
Abstract
We examined associations between magnetic resonance imaging (MRI)–obtained cervical spine flexor and extensor muscle fat infiltrate and muscle volume with (1) return-to-play clearance and (2) postconcussion injury incidence. Adolescents (N = 30, age = 15.8 ± 1.3 years, 60% female) underwent cervical spine MRI initially postconcussion and were monitored until return to play. After return-to-play clearance, participants underwent follow-up MRI and completed monthly injury surveys for 12 months. Cox proportional hazards regression examined associations between muscle fat infiltrate and muscle volume (1) initially postconcussion with return-to-play clearance and (2) at return-to-play with subsequent injury incidence. Adjusting for covariates, return-to-play clearance was not associated with cervical spine muscle fat infiltrate (hazard ratio [HR] = 0.99, 95% confidence interval [CI]: 0.96-1.02) or muscle volume (HR = 0.98; 95% CI: 0.96-1.01). Adjusting for covariates, postconcussion injuries were not associated with muscle fat infiltrate (HR = 0.90; 95% CI: 0.78-1.05) or muscle volume (HR = 1.01; 95% CI: 0.97-1.04). Cervical spine muscle characteristics may not be affected after concussion, or our MRIs may have occurred too early to capture postconcussion dysfunction.
Introduction
After sport-related concussion, immediate removal from competition and evaluation by a health care professional is recommended to avoid further injury.1,2 In most cases, athletes with a concussion experience a resolution of symptoms and return to sports participation within 4 weeks of injury. 2 Unfortunately, once athletes receive clearance to return to play, they appear to be predisposed to increased risk of sustaining subsequent injuries in future sports participation. 3 Meta-analyses suggest that athletes with concussion have more than twice the risk of sustaining a subsequent sports-related injury (both musculoskeletal injuries and concussions) after return to play compared to athletes without a recent sport-related concussion.4,5 However, few objective measures (eg, biomarker or imaging approaches) exist to inform clinical recovery timelines or identify individuals at risk of subsequent injuries, 2 posing a challenge for health care providers assessing and managing patients at risk of adverse outcomes in the short or long term. In the absence of an agreed upon objective marker of clinical recovery, a multimodal assessment is recommended to determine concussion recovery and facilitate decisions regarding return to sports participation after concussion.2,6 Investigating whether imaging characteristics are associated with return-to-play clearance time and subsequent injury risk may inform assessment, treatment, and ultimately return-to-play decisions after concussion.
The forces acting on the head, neck, and body that cause concussion may also cause concomitant cervical spine injuries such as whiplash.7,8 The injuries underlying concussions and whiplash share mechanics and often similar symptom profiles including headache, neck pain, dizziness, and fatigue, 7 and functional deficits including cervical spine proprioception impairments. 9 The overlap between injury mechanisms, symptoms, and functional deficits makes it difficult to differentiate between the injuries,7,10,11 presenting a unique challenge for guiding treatment. After whiplash, cervical spine muscle characteristics obtained via magnetic resonance imaging (MRI) have been observed shortly after the traumatic event with changes persisting in individuals with prolonged symptom duration,12–16 which may also be useful in informing the clinical course of concussion. Specifically, individuals who experience persistent symptoms after whiplash have been observed to have higher levels of deep cervical spine muscle fat infiltrate and greater cervical spine multifidus muscle volume (including the muscle fat infiltrate component) compared with those who no longer experience symptoms at 1 year postinjury.12–16 Given the overlap between injury mechanisms, symptoms, and functional deficits, it is possible that similar muscle characteristic changes exist after concussion and may identify individuals at risk for poor recovery outcomes, although this has yet to be investigated after concussion.
Although the mechanisms for how the observed deep cervical spine muscle changes negatively influence whiplash recovery are not fully understood, several theories exist. For example, muscle fat infiltrate in the cervical spine muscles could be a result of an inflammatory process (ie, increased expression of pro-inflammatory cytokines), muscle disuse or denervation, changes in sympathetic nervous system activation, and/or general inactivity post-injury. 13 Elevated muscle fat infiltrate may, in turn, result in larger cervical spine muscle volume among individuals with persistent whiplash symptoms compared with those no longer experiencing symptoms, potentially resulting in negative consequences for muscle function. 15 More muscle fat infiltrate in the cervical spine multifidus is associated with postural instability among individuals with other cervical spine pathologies (ie, cervical spondylotic radiculopathy). 17
Although not yet studied, it is possible that similar changes in cervical spine muscle characteristics exist after concussion given the similar biomechanical injury mechanisms. It is therefore possible that concomitant cervical spine injuries could lead to similar cervical spine muscle changes after concussion as observed after whiplash. These changes may contribute to functional deficits such as postural instability commonly observed after whiplash and concussion,18–20 and may ultimately predispose individuals to subsequent injuries, as has been observed among athletes upon concussion return to play.4,5 It is also possible that cervical spine muscle characteristics (ie, muscle fat infiltrate and muscle volume) may predispose individuals to sustaining a concussion. Investigating cervical spine muscle characteristics (ie, muscle fat infiltrate and muscle volume) after concussion represents a novel and innovative method to identify a potential factor underlying the development of prolonged return-to-play time and subsequent injury risk after concussion. Importantly, a 10-week cervical spine strengthening program for individuals experiencing persistent symptoms after whiplash was observed to reduce muscle fat infiltrate in the cervical spine multifidus muscles. 21 Thus, in addition to representing a potential mechanism of poor concussion outcomes, cervical spine muscle characteristics may also present a potential therapeutic target.
Given the similar biomechanical mechanisms and symptom profiles between concussion and whiplash injuries,7,8 it is possible that similar muscle morphometry characteristics exist after concussion and may be associated with recovery outcomes including return-to-play clearance time and subsequent injury risk. Therefore, our primary objective was to investigate whether deep cervical spine flexor and extensor muscle fat infiltrate or muscle volume were associated with return-to-play clearance time after sport-related concussion. Our secondary objective was to investigate whether deep cervical spine flexor and extensor muscle fat infiltrate or muscle volume were associated with postconcussion injury risk (ie, subsequent concussions and musculoskeletal injuries) in the year after return to play after concussion. We hypothesized that higher muscle fat infiltrate levels and larger overall muscle volume (including the muscle fat infiltrate) would be associated with longer return-to-play clearance time and increased risk of subsequent injury after concussion return to play.
Materials and Methods
Participants and Study Design
We recruited and enrolled adolescent athletes participating in organized sports (ie, with a coach and structured practices and competitions) for this prospective, longitudinal study between February 2021 and April 2024. Study inclusion criteria consisted of being 13-18 years of age, diagnosed with a concussion by a sports medicine physician or athletic trainer, undergoing initial study assessment within 3 weeks of sustaining a concussion, planning to return to sports once cleared by their physician, and having concussion symptoms on enrollment defined as scoring ≥9 points on the Post-Concussion Symptom Inventory. 22 Exclusion criteria were sustaining a concussion via a high-velocity mechanism such as a motor vehicle collision and findings of a structural brain injury on neuroimaging if performed as part of routine care for concussion evaluation. Participants and guardians provided written informed assent/consent. Before study commencement, the local institutional review board reviewed and approved the study protocol.
