
Abstract

A 17-year-old woman with nonlesional focal epilepsy underwent implantation of a responsive neurostimulation (RNS) system, consisting of a neurostimulator implanted in the left parietal skull region and 2 RNS depth electrodes placed in the left precentral cortex. One RNS depth electrode was positioned in the superior left precentral gyrus with extension into the anterior paracentral lobule, whereas the second was placed in the left precentral region with extension into the posterior paracentral lobule. At 20 months after implantation, she had achieved an approximately 50% reduction in seizure frequency. She developed new events of prolonged right leg weakness and behavioral arrest amid psychosocial stressors, prompting scalp electroencephalogram (EEG) evaluation. These events were captured during scalp EEG monitoring and were determined to be nonepileptic in nature. On baseline RNS settings (7.1 Hz, 160 µs, 1000-ms bursts, 3.0 mA, estimated charge density of 1.5 µC/cm2), frequent left centroparietal 7-Hz ∼20 ms sharp transients lasting ∼2.25 seconds were seen, followed by a large-amplitude transient and slow wave with overriding paroxysmal fast activity (Figure 1A). Comparison with RNS electrocorticography (ECoG) (Figure 1D, 7.1 Hz stimulation) and disappearance after turning off RNS stimulation (Figure 1B) confirmed these as RNS artifact. After changing RNS parameters (200 Hz, 160 µs, 100-ms bursts, 2.0 mA, estimated charge density of 2 µC/cm2), the 7-Hz periodic pattern resolved, whereas the large-amplitude transient with slow wave and fast activity persisted (Figure 1C). This case illustrates that RNS stimulation parameter variation can alter scalp EEG artifact morphology.
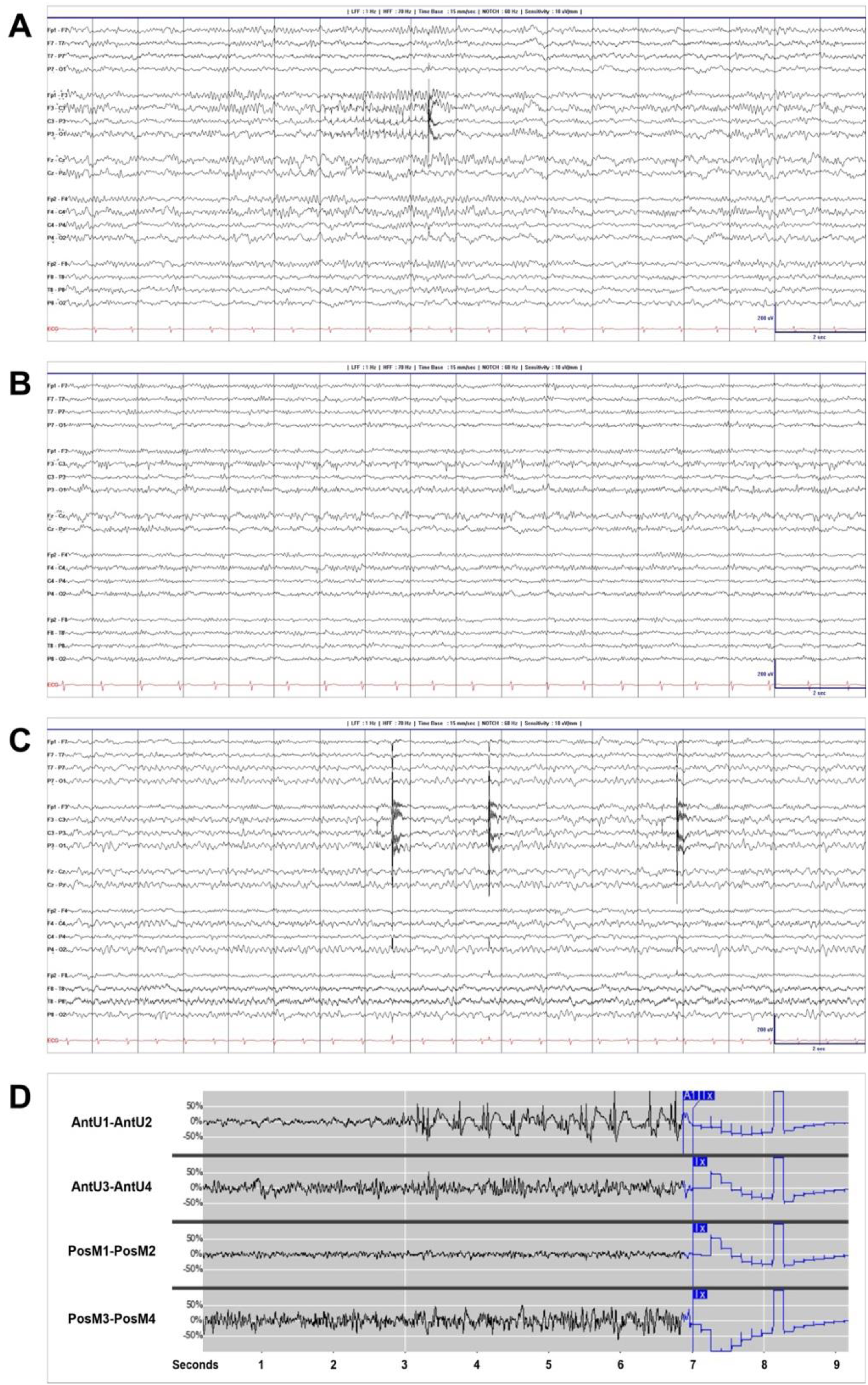
(A) Scalp EEG (bipolar longitudinal montage) with RNS stimulation set at 7.1 Hz. (B) Scalp EEG with RNS stimulation turned off. (C) Scalp EEG during 200 Hz RNS stimulation. (D) RNS ECoG recorded with stimulation programmed at 7.1 Hz, demonstrating rhythmic epileptiform activity that met detection criteria and triggering a stimulation burst at approximately 7 seconds, visible across all displayed channels and associated with a subsequent alteration in waveform morphology. ECoG, electrocorticography; EEG, electroencephalograph; RNS, responsive neurostimulation.
