
Abstract
This case-control study assessed symptom severity and prevalence of obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and autism spectrum disorder (ASD) in children attending a headache clinic compared to controls. We included 343 patients (5-19 years) and 130 controls (6-19 years; no prior headache diagnosis/medical contact for headache) between October 2018 and January 2024. Controls were divided into CH+ (experiencing headaches) and CH– (headache-free). Severity was assessed using scores from questionnaires, and prevalence was defined by prior diagnosis or symptom scores above clinical cutoffs, therefore indicating symptom burden over confirmed diagnoses. Patients had more severe symptoms of OCD, ADHD, and ASD than CH–. CH+ had the most severe symptoms of OCD and ADHD. OCD, ADHD, and ASD research diagnoses were present in 20.8%, 17.3%, and 10.1% in patients; 27.8%, 18.8%, and 4.4% in CH+; 1.7%, 7.0%, and 1.8% in CH–. Headache in youth, even in non-clinical settings, is linked to psychiatric symptoms; hence, routine screening is recommended.
Keywords
Headache symptoms and primary headache diagnoses are linked to psychiatric and neurodevelopmental disorders. The association between migraine and anxiety/depression in children and adolescents is well established. 1 However, evidence for a link between headache and obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and autism-spectrum disorder (ASD) is limited.
Adult studies suggest comorbidity between OCD and migraine, particularly chronic migraine and medication overuse headache.2-6 In children and adolescents, the presence of OCD in children with headache has been examined in 2 studies.7,8 One found obsessive-compulsive symptoms to be equally prevalent in patients receiving care for headaches in a pediatric outpatient clinic and in children from the background population with headaches who had not sought help in managing their symptoms. 7 For both groups, OCD was more prevalent compared to controls without headache. 7 Another study found no increased prevalence of OCD in children with primary headache disorders compared to controls but observed higher prevalence in children with migraine than in children with tension-type headache (TTH). 8
Meta-analyses suggests an association between headache and both ADHD and ASD in children and adolescents.9-11 However, most studies have examined children with ADHD and ASD, and not headache, as their primary diagnosis.9-11 ADHD has been most strongly associated to migraine or headache in general, and not to TTH.9,10 Although children with ASD have been shown to have higher odds of experiencing migraine/headaches than controls, 11 symptoms of ASD in children with headache disorders as their primary concern has not previously been investigated.
The causal relationship between psychiatric disorders and headache in childhood is unclear, but likely bidirectional: headache may be a symptom of an underlying psychiatric disorder, as seeking care for headache has been hypothesized to precede ASD diagnosis, 12 or headaches can cause symptoms resembling psychiatric disorders, such as attention deficit. 13 They also co-occur, with evidence of a synergistic effect, as in adults where OCD symptoms increase with migraine frequency. 4 Lastly, a shared pathophysiological link between headache (primarily migraine) and all 3 conditions has been suggested.14-18
In the present study, we compared children and adolescents referred to a headache outpatient clinic with a control group drawn from the general population. Controls were not allowed to have a headache disorder or receive medical attention for headaches. However, because headache is highly prevalent in this age group—with Danish studies showing that up to 95% experience headache and 58% to 67% more report headache within the past 2 weeks19,20—controls were not required to be completely headache-free.
To better explore the relationship between headache and psychiatric comorbidity, we divided the control group into 2 subgroups based on headache frequency: those with headaches (at least 1 headache in the past month) and those who were headache-free (no headaches in the past month). These groups we simply called controls with headache and headache-free controls. This allowed us to investigate whether psychiatric comorbidity is specific to children with a primary headache disorder, which might support a shared pathophysiology, or whether similar patterns are also present in children from the general population who experience headaches but have not sought help in managing their headaches, suggesting a broader or more complex relationship.
Identifying psychiatric comorbidities in children and adolescents with headaches is crucial, as these conditions may represent underlying causes or contributing factors to the headache itself. Early recognition and treatment of psychiatric comorbidities may therefore not only improve overall well-being but also address the root cause of the headache in some cases. Moreover, increased awareness of these associations may support the implementation of routine screening for these psychiatric comorbidities in children presenting with headaches, enabling early identification and intervention.
The primary aim of the study was to assess the prevalence and symptom severity of OCD, ADHD, and ASD in children and adolescents attending a headache outpatient clinic compared to controls with and without headache. Our secondary aim was to investigate the association between headache frequency and the symptom severity of these disorders.
Materials and Methods
This case-control study is outlined in Figure 1. Patients were recruited from the Headache Outpatient Clinic, Department of Pediatrics and Adolescents, Copenhagen University Hospital–Herlev and Gentofte, Denmark (“the clinic”), between October 2018 and April 2021. Patients were recruited through 2 approaches: (1) data collection in the clinic and (2) participation in a clinical research project. Inclusion criteria for both approaches were being a patient at the clinic, aged 5-19 years, and having sufficient proficiency in Danish to complete questionnaires. Symptom severity and research diagnosis of the conditions were based on screening instruments and prior diagnosis of the conditions.
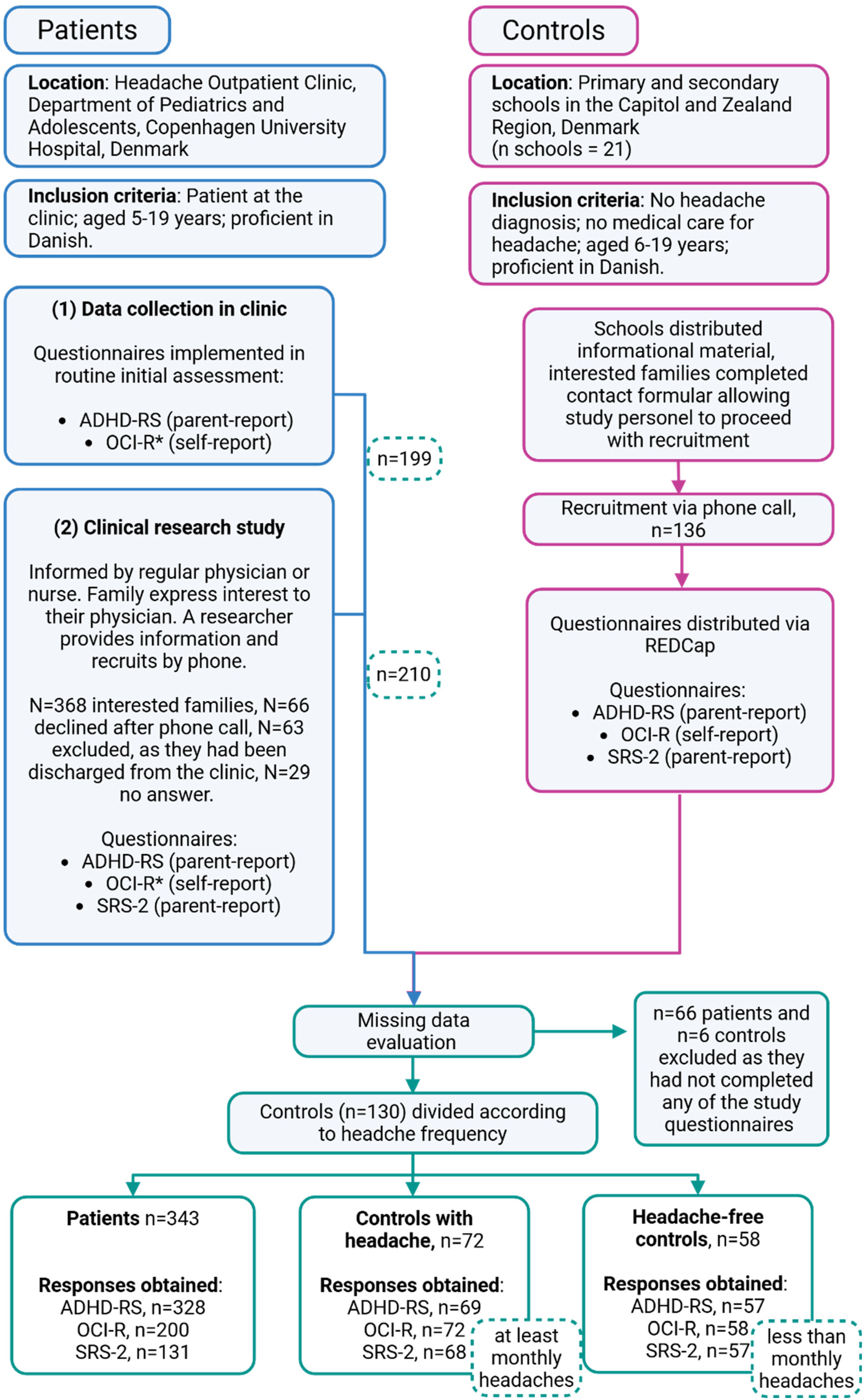
Study flow outlining methods, recruitment, missing data evaluation, and inclusion process. Figure 1 outlines key elements of the study design, including recruitment, inclusion, and sample sizes of the responses obtained. ADHD-RS, Attention-Deficit Hyperactivity Disorder Rating Scale Extended; OCI-R, Obsessive-Compulsive Inventory–Revised; REDCap, Research Electronic Data Capture tool; SRS-2, Social Responsiveness Scale 2. *See text for explanation.