During the initial study assessment, participants underwent cervical spine MRI. We then monitored participants until they were cleared by their physician to begin the return-to-play protocol in line with the most recent consensus statement on concussion in sport at the time of their study participation2,23 (Figure 1). To determine associations with return-to-play clearance time, our outcome was the number of days from concussion until clearance for return to play by their physician. Participants returned for a follow-up assessment on receiving return-to-play clearance, during which they underwent another cervical spine MRI. We then monitored participants for subsequent sport-related injuries (ie, musculoskeletal, concussion) in the following year using monthly electronic injury surveys. The outcome for determining associations with subsequent injury risk was the number of days between return-to-play clearance and sustaining a subsequent injury.
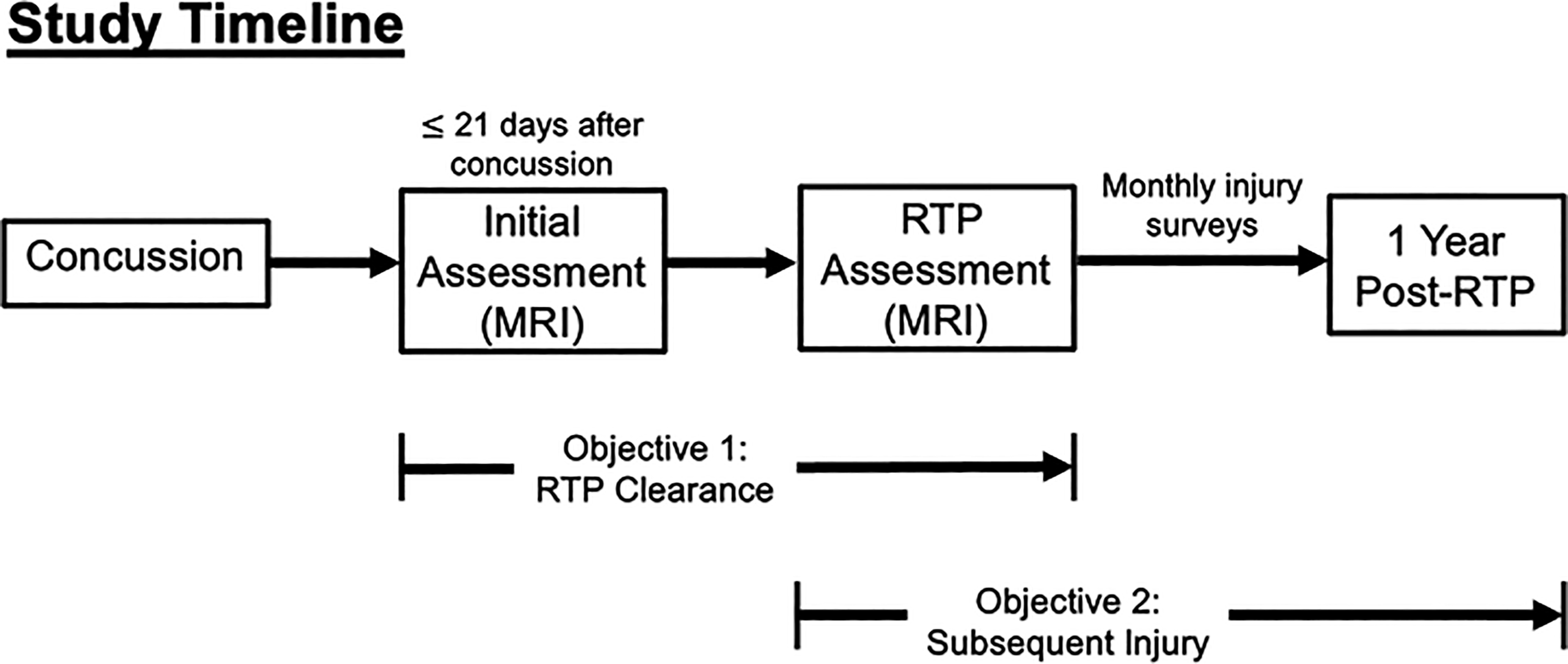
Study timeline line detailing timing of MRI scans and each outcome of interest (RTP clearance time, time to post-concussion subsequent injuries). MRI, magnetic resonance imaging; RTP, return to play.
Outcome Measures
At each assessment, participants underwent MRI of their deep cervical spine flexor (longus colli, longus capitis) and extensor (multifidus, semispinalis cervicis) muscles from C3-C6 (Figure 2). 24 MRI was performed using a 3.0-tesla Siemens Skyra scanner (Siemens, Erlangen, Germany) with a 64-channel head/neck coil with a dual-echo gradient-echo FLASH Dixon sequence (acquisition time = 4 minutes 57 seconds, TR = 7.05 milliseconds [ms], TE1 = 2.46 ms, TE2 = 3.69 ms, flip angle = 12°, field of view = 320 × 320 mm2, slice oversampling = 20% with 40 slices per slab, slice thickness = 3.0 mm, resolution = 0.7 × 0.7 mm2, number of averages = 6). We used a previously developed and validated multi-muscle convolutional neural network model for automated segmentation of cervical spine muscles from Dixon fat-water images.24,25 The automated segmentation was performed using a U-net convolutional neural network model to quantify muscle fat infiltrate and muscle volume using the MONAI framework for deep learning in health care imaging.26,27 Using the fat and water signal intensities from each muscle segmentation, muscle fat infiltrate was calculated using the following equation: fat signal / (fat signal + water signal) × 100%.13,24
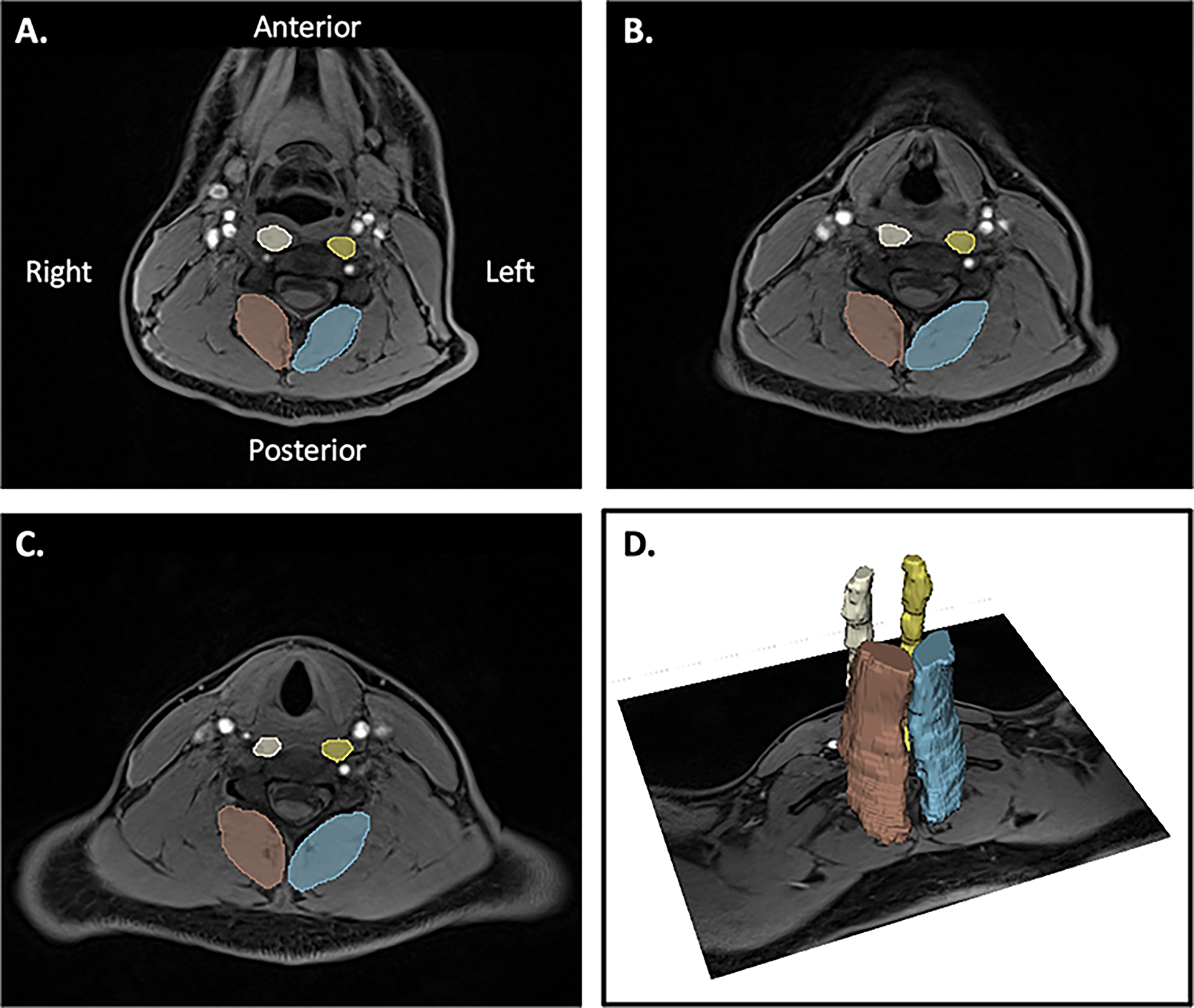
Example images of the automated segmentation for the cervical spine muscles at (A) C4, (B) C5, (C) C6, and (D) a 3-dimensional image of the cervical spine muscles. The segmented muscles include longus colli and longus capitis (left = yellow, right = white) and multifidus and semispinalis cervicis/capitis (left = blue, right = brown).
