
Abstract
Introduction:
Neurologic disorders contribute significantly to the global burden of diseases and especially have major consequences for children. Many paediatric neurologic conditions are chronic, causing disability, requiring multiple hospitalisations, and leading to significant psychosocial challenges. The constant health care visits can be distressing to the children.
Methodology:
Using an exploratory research design, this study aimed to understand the experiences of children receiving inpatient care for neurologic disorders in a tertiary care hospital. Data were elicited through interviews guided by a picture-based tool developed by the researcher, and the interviews were thematically analysed.
Results:
The participants were in the age group of 8-14 years, both male and female. The overarching theme that came out from the interviews was ‘the illness and the hospital world’. Under this, major themes elicited were the illness, hospitalisation as an unpleasant event, disrupted normalcy and no end in sight.
Conclusion:
The study highlights the need to pay attention to the child-patient. Children are often invisible in health care interactions, with the conversations happening over their heads. The findings point towards the need for being sensitive to the children's experiences while in hospital and to focus on psychosocial care during hospitalisation and beyond for children with neurologic disorders.
Neurologic illness has been the second leading cause of disability-adjusted life years across the life course. 1 Neurologic illness in children is a cause for concern as failure for early and accurate diagnosis and treatment can have significant long-term consequences. The diseases can range from neonatal and congenital structural defects to genetic and metabolic disorders. 2 Many of these conditions are chronic in nature and can cause significant disability and interrupt the child's growth and achievement of developmental milestones. Some diseases require lifelong management, whereas some can be life-threatening. Pediatric neurologic disorders are also a common reason for tertiary care hospital referrals. 3 About 10.7% of all pediatric hospitalizations are for neurologic conditions, and the length of stay was significantly longer for children with neurologic illness than other children.4 The care for many children with neurologic illnesses is driven by crisis events and are also known to be more in need of emergency health services and frequent hospitalizations with subsequent readmissions. 5 Thus, children with acute conditions enter hospital-based care at a young age, and they are new to the hospital environment. Children with chronic conditions would have had multiple emergency room visits and hospitalisation experiences. With regards to both these situations, the associated difficulties are enormous. Because such children undergo frequent hospitalizations and tend to have longer stay in the hospital, it is understood that this group has more risk for adverse effects in the biological, psychological and social realms with significant distress. 6 Moreover, when the condition causes a disability, it affects the child's physical, mental, and social development and well-being.
The conditions and the associated symptoms lead to significant disruption in the normal functioning of the child, starting from the child's regular play or academic time to the way the child is treated at home, either by overprotective parents or by families that disregard the child's socio-emotional needs. In the case of a child with an acquired neurologic condition, the existing socio-emotional functioning such as scholastic performance, social participation, behavioural and emotional well-being can be compromised because of the illness and management. Given the nature of most of the neurologic disorders affecting children, hospitalisation potentially could be the beginning of a long-term management of the illness marked by multiple hospital visits, investigations and treatment, the effects of which are often compounded by the impairment due to the neurologic illness per se. Children might be left with disability that would need additional accommodation and support for their special needs. These factors can lead to the isolation of children with disabilities, which would lead to increased levels of stress and decreased levels of self-esteem in the children. Children are hence at risk for the adverse effects of illness, such as dropping out of school, lack of time with peers, and hospitalization becomes another stressful event with multiple psychosocial consequences.
Lack of familiarity with the hospital environment can result in significant adjustment-related issues; the procedures can sometimes be painful for the children, which can lead to fear, anxiety, etc. 7 Children also tend to miss out on their usual activities as a result of hospitalisation which can further affect their emotional health. Therefore, the treating professionals need to facilitate psychosocial support for children that would focus on multiple age-appropriate domains of the child's life. A significant literature gap pertaining to understanding the psychosocial correlates of children receiving in-patient care for neurologic conditions emerged during the review of existing literature. Hospitalization as a stressful event has also not been well explored in the Indian context. Therefore, this study aimed to understand the subjective experiences of children with neurologic disorders as they were receiving hospital-based care. The objectives of the study were to understand the psychosocial correlates associated with inpatient care for children with neurologic disorders.
