
Abstract
This study aimed to evaluate the impact of a triage-based blunt trauma assessment (best practice advisory) on Pediatric Emergency Care Applied Research Network (PECARN)-guided recommendations and actual head computed tomography (CT) use in children <18 years old presenting with head injury. We examined agreement between best practice advisory recommendations, PECARN risk categories, and head CT use, as well as risk factors associated with deviation from PECARN guidance. Group comparisons were analyzed by Mann-Whitney rank-sum test, Kruskal-Wallis test, Fisher exact test, or χ2 test, as indicated. Best practice advisory and PECARN agreement was 47%. The best practice advisory aligned with CT use in 39% of cases, whereas PECARN aligned 73%. In children <2 years, 42% received a head CT despite a PECARN recommendation against it (P < .001). In children ≥2 years, 38% received a head CT against PECARN recommendations (P < .001). Overall agreement among best practice advisory, PECARN, and head CT use was 35%. Symptoms such as speech changes, lethargy, altered mood, and gait abnormalities were associated with deviations from PECARN. Findings suggest that although PECARN guides imaging decisions, numerous clinical factors and best practice advisory recommendations influence provider behavior, highlighting opportunities to improve decision support and reduce unnecessary CT scans.
Keywords
The diagnostic standard for the evaluation of pediatric head injury and concerning signs of clinically important traumatic brain injury or severe traumatic brain injury (TBI) is a head computed tomography (CT) scan.1,2 Prediction tools have been developed to aid in the clinical decision of safely ruling out the presence of clinically important traumatic brain injury,1,2 including those that require neurosurgical intervention among pediatric head injuries without the need for CT imaging.3,4 Literature suggests less than 1% of children with mild traumatic brain injury require acute neurosurgical intervention5–8; however, approximately a third of these patients receive neuroimaging. 9
The Pediatric Emergency Care Applied Research Network (PECARN) developed a prediction rule to identify pediatric patients with a clinically important traumatic brain injury and, in turn, decrease the number of unnecessary head CTs in children with mild traumatic brain injury.3,10 This tool has shown high sensitivity in predicting positive CT results, making it effective at identifying patients at risk for significant injuries and superior to similar clinical decision rules.11–15 The PECARN head injury prediction rule is widely used, reliable, 16 extensively validated, 17 and implemented via computerized decision support in hospitals’ electronic medical record systems. 5 Despite the knowledge of the PECARN prediction rule and its implementation, head CTs in pediatric patients with mild traumatic brain injury remain high. 18 Furthermore, the factors related to the deviation from decision-making tools, like the PECARN prediction rule and computerized decision support recommendations in favor of performing neuroimaging in pediatric patients with head injuries in the emergency department are limited. Therefore, the study aimed to describe the best practice advisory recommendations on neuroimaging use, correlate these recommendations with the PECARN prediction rule, and examine the correlation between PECARN recommendations, neuroimaging practice, and the findings from these practices.
Materials and Methods
Study Design and Setting
This was a retrospective electronic medical record review of pediatric patients who visited the emergency department of a university-affiliated, free-standing pediatric hospital. This study was approved by the institutional review board. The reporting of this study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline.
Participants
We included children aged 0 months to younger than 18 years who visited the emergency department with a chief complaint of head injury from January 1, 2019, to December 31, 2019. We excluded patients with a previous head injury, history of medical complexity, evaluation for nonaccidental trauma, motor vehicle accident, and history of bleeding or bone disorders. Medical complexity, identified by the 3M Clinical Risk Group Software within our electronic medical record, was clinically defined as children with 1 or more chronic health conditions that lead to significant morbidity and mortality, impacts daily activities, requires high health care use including 3 or more specialties, and necessitates dependence on technology. 19
Study Variables
Collected data included demographic characteristics, emergency department visit characteristics, chief symptom, emergency severity index (ESI), best practice advisory documentation, mechanism of injury, symptomatology, physical findings, time lapse since head injury, radiologic order, time of neuroimaging order, neuroimaging result, medications administered in the emergency department, final diagnosis, disposition, and emergency department length of stay.