The MRI at our facility underwent a software upgrade from VE11C to XA30A in September 2022. Because of slight differences in the MRI sequence following this upgrade, the values for muscle fat infiltrate and muscle volume were significantly different between participants scanned before and after the upgrade. Thus, we adjusted for the software upgrade in our statistical analysis by performing a meta-analysis of pre- and postupgrade data to allow for use of all available MRI data. 28
After the return-to-play assessments, participants completed monthly electronic surveys for 12 months about subsequent sport-related injuries and athletic exposures. 29 Each month, we sent surveys to participants using REDCap. 30 Participants reported any sport-related injury they sustained that resulted in missing ≥1 practice or competition, and the number of practices and competitions they participated in for each sport during that month. If any injuries were sustained, participants answered additional questions about each injury. Questions included the date of injury, area of the body that was injured, the type of injury sustained, the sport during which the injury was sustained, the type of medical provider who diagnosed the injury, the amount of time lost from their sport due to the injury, and a narrative description of each injury sustained.
Statistical Analysis
To investigate the association between return-to-play time and cervical spine muscle health characteristics, we used separate univariable Cox proportional hazards regression models for each muscle variable (ie, muscle fat infiltrate and muscle volume). For both models, time to return-to-play clearance was the outcome. We used average muscle fat infiltrate of the deep cervical spine flexors and extensors as the predictor variable in one model, and muscle volume of the same flexor and extensor muscles as the predictor in the other model. Because of the software upgrade, we analyzed pre-upgrade and post-upgrade participants separately. We then performed a fixed effects meta-analysis to combine the hazard ratios for return-to-play clearance for participants pre- and post-upgrade. To maximize our sample, we only inferred data using the meta-analysis (combined) approach.
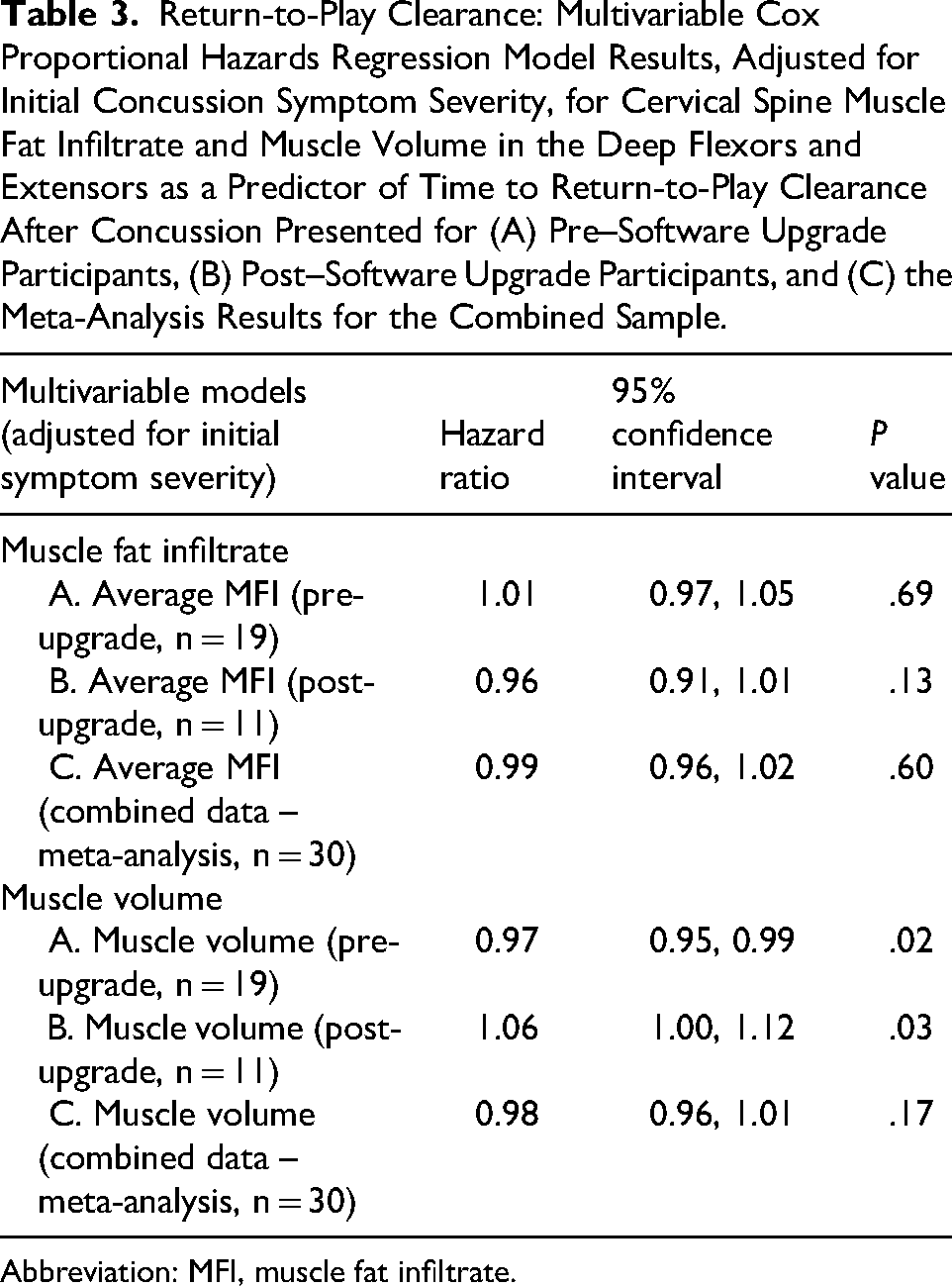
We then repeated these steps using a multivariable Cox proportional hazards regression model to investigate the relationship between return-to-play time and muscle fat infiltrate or muscle volume while adjusting for initial concussion symptom severity (initial Post-Concussion Symptom Inventory score) as that is the most consistent predictor of recovery time in previous research. 31 We again used a fixed effects meta-analysis to combine the hazard ratio for return-to-play clearance from participants pre- and post-upgrade, adjusting for initial symptom severity.
