
Abstract
Background
Epilepsy is a common pediatric diagnosis, and recent national and international efforts aim to improve care for neurologic conditions. This study examined initial clinical differences between English- and Spanish-speaking pediatric epilepsy patients.
Methods
We used single-center retrospective analysis of pediatric English- and Spanish-speaking patients with epilepsy. Demographic information was recorded. Initial encounters and subsequent care for the first 6 months were reviewed. Wilcoxon rank sum tests, Fisher exact tests, and multivariable logistic regression were used.
Results
A total of 118 English-speaking and 112 Spanish-speaking patients met the inclusion criteria. Epilepsy classification, presenting seizure type, initial encounter location, medications prescribed, and subjective seizure improvement rates did not differ between language cohorts. Differences between language cohorts were seen in communication rates and medication trials. Some differences were found depending on race within Spanish-speaking populations.
Conclusion
Despite many similarities in care, institutional processes—specifically our triage differences for English- and Spanish-speaking patients—may explain differences in contact rates and medications trials with similar rates of seizure improvement. The intersection of race within Spanish-speaking patients with epilepsy should be explored further.
Epilepsy is a pediatric neurologic disorder with an estimated prevalence of 6.8 per 1000 children. 1 Both global and national initiatives have increasingly focused on expanding access to care and reducing disparities linked to social determinants of health. In 2022, the World Health Organization (WHO) launched the Intersectoral Global Action Plan on Epilepsy and Other Neurological Disorders, to enhance treatment accessibility and improve the quality of life for individuals living with neurologic disorders. 2 Similarly, in 2025, the American Epilepsy Society released the National Plan for Epilepsy, which aims to improve outcomes and reduce socioeconomic and racial barriers for the millions of Americans living with epilepsy. 3 In Colorado, 52% of immigrants are from largely Spanish-speaking, Latin countries. 4 With ongoing shifts in US federal and health care policies, it is important to examine disparities in outcomes for Spanish-speaking patients with epilepsy.5-7
A 2018 review identified several key factors contributing to disparities in epilepsy care for ethnically Latino and non-White patients including fear of treatment, limited access to care, communication barriers, low health literacy, limited education, mistrust of health care systems, and insufficient social support. 8 Subsequent research has further demonstrated several inequities in clinical management, with minority patients experiencing lower rates of antiseizure medication prescriptions, less frequent EEG monitoring, higher hospitalization rates, and reduced access to newer therapies.9-15
These disparities exist beyond initial presentation and are also evident in seizure control and disease remission. In a cohort of 776 pediatric patients, after adjustment for socioeconomic and demographic factors, children of Hispanic ethnicity had a significantly lower likelihood of antiseizure medication responsiveness and longer median time to remission compared with non-Hispanic White counterparts (8 years and 5.6 years, respectively). 16 Furthermore, Hispanic and other ethnic minority groups had significantly lower odds of undergoing epilepsy surgery compared with non-Hispanic White patients, and this disparity persisted even among patients with private insurance. 17
Language barriers further exacerbate these inequities and pose unique challenges that can worsen clinical outcomes and delay care.9,18-21 Prior research has demonstrated that language discordance between patients and providers is associated with reduced communication with the medical team and increased emergency department utilization in both the short (3-7 days) and long term (6 months).12,14 Importantly, the use of verified interpretation services has shown to mitigate some of these disparities. 12
To comprehensively address these gaps, it is essential to examine the FACETS of disparity—fear of treatment, access to care, communication barriers, education, trust between patient and physician, and social support—which collectively shape neurology care for several distinct populations. 8 Specifically, our study sought to investigate the role of communication barriers, treatment bias, and access limitations, recognizing that these factors are interrelated and influenced by broader social and structural determinants encompassed within the FACETS framework.
In this study, the objective was to compare early clinical management and outcomes between Spanish-speaking and English-speaking epilepsy patients in the first 6 months following their initial evaluation by neurology (defined by first face-to-face contact with a neurology clinician).
We hypothesized that outcomes at our center would parallel previously reported findings with Spanish-speaking patients demonstrating greater reliance on emergency services including higher rates of first neurology encounters occurring in the emergency department. 12 We also anticipated increased interval emergency department use between visits, fewer patient-provider communications, different rates of seizures medications prescribed, and lower rates of reported seizure improvement.
Methods
Patient identification occurred through a single-center retrospective analysis of outpatient clinic patients scheduled between December 1, 2023, and December 1, 2024, at our primary hospital campus. Chart review was used to examine their initial epilepsy diagnosis and encounters. Inclusion criteria included clinically confirmed diagnosis of epilepsy and an initial diagnosis occurring at our institution. Our analysis identified Spanish-speaking patients based on the preferred language documented in the electronic medical record. We were unable to determine because of inconsistent social history documentation whether this designation applied uniformly to all household members, whether some patients or caregivers possessed greater English proficiency, or whether the household functioned as bilingual. Patients who completed their initial face-to-face prior to 2008, when our electronic medical record was established, and those diagnosed after 18 years of age were excluded. Patients with febrile seizures only were excluded. If a child was less than 6 years old and had a seizure with a fever as their first presentation but was diagnosed with epilepsy within the following 6 months, they were included in the study. Patients with diagnoses of infantile spasms were excluded, given fundamental differences in both their clinical course and urgency.
