
Abstract
Background
Child neurology in low- and middle-income countries (LMICs) faces persistent disparities in workforce capacity, subspecialty training, and structured mentorship. To address these gaps, the Child Neurology Society International Affairs Committee (CNS-IAC) launched a 2-phase initiative to identify regional needs and develop SMART (Specific, Measurable, Achievable, Relevant, Time bound) goals and action plans.
Objective
To identify educational and clinical priorities of child neurologists practicing in LMICs and translate these findings into region-specific SMART goals and action plans.
Methods
A mixed method study was conducted in 2 phases. Phase 1 (2024) used a de novo Qualtrics survey reviewed by the international child neurology experts. The survey assessed 12 clinical domains, preferred educational resources, and open-ended needs. Phase 2 (2025) consisted of structured regional working groups at the CNS Annual Meeting, where participants codeveloped SMART action plans through facilitated discussion and iterative refinement.
Results
A total of 48 clinicians from 18 LMICs contributed to phase 1 of the initiative
Conclusions
The CNS-IAC model provides a practical, scalable framework for moving from needs assessment to regionally driven action to strengthen child neurology capacity in LMICs.
Introduction
Child neurology in LMICs continues to face disparities in access to diagnostic tools, specialized training, and professional mentorship. 1 Although advances in neurodiagnostic, neurogenetics, and neurorehabilitation have expanded rapidly in high-income settings, these improvements have not been universally accessible. Existing reports highlight shortages of trained child neurologists, limited exposure to subspecialty care, restricted availability to essential diagnostic tools such as neuroimaging, electrophysiology, and inadequate opportunities for structured mentorship and research collaboration in many LMICs.2–4 These challenges not only contribute to delay in evaluation, diagnosis, and treatment but also demotivate doctors in training from pursuing careers in pediatric neurology, thereby leading to disproportionately high morbidity and mortality among children with neurologic disorders and exacerbated shortage. 5
Recognizing the need for coordinated global support, the Child Neurology Society International Affairs Committee (CNS-IAC) initiated a multiphase initiative in 2024 to identify educational needs and codevelop regionally contextualized goals and action plans. This approach aimed at aligning CNS educational goals with the realities of clinical practice in LMIC settings while promoting bidirectional knowledge exchange and regional ownership. The initiative was informed by global frameworks such as the International Child Neurology Association (ICNA) capacity reports and the World Health Organization Intersectoral Global Action Plan (WHO-IGAP) on epilepsy and neurologic conditions.6,7 This manuscript summarizes the multicenter mixed methods process used to identify priorities and develop regional SMART action goals, with the objective of providing a replicable model for global child neurology capacity building. This reflects evolving engagement across the 2-year process, rather than static cohorts.
Methods
Study Design
The study design consisted of 2 phases and uses a descriptive mixed method design. The CNS-IAC coordinated both phases to ensure consistency, context relevance, and integration of findings into action planning.
Phase 1: 2024 Needs Assessment
Survey development
The online survey was developed de novo by CNS-IAC members based on prior global child neurology training frameworks, International Child Neurology Association (ICNA) reports, and WHO-IGAP domains. Twelve clinical subspecialty domains were included based on consensus expert opinions from CNS-IAC membership and prior to global training literature. The survey was reviewed by the CNS-IAC task force. The task force reviewed the survey for relevance and cultural applicability. Minor revisions were made based on task force feedback. The survey was administered in English, except in south America where both English and Spanish versions were used.
Pilot testing
The survey underwent informal pilot testing by 2 CNS-affiliated clinicians practicing in LMICs (S.Q., M.R.) to ensure clarity and feasibility. Feedback led to minor wording adjustments.
Inclusion criteria and distribution
Inclusion was limited to child neurologists and trainees practicing in LMICs according to World Bank classification. 8 Clinicians from high-income countries who worked in close association in LMIC-based programs were also included, for example, through volunteer programs and local institutional support programs. The survey was disseminated through CNS-IAC networks, including CNS connect webpage, regional WhatsApp groups, SIG mailing lists, institutional partners, and regional child neurology professional associations. Participation was voluntary and anonymous.
Data collection and quantitative analysis
The survey was conducted through an online survey platform, Qualtrics. Descriptive statistics (frequency and percentages) were generated using Qualtrics, and further analysis and data consolidation were conducted in Microsoft Excel. Missing data were handled using pairwise omission, and denominators were specified for each item to address partial responses.
Qualitative analysis
Open-ended responses were analyzed using inductive thematic analysis. The independent reviewers’ coded responses developed a codebook iteratively and resolved discrepancies through consensus discussion. Themes were reviewed by a CNS-IAC chairperson to enhance analytic rigor.