In October 2018, the Attention-Deficit/Hyperactivity Disorder Rating Scale–Extended Version (ADHD-RS) was implemented in the clinic's routine initial assessment along with other questionnaires. All newly referred patients received this questionnaire on paper at their first visit as part of standard care. The completed questionnaire was scanned to the patient's medical record. We chose the questionnaires suitable for implementation based on the following rationale: there should be a limited number of questionnaires administered to avoid overwhelming the family; shorter questionnaires were favored 21 ; and each questionnaire was expected to provide a clinical benefit, specifically, by addressing the expected association between headache and ADHD.
From April 2019, patients had the option of participating in a clinical research project. Beyond the questionnaires distributed as standard care, this included the Obsessive-Compulsive Inventory–Revised (OCI-R) and the Social Responsiveness Scale–Second Edition (SRS-2). Patients were informed of the project by their regular physician and, if interested, were recruited by a researcher over phone (Figure 1). They completed questionnaires using Research Electronic Data Capture tool (REDCap).22,23
In February 2020, we conducted an interim analysis in the clinical research project showing a high prevalence of obsessive-compulsive symptoms. Screening for OCD proved to be highly clinically relevant, and therefore, OCI-R was subsequently incorporated into standard care along with ADHD-RS.
Data were collected through these 2 approaches until April 2021. Hereafter, the medical records of all patients who had attended the clinic from October 2018 to April 2021 (N = 800) were reviewed. Patients who had completed at least 1 of the mentioned questionnaires were identified and included in the final patient sample, along with all patients who had completed one of the questionnaires as part of the clinical research project. Because inclusion required completion of only 1 questionnaire, not all participants completed all questionnaires. The responses obtained for each questionnaire are presented in Figure 1.
Controls were intended to match patients on age, sex, and geographical location. They were recruited from schools across the Capital Region and Zealand Region between November 2022 and January 2024. Inclusion criteria were as follows: age 6-19 years, no headache diagnosis, no history of medical treatment for headache, sufficient proficiency in Danish to complete the questionnaires, provision of information on headache frequency, and completion of at least 1 study questionnaire. The lower age limit of 6 years was chosen both because only 2 patients were below this age and because formal schooling in Denmark begins at age 6 years. Questionnaires were completed in REDCap.22,23 Controls were divided post hoc based on headache frequency into 2 groups: controls with headache (CH+) (≥1 headache in the past month) and headache-free controls (CH–) (no headaches in the past month).
Measurements and Variables
Obsessive-Compulsive Inventory Revised
Symptoms of OCD in the past month were measured with OCI-R, consisting of 18 items comprising 6 subscales and a total score. 24 The subscales are washing, obsessing, ordering, checking, neutralizing, and hoarding.24,25 OCI-R was completed by the child/adolescent as self-report. OCI-R is validated as a screening instrument to be used in adolescents ≥16 years old. 26 It has been translated into Danish and is used across all age groups because of current practice and availability. The OCI-R is a valid and reliable measure, with high internal consistency and moderate to high test-retest reliability.24,25,27-29 Participants received a research diagnosis of OCD if the total score was above the empirically derived cutoff score of 15. 27 The OCI-R total score was used to estimate symptom severity of OCD.
Attention-Deficit/Hyperactivity Disorder Rating Scale Extended Version
The ADHD-RS was used to assess symptoms of ADHD within the last six months. 30 The ADHD-RS is a revised 26-item version of the ADHD-RS-IV, including items on the subscales inattention, hyperactivity/impulsivity and Oppositional Defiant Disorder.31-33 It is validated as a screening instrument in children ages 4-17 years. The parent-report version was completed by the child's caregiver/parent. The ADHD-RS is a valid and reliable tool, with high internal consistency, good to really good test-retest reliability, and excellent predictive ability for ADHD.30,34,35 Danish national norm scores exist, with rater-, sex-, and age-dependent cutoff scores for each subscale (Appendix A, Table A.1).30,36 A research diagnosis of ADHD was assigned if the participant scored above the national norm score on either one or both subscales for inattention and hyperactivity/impulsivity. ADHD symptom severity was measured with the total score.
Social Responsiveness Scale–Second Edition
SRS-2 was used to quantify symptoms of the ASD within the past month.37-39 The scale has 65 items and five subscales: social awareness, social cognition, social communication, social motivation, and restricted interests and repetitive behavior. It is validated as a screening instrument for children ages 4-18 years, and the parent-report version was completed by the child's caregiver/parent. The SRS-2 is reliable, with high internal consistency, good interrater and test-retest reliability, and good validity.38,40-43 When scoring, the scores are converted to rater-, sex- and age-specific T scores. A research value for the total T score of 65 is recommended and applied to assign a research diagnosis of ASD. 40 Symptom severity of ASD was estimated with the total T score.
Research Diagnosis of Psychiatric Comorbidity
A research diagnosis of OCD, ADHD, and ASD was given to participants who either had a prior clinical diagnosis given by a child and adolescent psychiatrist or who met research diagnostic criteria based on their questionnaire scores. Data on prior diagnosis was collected during the medical record review for patients and as self-report in controls. Participants with a prior diagnosis were considered to have the condition irrespective of their questionnaire results, reflecting the expectation that effective management may reduce symptoms below the diagnostic threshold for a research diagnosis. Throughout this study, the term prevalence therefore refers to individuals with either a prior diagnosis or symptom scores above established clinical cutoffs.
Headache Diagnosis
For patients, medical records were reviewed manually and headache diagnosis assigned according to the International Classification of Headache Disorders–III criteria (ICHD-3). 44 This approach was chosen over relying on diagnoses assigned in clinic, ensuring homogeneity of the symptoms experienced within each diagnostic group and to improve comparability with other research. Patients were classified as follows: All Patients (regardless of headache diagnosis), Migraine group (including both migraine with and without aura), TTH group, Mixed group (patients with both migraine and TTH), and Unclassified Headache group (patients who did not fully meet ICHD-3 criteria). Patients with secondary or cluster headaches were included only in the All Patients group. The All Patients group was intended to represent the entire clinical population typically seen in a headache outpatient clinic, while the subgroup analyses provided insight into whether associations with psychiatric symptoms were specific to primary headache types or also present among patients with unclassified headache.
Headache Frequency
Headache frequency (past month) was obtained from medical records for patients and from self-report questionnaires for controls. Headache frequency was categorized into daily (≥15 days per month), weekly (4-14 days per month), monthly (1-3 days per month), and less than monthly headache. This categorization differs from the frequency categories defined by ICHD-3, as the available data only reflected headaches in the past month, whereas ICHD-3 considers a longer duration. However, a cutoff of ≥15 days per month is consistent with the ICHD-3 criteria for chronic headache.