A frequency-matched cohort of English-speaking patients (ENG) with epilepsy was selected at random. Specifically, the English-speaking cohort was date-matched to the Spanish group by randomly selecting a patient who received their initial diagnosis on the same calendar day as each of the Spanish-speaking patients (SPAN).
Patient characteristics examined included prior visits in neurology for non-epilepsy concerns (such as developmental delay or abnormal movements), presenting seizure type (convulsion, focal, absence, or other), and epilepsy classification if known and declared in the first 6 months.
Recognizing that Latinos and Hispanic populations encompass a wide range of racial identities, we examined differences based both on ethnicity and race. Given the available classifications in our electronic medical record system and the scope or analysis, ethnicity was divided into 2 broad groups, Hispanic or non-Hispanic, and race was categorized as White/Caucasian and Non-White/Caucasian. 22
The location (emergency department or outpatient neurology clinic including satellite locations) of the first face-to-face encounter with neurology was assessed, timing of antiseizure medication initiation (before the first face-to-face with neurology, at the first face-to-face with neurology, or after the first face-to-face with neurology) as well as the type of medication selected (or lack thereof). The data collection also included whether rescue medication was prescribed and which medication was prescribed. We recorded whether a follow-up face-to-face (clinic visit or in-person face-to-face via the emergency department or admission) was completed and the duration (in days) between the first and second face-to-face neurology encounters.
The number of contacts (totaling both phone calls and secure electronic health messages) with neurology clinicians and nurses was collected between the first and second face-to-face neurology encounters as well as the topic for the contacts separated into several categories: more seizures or possible seizures, medication side effects, difficulty obtaining medications, or seizure school plan needs. Phone calls included those that were patient initiated or clinician initiated (such as primary care provider or emergency department clinician). Communications with schedulers were not considered a contact because it did not directly change clinical management at that time but communication with nurses and direct electronic messages to providers were considered contacts. Documented communication between providers about patient care, for example, from the primary care provider to the neurologist on call, were considered contacts because they often resulted in immediate effects on clinical care.
Logistical regression was used to compare the difference in contact topics when controlling contact rates. Admissions or emergency department visits at our hospital or outside hospitals between the two face-to-face encounters were collected. If a child went to the emergency department at our institution but neurology was not asked to consult and evaluate the patient, this would not count toward a face-to-face encounter.
Outcomes included subjective seizure improvement, defined as >50% seizure reduction in seizure frequency as reported by caregivers at the second face-to-face. Improvement was characterized as either no seizures since the previous visit or a clinically estimated reduction of more than 50% based on parental report, clinical history, and chart documentation. Sex (assigned at birth) was also recorded.
We also recorded the total number and locations (outpatient neurology clinic or emergency department/hospital admission) of face-to-face encounters in the first 6 months following diagnosis. Finally, we examined the total number of antiseizure medication trials in the first 6 months.
Study data were collected and managed using REDCap electronic data capture tools hosted at University of Colorado Health Sciences REDCap (Research Electronic Data Capture). 23
This study received ethical approval from the Colorado Multiple Review Board (COMIRB) (approval no. 24-0309). All patient information was deidentified and did not require patient consent.
Statistical Methods
Data were summarized using medians (IQRs) for continuous variables and counts (percentages) for categorical variables. Medians (IQRs) were used to summarize variables based on whether a variable was normally distributed or not. Since the Shapiro-Wilks tests showed non-normality, we show median (IQR) because it is a better measure of central tendency. Comparisons between English- and Spanish-speaking patients were made using Wilcoxon rank sum tests (continuous variables) or Fisher exact tests (categorical variables). Multivariable logistic regression models were developed to assess the relationship between independent variables of interest with the outcome after adjusting for confounding variables. All P values were 2-sided and a P value less than .05 was considered statistically significant. All analyses were evaluated using R-4.5.1 (The R Foundation for Statistical Computing).
Results
Demographic Results
One hundred twenty patients were identified for inclusion in each of the English-speaking (ENG) and Spanish-speaking (SPAN) groups. After removing patients diagnosed with infantile spasms, there were 112 patients remaining in the ENG group and 118 in the SPAN group. Patients in the SPAN group were more likely to have home addresses in Colorado. Although not significant, there was a trend in younger age at presentation for ENG patients (P = .082). Median age at initial visit was 4.9 (2.4, 8.5) for ENG patients and 7.3 (1.7, 11.7) for SPAN patients. ENG patients were more likely to be female (P = .047). Eighty percent of ENG and 51% of SPAN cohorts identified as White/Caucasian. Ethnically, 98% of the SPAN and 31% of the ENG cohorts identified as Hispanic or Latino (Table 1).
Demographic Descriptions.