In-person synthesis session (2024)
Nineteen participants contributed to discussions during the CNS-IAC SIG at the 2024 CNS Annual Meeting. Some participants had also completed the online survey. Discussions were summarized and integrated with survey findings.
Phase 2: 2025 SMART Action Planning
In 2025, a total of 39 clinicians participated in region-specific SMART planning sessions at the CNS Annual Meeting. The participants were self-selected into regional groups: Asia and Middle East, Africa and Caribbean, Latin, and South America. Each group was supported by CNS-IAC faculty moderators. Summaries of phase 1 findings were provided to the participants. Each group used structured worksheets to draft SMART goals and presented these to the entire group. Consensus was achieved through group discussion and iterative refinement. The follow-up virtual meetings ensured completion of timelines and measurable indicators.
Ethics
This initiative was categorized as educational program evaluation without human subjects research components and was therefore, based on consensus decision, IRB approval was not sought. All participation was voluntary and deidentified.
Results
Phase 1: Need Assessment
Forty-eight child neurologists from 18 LMICs participated in both online and in-person components (Table 1). There were 29 online participants and 19 in-person contributors with overlap of 2 participants, hence 46 unique contributors. Respondents represented diverse practice settings, predominantly tertiary care or teaching hospitals.
Phase 1 Data.
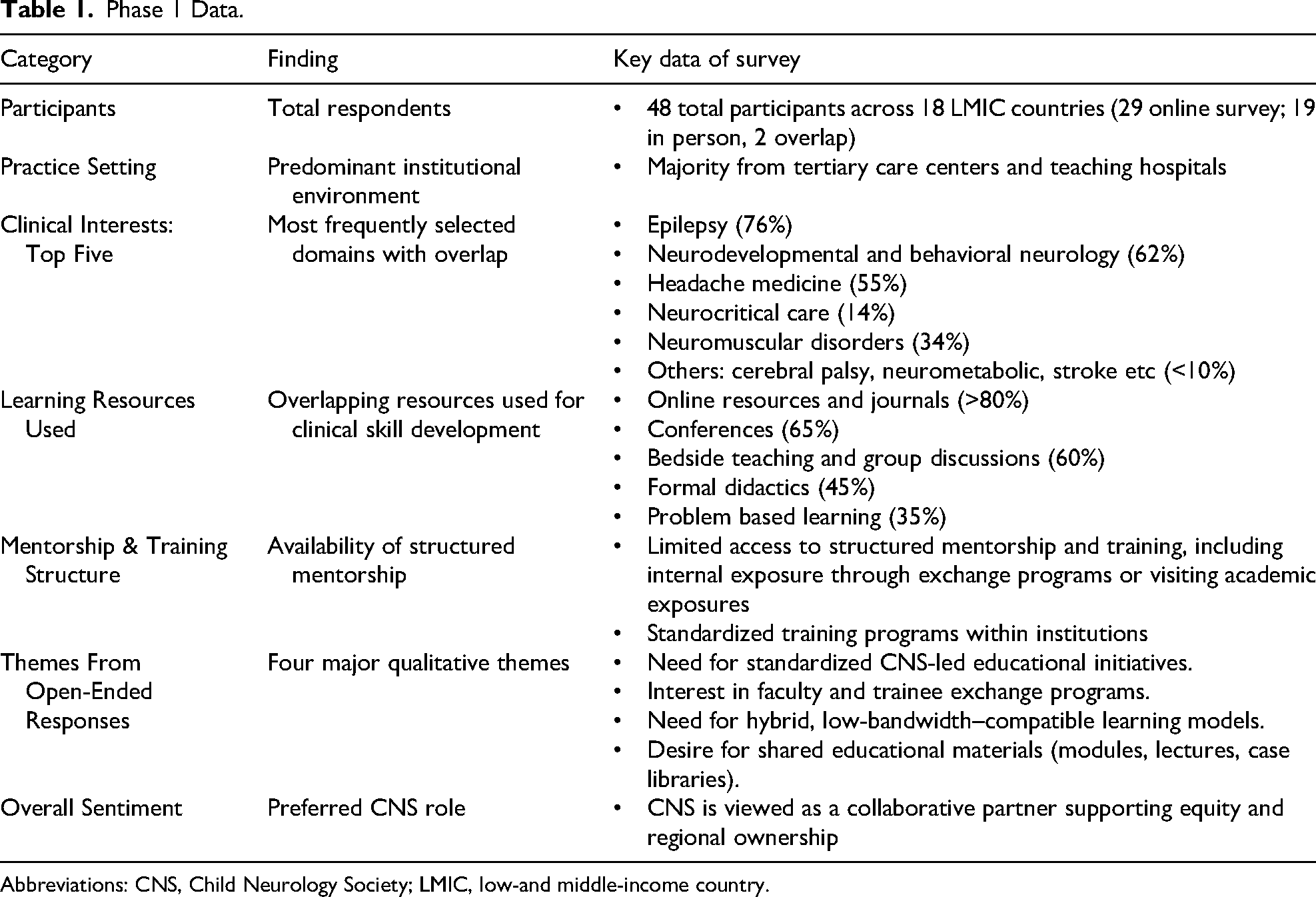
Abbreviations: CNS, Child Neurology Society; LMIC, low-and middle-income country.