Data Measurements
We used the PECARN Pediatric Head Injury Prediction Rule as a control to measure the appropriateness of neuroimaging based on the patient's age, history, and physical findings. 3 The PECARN algorithm's objective is to minimize unnecessary CT scans while identifying children at significant risk for clinically important traumatic brain injury, defined as traumatic brain injuries requiring acute interventions, including neurosurgery or hospitalization, for ongoing symptoms or signs of traumatic brain injury. The PECARN algorithm is stratified by age (ie, children under 2 years of age and children aged 2 years and older) and high-risk, intermediate-risk, and low-risk indicators. The ESI ranks acuity from 1 (most severe) to 5 (least severe). 20 A head CT was deemed abnormal if it described the presence of a skull fracture, scalp or brain contusion, intracranial bleeding, cerebral edema, or nonspecific findings that could not exclude traumatic brain injury presence. We used the World Health Organization's (WHO) Collaborating Centre Task Force's definition for the presence of traumatic brain injury on neuroimaging as any of the following: intracranial hemorrhage or contusion, cerebral edema, traumatic infarction, diffuse axonal injury, shearing injury, sigmoid sinus thrombosis, midline shift of intracranial contents or signs of brain herniation, diastasis of the skull, pneumocephalus, or skull fracture depressed by at least the width of the table of the skull.3,21 We used a Blunt Head Trauma Assessment completed by a triage nurse to generate a best practice advisory for the emergency department medical provider (Supplementary Table 1). Although the best practice advisory is institution-specific, it incorporates PECARN criteria and established clinical guidelines to reduce unnecessary radiation exposure and associated risks. 10 Although found to be valid and reliable within our institution, this computerized decision support tool has not been independently externally validated. A best practice advisory is a computerized decision support tool embedded in the electronic medical record to evaluate neuroimaging recommendations. The best practice advisory is a pop-up alert designed to remind and guide clinical decision making. 22
We created categories to evaluate the agreement between best practice advisory recommendation, PECARN prediction rule, and head CT provider practice. Best practice advisory recommendations were split into 4 categories: CT not recommended, observation vs CT, CT recommended, and best practice advisory did not populate on emergency department chart opening. The PECARN recommendation was split into 3 categories: CT recommended, CT not recommended, and observation recommended among children <2 years and ≥2 years of age. A medical provider's head CT practice was separated into 2 categories: head CT ordered, or no head CT ordered. Agreement among best practice advisory, PECARN, and head CT was determined by the concordance between the recommendation and occurrence of neuroimaging (ie, CT is not recommended with no CT