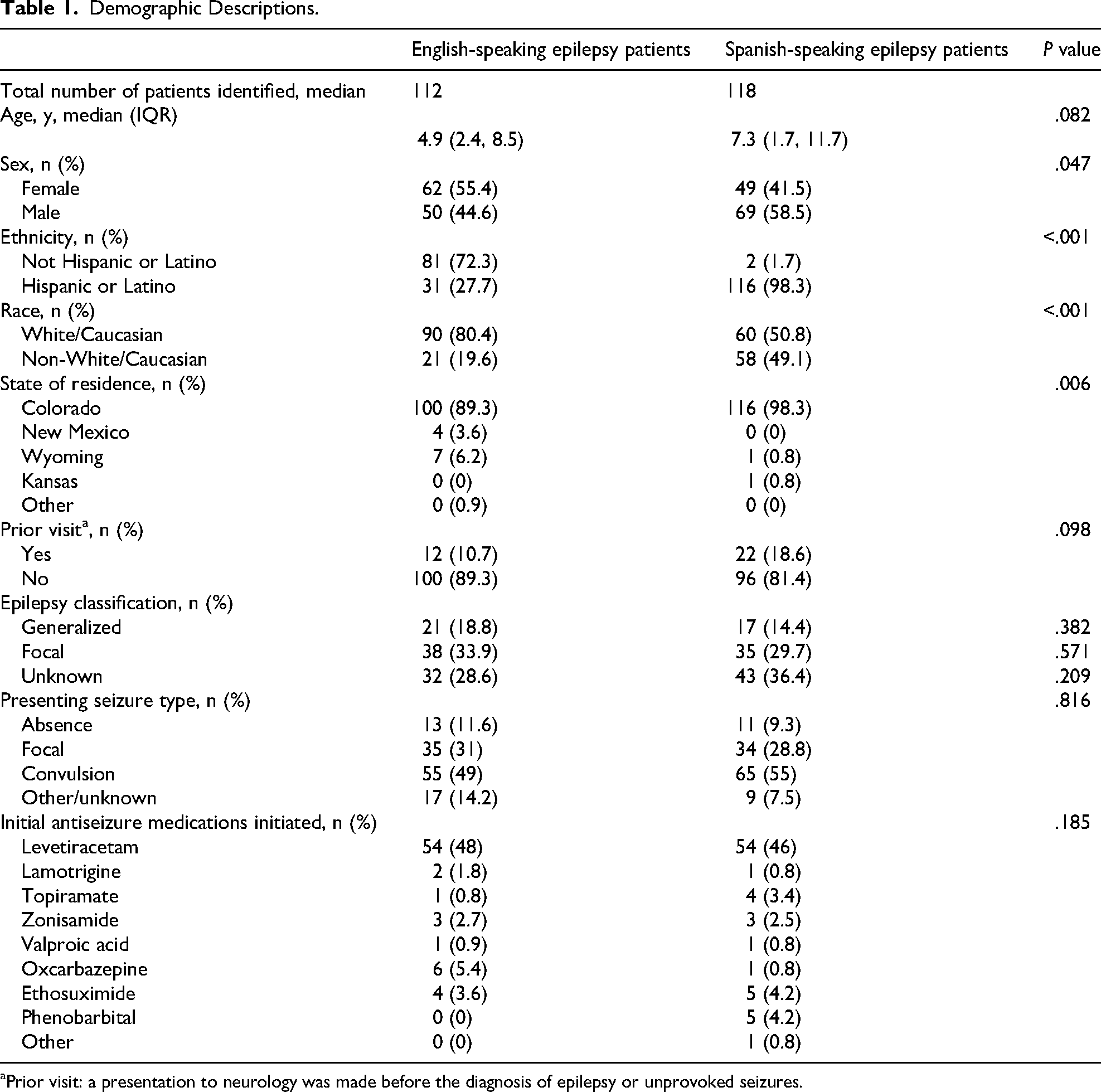
Prior visit: a presentation to neurology was made before the diagnosis of epilepsy or unprovoked seizures.
Eleven percent and 18.6% of ENG and SPAN patients, respectively, had been seen previously in the neurology clinic with chief complaints other than epilepsy, and the difference between the 2 groups was not significant (P = .098). Sixty percent of the chief complaints for both cohorts at those visits was developmental delay, with the remaining comprising a mixture of spells, febrile seizures, or “other” (such as abnormal movements, incidental abnormal imaging findings, etc). There was no difference in chief complaints between the language cohorts (P = 1.00) (Table 1).
There was no significant difference between the epilepsy classification nor the difference in seizure type at presentation between the language cohorts. When examining data based on race, non-White/Caucasians were more likely to have a classification of focal epilepsy (P = .037). There was no difference in epilepsy classification by ethnicity (generalized: P = .855; focal epilepsy: P = .187; and unknown: P = .384) (Table 2).
Epilepsy Classification by Race and Ethnicity.
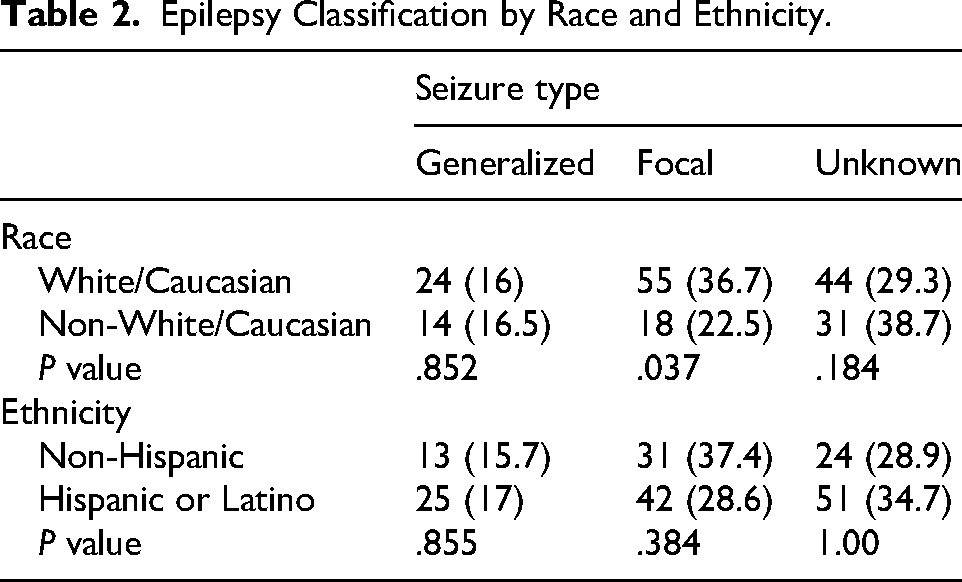
There was no difference in presenting seizure type between language cohorts (P = .816). Neither ethnicity nor race varied with the presenting seizure type (P = .305 and P = .099, respectively).