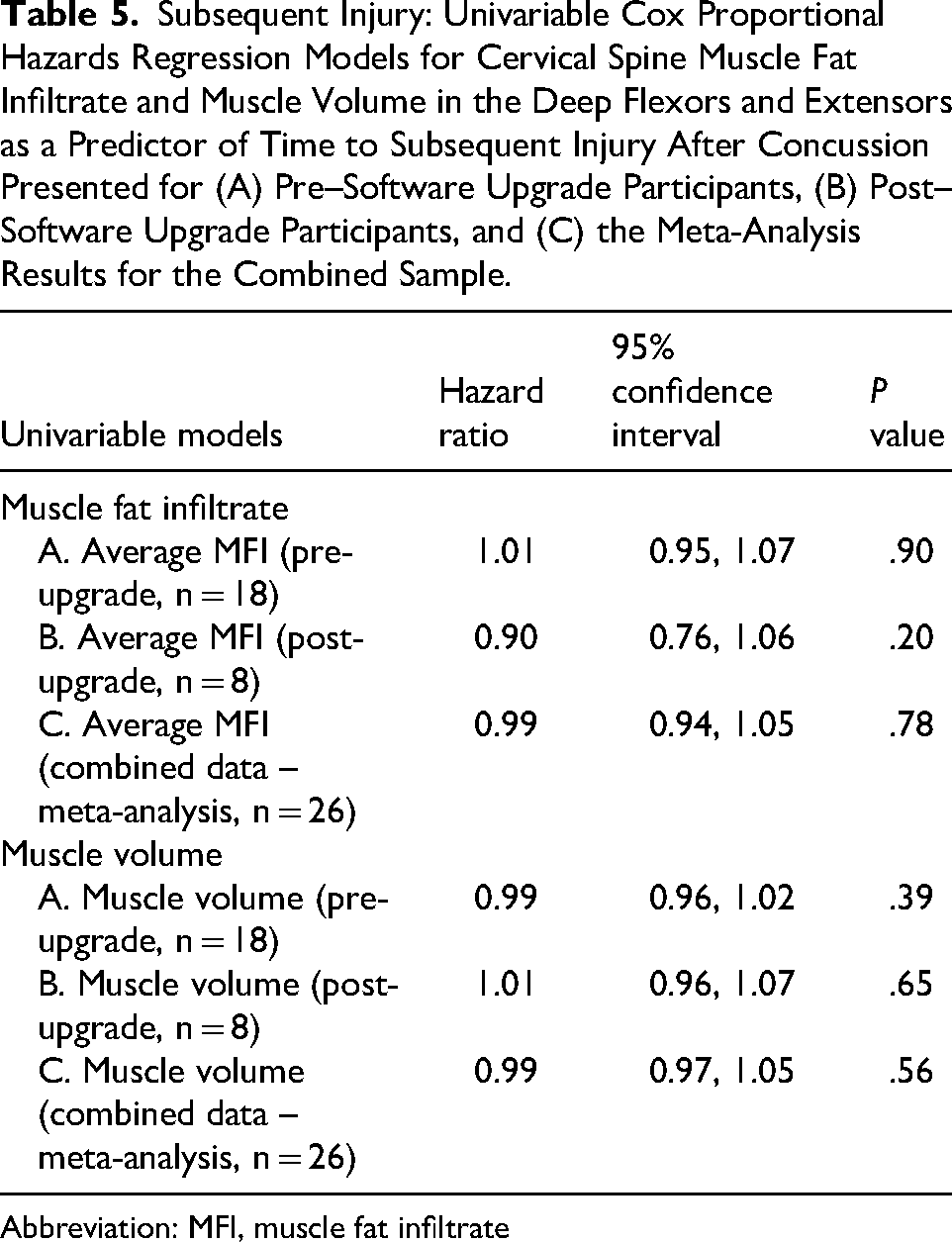
To investigate the association between time to subsequent injury and cervical spine muscle fat infiltrate and muscle volume assessed at the return-to-play clearance visit, we used univariable Cox proportional hazards regression models with time to subsequent injury as the outcome. We used separate models for muscle fat infiltrate and muscle volume of the deep cervical spine flexors and extensors. As a result of the software upgrade, we analyzed pre-upgrade and post-upgrade participants separately. We then performed a fixed effects meta-analysis to combine the hazard of subsequent injury from participants pre- and postupgrade. 28 Because of model convergence issues for post-upgrade participants, we were unable to adjust for additional variables in the meta-analysis and thus performed a univariable analysis only. We censored participants who did not sustain an injury during the follow-up period or did not complete the 12-month follow-up period, and we used their available data for the analysis.