Confounders
Confounders included age (continuous and categorized as child <12 years or adolescent ≥12 years), sex (biological sex assigned at birth), and socioeconomic status (SES). SES was determined by the education and occupation of the parent and graded using a scale by the Danish National Centre for Social Research. 45 The highest SES among the parents was chosen, assuming the child primarily benefits from the parent with the higher SES, irrespective of the other parent's standing.
Bias
The approach of introducing questionnaires in the routine initial assessment in clinic was chosen to reduce selection bias, which might otherwise favor families with the time and resources to participate in a clinical study. Support from a registered nurse was available if needed, helping to ensure broad representation among patients participating through this approach. However, as not all study questionnaires could be integrated into the routine initial assessment, patients were recruited through 2 approaches. This may have introduced different selection biases, depending on the approach. In terms of resources and patient motivation, those completing questionnaires as part of standard care likely represent a more heterogeneous group, whereas participants in the clinical research project may reflect a smaller, more motivated sample with greater family resources. The 2 approaches may also have reduced statistical power because of the smaller sample size in approach (2).
When recruiting controls for a headache study, there was an inherent risk of attracting participants who experience headaches more frequently than the general population. To minimize this risk, we emphasized the recruitment of “healthy” participants—defined as children without a headache diagnosis and no prior medical care for headache—in both the written information materials and verbally throughout the recruitment process.
Study Size
No formal sample size calculation was performed, as the study was designed to include all eligible patients attending the clinic during the recruitment period. The sample size was thus determined by the clinic's annual intake, which is a minimum of 200 newly referred patients. We aimed to recruit approximately 400 patients, with 100 individuals in each diagnostic group. In addition, we aimed to recruit at least 100 controls to enable group comparisons.
Ethics
Danish Regional Scientific Ethics Committee (reference: H-19003374) and the Danish Data Protection agency (reference: VD-2019-222 and R-22069732) have approved the study. Before participation, signed and informed consent was obtained from all adults with parental custody.
Statistical Methods
Analysis was performed with R version 4.2.2 (Vienna, Austria: R Foundation for Statistical Computing). 46 The analysis followed a stepwise approach. (1) To address the primary aim, we analyzed across groups, comparing the All Patients, Migraine, TTH, Mixed, and Unclassified group to both CH+ and CH–. (2) To address the secondary aim, we analyzed across headache frequency. This was done by pooling all participants (patients and controls), which we divided according to headache frequency. Comparisons were then made across the headache frequency groups, using those with the least frequent headaches (ie, “less than monthly”) as the reference category. (3) To further investigate the relationship between headache and psychiatric symptoms, we examined the association between symptom severity and headache frequency within each group (see below).
Missing data were managed as follows: For the OCI-R, ADHD-RS, and SRS-2, a questionnaire was considered “complete” if all items within at least 1 subscale had been answered. Total and subscale scores were calculated only when all items within the respective scale were completed. Because of variations in sample size across measures (resulting from the study design), the sample size for each analysis is reported in the tables to ensure transparency.
Descriptive statistics were analyzed. Age and SES (scored 1-5, with 1 indicating highest SES) followed a non-normal distribution, and was reported with median and IQR. Sex and headache frequency were reported with frequencies. Age was compared across groups using the Kruskal-Wallis test, whereas sex, SES, and headache frequency were compared using pairwise Fisher exact tests.
Symptom severity was assessed by comparing total questionnaire scores between groups. Scores were treated as count data: negative binomial regression was used for the OCI-R and ADHD-RS, and quasi-Poisson regression for the SRS-2. All models were adjusted for age and sex. OCI-R and ADHD-RS scores were non-normally distributed and are presented as median (IQR), whereas SRS-2 scores followed a normal distribution and are reported as mean ± SD. Subscale scores are reported in Appendix B.
Prevalence of comorbidity (OCD, ADHD, and ASD) was assessed using binomial regression with a logit link. This approach was chosen over log-binomial models because of its greater numerical stability while allowing adjustment for age and sex. Results are presented with percentages and odds ratios with 95% CIs.
To assess the association between symptom severity and headache frequency, the same regression models were used (negative binomial for OCI-R and ADHD-RS; quasi-Poisson for SRS-2), comparing symptom severity across headache frequency groups, using the group with the least frequent headaches as the reference.
To assess the association between symptom severity and headache frequency within each group, analyses were conducted within each group, stratifying for headache frequency, again using the group with the least frequent headaches as the reference. For this analysis, control participants were included as a combined group, with CH– (less than monthly headaches) serving as the reference category. These results are provided in Appendix C.
For all analyses, model checks were performed to assess model fit and adequacy. The significance level was set at P <.05.
Results
Descriptive Statistics
A total of 343 patients with headache and 130 controls were included: 72 in the CH+ group and 58 in the CH– group (Figure 1). Of the 343 patients, 86 were diagnosed with migraine, 101 with TTH, 81 with mixed, 1 with cluster, and 21 with secondary headache, and 53 remained unclassified. Headache frequency was obtained for 459 participants: 116 had daily, 154 had weekly, 108 had monthly, and 81 had less than monthly headaches. In Table 1, the descriptive statistics of patients and controls are presented.
Descriptive Statistics by Headache Diagnostic Group for Patients and Controls.a
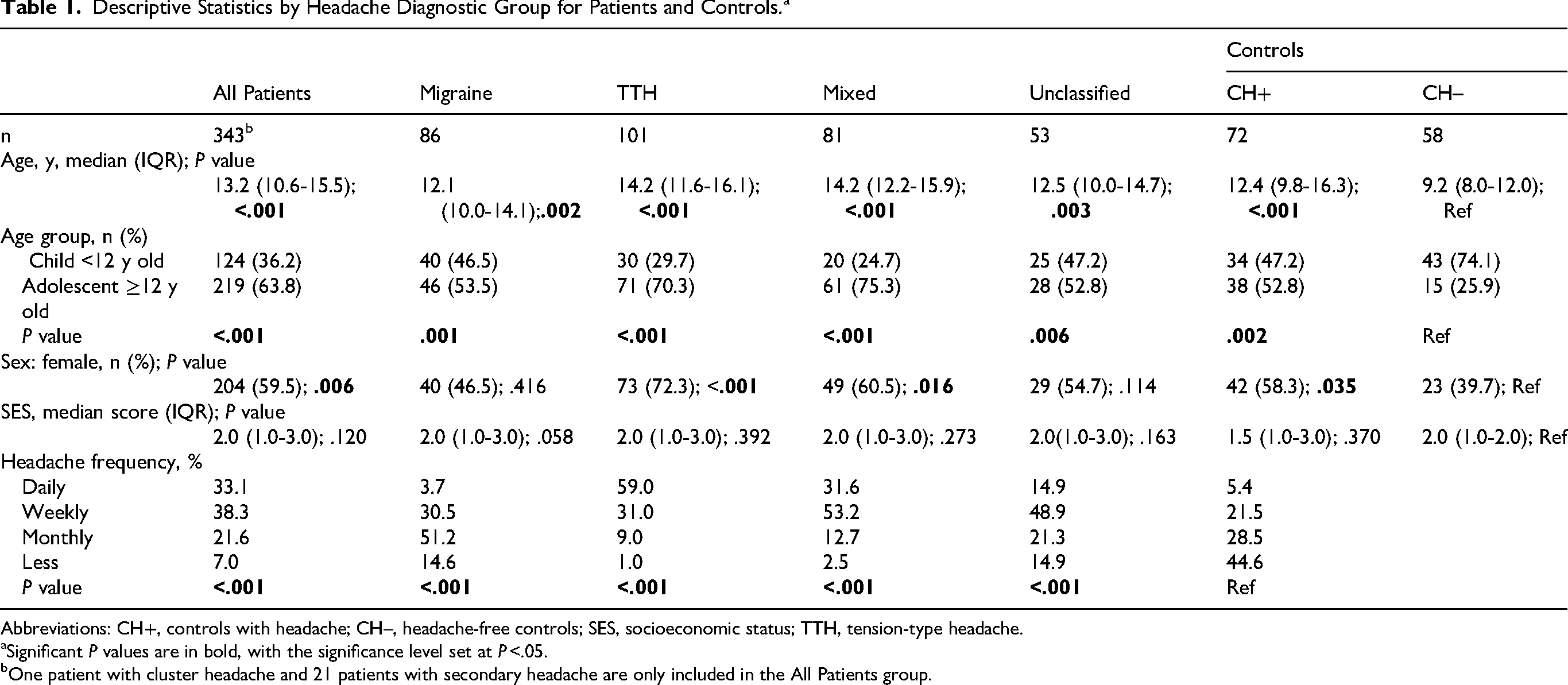
Abbreviations: CH+, controls with headache; CH–, headache-free controls; SES, socioeconomic status; TTH, tension-type headache.