There were also no differences in the selection of initial antiseizure medications between language cohorts (P = .185) (Table 1).
Neither race nor ethnicity differed based on medication selection (P = .488 and P = .783, respectively).
Initial Clinical Presentation
Seventy-two percent of ENG and 65% of SPAN were first evaluated for a chief complaint of seizures in an outpatient neurology clinic. The remaining 28% of ENG and 35% of SPAN patients were first evaluated for seizures in the emergency department (ED) or hospital admission. There was no statistical difference between the language cohorts (P = .259). When assessing this difference based on race and ethnicity, there were also no significant differences (P = .161 and P = .400, respectively).
Notably, there was no difference between language cohorts as to whether an antiseizure medication was initiated at the first face-to-face encounter (41% ENG, 43% SPAN; P = .608). There was also no difference in antiseizure medication initiation as it pertained to either ethnicity and race (P = .812 and P = .402, respectively).
In 13.4% and 13.6% of ENG patients and SPAN patients, respectively, the patients were started on medications by primary care physicians (PCPs) or from the emergency department, and these were continued at the first face-to-face encounter. In a small number of ENG epilepsy patients and SPAN patients (3.6% and 0.8%, respectively), a previously prescribed medication that was started before the first face-to-face neurology evaluation was stopped after evaluation by neurology.
If medications were not started at the initial face-to-face with neurology, there was no significant difference between when antiseizure medications were subsequently prescribed between language cohorts (P = .77). Seven percent of ENG patients and 11% of SPAN patients started antiseizure medications through the emergency department after the first face-to-face encounter with neurology. Seven percent of ENG patients and 8% of SPAN patients initiated antiseizure medications at the second face-to-face encounter with neurology. Eight percent of each language cohort started antiseizure medications sometime after the second face-to-face encounter.
Treatment Trials
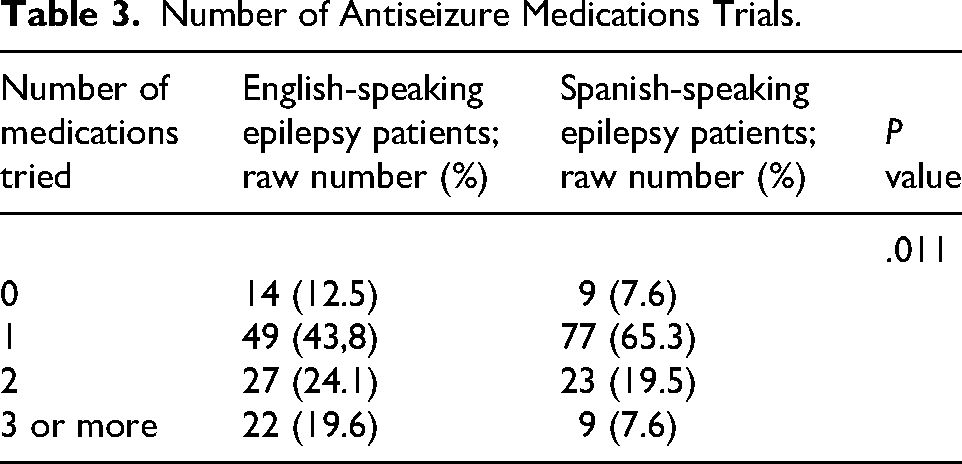
There was a statistical difference between ENG and SPAN patients’ treatment trials in the first 6 months, in that ENG patients were more likely to have trialed more antiseizure medications than SPAN patients (P = .011) (Table 3).
Number of Antiseizure Medications Trials.
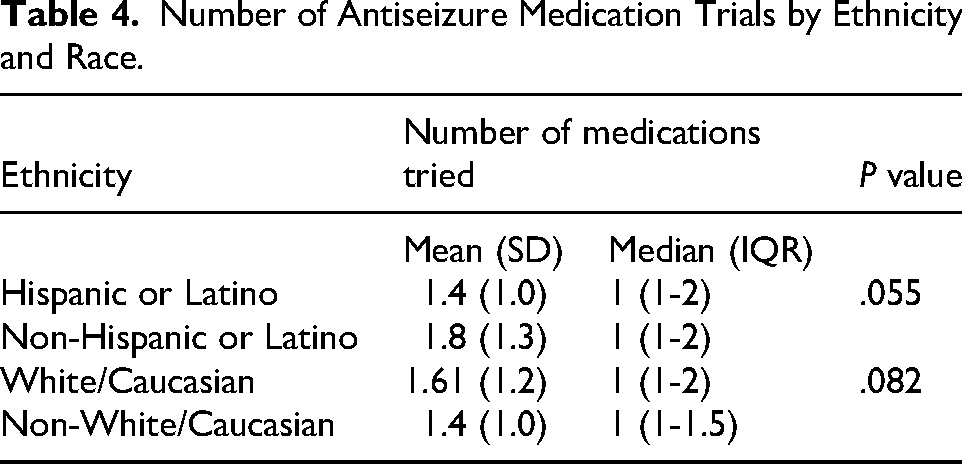
When assessing differences by race, there was no difference in treatment trials in the first 6 months (P = .082) although there was a trend of ethnically non-Hispanic patients to try a higher number of medications (P = .055) (Table 4).