Methods
An exploratory, qualitative research design was used to explore the experiences among children admitted to the hospital for management of neurologic illness. The study was part of a larger study aiming to understand the psychosocial correlates of hospitalisation in children. The qualitative component presented in the current article adopted a child-centric approach and focused on an attempt to access children's own experiences related to hospitalisation secondary to a neurologic condition. The study received ethical approval from the institutional review board. All measures were taken to ensure that the child is comfortable and in a safe space to share what he or she felt. Informed consent from the parents and assent from the children were obtained.
Theoretical Framework
ABCX model of family stress and coping 8 was used as the basis for the larger study exploring psychosocial correlates, which gives a framework to understand the need for catering to the often under-recognised needs of the children and the parents to help them have a better way out of the crises of illness and hospitalisation, enabling the restoration of family equilibrium. The model explores how a crisis can draw varied responses from families, 9 including changes in the provision of resources, emotional support, parenting, and child socialisation. 10
Participants and Recruitment
Children in the age group of 8-14 years receiving in-patient care from the Department of Neurology in a tertiary care hospital for a minimum of 5 days, or those who were likely to require inpatient care for more than 5 days, were approached to share their experiences. The study mainly intended to capture the hospitalisation experiences of children diagnosed with neurologic conditions, irrespective of the nature and course of the condition. The children were purposively selected for the interview based on their willingness and ability to share about their experiences. The inclusion criteria included children who can speak English, Tamil, Kannada or Malayalam who provided assent to participate and whose parents provided consent.
Children who were not able to communicate verbally as a result of the severity of their condition or were under high support, such as feeding tubes, diapers, catheters wherein they were highly dependent for their activities of daily living and on ventilator or emergency support and were unable to participate were excluded from the study. Children in the above-mentioned situations were not included because their medical condition precluded their involvement in the data collection, as was planned in the study, and managing the medical emergency was of primary importance during their in-patient care. The sociodemographic and clinical details of the children who completed the interviews are in Table 1.
Socio-Demographic and Clinical Profile of Children Who Were Part of the Qualitative Study.
Abbreviation: CwNI, child with neurologic illness.
Interview Process
Socio-demographic Data Sheet
This was developed by the researcher to understand the socio-demographic and clinical profile of the children. This included details on socio-demographic and illness details of the child, which were collected by reviewing the case files.
Semi-structured Interview Guide
This tool was designed in such a way that the children can be engaged as well as provide information regarding their experiences in a protected, expressive way, which would be more child-friendly.11,12 The incorporation of art into practice and research can expand the Social Health of children and their families. Studies have explored the use of picture-based or child-friendly techniques in research.13–15 Pictures were used as part of the topic guide because of their usefulness in eliciting the emotional experiences from the children. Children are generally familiar with such techniques, which reduces the power hierarchy between the researcher and the children, thereby enabling better rapport and better expression of experiences. Once developed, the tool was validated by experts working with children and qualitative researchers.