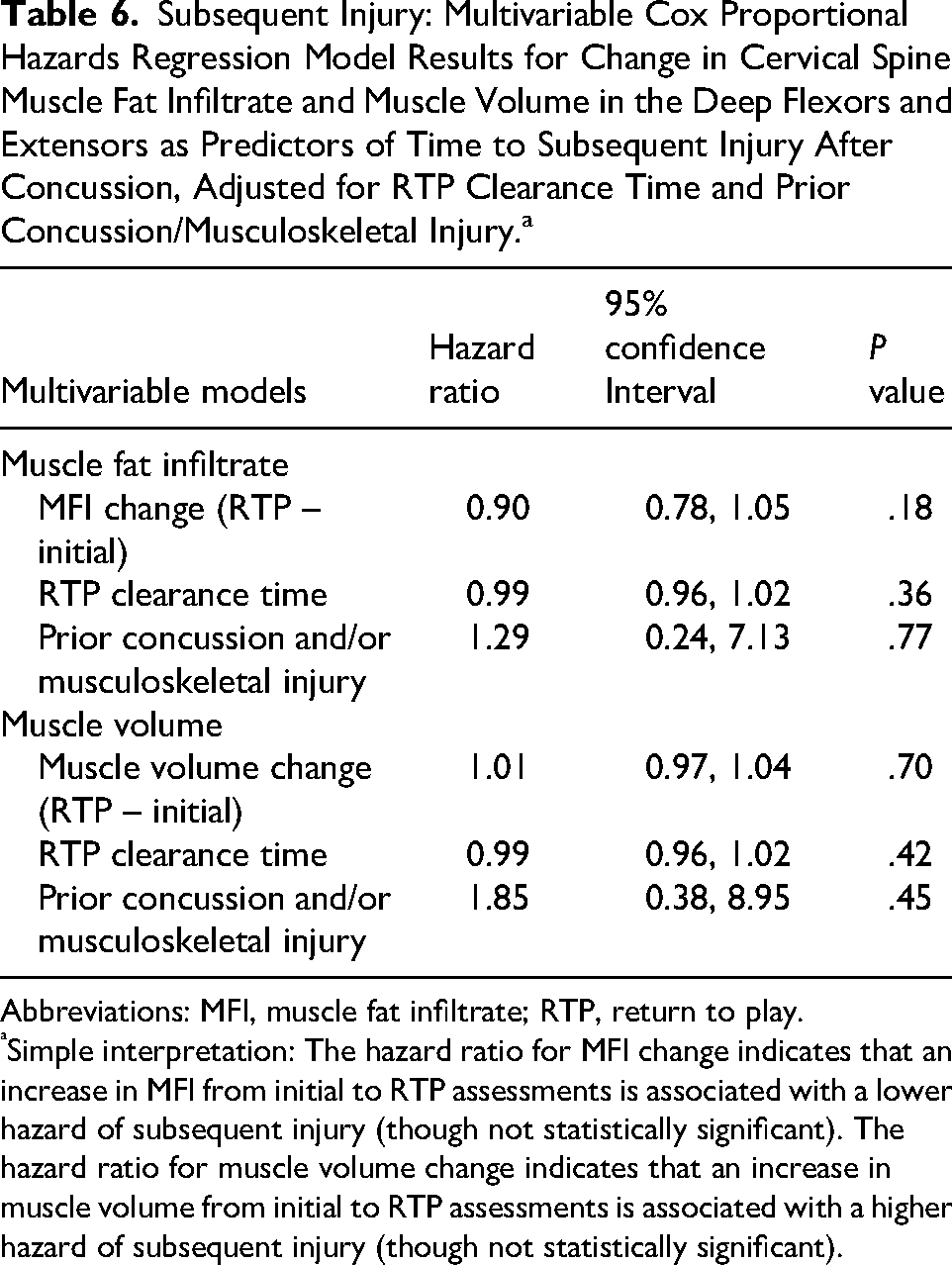
To understand the association between subsequent injury and cervical spine muscle fat infiltrate and muscle volume, we calculated the change between initial and return-to-play measures of cervical spine muscle fat infiltrate and muscle volume (return to play minus initial). Thus, a positive value indicates an increase in muscle fat infiltrate or muscle volume over time, and a negative value indicates a decrease. We used the within-person muscle fat infiltrate and muscle volume change in multivariable Cox proportional hazards regression models, adjusting for return-to-play clearance time and prior concussion and/or musculoskeletal injury.
All tests were 2-sided and statistical significance was set a priori at P <.05. Statistical analysis was performed using R studio (version 4.2.2, R Core Team 2022, Vienna Austria) and the Metafor package (version 4.6-0). 32
Results
We enrolled and initially assessed 30 participants whom we monitored through return-to-play clearance (Table 1). The participants who underwent MRI scans pre- and post-software upgrade were similar in demographics and clinical characteristics including age (15.8 ± 1.3 vs 15.7 ± 1.5 years, P = .82), proportion of female participants (58% vs 64%, P > .99), prior concussion history (37% vs 55%, P = .45), musculoskeletal injury history (63% vs 36%, P = .14), height (171 ± 11.3 vs 166 ± 7.3 cm, P = .25), and weight (66.7 ± 18.9 vs 62.6 ± 11.7 kg, P = .51). The meta-analysis results for the univariable Cox proportional hazards regression models indicated there was not a significant association between return-to-play clearance time and cervical spine muscle fat infiltrate or muscle volume of the deep cervical spine flexor (longus colli, longus capitis) and extensor (multifidus, semispinalis cervicis) muscles (Table 2). Similarly, after adjusting for initial symptom severity, the multivariable meta-analyses indicated there were no significant associations between return-to-play clearance time and cervical spine muscle fat infiltrate or muscle volume (Table 3).
Participant Characteristics.
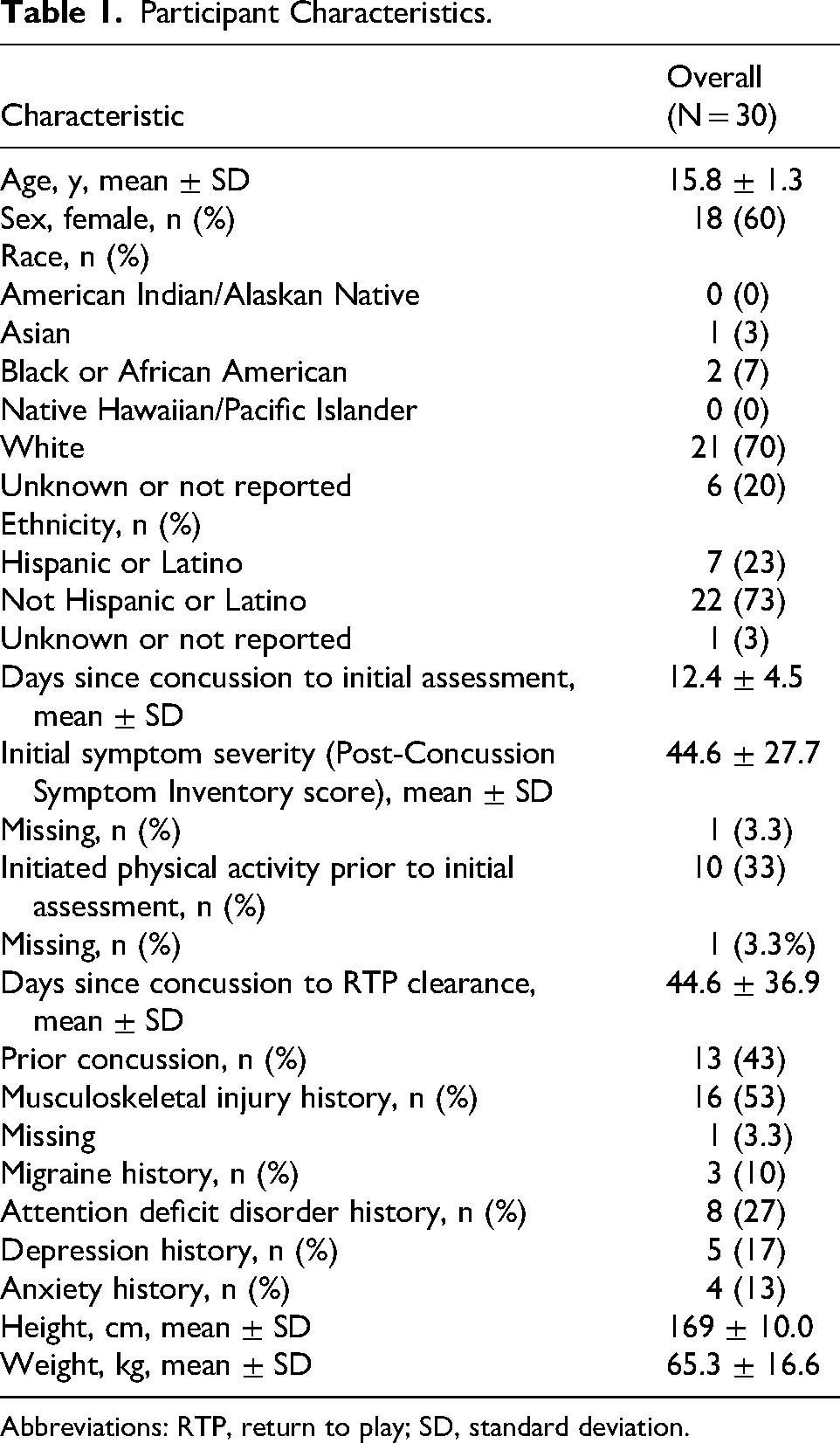
Abbreviations: RTP, return to play; SD, standard deviation.