Number of Antiseizure Medication Trials by Ethnicity and Race.
Rescue Medications
There was no difference between the ENG (84%) and SPAN patients (77%) with respect to rescue medication prescription rates (P = .115). Additionally, there was no difference in rescue medication prescription rates depending on race or ethnicity (P = .230 and P = .178). There was no difference in the route (nasal, rectal, buccal) of the rescue medication prescription between the language cohorts although there was a trend toward reduced rectal diazepam prescriptions in SPAN patients (P = .070).
Follow-up Clinical Experience
There was no difference in frequency of second face-to-face encounters between ENG and SPAN patients (100% ENG, 98% SPAN; P = .25). When assessing this difference based on race and ethnicity, there were still no significant differences (P = .200 and P = .297, respectively). The number of face-to-face encounters completed after the first face-to-face in the first 6 months was not different between the language cohorts either (P = .437). Additionally, the location of the subsequent second, third, and fourth face-to-face encounters occurring in the first 6 months was not significantly different between the language cohorts (P = .106, P = .861, P = .677, respectively).
Furthermore, time to the second face-to-face was not significant between ENG and SPAN cohorts (P = .66) (Table 5).
Number of Face-to-Face Encounters Following the First Face-to-Face in the First 6 Months; Time Between First and Second Face-to-Face Encounter.
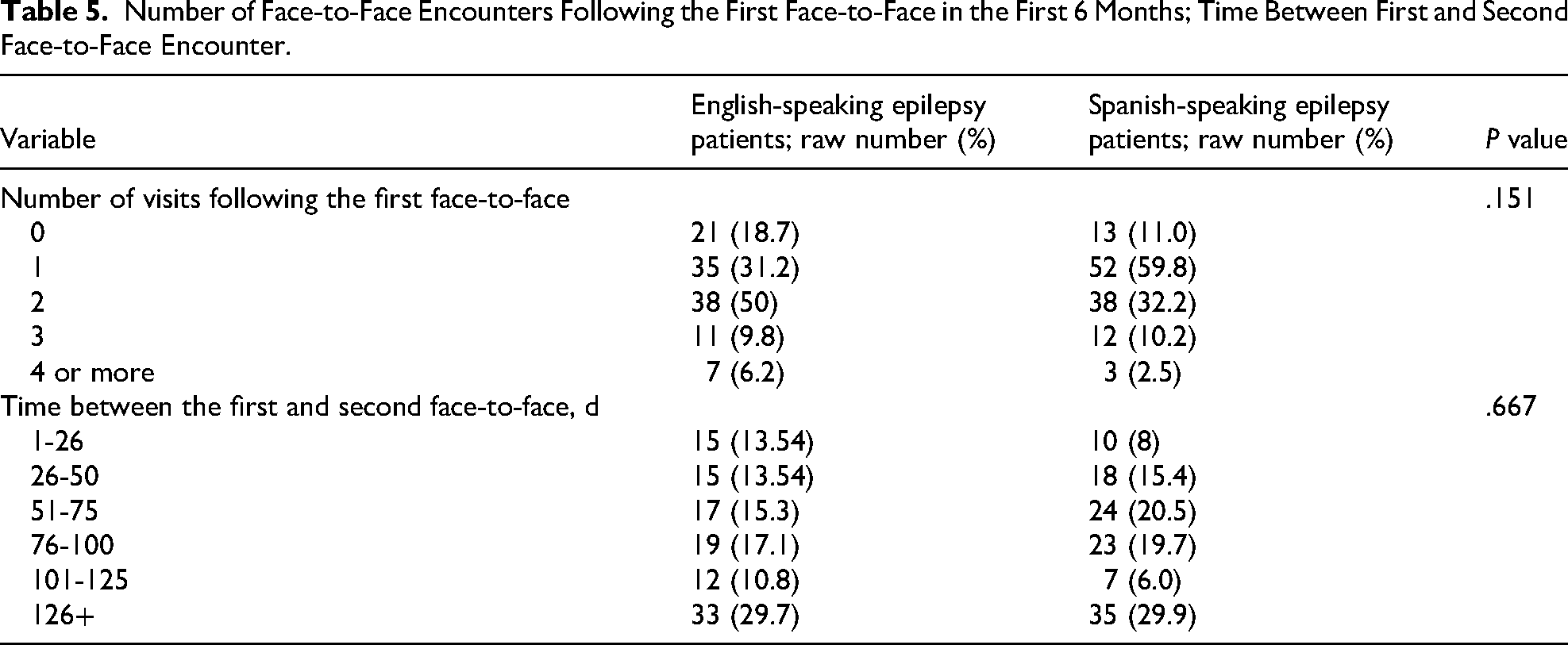
The rate at which patients reported seizure improvement greater than 50% at the second face-to-face with neurology was not different between the language cohorts (P = .105), with 40.5% of ENG and 54% of SPAN patients reporting improvement. Additionally, there were no differences when assessing seizure outcomes based on race (P = .092), although there was a trend for ethnically Hispanic/Latino patients to report seizure improvement (P = .060).