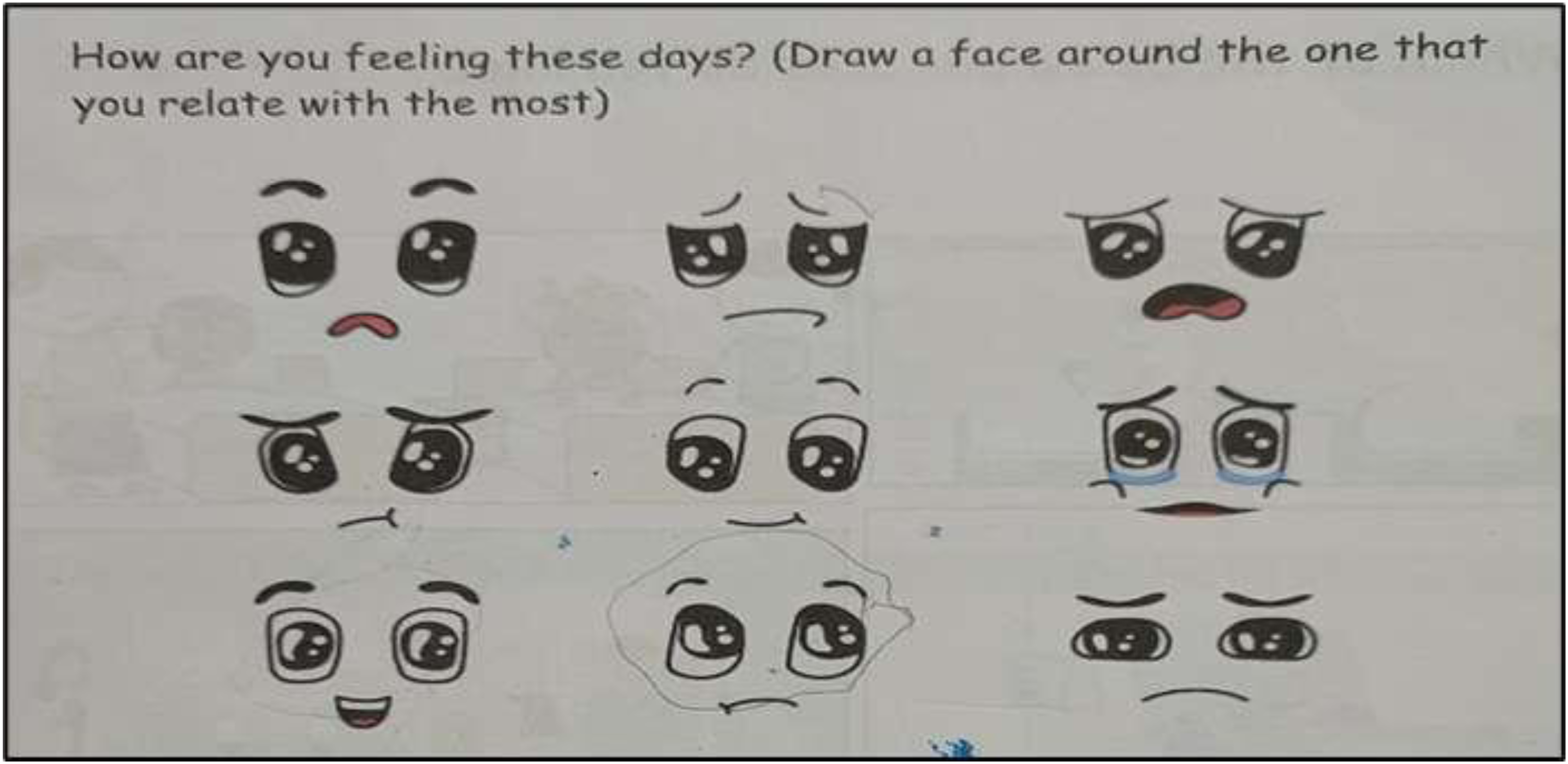
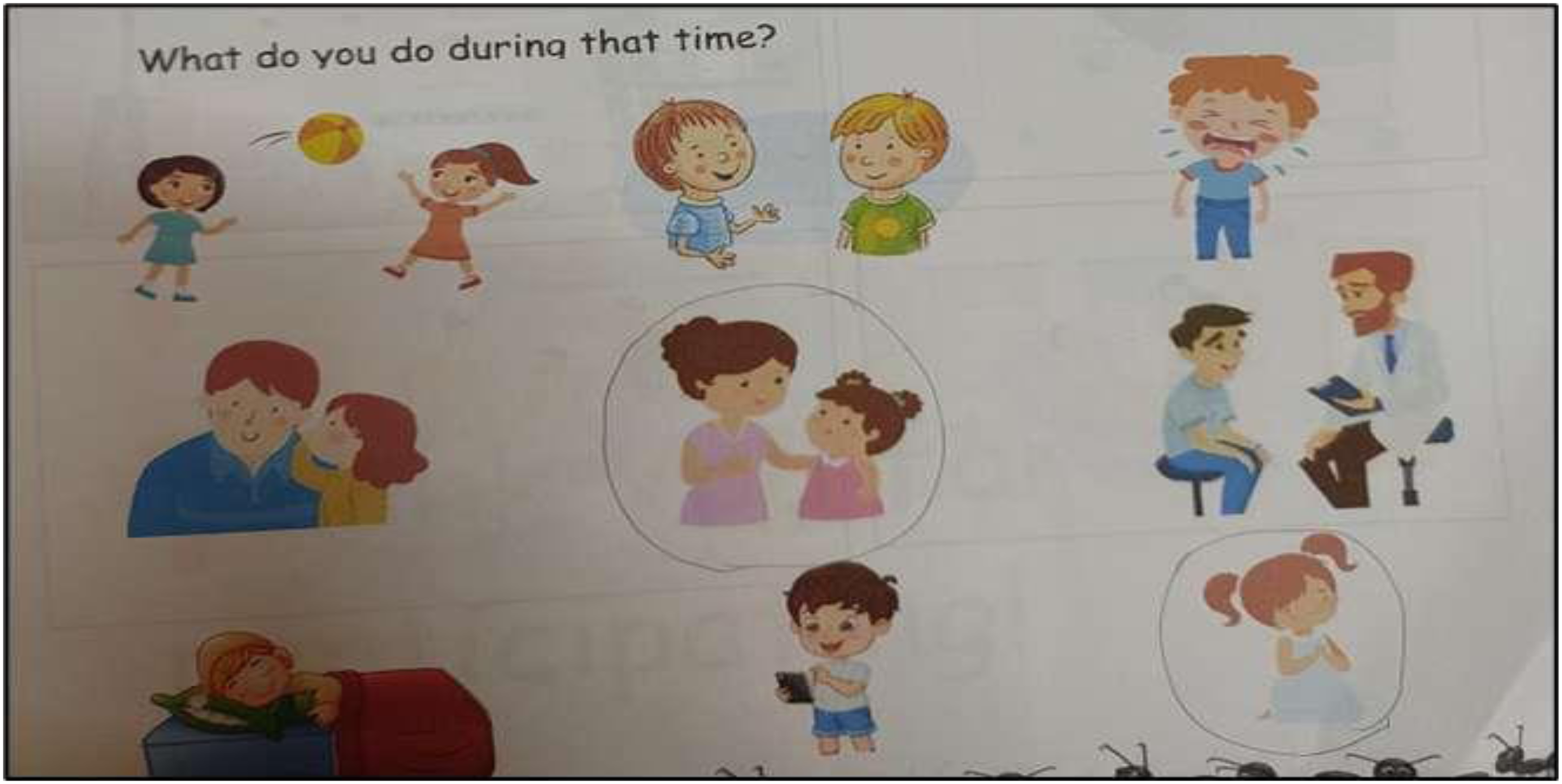
The first part of the schedule consisted of spontaneous drawing and colouring of pictures related to the hospital care by the child. This is to understand the child's perceptions or preoccupations. The second part consisted of pictures depicting the emotional aspects of the child. The first item covered the emotions of the child, adapted from the Wong-Baker Faces (FACES) scale and the visual analogue scale (Figure 1). The second item covered the child's expression of those emotions and the coping mechanism used. Several pictures as applicable to the age of the children were included (eg, sharing with parents, sleeping, praying, crying) (Figure 2). The third item included a few pictures that depict the hospital (Figure 3), a pediatric ward (Figure 4). This was to engage the children in colouring as well as to understand their perceptions and understanding of each of the pictures. The third part mainly focused on understanding the social aspects around the child's hospitalization. This involves direct items where the child was asked to choose the best out of 2 similar pictures with identifiable changes. Sub-item 1: Children in a ward with child-friendly professionals with a toy vs children with parents next to them. Sub-item 2: A patient who is left unattended and alone vs a child who is being told about his reports or illness by a professional. Sub-item 3: A child who has parents by his side, worried about the child vs a child whose parents are engaged with the child. The fourth part consisted of 2 open-ended questions to understand the child's dreams or hopes or disruption in normal routines: (1) What the child misses the most? and (2) What else the child would like to engage in during the hospitalization?
Response from a child on the predominant mood. Response from a child on the coping pattern. Response from a child on hospitalisation experience. Colouring activity (CwNI03).