performed, CT is recommended with CT performed). Missing data were addressed by analyzing only those cases with complete documentation for the best practice advisory and PECARN variables (Figure 1). Analyses that correlated best practice advisory recommendations with PECARN or head CT use were conducted using only patients with complete best practice advisory documentation. Subgroup analyses were performed to evaluate patient outcomes among children with best practice advisory and those without it. PECARN variables were available for all included patients, allowing complete calculation of the PECARN risk categories.
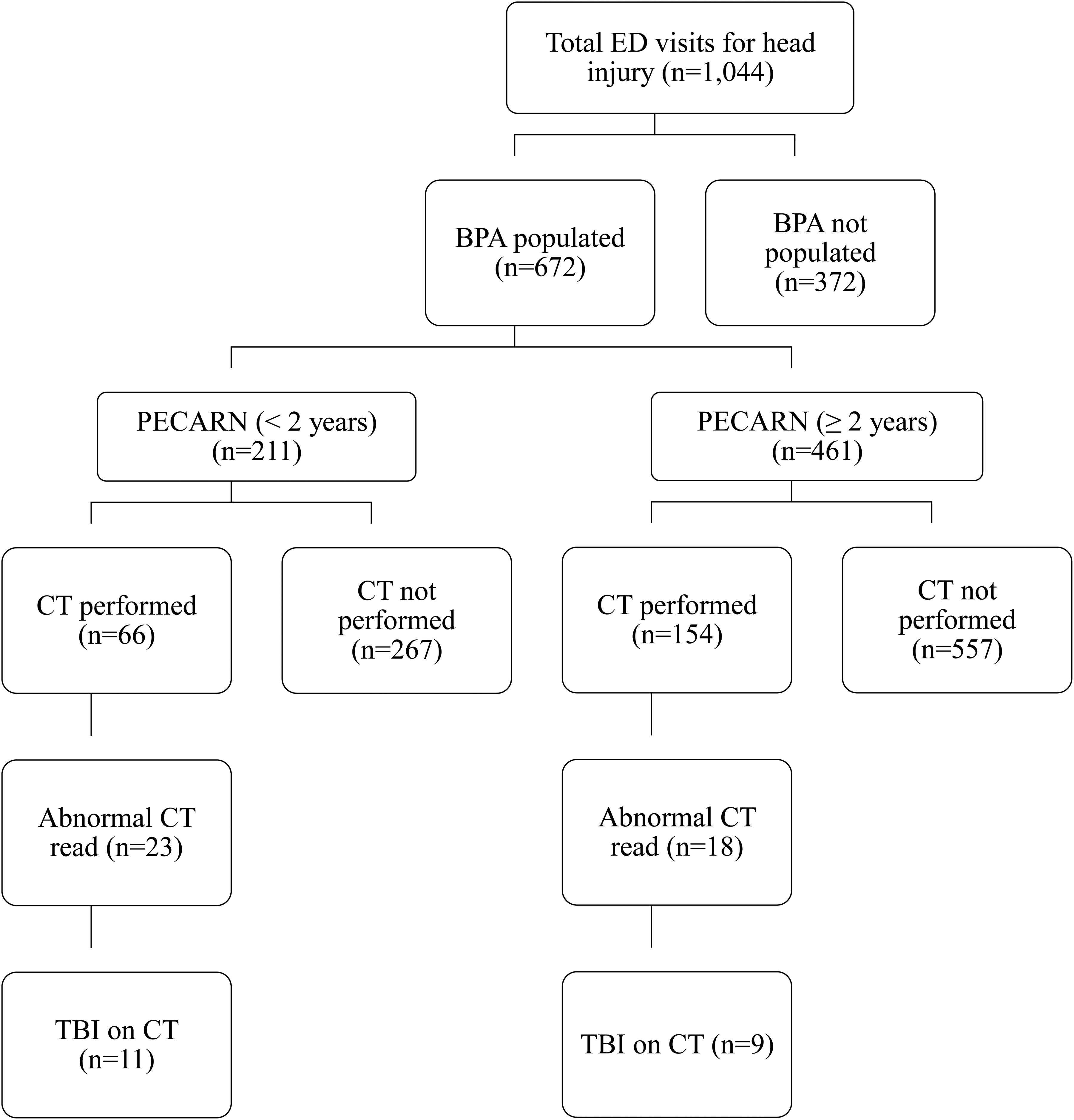
Flow of study population by BPA availability, PECARN pathway, neuroimaging use, and outcomes. BPA, best practice advisory; CT, computed tomography; ED, emergency department; PECARN, Pediatric Emergency Care Applied Research Network head injury prediction rule; TBI, traumatic brain injury.
Outcome Measures
The primary outcome measures were (1) the percentage of agreement between best practice advisory–based and PECARN-based recommendations on neuroimaging use, (2) the percentage of agreement between PECARN and best practice advisory recommendations and clinical practice in ordering neuroimaging, and (3) the prevalence of abnormal neuroimaging findings in patients with and without best practice advisory and PECARN recommendations. Secondary outcomes of interest included the prevalence of concussion symptomatology, date and time of emergency department visit, and emergency department length of stay.
Statistical Analysis
We used descriptive analysis, including frequency of distribution and measures of association. Counts and percentages analyzed categorical variables, and continuous variables were analyzed as median and interquartile ranges (IQR [Q1-Q3]). Comparisons between groups (best practice advisory, PECARN, and head CT practice) were performed using the Mann-Whitney rank-sum test and Kruskal-Wallis test for continuous variables. Categorical variables were compared between groups using Fisher exact test or χ2 test. A logistic regression analysis was performed to identify predictive variables of PECARN deviation. Only significant variables in the univariate analysis were included in the multivariate logistic regression model. All statistical analyses were conducted in IBM SPSS Statistics 27 (IBM Corp, Armonk, NY). All tests were 2-sided, with a P value <.05 considered statistically significant.
Results
Of the 1044 children included, the median age was 4.25 years (IQR 1.5-9.1), with a predominance of males (60%) (Table 1). Neuroimaging was performed in 220 patients (21.1%). Children who underwent neuroimaging were more often evaluated by physicians (80.7% vs 46.0%, P < .001), presented with higher emergency severity indices (ESI 2-3: 61.8% vs 18.5%, P < .001), and were more likely to sustain a fall >3 feet (16.1% vs 5.1%, P < .001). Admission rates were significantly higher among imaged patients (7.8% vs 0.1%, P < .001).
Demographic Characteristics of the Population Under Study (N = 1044).