Using logistical regression models to examine the entire study sample, the odds are 2 times higher for a patient to have >50% reduction in seizures if they have fewer than 6 contacts (P = .0284). Furthermore, we found that higher rates of medication trials was associated with a lesser chance of seizures improvement rate >50% (P = .0482).
Thirty-eight percent and 39% of ENG and SPAN patients, respectively, were seen in the emergency department between the first and second face-to-face with neurology, which was not significant between the language cohorts (P = .164). Differences in emergency department visits was not impacted by race or ethnicity (P = .0.161 and P = .459, respectively). For those with an emergency department visit between the first and second face-to-face encounters, there was no difference in the rate of chief complaint for that encounter (26.8% for ENG and 35.6% for SPAN, P = .158).
Communications With Neurology Clinical Staff
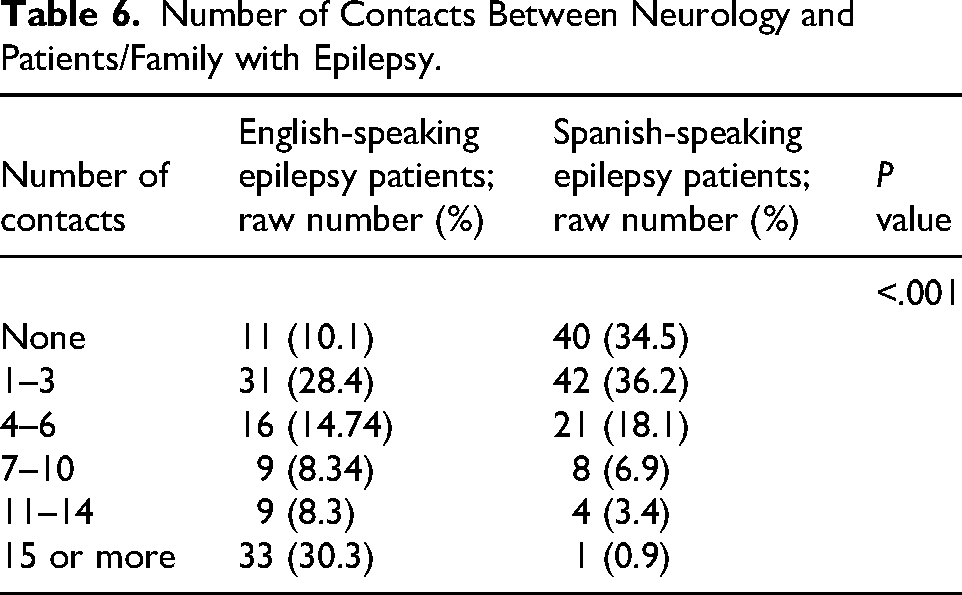
Notable differences were seen in the frequency of contacts with the neurology clinic between the first and second face-to-face neurology encounters between language cohorts (Table 6) (P ≤ .001). Contacts did not differ by race or ethnicity (P = .390 and P = 1.00, respectively).
Number of Contacts Between Neurology and Patients/Family with Epilepsy.
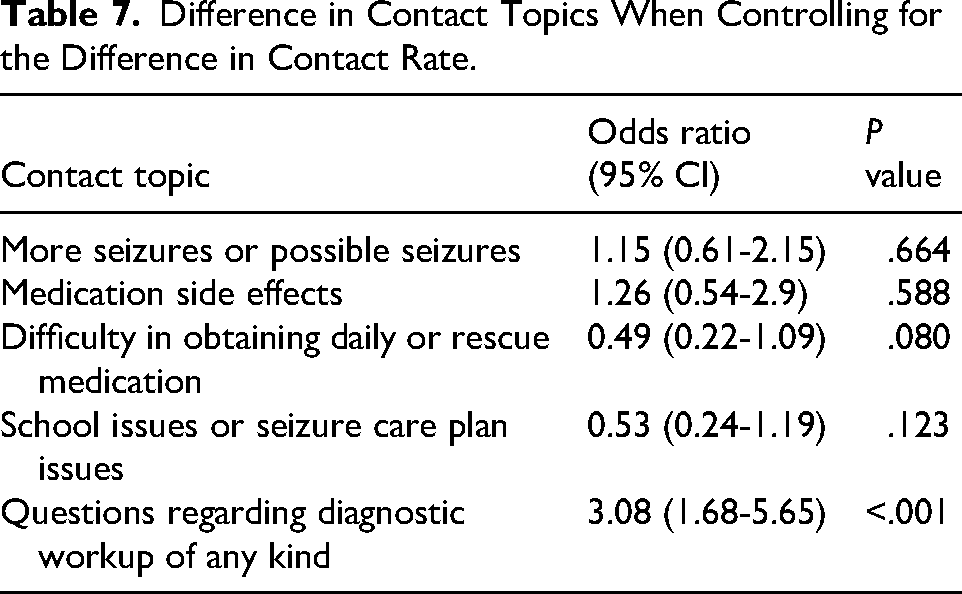
After developing a logistical regression model to examine whether there was a difference in the reasons for contacting the Neurology department between the language cohorts, the odds of questions regarding their diagnostic evaluation of any kind coming from ENG patients were 3 times higher than coming from SPAN patients. No other reason for contact was statistically significant after adjustment for the number of contacts (Table 7).