Through the interview, efforts were made to ensure that the child describes the experiences of hospitalisation, rather than the consequences of illness and disability per se. The developed topic guide was validated by subject experts as to its appropriateness to the research objectives. Each activity was introduced to each of the children and was used as a probe to guide the interview.
Data Analysis
Each interview took about 45 minutes to 1 hour. The researcher spent time with the children while parents were provided a space near the counselling room as the process was going on. The filled pictorial tools were digitally scanned. The interviews with the children were audio recorded, translated and transcribed in English. Thematic analysis was done based on the elicited themes using the Braun and Clark 16 guidelines. The transcribed data were read twice for familiarisation, during which repeatedly occurring initial codes were highlighted based on a colour code. Different patterns of codes were categorized under various sub-themes, and a cluster of sub-themes following a similar idea were categorized under a single theme. Reviewing of themes was done by the research supervisor, followed by a refinement. The themes were defined based on the expression of the participants. The whole process was carried out by the researcher with guidance from the supervisor.
Findings
All the children who were part of the study were in-patients at the Pediatric Neurology Ward and were receiving treatment, presenting with a variety of diagnosis including seizure disorder, and autoimmune conditions. Five children who were able to share their experiences orally were recruited for the interviews. Figure 5 shows the various themes and sub-themes that emerged from the verbatims of the children.
Themes and sub-themes elicited from the study.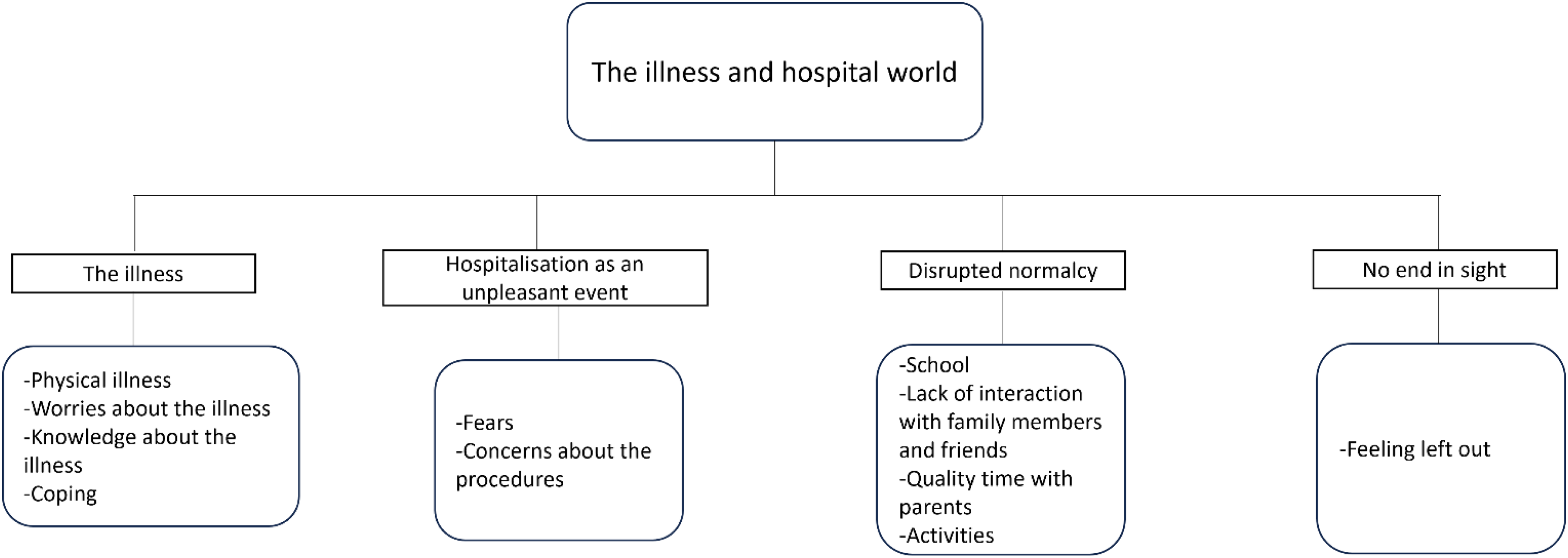
The Illness
The theme explains the various domains around the illness that created distress to the children. Because of several physical and social elements that may be ingrained in the condition, children and adolescents with neurologic disorders are more likely to develop depression and anxiety disorders. 17
Physical Difficulties
The children who were part of the qualitative study have reported concerns about their symptoms and were predominantly worried about the physical difficulties faced after their hospitalization or illness. They also expressed worries and fears regarding possible physical disability in future. My right hand was weak. I was not able to write. I was worried if it would become like that permanently. (CwNI01, 12 years old, female) My hand had problems. I felt very bad. . . . (silence) (CwNI02, 8 years old, female)
Worries About the Illness
Some of the children expressed worry by drawing tears, and also explained that the illness and subsequent hospitalization have made them sad. The children had lots of questions and confusion pertaining to the illness. Some of them added emotions to the already existing emotions by adding more tears. I was worried if it would become like that permanently. How do I go forward? How will my life be? I was feeling very sad and confused on the inside. (CwNI01, 12 years old, female)
Knowledge About the Illness
This sub-theme talks about how much the children were aware of their diagnosis. Most of the children were not aware of the nature or diagnosis of their conditions. They expressed their symptoms when asked about the reason for their hospitalization. Some of them were completely unaware as to why they were hospitalized. I don’t know why I was admitted to the hospital. (CwNI03, 8 years old, female) My leg was not fine. After the problem, I was ok for 3 years. Then I became weak, and then my father brought me here. (CwNI04, 11 years old, male)
Coping
Children's coping in stressful situations can be described as a collection of deliberate actions aimed at controlling various components of the self (emotion, cognition, behaviour and physiology) and the environment. Some of the children had employed positive mechanisms to cope with their illness and hospitalization whereas some could not. Talking to mother, friend, praying. All my relatives and family were in a lot of stress. Hence, I was not able to express it to them either, thinking that they would feel hurt. (CwNI0, 12 years old, female) I look at my phone when I am sad. (CwNI03, 8 years old, female)