Significant P values are in bold, with the significance level set at P <.05.
One patient with cluster headache and 21 patients with secondary headache are only included in the All Patients group.
The CH– group was significantly younger than all other groups, with a median age of 9.2 years (IQR 8.0-12.0) compared with 13.2 years (IQR 10.6-15.5, P < .001) in All Patients and 12.4 years (IQR 9.8-16.3, P < .001) in CH+. They were also predominantly male, with only 39.7% females compared with 46.5% to 72.3% in the other groups (Table 1). Patients reported more frequent headaches than the combined control group (Table 1). Headache frequency in the control group was comparable to, although slightly lower than, a large non-representative study of Danish schoolchildren from several municipalities (55.4% ≥ 1 day/month and 26.9% ≥ 4 days vs. 58%-67% ≥ 1 headache in 2 weeks).19,20
Symptom Severity
Symptom severity of OCD, ADHD, and ASD was assessed using total scores from the screening questionnaires, reported in Table 2. The All Patients and CH+ groups consistently reported more severe symptoms of all 3 comorbidities than the CH– group (Table 3). In the patient subgroups, only patients with migraine had more severe OCD symptoms; both patients with migraine and unclassified headache had more severe ADHD symptoms; and only patients with TTH had more severe ASD symptoms than the CH– group (Table 3). OCD symptoms increased with age, whereas ADHD symptoms decreased, and ASD symptoms showed no association with age (Table 2). Only symptoms of ADHD were associated to sex, with higher severity in males than in females (Table 2). In Table 2, we also compare symptom severity between patients and the CH+ group. We found that only OCD scores differed significantly, with the All Patients, TTH, and Mixed Headache groups reporting lower symptom severity than the CH+ group.
Association of Psychiatric Symptom Severity to Group, Age, and Sex.a
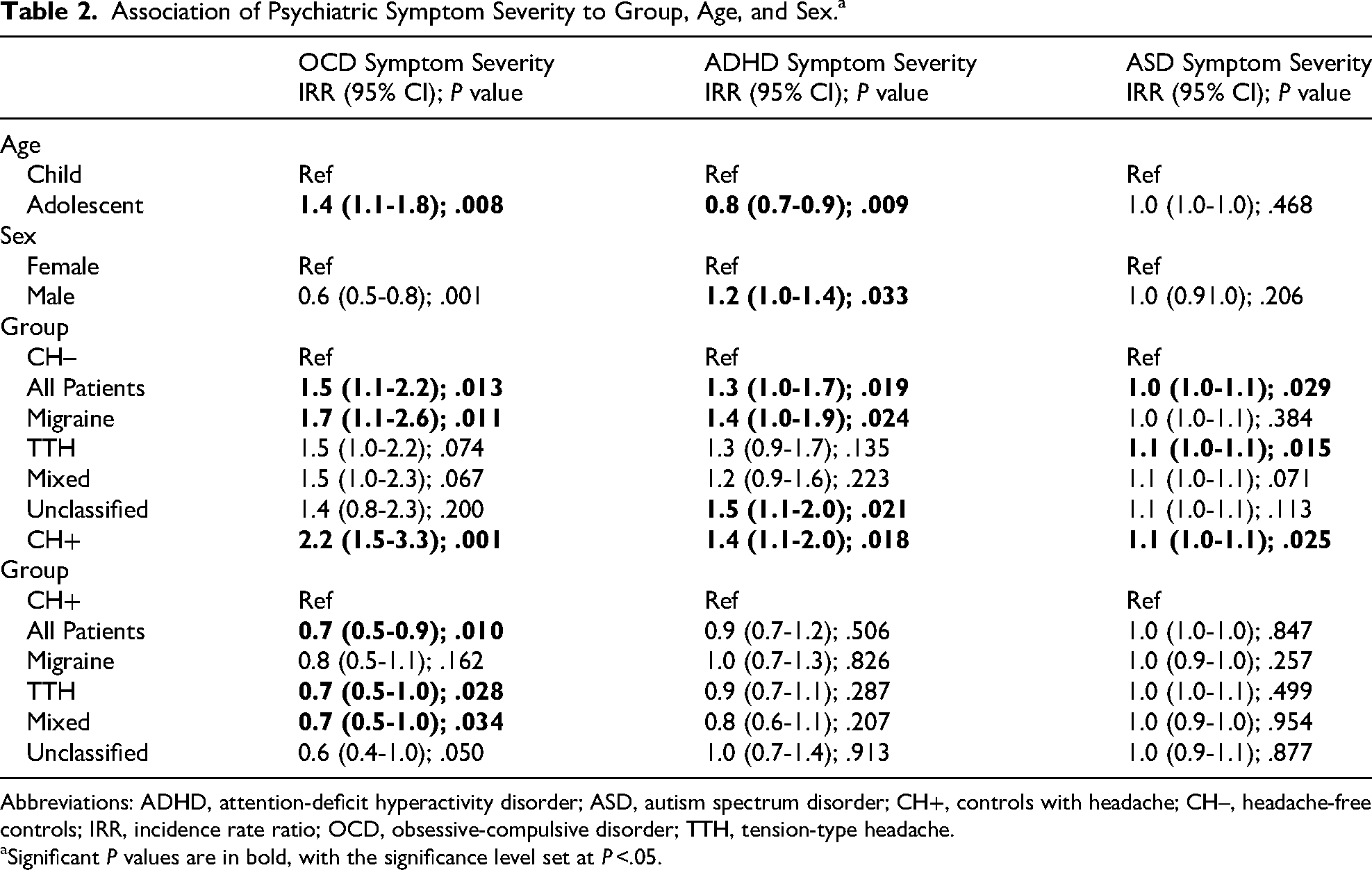
Abbreviations: ADHD, attention-deficit hyperactivity disorder; ASD, autism spectrum disorder; CH+, controls with headache; CH–, headache-free controls; IRR, incidence rate ratio; OCD, obsessive-compulsive disorder; TTH, tension-type headache.
Significant P values are in bold, with the significance level set at P <.05.