Return to Play Clearance: Univariable Cox Proportional Hazards Regression Model Results for Cervical Spine Muscle Fat Infiltrate and Muscle Volume in the Deep Flexors and Extensors as a Predictor of Time to Return-to-Play Clearance After Concussion Presented for (A) Pre–Software Upgrade Participants, (B) Post–Software Upgrade Participants, and (C) the Meta-Analysis Results for the Combined Sample.
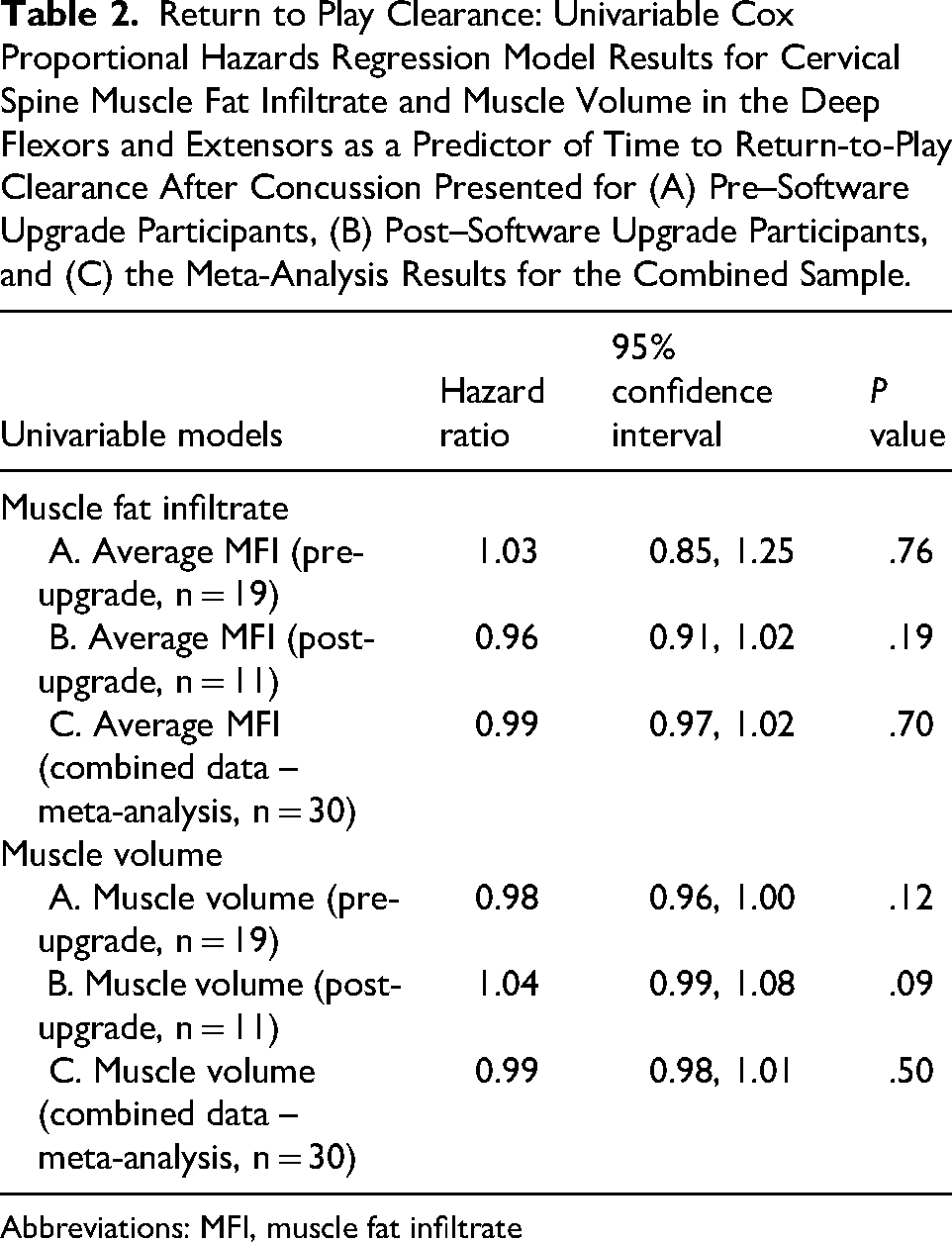
Abbreviations: MFI, muscle fat infiltrate
Return-to-Play Clearance: Multivariable Cox Proportional Hazards Regression Model Results, Adjusted for Initial Concussion Symptom Severity, for Cervical Spine Muscle Fat Infiltrate and Muscle Volume in the Deep Flexors and Extensors as a Predictor of Time to Return-to-Play Clearance After Concussion Presented for (A) Pre–Software Upgrade Participants, (B) Post–Software Upgrade Participants, and (C) the Meta-Analysis Results for the Combined Sample.
Abbreviation: MFI, muscle fat infiltrate.