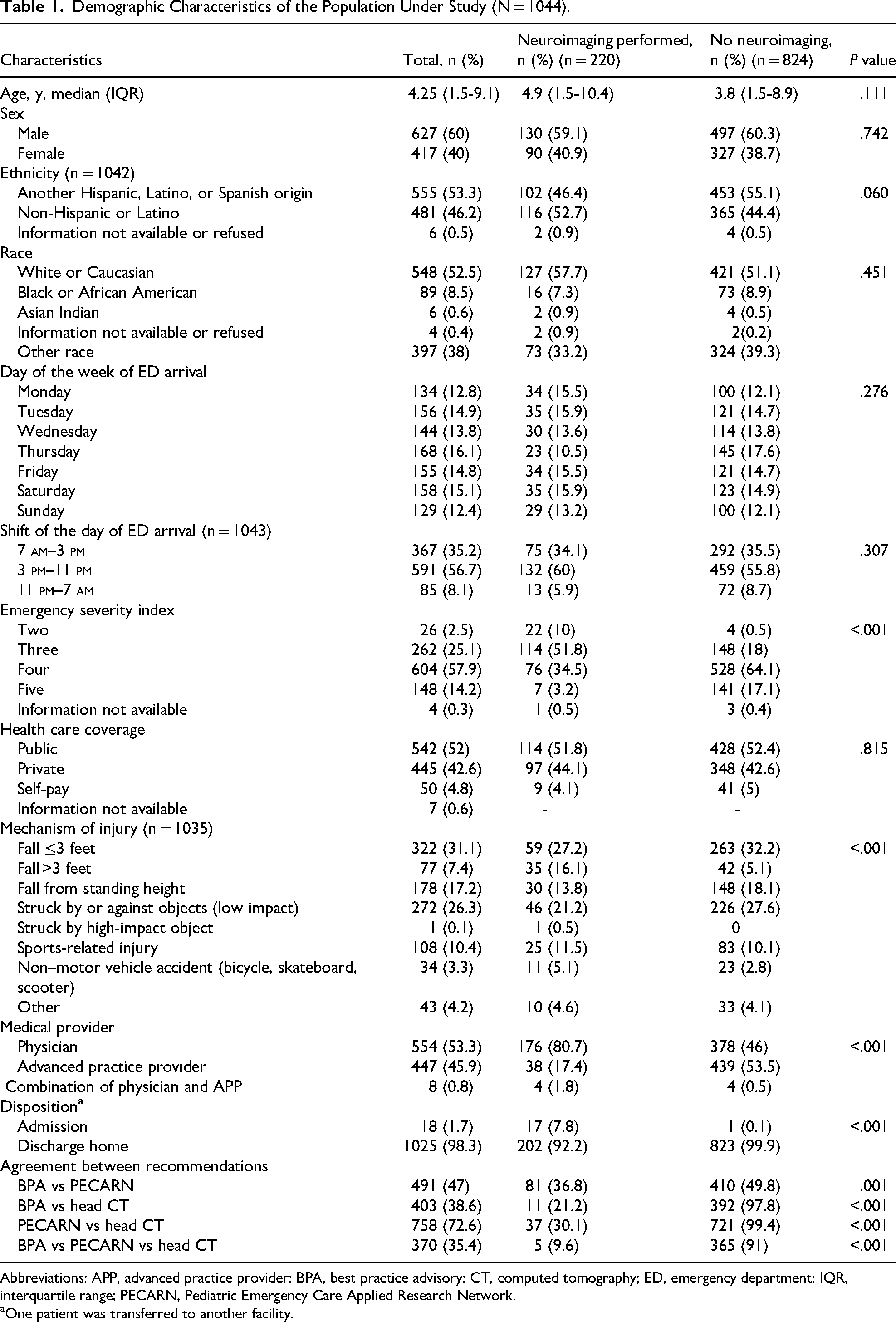
Abbreviations: APP, advanced practice provider; BPA, best practice advisory; CT, computed tomography; ED, emergency department; IQR, interquartile range; PECARN, Pediatric Emergency Care Applied Research Network.
One patient was transferred to another facility.
More than one-third (35.6%) of patients did not have best practice advisory recommendations populated.
Among children aged <2 years, CT use in situations where no CT was recommended was modestly higher without a best practice advisory (7.4%, P < .001) compared with a best practice advisory (6.5%, P = .034). In high-risk cases where CT was recommended, CT use was 100% regardless of best practice advisory presence (P < .001). In the intermediate-risk (observation vs imaging) group, providers without a best practice advisory obtained CTs more frequently (65%, P < .001) compared to those with best practice advisory (41.2%, P = .406). Similarly, in children ≥2 years, CT use when no CT was recommended was higher in the absence of a best practice advisory (9.9%, P < .001) compared to those with best practice advisory (7%, P < .001), whereas CT was obtained in nearly all cases when recommended (81.8%, P < .001) compared to those with best practice advisory (100%, P = .077). In the intermediate group among children ≥2 years, CT use was nearly identical whether best practice advisory for observation vs imaging was supported (54.8%, P < .001) or not (54.5%, P = .006).
Analyses of best practice advisory performance were therefore restricted to patients with complete best practice advisory data. Sensitivity analyses confirmed that exclusion of patients with missing best practice advisory data did not significantly alter results. Agreement between best practice advisory, PECARN, and CT practice was significantly lower among children who were imaged compared with those not imaged (9.6% vs 91.0%, P < .001).
There was a strong relationship between the best practice advisory recommendations and head CT use (P < .001), abnormal CT findings (P = .027), and traumatic brain injury on CT (P = .014) (Table 2). However, nearly one-third (29.3%) of children who underwent CT had a best practice advisory recommendation against imaging. Within this group, 17.1% had abnormal findings and 4.9% were diagnosed with traumatic brain injury. Conversely, the “observation over imaging” category had the highest frequency of CTs performed (62.9%) but yielded the lowest proportion of abnormal CTs (5.7%) and traumatic brain injuries (1.1%). Overall agreement between best practice advisory recommendations and CT practice was 38.6%, primarily reflecting alignment in avoiding imaging (37.5%).
Correlation Between BPA and Neuroimaging Practice.