Observed Symptom Severity of OCD, ADHD, and ASD in All Groups.a
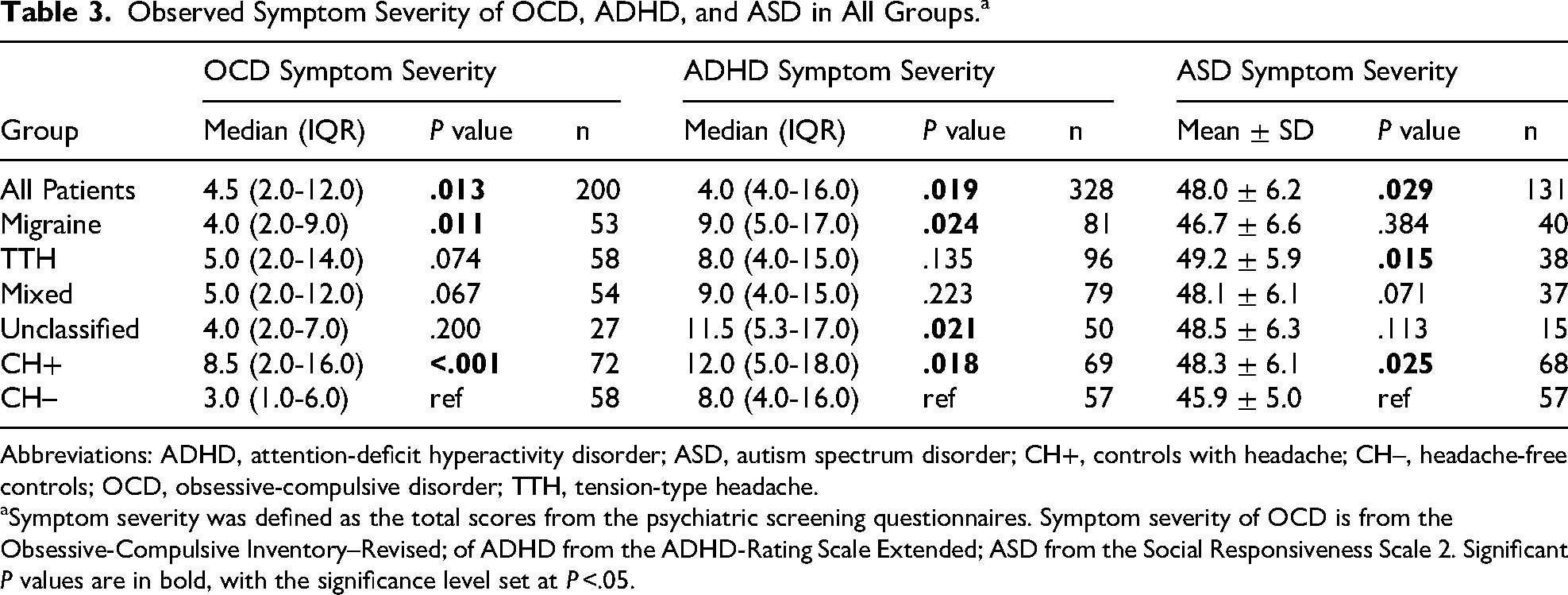
Abbreviations: ADHD, attention-deficit hyperactivity disorder; ASD, autism spectrum disorder; CH+, controls with headache; CH–, headache-free controls; OCD, obsessive-compulsive disorder; TTH, tension-type headache.
Symptom severity was defined as the total scores from the psychiatric screening questionnaires. Symptom severity of OCD is from the Obsessive-Compulsive Inventory–Revised; of ADHD from the ADHD-Rating Scale Extended; ASD from the Social Responsiveness Scale 2. Significant P values are in bold, with the significance level set at P <.05.
Symptom Severity and Headache Frequency
We found that psychiatric symptoms were associated to headache frequency (Table 4). For all 3 comorbidities, higher headache frequency was in some way associated with greater symptom severity. ASD symptoms consistently became more severe as headache frequency increased (Table 4). In contrast, the associations for OCD and ADHD were less consistent: weekly headache was associated with higher symptom severity for ADHD, whereas both weekly and monthly headache were associated with higher severity for OCD (Table 4).
Symptom Severity in Headache Frequency Groups.a
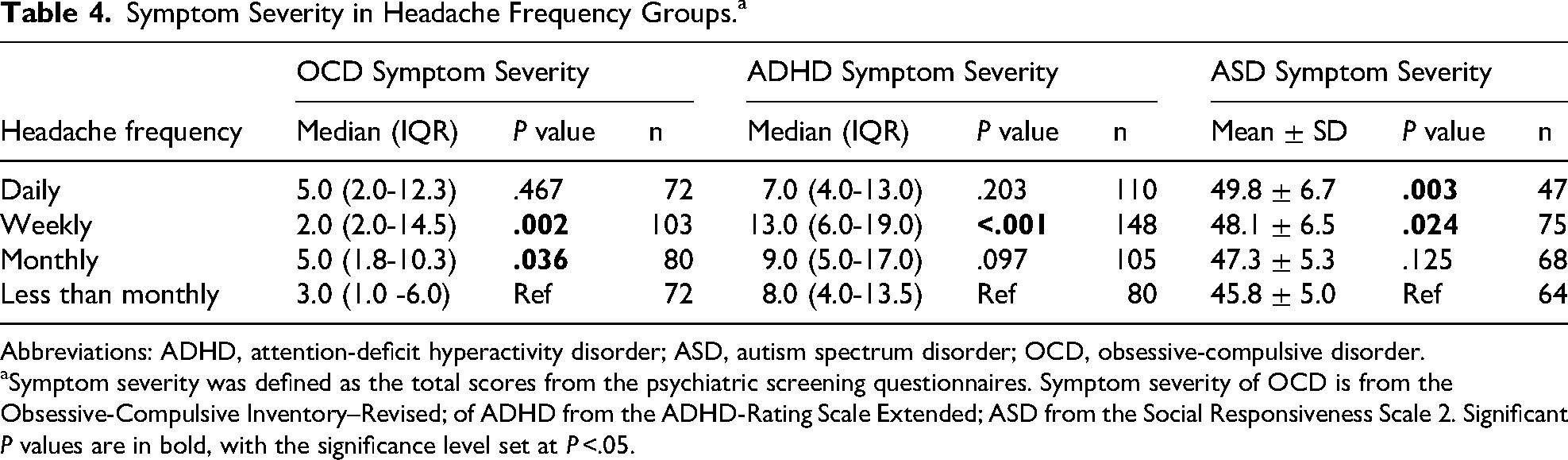
Abbreviations: ADHD, attention-deficit hyperactivity disorder; ASD, autism spectrum disorder; OCD, obsessive-compulsive disorder.
Symptom severity was defined as the total scores from the psychiatric screening questionnaires. Symptom severity of OCD is from the Obsessive-Compulsive Inventory–Revised; of ADHD from the ADHD-Rating Scale Extended; ASD from the Social Responsiveness Scale 2. Significant P values are in bold, with the significance level set at P <.05.
Further subgroup analysis revealed the association between frequency and psychiatric symptoms to be primarily driven by the control group (Appendix C). Thus, a strong association between headache frequency and OCD, ADHD, and ASD symptoms was found in the control group (Appendix C, Table C.1-C.3). The association also persisted in the Mixed Headache group for OCD symptoms, and in the Migraine and All Patients group for ADHD symptoms (Tables C.1 and C.2).
Prevalence
Prevalence rates of participants receiving a research diagnosis of OCD, ADHD, and ASD are shown in Table 5 and Figure 2. We compared prevalence rates with reference to both the CH– and the CH+ groups. OCD was significantly more prevalent in the All Patients (20.8%), Migraine (20.8%), TTH (27.1%), Mixed (20.4%), and CH+ (27.8%) groups, compared with CH– (1.7%). ADHD was significantly more prevalent in the All Patients (17.3%), Migraine (18.1%), Unclassified (26.4%), and CH+ (18.8%) groups compared with CH– (7.0%). ASD was significantly more prevalent only in the Unclassified group compared with CH– (17.6% vs 1.8%). There were no significant differences in the prevalence of any of the 3 comorbidities when comparing patient groups with CH+.
