those anti-MOG positive and 19% (8/42) in anti-MOG negative (P = .211) (Table 5).
The Relation Between Clinical and Laboratory Findings and Relapse.
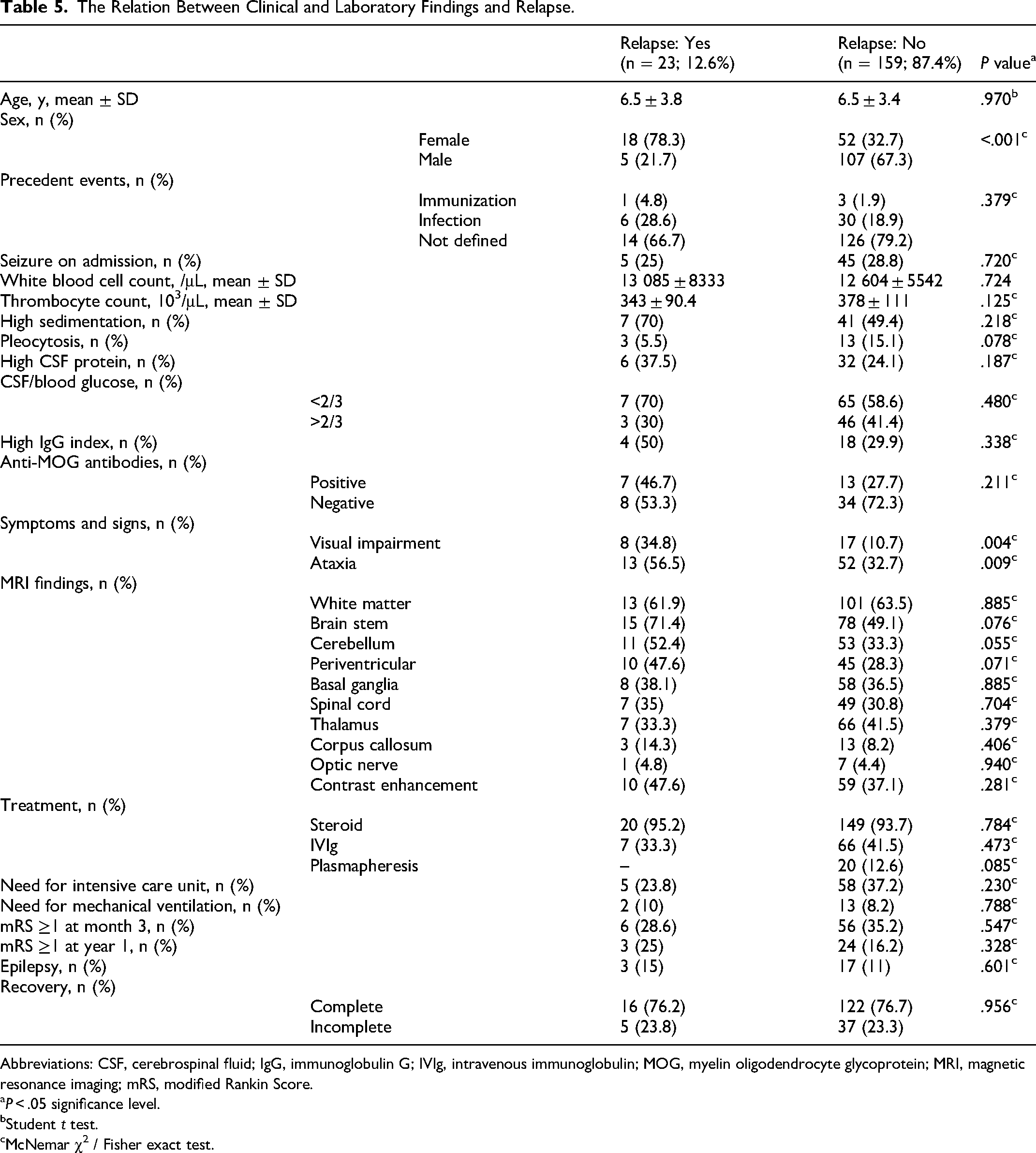
Abbreviations: CSF, cerebrospinal fluid; IgG, immunoglobulin G; IVIg, intravenous immunoglobulin; MOG, myelin oligodendrocyte glycoprotein; MRI, magnetic resonance imaging; mRS, modified Rankin Score.