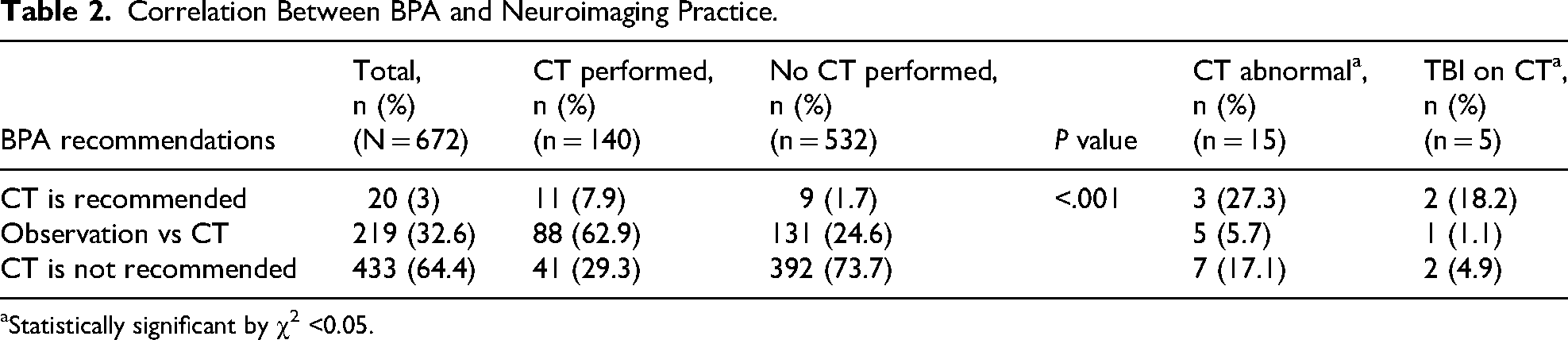
Statistically significant by χ2 <0.05.
Age-stratified analyses revealed differences in concordance between PECARN, best practice advisory, and CT practice (Tables 3 and 4). In children <2 years, concordance between best practice advisory and PECARN was low (12.1%), and agreement between PECARN and CT practice was only 23.3%. In contrast, among children ≥2 years, agreement improved (best practice advisory vs PECARN: 35%; PECARN vs CT: 49.4%). Across all ages, PECARN recommendations demonstrated the strongest alignment with CT practice (72.6%). Notably, 42.4% of children <2 years and 37.7% of those ≥2 years who received a CT had a PECARN recommendation against imaging (P < .001).
Association Between the Best Practice Advisory and the PECARN Pediatric Head Injury Prediction Rule.
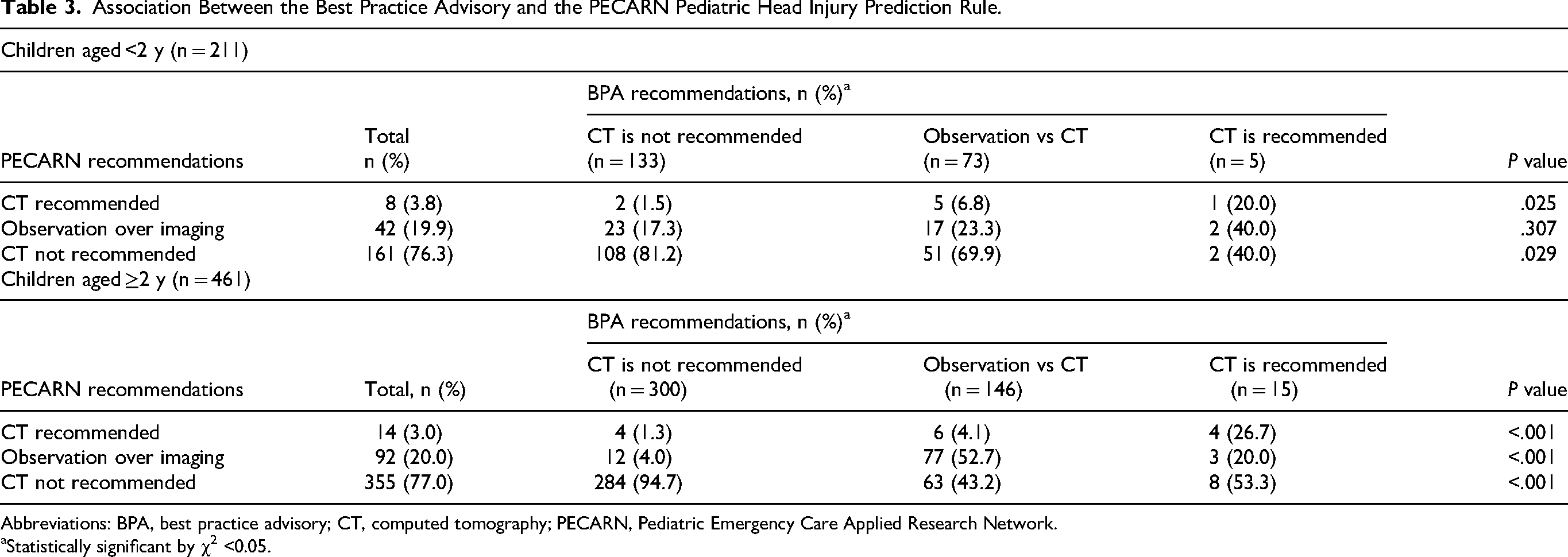
Abbreviations: BPA, best practice advisory; CT, computed tomography; PECARN, Pediatric Emergency Care Applied Research Network.