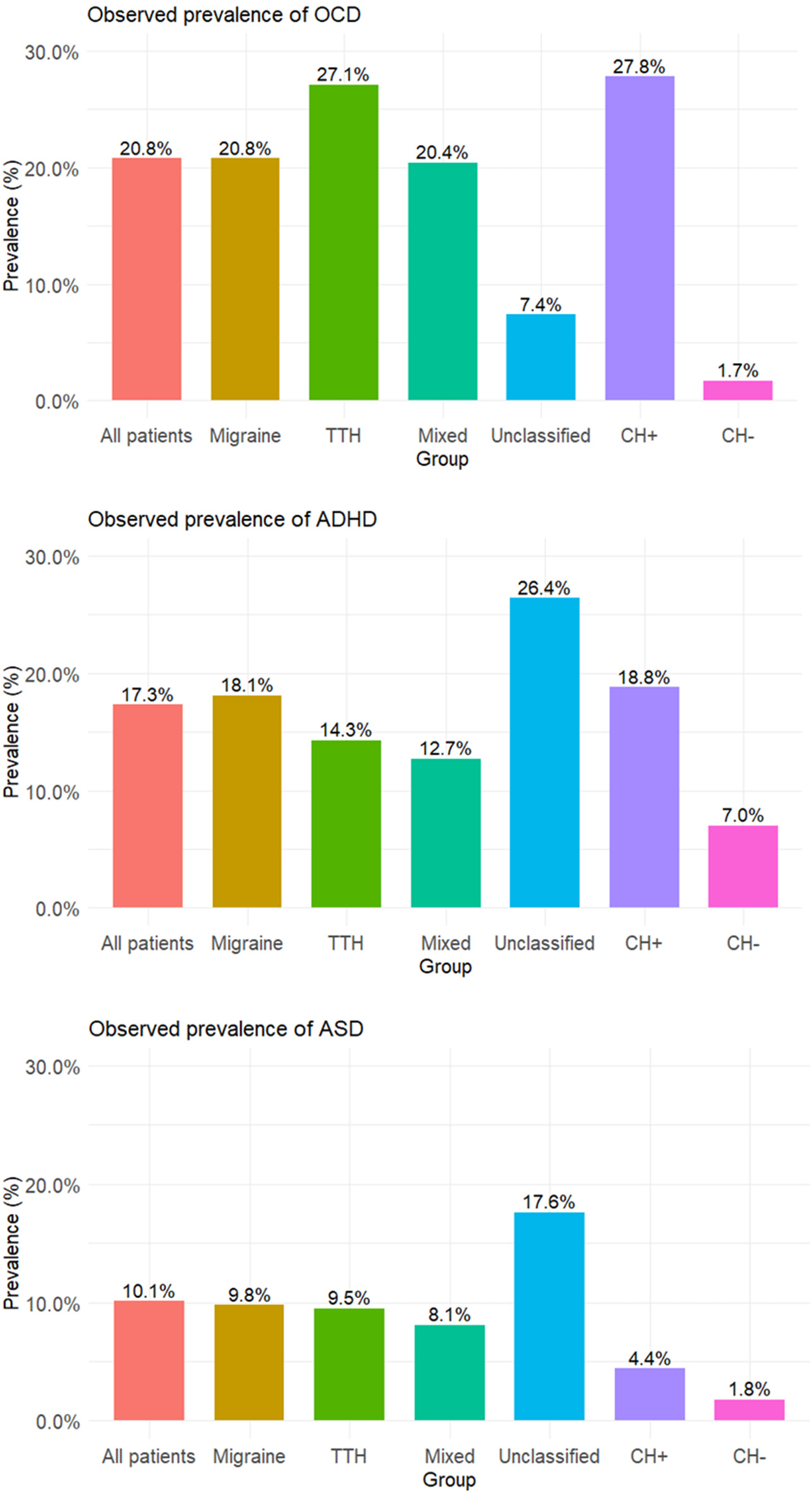
Bar plot of the observed prevalence of OCD, ADHD, and ASD in the groups. ADHD, attention-deficit hyperactivity disorder; ASD, autism spectrum disorder; CH+, controls with headache; CH–, headache-free controls; OCD, obsessive-compulsive disorder; TTH, tension-type headache.
Prevalence of OCD, ADHD, and ASD in the Groups.a
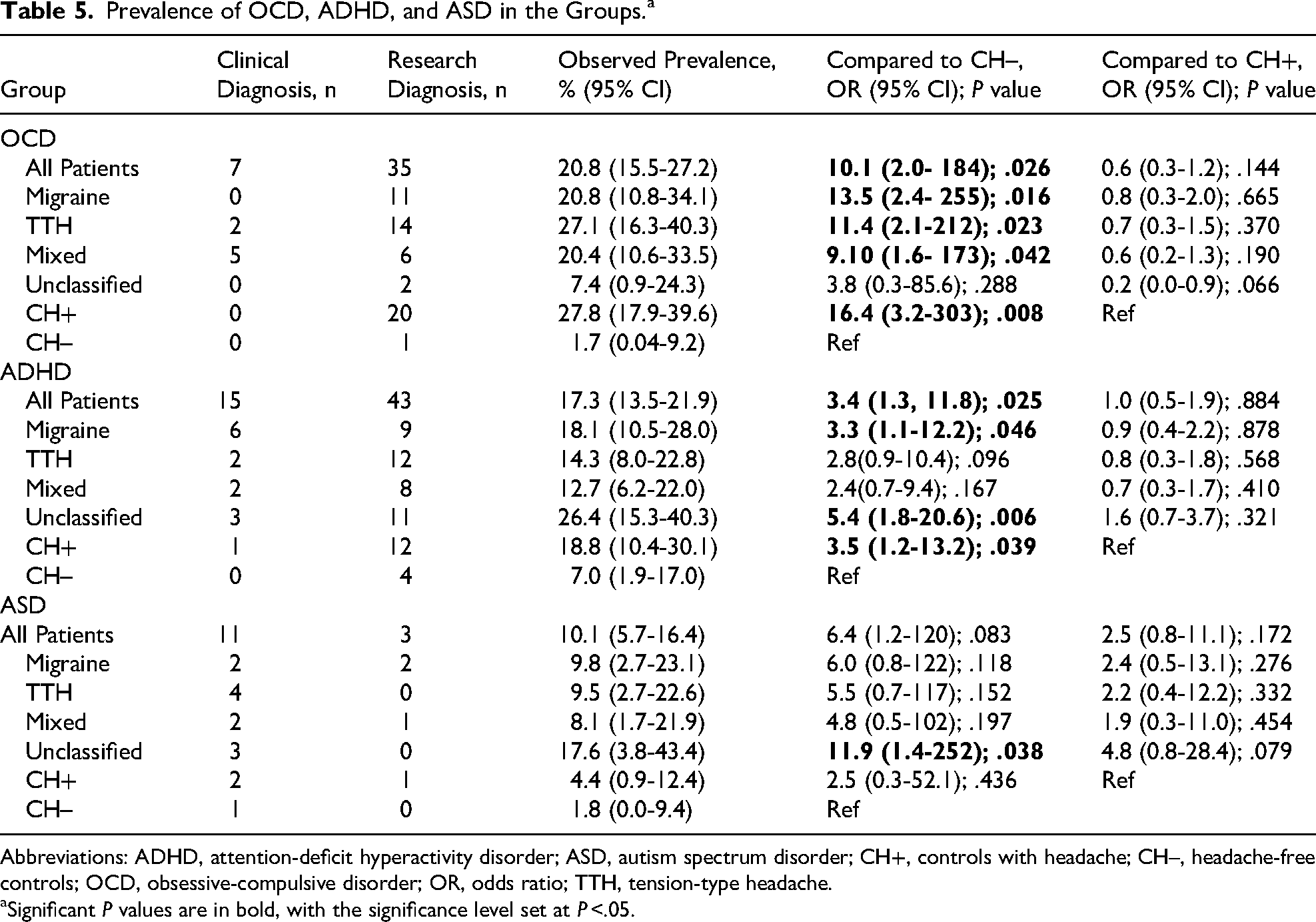
Abbreviations: ADHD, attention-deficit hyperactivity disorder; ASD, autism spectrum disorder; CH+, controls with headache; CH–, headache-free controls; OCD, obsessive-compulsive disorder; OR, odds ratio; TTH, tension-type headache.
Significant P values are in bold, with the significance level set at P <.05.