Clinical interests
Epilepsy (76%) was the most selected subspecialty interests, followed by neurodevelopmental and behavioral neurology (62%), headache medicine (55%), neuromuscular disorders (34%), and neurocritical care (14%). There was an overlap in subspeciality interests.
Learning resources
Various responses overlapped. More than 80% relied on online resources and journals for clinical learning. Conference participation (65%), bedside teaching and group discussions (60%), formal didactics (45%), and problem-based learning (35%) were also used.
Qualitative themes
There were 4 most common themes.
Need for standardized CNS led educational initiatives Desire for structured mentorship and faculty trainee exchanges Value of hybrid learning accessible in low-bandwidth settings Need for shared educational resources such as case libraries and lecture modules
Participants emphasized CNS's role as a collaborative partner rather than a traditional top-down educator.
Phase 2: SMART Action Planning
During phase 2, a total of 39 participants representing 3 geographic regions engaged in structured SMART action planning sessions at the 2025 CNS Annual Meeting (Table 2). These facilitated discussions built on findings from the 2024 needs assessment and enabled each group to translate regional challenges into measurable goals. The planning process revealed both cross regional priorities shared by all groups and distinct goals tailored to each region's specific context.
SMART Framework.
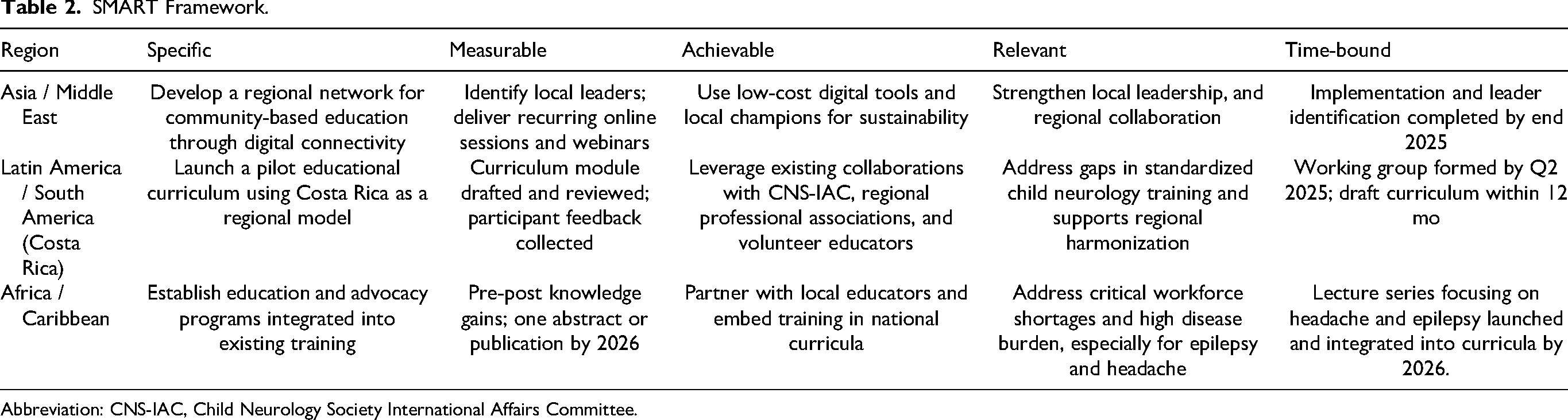
Abbreviation: CNS-IAC, Child Neurology Society International Affairs Committee.