Difference in Contact Topics When Controlling for the Difference in Contact Rate.
Discussion
Overall Statement
Our study showed many similarities in clinical care between English-speaking patients and Spanish-speaking patients newly diagnosed with epilepsy with respect to location of face-to-face evaluation, medication types, early emergency department visits/hospital admissions, medication initiation rates, number of follow-up encounters, and subjective seizure outcomes. However, there are differences in the rates of communication and number of medication trials in the first 6 months of treatment between English-speaking and Spanish-speaking patients with newly diagnosed epilepsy. Many differences may be impacted by our institution's phone call triage protocol as described in the discussion. Furthermore, our study identified only a limited number of differences in presentation and outcomes across racial and ethnic groups; however, these findings carry important real world clinical implications. In many ways, our study supports the FACETS framework in naming gaps in care. 8
Demographic, Previous Visits, and Presentation Similarities
A lack of difference between language cohorts as to whether they had been seen in neurology before their diagnosis of epilepsy could reflect similar levels of access to care. However, the fact that Spanish-speaking epilepsy patients were more likely to live in Colorado as opposed to out of state and trended toward being older at presentation suggests transportation and other potential factors could be barriers to initiating care such as increased reliance on more local rural facilities. Using the FACETS framework, this exemplifies disparities in access and communication. Furthermore, this is consistent with prior research showing patient care differing based on transportation in non–English-speaking patients.8,24,25 The social support domain of the FACETS model may also be relevant because obtaining care out of state often depends on substantial social support to facilitate caregiving of children and other dependents.
Sex differences were peculiar and could be related to the age differences seen between cohorts assuming certain sex-related disorder may present at different ages or could be attributed to the sample size.
The finding that epilepsy classification and seizure types were similar between language cohorts and based on ethnicity yet differed by race was particularly noteworthy. These differences may reflect racial differences such as clinician bias, decreased rate of diagnostic studies or could be attributable to the study's limited sample size. Incorrect or delay in clarification of epilepsy diagnosis could lead to disparities in outcome or increased time to certain interventions.26,27 Prior research has shown that health outcomes differ based on race within Spanish-speaking populations, and this intersection should be further explored as it pertains to pediatric epilepsy care. 28
Although prior data have shown Spanish-speaking patients tend to use emergency and urgent care facilities at a higher rate, there was no difference in the initial encounter location for the diagnosis of epilepsy, nor was there a difference in emergency department visits between the first and second face-to-face encounter with neurology.12,24,25 The difference, again, could be related to residence differences or age trends in that younger patients may be seen as clinically more acute.
Similarities in Initial Treatment Management
The comparable rates of medication initiation and similarity in medication selections across language, racial, and ethnic cohorts suggest a consistent standard of care within our center. This finding contrasts with prior research showing decreased use of newer-generation antiseizure medications as well as less participation in antiseizure medication trials for non-White Hispanic population.10,29 It was curious, however, that all the patients treated with phenobarbital were Spanish-speaking, which may reflect a difference in presenting epilepsy severity, differences in medication accessibility in different countries, clinician bias, or possibly economic disadvantage given the affordability of this medication.
Significant Differences in Follow-up and Communications
The duration between the first and second face-to-face encounters was not significantly different between the language cohorts, nor was the total number of face-to-face encounters with neurology in the first 6 months, which differs from prior research showing decreased appointments completed and increase in missed clinical appointments in non–English-speaking patients. 29 This may reflect the observed trend toward younger age at presentation among English-speaking patients, assuming potential increase in acuity in younger patients. However, the significant difference in communication frequency, with English-speaking patients participating in more communication with neurology staff, is consistent with prior research demonstrating that language discordance impacts the care of non–English-speaking families. This finding also illustrates the communication domain of the FACETS framework.14,20,26,27,30,31
Communications were likely impacted by our institution’s protocol of Spanish-speaking schedulers answering calls from Spanish-speaking families with an option to transfer to language-concordant nurses if needed, whereas English-speaking family calls are triaged by neurology nurses first.
It was beyond the scope of this study to investigate the type of clinician with whom our patients followed. Given the lack of clinic availability for our institutions’ epileptologists, our Spanish-speaking epilepsy patients may be followed by epileptologists at a lesser rate than English-speaking patients.9,26 If this were the case, it could reflect scheduling bias, referral bias, or more severe epilepsy in English-speaking patients in this cohort. This should be investigated further.
When examining communication topics alone, English-speaking epilepsy patients are 3 times more likely to inquire about diagnostic workup than Spanish-speaking epilepsy patients, which is consistent with previous research suggesting a higher rate of deference to clinicians in many Latin cultures or a lack of rapport to the health care provider secondary to language barriers.32-34 Alternatively this could suggest limited health literacy or a hesitancy to contact providers due to perceived language barriers. 35 Approaching this again from the FACETS model, these findings align with the physician trust or education disparities highlighted in this framework.
Although there were systems in place at our institution to support multiple languages such as phone interpreters, Spanish-speaking nurses, and translation services available for electronic messaging, it is unclear if patients are aware of these systems and how comfortable they feel navigating them, which aligns with the education disparity of FACETS. Culturally, society has entered a period of rapid advancement driven by artificial intelligence, with emerging data supporting its positive reception. It is anticipated that continued technological innovation will further reduce communication barriers and promote equitable health care delivery.36,37 Although security and privacy concerns are still being navigated as well as ensuring accuracy of these tools, we must continue to use and promote all currently available translation services available in our individual health care facilities.