P < .05 significance level.
Student t test.
cMcNemar χ2 / Fisher exact test.
Based on clinical, radiographic, and biochemical evidence, 20 of the 23 patients who experienced relapse were diagnosed as either multiphasic acute disseminated encephalomyelitis (n = 9, three anti-MOG antibody positive), acute disseminated encephalomyelitis–optic neuritis (n = 3, one anti-MOG antibody positive), or multiple sclerosis (n = 8, all female) (Figures 1 and 2). Three relapsing patients with anti-MOG antibodies who did not fully meet the criteria for any demyelinating disease remained as unclassified MOG antibody–associated disease patients. None of the 8 patients who received the diagnosis of multiple sclerosis within 10-60 months after the first attack had anti-MOG antibodies (Figure 2).
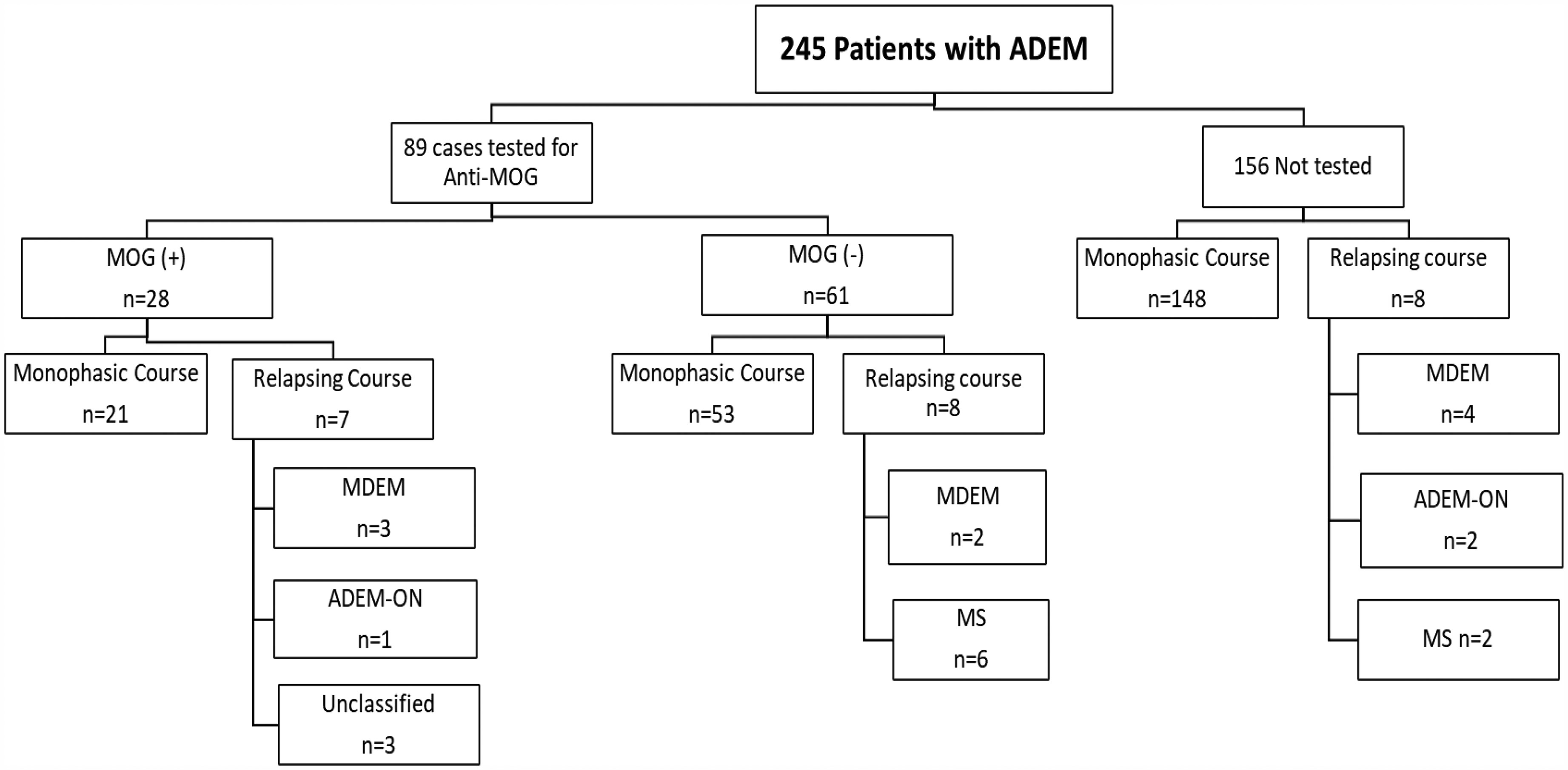
Flowchart of the whole cohort with ADEM regarding the disease course. ADEM, acute disseminated encephalomyelitis; anti-MOG Ab, myelin oligodendrocyte glycoprotein antibody; MOGAD, myelin oligodendrocyte glycoprotein associated disease; ON, optic neuritis; MS, multiple sclerosis; MDEM, multiphasic ADEM; ADEM-ON, ADEM-optic neuritis.
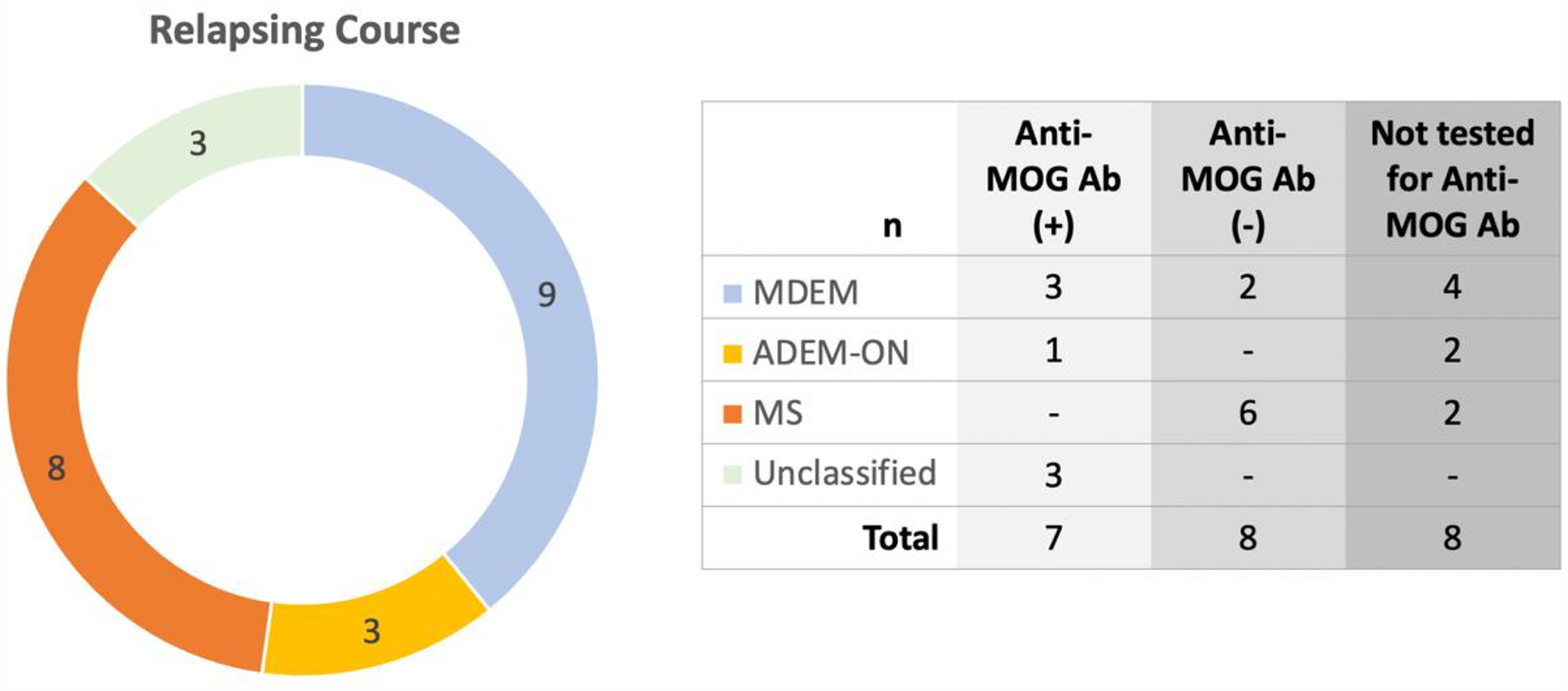
Final diagnoses of the relapsed patients with ADEM. ADEM, acute disseminated encephalomyelitis; MOG Ab, myelin oligodendrocyte glycoprotein antibody; ON, optic neuritis; MS, multiple sclerosis; MDEM, multiphasic ADEM; ADEM-ON, ADEM-optic neuritis.