Across all regions, participants emphasized 3 unifying priorities. First, there was consistent interest in developing standardized yet adaptable educational curricula that could be implemented across diverse training environments. Participants highlighted the importance of harmonizing core child neurology content while allowing flexibility to align with local clinical realities, resource levels, and training structures. Second, the need for strengthened leadership development and mentorship infrastructure emerged as a priority across settings. Clinicians identified a desire for sustainable models of mentorship, opportunities for leadership growth, and systems that support trainee development, especially in areas with limited subspecialty expertise. Third, all groups underscored the value of community engagement and sustainable educational implementation, emphasizing programs that build long-term capacity rather than short-term external support.
In addition to these shared themes, each region identified specific priorities shaped by its geopolitical, educational, and workforce landscape. The Latin and South America group selected Costa Rica as a pilot site for developing a regional curriculum model, recognizing its potential to serve as a scalable template for neighboring countries. Participants from the Asia and Middle East region prioritized the creation of digital learning networks, particularly low-bandwidth platforms for case-based discussions and ongoing professional exchange opportunities across geographically dispersed clinicians. The Africa and Caribbean group focused on advocacy and training programs, particularly for front-line general physicians, nurses, and allied health professions, targeting high-burden conditions such as epilepsy, cerebral palsy, neuromuscular disorders, and headache, integrating these efforts into existing local and national training frameworks.
Together, these region-specific goals reflect the diversity of needs across LMIC settings while maintaining alignment with a shared global vision for strengthening child neurology education.
Discussion
This 2-year initiative demonstrates a collaborative and transferable model for global child neurology capacity building within a professional society framework. By integrating data-driven needs assessment with regionally led action planning, the CNS-IAC translated broad educational challenges into concrete, contextually grounded strategies. This approach directly aligns with the priorities outlined in the World Health Organization's Intersectoral Global Action Plan (IGAP), which emphasizes workforce development, improved access to education, strengthened training pathways, and the creation of sustainable international networks. The initiative not only addresses these IGAP pillars but also models how a professional society can serve as a catalytic convener rather than an external direct force.9,10
Our findings also align with and complement existing global child neurology efforts, including the ICNA training surveys and reports. 1 Although ICNA reports have documented gaps in training, infrastructure, and mentorship across LMICs, the current CNS-IAC initiative has further advanced this work, particularly with respect to providing actionable region-specific solutions. The structured SMART framework offered a mechanism to translate needs into measurable goals, allowing each region to tailor its priorities while maintaining alignment with global capacity-building standards. Based on phase 1 work, CNS-IAC has successfully implemented an International Academic Visiting Professor Program at the University of Manitoba, Canada. This program is designed to offer hands-on education and training exposure in neurology (both general and subspeciality exposure) to 1 academic child neurologist from an LMIC per year. By the end of 2025, this new program is expected to host 1 academic child neurologist from Pakistan.
The SMART planning process also mirrors established global health approaches, such as cascade training, mentorship pyramids, and twinning models. 9 Cascade training employs a stepwise dissemination strategy in which content is transferred from experts to regional leaders and subsequently to frontline providers, allowing efficient scale-up while preserving curricular fidelity. The mentorship pyramid model uses a tiered structure in which senior clinicians mentor midlevel providers, who in turn support junior trainees, thereby fostering distributed leadership and sustainable mentorship capacity. Twinning models establish long-term, bidirectional partnerships between institutions in high- and low-resource settings, promoting shared curriculum development, faculty exchange, and durable systems strengthening through equity-based collaboration. These models succeed when they emphasize local ownership, shared decision making, and long-term sustainability, all of which were foundational principles in this project. 9 By centering regional voices and fostering collaborative problem solving, the initiative enabled the development of goals that were realistic, context appropriate, and grounded in the lived realities of clinicians across LMIC settings.
Regional outcomes achieved by this project illustrate how the CNS-IAC model can adapt to diverse needs and infrastructures. In Latin America and South America, the Costa Rica pilot demonstrated the feasibility of standardized curriculum development that can serve as a template for broader regional harmonization. In the Asia and Middle East region, digital learning networks emerged as a scalable solution for connecting geographically dispersed clinicians, leveraging low-bandwidth technology to facilitate case discussions, mentorship, and shared learning. 8 In the Africa and Caribbean region, participants highlighted systemic challenges including workforce shortages and limited training integration. Their resulting strategies focused on embedding neurologic content within existing pediatric and general medical training pathways, demonstrating a context informed approach. This strategy demonstrates contextual ingenuity, transforming barriers into opportunities for sustainable curriculum reform.11,12 However, the outcome data from the SMART goals developed in 2025, including curriculum implementation, number of training sessions, and measurable knowledge gains, are not yet available. Early outcomes are anticipated by late 2026.