Hospitalization as an Unpleasant Event
Fear
Many children reported fear and uncertainty regarding the process of hospitalization because it was mostly their first experience. After coming to the hospital, I was very scared. I was scared. I was scared as to what they would do in the hospital. There were tears. (CwNI04,11 years old, male) Hospital, ambulance. . . . I am scared of hospitals. They might give injections. (CwNI05, 9 years old, male)
Concerns About the Procedures
The children expressed significant concerns about pain and the various medical procedures. Because the children had not seen or undergone these procedures previously, they have expressed fear and unpleasant experiences, such as pain. They did many scans . . . MRI, scanning, blood check-up etc. It was scary. There was pain. I was not able to manage. (CwNI01, 12 years old, female) They gave me an injection on my back. Since then, I've been scared. The water didn't come. So they were seeing and seeing, and so they gave me a lot of injections. (CwNI05, 9 years old, male)
Disrupted Normalcy
For some youngsters, illness and hospitalization result in missed school days and educational opportunities. The children have expressed that there has been a disturbance in their schooling because of the illness. They have expressed how this illness and hospitalization have disturbed their school activities. Although it is natural to miss school for such disabling and serious conditions, this unexpressed concern remains unspoken many a times. My school was going on. I had taken leaves. How many days does it take was a question that I had. If there were classes happening, I had to see what was happening, what were the homeworks that were given. (CwN101, 12 years old, female) One girl is studying and the other girl is drawing pictures. I am the one studying . . . (pointing to the item number 2(b) in the pictorial tool). (CwNI03, 8 years old, female)
Lack of Interaction with Family Members and Friends
Families encounter a variety of obstacles when trying to see their hospitalized loved ones. Potential obstacles include time restraints brought on by the need to continue working to support one's family or to care for other children or family members at home. The children also expressed worries of not being able to be in close proximity with the other loved ones like before. I miss my dad. Because he had lots of work and he had to take care of my grandmother, he couldn't come. He video calls me everyday asking if I am ok. So I miss him. (CwNI01, 12 years old, female) This is me, my sister and brother. I think of them sometimes (pointing to a picture which she drew). (CwNI02, 8 years old, female) I don't have friends like that in the ward. (CwNI05, 9 years old, male)
Quality time with parents
Children's illness affects the psychological and social aspects of parents to a larger extent, wherein their focus turns primarily toward the illness. As a result, their role in taking care of the child's psychosocial needs becomes minimal, thereby reducing their quality interaction with the children. Here, children have expressed the need for quality time with their family. If doctors are there, they talk only about the medicine and the problem. If family members were there, they would talk well, they will try to make us laugh. (CwNI01, 12 years old, female)
Activities
Being in the hospital becomes unpleasant for many children who have to leave their familiar surroundings, like their home, and the people who are important to them while also having to stop their favourite activities, like playing, reading, drawing etc. This sub-theme shows the children's expression of the same. Other children sometimes come near the bed, so I talk to them. I don't have a pen or pencil. (CwNI05, 9 years old, male)
No End in Sight
Feeling Left Out
Although children were not very much aware of the reason behind their illness, they had significant worries related to what the condition could be. Existing stigmatization and possible stigmatization in future were some of the factors expressed by the children. Will people think I have COVID or something. . . . How do I continue my treatment when I go to school? (CwNI01, 12 years old, female) Nobody talks to me at school. I’ll be sitting alone. Everyone makes faces at me and say they won’t talk to me. (CwNI03, 8 years old, female)