Statistically significant by χ2 <0.05.
Association Between PECARN Pediatric Head Injury Prediction Rule, Neuroimaging Practice, and Findings.
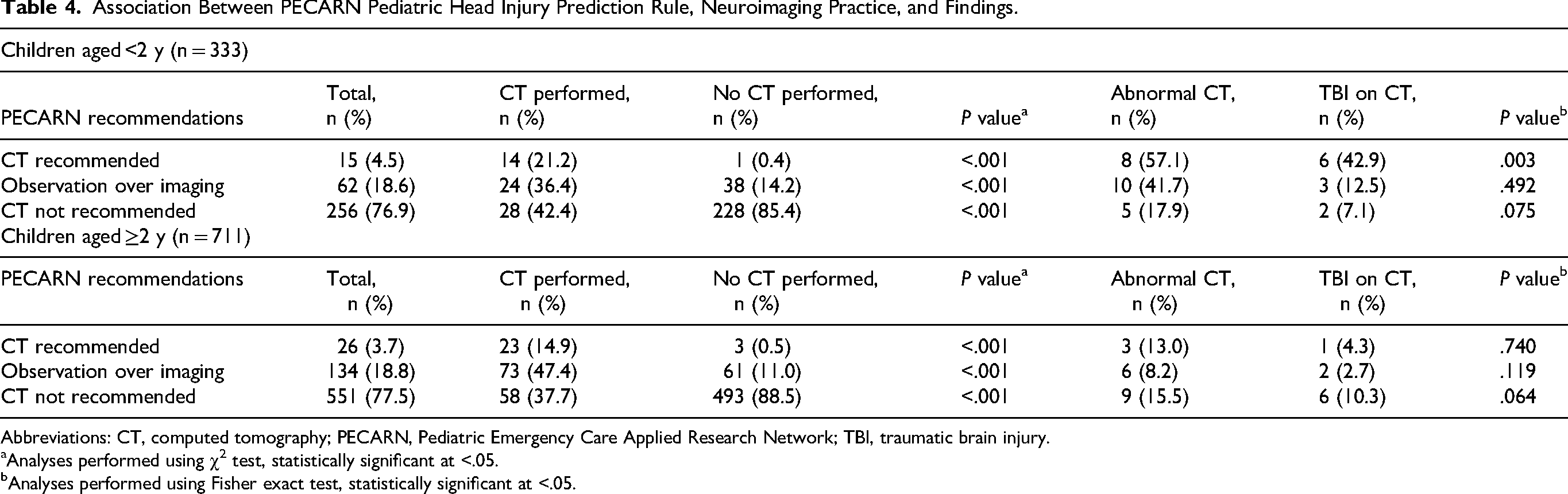
Abbreviations: CT, computed tomography; PECARN, Pediatric Emergency Care Applied Research Network; TBI, traumatic brain injury.
Analyses performed using χ2 test, statistically significant at <.05.
Analyses performed using Fisher exact test, statistically significant at <.05.
Multivariate regression identified several independent risk factors associated with CT use, regardless of best practice advisory or PECARN recommendations, including dizziness (odds ratio [OR] 1.6, 95% confidence interval [CI] 1.1-2.3), confusion (OR 2.6, 95% CI 1.8-3.7), nausea (OR 2.6, 95% CI 2.0-3.4), speech changes (OR 4.0, 95% CI 3.5-4.7), lethargy (OR 2.3, 95% CI 2.2-4.7), altered mood or behavior (OR 2.9, 95% CI 2.1-4.3), and gait abnormality (OR 2.9, 95% CI 1.9-4.4). CT use was not associated with the time of emergency department arrival, day of the week, race, ethnicity, or insurance coverage.
Most patients were discharged home (98.3%), with a 19.7% CT rate among this group (P < .001). Twenty children had traumatic brain injury findings of CT, 90% of which were clinically important traumatic brain injury requiring hospitalization, though none required neurosurgical intervention (P < .001). Admission rates for traumatic brain injury differed by age, with 45.5% in children <2 years vs 55.6% in those ≥2 years (P < .001). The median emergency department length of stay was 114 minutes (IQR 77-161), and 1.6% returned to the emergency department within 30 days for persistent or recurrent symptoms.