Total Antiseizure Medication Trials and Seizure Outcomes
The increased number of medication trials in the first 6 months by the English-speaking epilepsy patients was not surprising given the higher rates of communications between visits. However, the comparable seizure outcomes, despite the large differences in communication rates, suggest that increased communications did not impact outcomes between language cohorts. Increasing contacts was inversely related to subjective seizure outcomes, but given similar subjective seizure rates between language cohorts, this does not suggest a difference in epilepsy severity between cohorts. Furthermore, subjective seizure improvement is not a reliable measure given the aforementioned lack of rapport with language-discordant providers and deference to medical providers commonly seen in Spanish-speaking communities.32-34
Further research into the benefit of increased communications with providers is needed given increasing clinician burnout with electronic health message in medical practice.38-41 Moreover, prior research suggests increasing medication changes results in adverse patient outcomes, and our study suggests increasing medications trials are inversely related to subjective seizure improvement rates.42-44 These factors should result in clinical practice changes for neurology practices to reduce frequent medication changes.
Limitations
This was a retrospective chart review and therefore the reasons and perceptions behind the findings could not be explored. These findings represent the care provided at a single institution that covers a large geographic region, and the generalizability is not clear as institution policies and populations differ. As an example, our department policy for incoming calls for English-speaking patients is initial triaging by a clinical nurse. Conversely, our Spanish-speaking epilepsy patients initially speak with schedulers, and if clinical questions exist, they are connected to nurses.
Although our date-matching could result in improved consistency of medical provider population as well as consistency of medication availability, it could be influenced by scheduling preferences and/or provider work weeks and availability.
The scope of this study did not capture the utilization of public vs private transportation or hospital assistance in fuel reimbursement, which may have affected our similarities seen in location of initial visits. Additionally, it was beyond the scope to assess no-show rates, same day cancellations and late arrivals, which could reveal access to care disparities.
It was also beyond our scope to assess the rate at which emergency department providers called our hospital's on-call neurology provider for input on these neurology patients, which could reveal clinician bias between cohorts if assessed.
Given the sample size and limited options for a selection of race identification in our electronic medical record, we opted to assess racial outcomes along White/Caucasian and non-White/Caucasian differences. The intersectionality of race within Spanish-speaking populations requires further exploration.
Additionally, neurology does not complete emergent in-person consultations at our institution’s satellite emergency departments; thus, if they presented to the emergency department at a satellite location and neurology was called for input, this would be considered a phone call and emergency department visit but would not be characterized as a face-to-face visit with neurology. If that patient was transferred for admission and seen by neurologists during the admission, this would count as a face-to-face encounter. We did not differentiate patient-initiated calls from outside clinician-initiated calls, which may have impacted results, and this should be investigated in future studies.
As our study was retrospective, we are unable to determine insurance coverage at the time of their visit. As such, our study did not account for financial or insurance status to assess if differences existed between the 2 cohorts when accounting for socioeconomic status. Additionally, our electronic medical records reflect only current addresses, not past addresses, so disparities in income could not be assessed based on county of residence.
This was a retrospective cohort study including patient encounters dating back to 2008, and complete records of all Spanish-translator certification clinical staff are unavailable. We were unable to determine the impact of Spanish-speaking staff on the clinical care over such an amount of time.
Conclusion
Although our institution identified many similarities in care between language cohorts, this may likely be attributed to our policy of English-speaking epilepsy patient calls being triaged by neurology nurses and Spanish-speaking epilepsy patients calls going first to scheduling. This may also affect the large differences seen in total contacts and medication trials. Although it was encouraging to see many similarities, our institution, like many institutions, should continue to optimize technology and other resources to increase accessibility of equitable forms of communication and accessible health care. Many results of this study support the FACETS framework of disparities, namely, communication and access to care, which highlights the applicability of this model. Further exploration of the intersection of race within the Spanish-speaking population should be explored further in patients with epilepsy. With increasing limitations on federal support for medicine, creative solutions are needed to avoid adverse health outcomes especially for marginalized patient populations.
Footnotes
Acknowledgements
All research was done at Children's Hospital Colorado. This has not been previously presented, and artificial intelligence was not used in crafting this publication.
Author Contributions
Stillman Made a significant contribution to the concept, design, acquisition, analysis and interpretation of data Drafted the article or revised it critically for important intellectual content Approved the final version of the article for publication Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity Knupp: Made a significant contribution to the concept, design, analysis and interpretation of data Revised article critically for important intellectual content Approved the final version of the article for publication Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity Eschbach: Made significant contribution to the analysis and interpretation of data Revised article critically for important intellectual content Approved the final version of the article for publication Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity Patterson: Made significant contribution to the concept and design, analysis and interpretation of data Revised article critically for important intellectual content Approved the final version of the article for publication Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity Berrios-Siervo Made significant contribution to interpretation of data Revised article critically for important intellectual content Approved the final version of the article for publication Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity Silveira: Made significant contribution to analysis of and interpretation of data Revised article critically for important intellectual content Approved the final version of the article for publication Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Potential Conflicts of Interest
Kelly Knupp receives funding from UCB, Stoke, Encoded, Longboard/Lundbeck; consulting funding from UCB, Stoke, Encoded, Longboard/Lundbeck; funding from The Epilepsy Study Consortium; and sits on a DSMB for Harmony therapeutics.
All other authors have no conflicting funding to disclose.