Discussion
This multicenter study provides a comprehensive overview of the clinical landscape for pediatric acute disseminated encephalomyelitis patients with a focus on relapse rates and long-term overall outcomes. Key findings include the rates and risk factors associated with incomplete recovery and post–acute disseminated encephalomyelitis epilepsy. Additionally, the study provides the rate of MOG antibody–associated disease among acute disseminated encephalomyelitis cases in a large nationwide cohort.
Acute disseminated encephalomyelitis typically affects children younger than 10 years of age, mostly between 5-8 years, with a slight male predominance.21-24 Our findings were similar, with a mean age at diagnosis of 6.3 ± 3.8 years and a male-to-female ratio of 1.66:1. Anti-MOG antibody–positive patients were younger at diagnosis (mean 5.1 ± 2.7 years) and had a sex ratio consistent with previous reports. 25 Acute disseminated encephalomyelitis follows an acute infection in 50% to 86% of cases, whereas post-vaccine acute disseminated encephalomyelitis is rare, occurring in only 0.1 to 0.2 per 100 000 children.9,10,26-28 Similarly, 77.6% in our study had antecedent infections, whereas significantly fewer (2.4%) had an immunization. Neurologic manifestations of acute disseminated encephalomyelitis include pyramidal signs, ataxia, brainstem symptoms, optic neuritis, and transverse myelitis. In our cohort, the most common symptoms on admission aside from encephalopathy were motor deficit (58.8%), fatigue (57.1%), and headache (40.4%). The localization of lesions in our study aligns with findings from earlier research in acute disseminated encephalomyelitis patients: the subcortical white matter was the most commonly affected area.22,29 Approximately one-third of the patients had spinal cord involvement, usually extensive and asymmetric, often spanning several vertebral levels. These lesions were usually centrally located, affecting the white matter, and to a lesser degree, the gray matter.3,6 Various studies defined a difference in lesion localizations on MRI between MOG antibody positive and negative patients, indicating an increased number of extended spinal cord lesions, 30 more cortical and thalamic involvement, 31 and a higher incidence of cerebellar lesions 8 in anti-MOG antibody–positive children with acute disseminated encephalomyelitis. In our study, the only significant difference was more frequent basal ganglia involvement in anti-MOG antibody–positive patients (P < .05). Additionally, although statistically insignificant, patients with anti-MOG antibodies exhibited more spinal cord involvement than the seronegative children.
The present study demonstrated no correlation between lesion localization or contrast enhancement and recovery or relapse in the pediatric acute disseminated encephalomyelitis cohort. Prior studies have documented certain associations between MRI results and outcome: Tenembaum et al 6 identified a correlation between optic nerve involvement at presentation and final disability. Chen et al 32 indicated children with acute disseminated encephalomyelitis who had cerebellar lesions had significantly worse functional outcomes. Kanmaz et al 33 reported children with acute disseminated encephalomyelitis who had basal ganglia lesions on MRI tended to have more cognitive problems.