Discussion
We aimed to measure the symptom severity and prevalence of OCD, ADHD, and ASD in children and adolescents attending a headache outpatient clinic, compared to controls with and without headache (the CH+ and CH– groups). Findings were based on screening instruments and thus reflect symptom burden rather than confirmed clinical diagnoses. To our knowledge, this is the first study to evaluate ASD symptoms in children whose primary diagnosis is headache. We found a high prevalence—based on research diagnoses—of all 3 comorbidities, and surprisingly, these comorbidities were not limited to our patients but also prominent in our CH+ group. The CH+ group, surprisingly, had the most severe symptoms of all 3 conditions, when measured with total scores on the questionnaires, and had the highest research-based prevalence of OCD—suggesting a broader association between headache and psychiatric symptoms.
We also examined the relationship between symptom severity and headache frequency. In the control group, we observed a strong association between higher headache frequency and increased symptoms of OCD, ADHD, and ASD. This association is supported by existing literature.2,4,47
Obsessive-Compulsive Disorder
One in 5 of All Patients received a research diagnosis of OCD compared with 1 in 4 of CH+, and 1 in 59 of CH–. Among patient subgroups, TTH had the highest prevalence, surpassing that of patients with migraine (27.1% vs 20.8%). In line with previous research, we replicated the finding that both patients and CH+—who had not sought help in managing their symptoms—experienced a significantly higher symptom burden of OCD than CH–. 7 Contrary to existing literature, however, we found a higher prevalence of OCD in patients with TTH compared to those with migraine. 8
It is important to note that the high prevalence may reflect an important limitation of our methodology—that we used a self-report questionnaire validated for use only in individuals ≥16 years, with cutoff scores based on adult data.26,27 The validity of this instrument for use in younger children is uncertain. Nevertheless, OCD symptoms experienced by children are similar to those reported by adults, 48 and although the questionnaire might not be appropriate for diagnosing OCD in children, it may still provide a meaningful indication of overall symptom burden.
Attention Deficit/Hyperactivity Disorder
A research diagnosis of ADHD was given in 1 in 6 of All Patients, 1 in 5 of CH+, and 1 in 14 of CH–. Here, among patient subgroups, patients with unclassified headache had the highest prevalence, followed by patients with migraine and then patients with TTH (26.4% vs 18.8% vs 14.3%). We are the first to compare prevalence of ADHD in patients to both CH+ and CH– simultaneously. However, our findings are not unexpected. Previous clinical studies (eg, in pediatric headache outpatient clinics) have also reported more ADHD symptoms in patients with primary headache compared to CH–.49-51 Contrary to us, however, they found that patients with TTH had similar 51 or higher49,52 prevalence/symptom severity than patients with migraine. Results from population-based studies are mixed: some report an association between frequent headaches or headache disorders (based on self- or parent-reported symptoms) and ADHD,53-56 whereas others do not support this association.57,58 This mirrors our comparison between the CH+ and CH− groups.
What stands out is the particularly high prevalence of ADHD in the Unclassified Headache group, where nearly one-third of participants received a research diagnosis. First, we raise the question of why these children fall in the Unclassified Headache category. It may reflect our methodological choice to manually assign headache diagnoses based on medical record review, rather than relying on clinically assigned headache diagnoses. The ICHD-3 criteria are adult-based, 59 and in clinical practice, neuropediatricians may adapt them to account for age-specific headache presentations,60,61 such as shorter migraine duration. As a result, clinical diagnoses are not always strictly ICHD-3 compliant. For research purposes, however, strict adherence to the diagnostic criteria is paramount, allowing us to ensure homogeneity within groups and comparability across studies. However, this approach can result in a subset of patients being categorized as “unclassified” because of incomplete information in their medical records or because their symptoms do not strictly meet ICHD-3 criteria.
However, the high prevalence of ADHD offers an important new perspective. Although hypothetical, it raises the possibility that, for some children, the headache symptoms could be secondary to or influenced by an underlying ADHD condition. Notably, 11 of 14 children in this group received their ADHD research diagnosis based on their scores on the screening questionnaire. The diagnosis is not confirmed by a child and adolescent psychiatrist in this study; however, this could indicate that some children have ADHD symptoms that have previously gone unrecognized, warranting further exploration of whether they could benefit from psychiatric evaluation. These findings may support a possible bidirectional relationship between ADHD and headache.
Autism Spectrum Disorder
ASD was present in 1 of 10 of All Patients, 1 in 23 of CH+, and 1 in 56 of CH–. In contrast to the other conditions, most individuals with ASD had a prior diagnosis, and only a few received a research diagnosis based on their questionnaire scores. Once again, the patient subgroup with unclassified headache had the highest prevalence, followed by migraine and TTH (17.6% vs 9.8% vs 9.5%). As our study provides novel data on the presence of ASD in patients with headache as their primary diagnosis, comparisons with previous research are limited. However, as mentioned, existing studies found that individuals with ASD have higher odds of experiencing migraine or headaches.11,62 Although we observed numerically higher odds of ASD in patients with migraine compared with CH–, this difference did not reach statistical significance. This is likely due to a significant limitation of our ASD data: sample size.
The SRS-2 was the only questionnaire to be solely distributed through the clinical research project approach, making it the questionnaire with the lowest response rate. It was also the longest questionnaire, and with only 131 of 183 fully completed (76%), this introduced a potential non-response bias. It is possible that those who chose to respond were those who found the content more relevant or reflective of their own experiences. For instance, those who had a prior diagnosis of ASD may be more familiar and willing to complete the questionnaire, which could overestimate the symptom severity based on questionnaire scores reported in this study. However, an important counterpoint is that the majority diagnosed with ASD (14 of 18; 78%) had already received their diagnosis prior to participation in the study—for them, the research diagnosis given was not based on their questionnaire scores. This suggests that the potential bias from non-responders may have had limited influence on the reported prevalence. Therefore, despite the small sample size, a key strength of our ASD data is that most diagnoses were confirmed as they were given by a child psychiatrist. This supports the notion that ASD and headache disorders are comorbid conditions.11,62
Another interesting finding was that the TTH group was the only patient group with significantly more severe ASD symptoms than the CH– group. This could suggest that neurologic traits observed in ASD—such as sensory sensitivity or altered pain processing63,64—may also play a role in the development or maintenance of TTH. Such shared mechanisms could reflect overlapping neurobiologic pathways, for example. involving central sensitization or atypical sensory integration.65-68
Evidence for a Bidirectional Relationship
The relationship between headache and psychiatric disorders is still being explored. One theory is that there are shared pathophysiological mechanisms behind the conditions. For example, migraine and anxiety disorders such as OCD both involve the limbic system, which plays a role in migraine's prodromal phase and in anxiety-related threat processing.18,69,70 Neuronal hyperexcitability in migraine may sensitize limbic structures, increasing vulnerability to anxiety18,71 Migraine and ADHD may also share mechanisms, such as dopamine dysregulation,72,73 disrupted sleep-wake cycle,72,74 and impaired brain iron metabolism. 72 Similarly, links between migraine and autism have been proposed. These may be linked to minicolumnopathy, which leads to a hyperexcitable cortex and serotonergic imbalance, 15 genetic calcium signaling anomalies, 16 and a shared sensory hyperreactivity. 17
Another theory is that patients with primary headache exhibit associated symptoms that resemble a psychiatric disorder. For instance, Villa et al 75 found impaired visual attention in children with migraine and proposed that altered levels of noradrenaline and dopamine may predispose these children to attentional difficulties. Similarly, children with migraine report challenges with concentration in school, 76 and a recent review concluded that children with primary headache can have altered neuropsychological functions, including reduced attention, slower processing speed, and impaired memory. 13 This raises the possibility that some of the psychiatric symptoms observed in our study may, in fact, reflect associated symptoms of having headaches rather than distinct comorbid disorders. OCD and ADHD were primarily identified through research diagnoses, which required a high symptom load during assessment—unlike ASD, where only a few participants showed symptoms severe enough to meet the research diagnostic criteria. This may suggest that the psychological symptoms linked to headache more often resemble anxiety or attention-related difficulties, rather than social-communication challenges.