Discussion
Neurologic conditions contribute to significant disabilities in children worldwide, as the majority of them can be of a disabling nature and require multiple hospitalizations. Hospitalization becomes an additional crisis for those who have already been trying to cope with the crisis of the illness. The focus shifts from regular activities to the illness, thereby causing more distress because of the disrupted routines. Exploring the psychosocial stressors around those children admitted for neurologic conditions and their parents becomes a need of the hour as it can have long-standing mental health and psychosocial adversities for both the children and the parents in the long run. Supporting them by addressing their needs in terms of family support and coping would prevent further worsening of the crisis. The present study has attempted to understand the psychosocial needs of children with neurologic disorders receiving inpatient care from the pediatric neurology ward of a tertiary care hospital. The results show the various themes and sub-themes elicited from the children. During their participation in the pictorial activities, they have also subtly and directly expressed various psychosocial issues and needs.
The interview process was solely based on the child's physical ability, willingness, and the child's need to start, stop and do the activities. Some of the children had stopped with a few activities which facilitated verbal expression. The spontaneous drawing of the children mainly contained pictures of trees, flowers, butterflies or a house. During the interviews, some of the children were not able to explain their drawings in relation to their hospitalisation experiences. This could probably be a context-specific factor where expressive arts are not taught or practised as a means of expressing oneself. It was also noticed that the children had difficulties explaining their concerns in detail.
The main themes elicited from the qualitative interview were the illness, hospitalization as an unpleasant experience, disrupted normalcy and no end in sight. The first theme described the children's concerns about their illness. These concerns mainly revolve around the physical difficulties, knowledge about the illness, coping and worries about the illness. Studies 18 have shown that children having chronic physical health conditions have significant anxiety. Patients of any age who have a thorough understanding of their chronic illness report less anxiety, less confusion, higher levels of satisfaction with their care, better adherence to treatment, and improved emotional well-being—all of which are essential components of a high quality of life when it comes to one's health. The second theme talks about how the children view hospitalization as an unpleasant event due to their general fears and worries regarding the procedures. Previous research has demonstrated that hospitalized children have anxiety brought on by the physical, social, and symbolic surroundings, child-staff interactions, the unfamiliar environment or lack of knowledge. 19
When a child's sickness is severe enough to require hospitalization, they frequently report feeling alone and afraid because they are removed from the supportive and safe setting of their home and are instead required to live in an unsettling, scary, and uncomfortable environment. 20
The third theme focuses on the disrupted normalcy of the children with regards to school, activities, quality time with parents and family. This highlights how children hospitalized for neurologic conditions require the same social stimulation and guidance just like any other child. Generally, illness draws a family's full attention, and worries about the illness are given more time than the children. Children who are hospitalized and managing their sickness are thought to benefit greatly from regular school attendance and prompt school re-entry. 21 It is natural that normal activities are disrupted during hospitalization for such disabling conditions. However, it remains important that such concerns are validated and provided a safe space for expression.