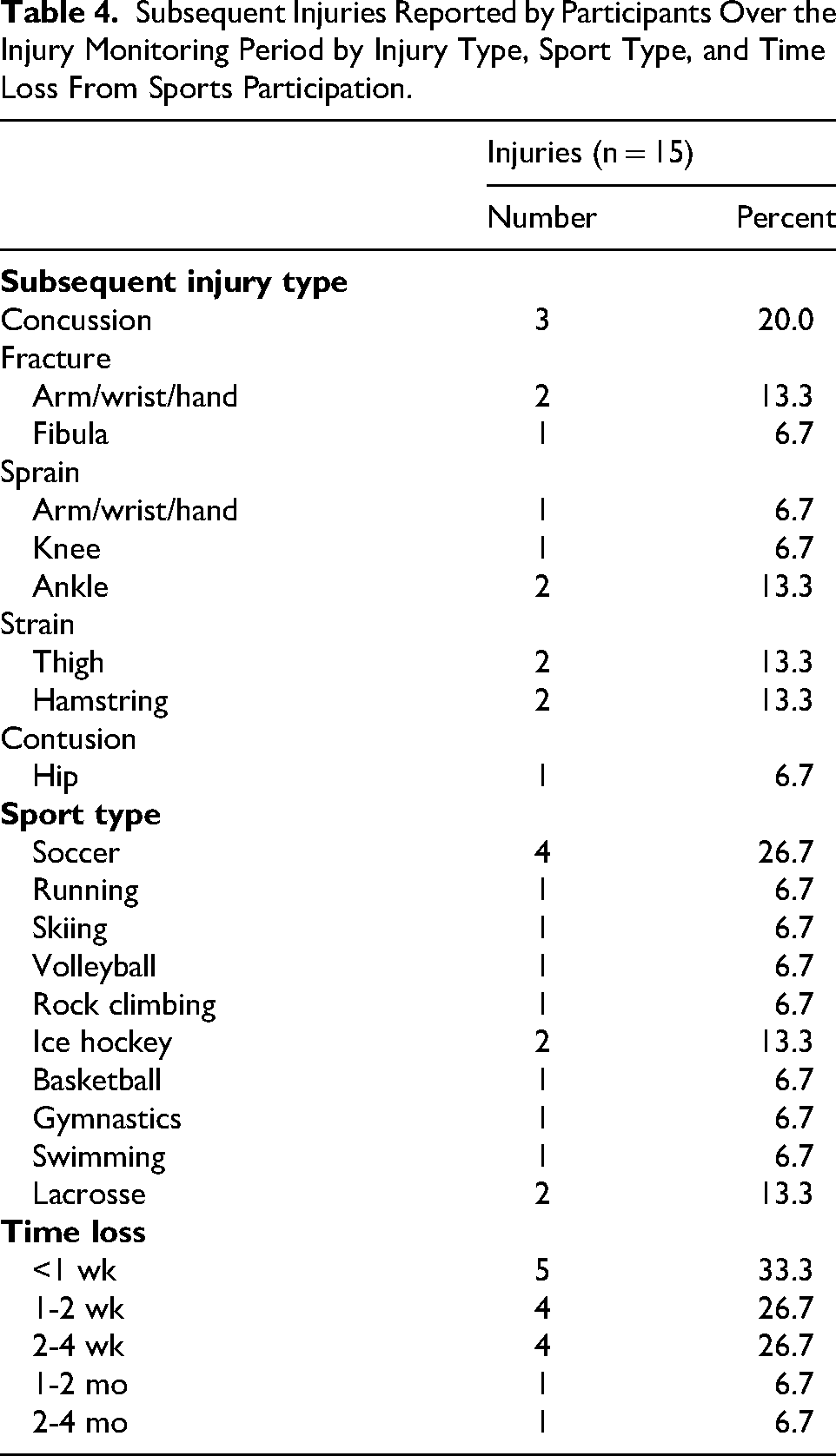
Twenty-six participants returned for follow-up MRI scans on receiving return-to-play clearance (age = 15.7 ± 1.4 years; 58% female; return-to-play assessment = 36.6 ± 16.4 days postconcussion) and 4 were lost to follow-up (age = 15.9 ± 0.6; 75% female). The 26 participants were monitored for subsequent injuries via monthly injury surveys. During the injury monitoring period, 10 participants (38% of the sample) sustained a total of 15 injuries (Table 4). The meta-analysis results for the univariable Cox proportional hazards regression models indicated there was not a significant association between hazard of subsequent injury and cervical spine muscle fat infiltrate or muscle volume in the deep cervical spine flexors and extensors (Table 5). When using the within-participant change from initial to return-to-play assessments for cervical spine muscle fat infiltrate and muscle volume, we did not observe significant associations with hazard of subsequent injury after adjusting for return-to-play clearance time and prior concussion and/or musculoskeletal injury in the multivariable model (Table 6).
Subsequent Injuries Reported by Participants Over the Injury Monitoring Period by Injury Type, Sport Type, and Time Loss From Sports Participation.
Subsequent Injury: Univariable Cox Proportional Hazards Regression Models for Cervical Spine Muscle Fat Infiltrate and Muscle Volume in the Deep Flexors and Extensors as a Predictor of Time to Subsequent Injury After Concussion Presented for (A) Pre–Software Upgrade Participants, (B) Post–Software Upgrade Participants, and (C) the Meta-Analysis Results for the Combined Sample.
Abbreviation: MFI, muscle fat infiltrate
Subsequent Injury: Multivariable Cox Proportional Hazards Regression Model Results for Change in Cervical Spine Muscle Fat Infiltrate and Muscle Volume in the Deep Flexors and Extensors as Predictors of Time to Subsequent Injury After Concussion, Adjusted for RTP Clearance Time and Prior Concussion/Musculoskeletal Injury.a
Abbreviations: MFI, muscle fat infiltrate; RTP, return to play.
Simple interpretation: The hazard ratio for MFI change indicates that an increase in MFI from initial to RTP assessments is associated with a lower hazard of subsequent injury (though not statistically significant). The hazard ratio for muscle volume change indicates that an increase in muscle volume from initial to RTP assessments is associated with a higher hazard of subsequent injury (though not statistically significant).
Discussion
We did not observe significant associations between MRI-obtained cervical spine muscle fat infiltrate or muscle volume of the deep cervical spine extensors and flexors and return-to-play clearance time or subsequent injury risk, contrary to our hypotheses. After whiplash, more cervical spine muscle fat infiltrate and larger multifidus muscle volume have been observed among individuals who experience persistent symptoms.12–16 This prior evidence suggests that MRI-obtained muscle health measures, specifically muscle fat infiltrate and muscle volume, may represent mechanisms of poor recovery after not just whiplash injuries, but other neuromuscular conditions (eg, Charcot-Marie Tooth and sarcopenia) and diseases (eg, cancer and diabetes).12–16,33–36 Given that the cervical spine is often injured concomitantly with concussion,7,8 it is important to consider how cervical spine dysfunction after concussion may present to better inform assessment, treatment, and prognosis. Understanding factors that have associations with subsequent recovery timelines (ie, return-to-play clearance, subsequent injury) could be helpful for health care providers in determining concussion prognosis and setting recovery expectations. Our results, however, suggest that cervical spine MRI muscle health measures obtained within 3 weeks of sustaining a sport-related concussion and again on receiving return-to-play clearance (36.6 ± 16.4 days postconcussion) are not associated with return-to-play clearance time or subsequent injury risk among adolescents recruited from a sports medicine clinic.
Because of the similar injury mechanisms between concussion and whiplash,7,8 we hypothesized that higher cervical spine muscle fat infiltrate and larger muscle volume in the deep flexors and extensors would be similarly associated with prolonged recovery after concussion (ie, longer return-to-play clearance time) as it is after whiplash.12–16,37 However, we did not observe significant associations between cervical spine muscle morphometry and return-to-play clearance time in our univariable or multivariable models that adjusted for initial symptom severity. Similarly, both our unadjusted and adjusted results suggest that cervical spine muscle fat infiltrate and muscle volume after adolescent concussion are not associated with subsequent injury risk. The lack of associations we observed between cervical spine muscle measures and concussion outcomes may be partially due to the timing of the MRI scans. The initial scan occurred an average of 10 days after concussion, and the follow-up scan occurred approximately 5.5 weeks after concussion. After whiplash, no differences in cervical spine multifidus muscle fat infiltrate between those who recovered fully and those who developed persistent symptoms were observed at 4 weeks. 12 However, at 3 months postinjury, muscle fat infiltrate was higher among those with ongoing whiplash symptoms compared with those who recovered. 12 Similarly, increased cervical spine multifidus volume has been observed between 3 months and 3 years after whiplash among individuals with persistent whiplash symptoms, 15 although other studies have reported no associations between persistent whiplash symptoms and deep cervical spine extensor and flexor muscle volume.38,39 It may be that if changes in cervical spine muscle health exist after concussion, they would be observed at a later time postconcussion than our study evaluated. Thus, our MRI scans may have occurred too early during the post-injury period to adequately capture the chronic dysfunction necessary to result in cervical spine muscle volume and muscle fat infiltrate changes on MRI.