About 15% to 25% of children with acute disseminated encephalomyelitis require admission to a pediatric ICU, generally because of respiratory failure caused by coma, brainstem involvement, and status epilepticus.3,10,34 Our study revealed a similar rate (35%). The population-based study by Absoud et al 34 from the United Kingdom reported that the need for invasive mechanical ventilation among children with acute disseminated encephalomyelitis who were admitted to the ICU was 78%; this rate was only 19% in our cohort. The decision about ICU admission for acute disseminated encephalomyelitis patients tends to depend on institutional practice. A notable finding in this study was that the need for ICU admission and the need for mechanical ventilation were significantly associated with incomplete recovery in the long term, possible reflecting the severity of the initial acute event.
Most children with acute disseminated encephalomyelitis seem to have a complete recovery without any neurologic deficits.9,10,26 The rate of complete recovery, 76.7% in our cohort, is comparable to the 50% to 94% rates reported in the literature.9,10 The majority of publications define “complete” or “incomplete” recovery according to neurologic sequelae like post–acute disseminated encephalomyelitis epilepsy and physical impairment based on formal disability scores, such as the Expanded Disability Status Scale (EDSS) and the modified Rankin Score. However, long-term cognitive and psychiatric problems may arise in up to half of the patients and are less be likely to recognized during routine clinical visits.33,35,36 Chen et al 32 evaluated prognostic factors for functional recovery in children with moderate to severe acute disseminated encephalomyelitis, defining poor functional recovery as a modified Rankin Score ≥3. The absence of prodromal headache, the presence of myoclonus, and the detection of cerebellar lesions on neuroimaging were associated with poor functional recovery, which was observed in 23% of the patients. Several previous studies suggested that age may impact acute disseminated encephalomyelitis outcomes, with adult patients having poorer motor recovery than children, and older children experiencing higher neurocognitive sequelae than younger ones.29,37 The study conducted by Baumann et al 38 revealed patients with anti-MOG antibodies had higher rates of complete recovery. Unlike those studies, and in line with the work of Anlar et al, 4 we found no association between the preceding symptoms, age of onset, lesion localization on MRI, or the presence of anti-MOG antibodies with recovery. We identified that incomplete recovery were associated with a Glasgow Coma Scale score <10 on admission, the need for an ICU and mechanical ventilation, and the presence of seizures on admission. However, the multivariate analysis revealed only 2 significant parameters: the presence of seizures on admission and the need for an ICU.
Seizures are one of the common symptoms of acute disseminated encephalomyelitis. Various studies have documented that 12% to 50% of children with acute disseminated encephalomyelitis experienced seizures during the acute period.4,6,10,11 This rate was 28.2% in our patients, with generalized seizures representing about half (55%). This finding differs from Tenembaum et al's study, 6 where focal motor seizures predominated. This may be due to our exclusion of the encephalitic form. Methodologic differences are likely to produce the wide range observed in the rate of post–acute disseminated encephalomyelitis epilepsy: 0% to 16%.4,6,10,11 In the present cohort, we defined post–acute disseminated encephalomyelitis epilepsy as unfavorable outcome (incomplete recovery). Chen et al 32 found no significant correlation between seizures in the acute period and poor functional recovery (based on modified Rankin Score ≥3). Post–acute disseminated encephalomyelitis epilepsy, was also reported as associated with positive oligoclonal band, anti-MOG positivity and more than 1 acute disseminated encephalomyelitis episode.7,11 However, we found no association between the rate of post–acute disseminated encephalomyelitis epilepsy and oligoclonal band, anti-MOG positivity, or relapsing course.