Discussion
The head CT rate for children with minor blunt head trauma in emergency departments across the United States ranges from 10% to 40%,3,5,9,23–26 with lower rates typically observed in emergency departments that have adopted computerized decision support tools such as the best practice advisory. In our cohort, 1 of every 5 children (20%) presenting with head injury underwent CT imaging, a rate consistent with national trends. These findings provide important new insight into how computerized decision support influences neuroimaging decision making in children, highlighting both concordance and discordance between electronic decision support and clinical practice.
Although prior studies have established the validity of the PECARN clinical decision rules in safely reducing unnecessary CT use without compromising detection of clinically important traumatic brain injury, much less is known about how real-time electronic best practice advisories shape practice. At our institution, best practice advisory recommendations are generated at triage, entered primarily by nursing staff, and serve as real-time, evidence-based reminders within the clinical workflow.27,28 However, more than one-third of patients did not have best practice advisory recommendations populated, likely due to incomplete triage documentation or technical integration problems, limiting the tool's reach. Subgroup analysis of these encounters provided valuable insights into provider behavior in the absence of computerized decision support. In high-risk cases, CT use was uniformly high regardless of best practice advisory presence, and in low-risk cases, rates remained low. The greatest variability occurred in the intermediate-risk (observation vs imaging) category.5,29 Providers were more likely to obtain CT scans in the absence of a best practice advisory compared to when the best practice advisory was present, suggesting that computerized decision support may have its greatest utility in situations of diagnostic uncertainty by helping to reduce unnecessary imaging when observation is a reasonable alternative. This pattern is consistent with prior evidence that computerized decision support reduces variability and promotes adherence to guidelines, particularly in ambiguous cases. Savioli et al 30 and Abreu et al 31 emphasized the value of structured pathways in curbing discretionary imaging and improving diagnostic consistency, whereas Rivero et al 32 demonstrated how electronic alerts reduced unnecessary interventions in pediatric surgical decision making. Similarly, Lesyk et al 33 showed in a systematic review that computerized decision support interventions exert their greatest influence in intermediate-risk or “gray zone” populations, reinforcing our findings.
Our age-stratified analysis adds further nuance. In children <2 years, concordance between best practice advisory and PECARN was lowest, with nearly half of CTs performed in cases where PECARN recommended against imaging. This reflects the inherent diagnostic challenges in infants and toddlers, where symptoms are subtle and PECARN criteria are deliberately conservative.4,7 In contrast, ≥2 years showed better alignment between PECARN and clinical practice, although more than one-third still underwent CT despite “no CT” recommendations. These results reinforce prior observations that providers apply prediction rules with greater confidence in older children, while remaining more cautious in infants and toddlers due to diagnostic uncertainty.
Notably, even when best practice advisory guidance was available, nearly one-third of children with a “no CT” recommendation still underwent imaging. This underscores the persistent influence of provider discretion, parental expectations, and risk tolerance.18,25 Importantly, clinically important traumatic brain injury was detected across all best practice advisory categories, illustrating the difficulty of balancing structured computerized decision support recommendations with individualized patient care.5,18,29
Consistent with prior work, younger age and low-impact mechanisms were less likely to result in CT use, whereas higher-risk mechanisms, such as falls from greater than 3 feet, were strongly associated with imaging.3,34 Despite these patterns, overall alignment between best practice advisory, PECARN, and CT practice was modest, with only 35% of cases showing agreement across all three. PECARN recommendations showed the strongest correlation with practice, consistent with its prior validation studies across diverse populations.3,11,16 Yet, adherence to PECARN remains variable, particularly outside pediatric specialty centers and during interfacility transfers. 8
Our study makes several novel contributions. First, it directly evaluates how an embedded electronic medical record-based best practice advisory influences actual imaging practice in a large, real-world cohort, providing a more detailed picture of concordance and discordance than prior PECARN validation studies. Second, it quantifies provider behavior in the “observation vs imaging” group, the area of greatest practice variability and the most clinically ambiguous category. Third, it demonstrates age-dependent differences in best practice advisory impact, confirming that infants and toddlers are more likely to undergo CT despite “no CT” recommendations. Together, these findings bridge an important gap between prediction rule validation and implementation science by showing how computerized decision support functions in everyday practice, beyond controlled research settings.
Several factors may explain the discordance between best practice advisory recommendations and provider practice. Concerns about missed or delayed intracranial hemorrhage, 35 parental pressure, and the realities of busy emergency department workflows likely contribute to persistent imaging. 18 Additionally, because best practice advisory recommendations depend on accurate triage data, any omissions or errors may lead to misaligned outputs. The division of responsibility is also relevant: whereas nurses populate best practice advisories at triage, final imaging decisions rest with physicians, who may place greater weight on PECARN criteria or their own judgment. Provider-level differences, such as greater likelihood of ordering CT by physicians compared with advanced practice providers, further underscore the need for tailored computerized decision support strategies.