With the growing adoption of neuromodulatory devices including RNS in contemporary epilepsy care, clinicians are increasingly encountering device-related findings during routine and inpatient scalp EEG evaluations with device-induced artifacts that can mimic interictal epileptiform activity.1–3 Lemus et al 2 showed that during scalp EEG monitoring (11 patients; mean 3.6 days), most RNS detections were brief (<10 seconds) and 67.1% of stored long episodes lacked a scalp EEG seizure correlate; when scalp correlates were present, intracranial events were longer (median 39.7 vs 16.8 seconds) with broader spread and higher ECoG amplitude, and brief potentially ictal rhythmic discharges (BIRDs) frequently accompanied long episodes not meeting scalp EEG seizure criteria. RNS stimulation scalp EEG artifacts are stereotypical, often with large-amplitude, broad-field, negative spikelike or periodic spiky burst patterns often maximal near the generator, typically without ictal evolution or postictal slowing, and abolished by deactivating RNS stimulation.3,4 Uniquely, this case demonstrates within-patient, parameter-dependent RNS scalp EEG artifact morphology, showing that reprogramming can selectively alter artifact patterns.
Practical workflow to evaluate suspected RNS-related patterns on scalp EEG:
Assess morphology for “artifact clues”: monomorphic, precisely periodic bursts; broad field; no spatial/temporal evolution; absent postictal slowing.3–5 Briefly disable stimulation to confirm artifact resolution, then restore settings.3,4 Correlate with ECoG RNS data (detections/long episodes) to determine whether there is a true intracranial event and whether it should be expected to appear on scalp EEG.
2
Document current RNS settings (frequency, pulse width, burst duration, current), note whether therapy occurred near the pattern, and reassess artifact morphology after any parameter changes. Integrate semiology, EEG-RNS correlation, and recent stressor/medication changes before concluding the finding is nonartifactual.
Footnotes
Acknowledgments
None
Author Contributions
T.H. provided clinical care to the patient; analyzed the data; drafting/revision of the manuscript. S.E.O. provided clinical care to the patient; analyzed the data; drafting/revision of the manuscript. P.J. provided clinical care to the patient; analyzed the data; drafting/revision of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.