Collectively, these regional insights illustrate the strength of a coordinated yet locally empowered model. The CNS-IAC initiative shifts global child neurology collaboration from isolated educational activities toward a more cohesive, multiregional strategy grounded in shared priorities, measurable outcomes, and sustained partnerships. As these SMART goals progress toward implementation, the initiative has the potential to serve as a replicable framework for other professional societies seeking to address global inequities in subspecialty training and clinical capacity. Importantly, clinicians actively practicing in LMIC settings contributed to both phases of the initiative and participated in regional working groups, ensuring that the resulting priorities and SMART goals reflected locally informed perspectives and clinical realities.
Limitations
This project has few limitations. We did not systematically collect detailed demographic information for in-person participants (eg, trainee vs attending status or country-level representation). Future iterations of this initiative will incorporate structured demographic tracking to improve transparency and representation assessment. The survey and meetings were conducted in English, which may have excluded some clinicians and introduced language bias. Participation relied on digital access, potentially underrepresenting clinicians in areas with limited connectivity. The denominator of invited clinicians is unknown, which limits calculation of response rates and introduces nonresponse bias. Participants may not represent the full spectrum of child neurologists within each region. Outcome data from the SMART goals, including curriculum implementation, number of training sessions, and measurable knowledge gains, are planned but not yet available. Early outcomes are anticipated in late 2026. Additionally, reliance on World Bank income classifications may oversimplify the realities of health-related inequities. Countries designated as high income by narrow gross national income thresholds (eg, US$14 000 annually) are categorized alongside nations with significantly higher income levels such as the United Kingdom and the United States. This classification does not account for unique economic pressures, interest rates, or resource constraints faced by Small Island States in the Caribbean and South Pacific. As a result, several health-reserved populations in these regions may be overlooked despite having needs like LMIC settings. 13
Future Directions
Moving forward, several strategic initiatives will be essential to sustaining and expanding the impact of this work across LMIC regions:
Together, these next steps will position the CNS-IAC as a sustained partner in global child neurology education and support long-term capacity building across regions.
Conclusion
This CNS-IAC initiative shows that global child neurology collaboration can be strengthened through intentional and structured engagement. Transitioning from a broad needs assessment to regionally owned SMART action goals created a scalable and replicable model that aligns with international frameworks. Empowering regional leaders fostered ownership, sustainability, and cross-regional learning, positioning the Child Neurology Society as a convener and catalyst for global child neurology capacity building.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738261453469 - Supplemental material for Global Child Neurology Capacity Building Through the Child Neurology Society International Affairs Committee: From Needs Assessment to SMART Action Goals
Supplemental material, sj-docx-1-jcn-10.1177_08830738261453469 for Global Child Neurology Capacity Building Through the Child Neurology Society International Affairs Committee: From Needs Assessment to SMART Action Goals by Sharoon Qaiser, Alcy Torres, Jorge Vidaurre, Maria T. Acosta, Thembi Katangwe-Chirwa, Dave Clark, Soe Mar, Carlos Palomino, Tarif Bakdash and Mubeen F. Rafay in Journal of Child Neurology
Supplemental Material
sj-pdf-2-jcn-10.1177_08830738261453469 - Supplemental material for Global Child Neurology Capacity Building Through the Child Neurology Society International Affairs Committee: From Needs Assessment to SMART Action Goals
Supplemental material, sj-pdf-2-jcn-10.1177_08830738261453469 for Global Child Neurology Capacity Building Through the Child Neurology Society International Affairs Committee: From Needs Assessment to SMART Action Goals by Sharoon Qaiser, Alcy Torres, Jorge Vidaurre, Maria T. Acosta, Thembi Katangwe-Chirwa, Dave Clark, Soe Mar, Carlos Palomino, Tarif Bakdash and Mubeen F. Rafay in Journal of Child Neurology
Footnotes
Acknowledgements
The authors thank the Child Neurology Society and its Child Neurology Society International Affairs Committee for supporting this initiative. We are grateful to the regional working groups for their leadership and to the clinicians whose insights and participation helped shape this project. We also acknowledge the valuable contributions of Andrea Espinoza Herrera, Federico Baltar Yanez, Noor Sabah, and Tipu Sultan to this work. The authors thank Aryeh Qaiser for volunteer assistance with session logistics.
Author Contributions
Maria T Acosta
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Current work for Maria T. Acosta is supported by the intramural NHGRI of the National Institute of Health (NIH). The contribution of the NIH author is considered work of the United States Government. The findings and conclusions presented in this paper are those of the authors and do not necessarily reflect the views of the NIH or the US Department of Health and Human Services.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.