The clinical implications are substantial. Overimaging exposes children to radiation and long-term malignancy risk,1,36 whereas practice variation across institutions reflects inconsistent adoption of validated rules.9,37 Prior work has shown that observation, when applied appropriately, safely reduces CT rates without increasing missed clinically important traumatic brain injury. Interventions such as provider education, 25 structured parent discussion tools, 27 and embedding PECARN into physician workflows28,29 may strengthen adherence. Ultimately, computerized decision support tools like best practice advisories are valuable, but insufficient as stand-alone interventions to change practice.26,38 A multimodal approach by combining computerized decision support with provider education, parental engagement, real-time feedback, and shared decision making, will likely be required to optimize imaging decisions, reduce unnecessary CTs, and improve patient safety.8,38–40
Limitations
This study has several limitations. First, it was conducted at a single institution, which may limit the generalizability to settings with different patient populations, provider training, or institutional cultures surrounding CT use. Moreover, our institution is not a designated trauma center, which may have limited capture of the most severe head injuries. However, because most blunt head injuries present to community hospitals, our study population is reflective of real-world practice and therefore highly relevant. Second, although the best practice advisory was designed to align with PECARN recommendations, our retrospective electronic medical record-based analysis was unable to capture the nuances of clinical reasoning, shared decision making, or contextual influences such as parental preferences or comorbidities. Third, best practice advisory recommendations depend on accurate data entry at triage; missing or misclassified data could have influenced both best practice advisory outputs and subsequent analyses. Fourth, although we observed a strong association between best practice advisory recommendations and CT use, this does not establish causality. Providers may have independently reached decisions consistent with best practice advisory guidance, and the tool may have functioned more as reinforcement than as the primary driver. Fifth, the relatively small number of abnormal CTs and traumatic brain injuries limited our ability to assess diagnostic yield across best practice advisory categories. Larger multicenter studies are needed to confirm the safety of best practice advisory adherence vs nonadherence. Sixth, we were unable to evaluate provider-level factors, such as years of experience, familiarity with PECARN, or personal risk tolerance, all of which may shape influence both responsiveness to best practice advisories and imaging decisions. System-level influences such as emergency department crowding, access to observation units, and availability of resources such as rapid magnetic resonance imaging were also not captured but could have influenced imaging practices. Lastly, alert fatigue remains a potential limitation, as we did not measure how often best practice advisories were dismissed or ignored, nor how provider attitudes toward best practice advisories evolved over time. A key strength of this study is its real-world design, leveraging a clinical decision tool already embedded in our electronic medical record and modeled after PECARN recommendations. Finally, our study fills a gap in the literature by comparing best practice advisory–based decision support with PECARN guidelines and actual CT practice, providing new insights into computerized decision support effectiveness in community-based pediatric emergency care.
Conclusions
Prediction models such as PECARN and best practice advisory–based computerized decision support tools can help curb the overuse of neuroimaging in children with blunt head trauma. However, discrepancies remain between model recommendations and real-world practice. Numerous clinical symptoms and physical findings were associated with CT use even when PECARN recommended against imaging, and strict application of computerized decision support would have missed some traumatic brain injuries. These findings highlight the persistent tension between guidelines-driven care and individualized clinical judgment. Future efforts should focus on enhancing provider education, integrating PECARN into physician workflows (not only triage), improving parent-clinician communication about the risks of CT and the safety of observation, and refining computerized decision support algorithms to better reflect nuanced decision making. Feedback mechanisms and continuous quality improvement strategies will also be essential. By addressing these barriers, health care systems can enhance adherence to validated decision pathways, minimize unnecessary imaging, and ensure patient safety during the evaluation of pediatric head injuries.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738251378937 - Supplemental material for Impact of a Triage-Based Blunt Trauma Assessment on PECARN Recommendations and Neuroimaging Use in Pediatric Head Injury
Supplemental material, sj-docx-1-jcn-10.1177_08830738251378937 for Impact of a Triage-Based Blunt Trauma Assessment on PECARN Recommendations and Neuroimaging Use in Pediatric Head Injury by Cheuk Kwok, Jamie Marliere, Shaye Busse, April Taniguchi, Kamal Chavda and Andrea Rivera-Sepulveda in Journal of Child Neurology
Footnotes
Ethical Approval
This study was approved by the Institutional Review Board (IRB).
Author Contributions
AR conceptualized the study, designed the data collection instrument, analyzed and interpreted the data, and drafted and critically revised the manuscript. CK and JM conceptualized the study, acquired the data, interpreted the data and drafted and critically revised the manuscript. SB and AT acquired the data and assisted in the interpretation of the data, and critically revised the manuscript. KC conceptualized the study, interpreted the data and critically revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Funding
This publication was supported by the (AHRQ-PCORI funded) PEDSnet Scholars Training Program (5K12HS026393-03), which is a national faculty development program that trains individuals in the competencies of learning health systems science.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.