According to a qualitative study conducted with the pediatric population, one of the subjects that can affect how sick patients interpret the reason they are in the hospital is their social interactions with other people in society. Children depend heavily on their parents for daily survival and well-being as they grow up, but especially when they are ill, they require their families’ support more than ever because they lack the coping mechanisms and emotional reserves necessary to handle the extreme physical and emotional strain that hospitalization places on patients. 20 The fourth theme talks about the stigma faced by the children where they feel that they cannot see an end to their problems. Worries and anticipations regarding how they would enter and live a normal life in society again also seems are genuine concerns of the children.
This shows the way for investing greater efforts in Psychiatric Social Work practice for pediatric neurology inpatients. However, it may also be important to uphold an additional perspective that many children might also adapt to their disability over time, learn to use the available resources and accept their condition, which would enable better adjustments and quality of life. In such cases, professional support in making those adjustments and enhancing sustainability would be interventions that psychiatric social workers should be prepared to offer.
Not many studies have focused on children's experiences of hospitalization, especially in the Indian context. The findings of the present study could inform directions for future studies in the area and also to develop sensitive and compassionate care settings in pediatric neurology settings. Being a qualitative study, it gives voice to the children, and the participants, besides throwing light on the psychosocial difficulties experienced by the children.
The child-centric intervention components can include elements such as adjusting to the hospital or illness, expressing and seeking help for emotional concerns, awareness about the illness, quality time with parents, staying in touch with friends in school, being engaged in activities, making friends in the ward, getting prepared to restart school, skill training at home/institution.
Pediatric neurology is an important area with tremendous psychosocial needs, some of which have been discussed in this study. Early identification and early intervention are the keys to any problem; understanding the psychosocial crises that are specific to children with neurologic illnesses would be one implication for the psychiatric social workers. The study also calls for the psychiatric social workers to develop and carry out their assessments and interventions in a timely and efficient way based on the needs of the children.
Limitations of the Study
Being done in a vulnerable population in the inpatient setting, the study has its limitations. The sample size is small, in keeping with the nature of the study. The study could not elicit all the felt needs of the participants since the interviews had to be conducted within a limited time range and space, because the children had to be back for other medical procedures. Although the primary focus was to understand children's subjective experiences to provide them a safe space to express, there were no alternative methods to collect data from children who were critically ill and hence they were excluded. Similarly, the qualitative interview with the children was not able to bring out themes from the spontaneous drawing component, as the children were not able to use art as a form of expression. The tools designed by the researcher were only face validated because of the limited time available to complete the study. Further validation of content by experts would have helped in designing a better tool thereby facilitating better collecting of data.
Conclusion
Illness and hospital admissions can be the first crises that a child can encounter in his or her lifetime, as is the case for most children. Along with this, the changes caused by the illness can be more challenging for the children and their families. Article 12 of the United Nations Convention on the Rights of Child (UNCRC) states that children have the right to be heard and stresses the need to take them into account with regards to matters that affect them. Many times, children hospitalized for illnesses, especially those such as neurologic conditions that can cause significant disability are not given a space to express their needs and opinions. The current study has discussed the felt experiences of the children. Ensuring quality of life and well-being for children in every way is the way forward. The need to give ears to the concerns of children would be the key to kick-start the process. This would facilitate support seeking and greater well-being for the children. This study has initiated a step in understanding children's needs and it emphasizes that all the health care professionals in the field of pediatric neurology need to approach these children, knowing that they could have multiple psychosocial stressors, thereby also referring them to the respective mental health professionals.
Footnotes
Ethical Consideration
The study was reviewed and approved by the Institutional Review Board of National Institute of Mental Health and Neurosciences, Bangalore, India.
Author Contributions
S.M. designed the study, collected data, analysed and drafted the manuscript. A.M. revised the manuscript. P.T.T. supervised the study and revised the manuscript. All 3 authors read and approved the final draft of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.