In addition to the relatively early timing of our MRI scans after concussion, the young age of the participants in our study (13-18 years) may be another reason that our results were not significant. Previous whiplash studies reporting elevated cervical spine muscle fat infiltrate after whiplash were performed among an adult population, and cervical spine muscle changes are more pronounced among adults compared with adolescents.12–15 Further, many of the previous MRI studies performed among the whiplash population included participants who sustained their injury in a motor vehicle collision.12–16,37 Given that we specifically excluded individuals who sustained their injury via a high-velocity mechanism, such as a motor vehicle collision, the forces sustained during sport-related concussions may not have elicited alterations in cervical spine muscle health because of a lower-velocity injury mechanism. Accordingly, future investigation of cervical spine muscle health after concussion among individuals with neck pain/neck-related dysfunction, an adult population, those with more chronic injuries and/or experiencing persistent concussion symptoms, and those who sustained concussions from high-velocity mechanisms may be worthwhile to further the understanding of cervical spine involvement throughout concussion recovery.
Both of our outcomes of interest, return-to-play clearance time and postconcussion injury risk, are complex and highly variable. For example, return-to-play clearance requires that concussion symptoms have resolved. 2 However, concussion symptoms are nonspecific, which may make it difficult to determine if symptoms are due to ongoing effects of the concussion, existed prior to the concussion, or were related to behavioral or biologic function unrelated to the concussion. 40 Further, although symptom resolution is necessary for return-to-play clearance, there are no established guidelines for determining physiologic recovery from concussion. 6 Thus, athletes may be cleared for return to play based on symptom resolution while still having underlying physiological dysfunction that is not detected with current return-to-play assessments. 40 There is also the subjective element of self-reported symptom resolution, which allows for potential over- or underreporting of symptoms, based on personal motivation to return to sports sooner or remain out of their sport longer.41,42 This collective evidence indicates that determining return-to-play readiness is complex and heterogenous, and objective markers to better determine readiness for return to play are needed. 43 Earlier identification and management of concomitant cervical spine injuries after concussion has been suggested as a factor that may mitigate the risk of prolonged recovery associated with cervical spine dysfunction. 44 However, our results suggest that cervical spine muscle health may not be useful for concussion recovery prognosis among adolescent athletes recruited from a specialized sports medicine clinic.
Similar to determining return-to-play readiness, identifying individuals at risk for subsequent postconcussion injuries is also a complex process. Although the increased risk of subsequent injuries after concussion return-to-play has been observed among male and female athletes across various sports and competition levels,4,5 the mechanisms of this increased risk are not fully understood. Many factors that have been investigated in the context of postconcussion injuries have not been associated with subsequent injuries and, therefore, do not help clinicians identify and intervene with at-risk individuals.45,46 Specifically, assessments of reaction time, standing balance, cognition, and mental health outcomes (ie, anxiety and depression) were not associated with subsequent injuries.45,46 In contrast, previous research has identified changes in lumbar spine multifidi cross-sectional area (ie, smaller multifidi) among individuals with a concussion history. 47 Smaller lumbar multifidi muscle size measured before a rugby season was associated with sustaining a concussion during the season, 47 which may have implications for other injuries, including subsequent injuries after return to play from concussion. Our results suggest that cervical spine muscle health measures obtained on athletes receiving return-to-play clearance after concussion were not associated with subsequent injuries over the following year. It is possible that cervical spine muscle changes may develop later after concussion and may represent a potential mechanistic explanation for subsequent injuries, rather than a predictive factor as we evaluated in this study.
Our study limitations should be considered when interpreting the results. Our participant population of adolescent athletes who were recruited from a sports medicine clinic within a pediatric hospital in one geographical region may not generalize to all populations of athletes with concussion. The specialized nature of the sports medicine clinic may have also biased the study sample to participants with longer than average recovery times because of the complexity of their clinical presentation. Adults and individuals who sustain a concussion during a high-velocity mechanism may have cervical spine muscle changes on MRI. Because our participant population consisted of adolescent athletes participating in a variety of sports, the variation across sports may have contributed to our nonsignificant findings. Collision/contact sports may result in higher-velocity mechanisms of injury, which may yield different results when investigating cervical spine involvement after concussion. Our monthly injury surveys relied on accuracy of participant reporting, and the results could have been affected by recall bias. The timing of our initial and follow-up MRI scans may have occurred too early after concussion to capture chronic dysfunction that may lead to muscle changes on MRI. Thus, cervical spine muscle changes may occur later after concussion than our study investigated. The relatively small sample size may have also limited our power to detect associations with return-to-play time and injury risk, and future research with a larger sample may help further the understanding of factors associated with postconcussion recovery outcomes.
Conclusion
Cervical spine deep flexor and extensor muscle fat infiltrate and muscle volume after concussion were not associated with return-to-play clearance time or subsequent injury risk among the adolescent athletes in our study. Although changes in cervical spine muscle health have been well documented among adults after whiplash, our results suggest that the same changes may not occur early after adolescent sport-related concussion.
Footnotes
ORCID iDs
Author Contributions
Katherine Smulligan: Conceptualization, methodology, investigation, formal analysis, visualization, writing – original draft. Andrew C. Smith: Conceptualization, methodology, investigation, visualization, writing – review & editing. Kenneth A. Weber: Conceptualization, methodology, formal analysis, visualization, software, writing – review & editing. Patrick Carry: Conceptualization, formal analysis, visualization, writing – review & editing. Carrie Esopenko: Conceptualization, methodology, writing – review & editing. Christine M. Baugh: Conceptualization, methodology, writing – review & editing. James Elliott: Conceptualization, methodology, software, writing – review & editing. Suzanne Snodgrass: Conceptualization, methodology, software, writing – review & editing. Evert Wesselink: Conceptualization, methodology, software, writing – review & editing. Julie Wilson: Conceptualization, methodology, writing – review & editing. David Howell: Conceptualization, methodology, writing – review & editing, supervision, project administration, funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this work was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development (R01HD108133), the National Institute of Health (T32AR080630), the Tai Foundation, and a Promotion of Doctoral Studies Scholarship from the Foundation for Physical Therapy Research.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Unrelated to this study, Dr Howell has received research support from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (R03HD094560), the National Institute of Neurological Disorders And Stroke (R01NS100952, R43NS108823), the National Institute of Arthritis and Musculoskeletal and Skin Diseases (1R13AR080451), and the Colorado Clinical and Translational Sciences Institute (UL1 TR002535-05). Unrelated to this study, Dr Smith has received research support from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (K01HD106928) and the Boettcher Foundation's Webb-Waring Biomedical Research Program. Unrelated to this study, Dr Wilson has received research support from the 59th Medical Wing Department of the Air Force. Unrelated to this study, Dr Esopenko has received research support from the National Institute of Neurological Disorders and Stroke (R01NS115957), the Department of Defense (W81XWH-21-S-TBIPH2), and the National Institute on Disability, Independent Living, and Rehabilitation Research (90DPTB0028). Unrelated to this study, Dr James Elliott serves on the advisory board for Health Hunter and for Ho’ola Na Pua, serves as Non-Executive Director for Survivors and Mates Support Network, and has 3% equity in Orofacial Therapeutics. The remaining authors have no other disclosures.