The relapse rates of acute disseminated encephalomyelitis varied greatly among research groups, ranging from 0% to 42%, the majority about 10%.4,6-11 Rossor et al, 11 in their series of 74 children with acute disseminated encephalomyelitis, observed that age at disease onset, gender, prodromal symptoms, cerebrospinal fluid findings (white blood cell count, protein level, oligoclonal band), or seizures at presentation had no effect on relapse risk; anti-MOG antibody positivity was the only significant predictor of relapse. Several other studies described higher relapse rates in anti-MOG–seropositive acute disseminated encephalomyelitis patients, spanning 21% to 54%, despite a better recovery.11,14-16,38,39 Wendel et al 17 indicated a relapse rate of 38% among their series of 116 pediatric MOG antibody–associated disease patients and a rate of 40% in those who initially presented as acute disseminated encephalomyelitis (n = 59). In our study, the overall cohort with at least 1-year follow-up had a relapse rate of 12.6%. Among all relapses, 56.5% occurred within the first year, 21.7% between months 13 and 24, 17.4% between months 25 and 48, and 4.3% beyond month 49. The anti-MOG antibody–positive group had a higher relapse rate of 35% during the same period. MOG antibody–associated disease patients exhibited a higher frequency of relapse than anti-MOG–negative individuals; nevertheless, the difference was not significant. We also identified a strong relation between female sex, ataxia at initial presentation, and visual impairment with a higher relapse rate. The rates of relapse may vary with the duration of the follow-up period. 39 Relapses in pediatric MOG antibody–associated disease patients typically occur within the first 12 months after the first episode; however, they have been reported as late as 10 years. 40 Therefore, our findings pertain only to the first year of follow-up.
The diagnosis changed to multiple sclerosis in 8 patients during the follow-up period. It is uncommon (less than 10%) for acute disseminated encephalomyelitis to be the initial symptom of multiple sclerosis or neuromyelitis optica spectrum disorder. 9 The observation of 2 of 3 factors may help to distinguish acute disseminated encephalomyelitis from multiple sclerosis and support the diagnosis of multiple sclerosis at the initial attack: (1) the presence of black holes, (2) the presence of 2 or more periventricular lesions, and (3) the absence of a bilateral lesion pattern. However, these criteria are not solely sufficient for a definitive diagnosis. 9 Among our 8 patients diagnosed with multiple sclerosis, 6 had periventricular lesions, 2 presented lesions in the corpus callosum, and none demonstrated black holes.
Our study has several limitations, mainly introduced by its retrospective and multicenter nature. As a result, anti-MOG antibodies could not be tested in all individuals but in 36.3% of the cohort. Second, the evaluation of long-term outcomes was limited to clinical parameters (relapse rate, modified Rankin Score, and post–acute disseminated encephalomyelitis epilepsy). We did not have a standardized cognitive assessment in all patients. Finally, because of the multicenter design of the study, there may be variations in patient approach, including first- and second-line treatments, maintenance therapy, antiseizure medication protocols, ICU admission criteria, and duration of the ICU stay. Despite these limitations, this exclusively pediatric series involving a large number of patients provides early and long-term outcomes with respect to the subgroups of anti-MOG antibody positivity and negativity.
In conclusion, the presented nationwide cohort study reveals the clinical landscape of acute disseminated encephalomyelitis in the anti-MOG antibody era, its predominantly monophasic nature, and the overall favorable outcome regardless of the anti-MOG antibody status. The presence of seizures and the need for ICU on admission, indicative of clinical severity, emerged as the most significant prognostic variables. These factors should be tested in the well-designed prospective longitudinal follow-up studies, possibly resulting in modifications of management protocols and guidelines. As the clinical course is heterogeneous and no large, randomized controlled trials or treatment guidelines exist in pediatric acute disseminated encephalomyelitis, identifying the indicators at admission that confer a high risk of unfavorable outcomes may help to provide a patient-based approach to management.
Footnotes
Author Contributions
SK, SY, DET, HT, BA conceptualized the study and reviewed and interpreted the results and revised the manuscript at all stages. SK, DET wrote the first manuscript. NOD, AA, MC, HP, İE, HG, YÖ, SÖ, İÖ, MÖ, ENM, HMS, GE, ŞB, GGM, AG, SŞ, CBÖ, AS, SP, GB, ÇG, DB, ZFK, DY, MK, EŞ, AÜ, NY, MÇD, UY, HT, CH, AD, MG, ÖH, EPÖ, OÜ, SK, HAÇ, BÖ, AC, AKA, AT, OG, ÇO, SE, SH, ES, HK, CDY, GOT, PG, UY, SÖ organized and analyzed the data and revised the manuscript. SY, HT, BA approved the final manuscript. All authors contributed to the critique and review of the final draft of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.