One of the most unexpected findings was the high prevalence of participants receiving a research diagnosis of ADHD and OCD in the CH+ group. This may support a third theory: that children with underlying psychiatric symptoms or difficulties may experience headaches as a manifestation of psychological stress–suggesting a reversed causal relationship. Some studies have found that headache can precede the diagnosis of psychiatric disorders.12,77 In this view, greater psychiatric symptom severity could be expected to coincide with increased headache frequency. Consistent with this, we observed a strong association between all three psychiatric conditions and headache frequency among controls.
We did not observe the same consistent association between psychiatric symptom severity and headache frequency in the patient groups. One explanation for this may be that treatment and management within the health care system have reduced headache frequency, thereby obscuring the observed link.
Perspectives and Clinical Implications
Our prevalence rates for OCD, ADHD, and ASD in our sample were markedly higher than national for patients aged 10-24 years in Denmark (0.65%, 4.50%, and 2.17%, respectively). 78 This may reflect an increased burden of neuropsychiatric symptoms among children with headache. However, research-based diagnoses are not equivalent to clinical diagnoses, and longitudinal studies are needed to assess diagnostic trajectories. Still, high symptom scores may indicate underlying psychosocial vulnerability, even without a formal diagnosis.
Current headache management guidelines recommend systematic assessment of anxiety and depression in children with headache.79,80 Based on our findings, we propose that this should be extended to include screening for OCD and ADHD. Screening for ASD, however, should be reserved for cases with clinical suspicion. Although we identified a high prevalence, most cases had already been diagnosed prior to participation. This supports a comorbid relationship between ASD and headache but suggests that routine screening may have limited utility, as children with ASD are likely to have already been identified.
As psychiatric comorbidities were also common in CH+, this points to a broader and more complex association between headache and psychiatric disorders. Recognizing this association is important—not only for health professionals but also for teachers, school nurses, and parents. When a child experiences frequent headaches, it may be a sign of underlying psychological strain. Awareness of this link can help ensure that attention is directed beyond the physical symptom, to better understand what might be going on beneath the surface.
Strengths and Limitations
Strengths in this study include employing broad eligibility criteria in our patients and manual assignment of the headache diagnosis, enabling analysis of both the entire patient cohort and specific diagnostic subgroups. Additionally, actively addressing selection bias increased the representativeness of the patients, and results are likely generalizable to other neuropediatric departments and headache outpatient clinics.
A post hoc division of the control group into headache (CH+) and headache-free (CH–) subgroups was motivated by the high prevalence of headache among controls and the observed association with psychiatric symptoms. The purpose was to present this pattern clearly. However, this data-driven approach may reduce generalizability and statistical power and carries a risk of overfitting. It may also complicate interpretation, as the CH+ group could represent a subset of controls sharing several characteristics with the patient group, thereby diluting the contrast between patients and controls. At the same time, this division may provide new insights. The CH+ group could represent an intermediate stage between headache-free individuals and patients who have sought medical care for their headaches. This perspective may also help clarify whether the observed differences are specific to patients in clinic or reflect broader associations with headache occurrence in the general population. The CH– subgroup was younger and more predominantly male. As headache prevalence increases with age81-83 and is generally higher among females, particularly after the onset of puberty,81-84 this distribution was expected. Although analyses were adjusted for age and sex, this may still have influenced the results.
A key limitation was using OCI-R, which is developed and validated for individuals aged 16 years and older. Although child versions exist,85,86 a Danish translation was not available at the time of data collection, and it is common practice to apply the adult version across age groups. This may have contributed to higher OCD symptom scores, as behaviors that are developmentally appropriate in younger children—such as ritualistic behaviors or collecting objects 87 —might be interpreted as obsessive-compulsive symptoms in older individuals. The child version of OCI-R includes similar content but with age-adapted wording, which substantially improves children's comprehension of the items. 88 Consequently, use of the adult OCI-R could have led to falsely inflated prevalence rates of OCD among our participants.
Another important limitation is that the prevalence of psychiatric comorbidity was based on research diagnoses derived from screening instruments rather than clinical assessments. Although screening instruments can indicate a greater risk of psychiatric disorders,27,40,89,90 they cannot alone serve as the basis for a clinical diagnosis.91-93 A clinical diagnosis requires a comprehensive evaluation by a child and adolescent psychiatrist, including contextual information about the child's everyday functioning. 94 Consequently, some participants who met research criteria for a psychiatric disorder might not have received a clinical diagnosis if assessed by a psychiatrist.
The OCI-R was completed by the children themselves, whereas ADHD-RS and SRS-2 were completed by a parent. For OCI-R, then, a limitation is that we could not determine or control the extent of the parent's involvement, as questionnaires were completed without study personnel present, potentially introducing bias. Younger participants likely received parental assistance—which is necessary and beneficial, as it would have improved response validity in the youngest participants. 95
Other limitations include patient recruitment through 2 approaches, which might have introduced different selection biases in patients (see subsection “Bias” above); dividing participants into groups, which decreased sample size, limiting statistical power and generalizability; being unable to match controls on age, despite targeted efforts, which—although adjusted for in the analysis—may still impact results; recruiting participants partly during the COVID-19 pandemic, which could have influenced the presence of headache and increased the level of psychiatric symptoms both during96,97 and after98,99 the pandemic; the time gap between examining patients and controls; and that clinical diagnosis of psychiatric comorbidity was collected through self-report in controls, potentially causing misclassification. We did not collect data on medication use, which—particularly for treating the psychiatric comorbidity—could confound severity of reported symptoms. To partly address this, we did not use questionnaire data from participants with a clinical diagnosis of psychiatric comorbidity when assigning a research diagnosis. However, medication use could still confound the estimated symptom severity. Furthermore, we did not collect detailed information on individuals who declined participation or did not complete the questionnaires in approach (1). Although approximately 800 patients were seen in the clinic during the study period, the number who attended an initial assessment and were offered the questionnaires was not recorded. Similarly, it was not possible to determine how many patients received a questionnaire but did not return it because of discharge or other reasons. This lack of registration limits the ability to assess potential selection bias. Also, in the analysis of headache frequency (Appendix C, Tables C.1-C.3), the reference group had the fewest observations, thereby reducing the likelihood of detecting differences. Because of the cross-sectional design, causal relationships cannot be established, and the findings should therefore be interpreted as associations only.
Conclusion
We found a high symptom burden and prevalence of research diagnoses of OCD, ADHD, and ASD among children and adolescents attending a headache outpatient clinic, as well as in controls with headache, compared with headache-free controls. In the control group, symptom severity consistently increased with headache frequency. This suggests that headache and psychiatric comorbidities are associated, regardless of whether the child has sought medical attention for their headaches.
OCD and ADHD emerged as particularly relevant conditions to screen for, and we therefore recommend routine screening for these disorders in children presenting with headache. In contrast, screening for ASD should be reserved for cases where there is clinical suspicion.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738261456884 - Supplemental material for Symptoms of Obsessive-Compulsive Disorder, Attention-Deficit/Hyperactivity Disorder, and Autism Spectrum Disorder in Children and Adolescents Attending a Headache Outpatient Clinic and School-Based Controls
Supplemental material, sj-docx-1-jcn-10.1177_08830738261456884 for Symptoms of Obsessive-Compulsive Disorder, Attention-Deficit/Hyperactivity Disorder, and Autism Spectrum Disorder in Children and Adolescents Attending a Headache Outpatient Clinic and School-Based Controls by Amalie Akulenok Berring-Uldum, Lisa Ysrea Pann, Maria J. Miranda and Nanette Marinette Monique Debes in Journal of Child Neurology
Supplemental Material
sj-docx-2-jcn-10.1177_08830738261456884 - Supplemental material for Symptoms of Obsessive-Compulsive Disorder, Attention-Deficit/Hyperactivity Disorder, and Autism Spectrum Disorder in Children and Adolescents Attending a Headache Outpatient Clinic and School-Based Controls
Supplemental material, sj-docx-2-jcn-10.1177_08830738261456884 for Symptoms of Obsessive-Compulsive Disorder, Attention-Deficit/Hyperactivity Disorder, and Autism Spectrum Disorder in Children and Adolescents Attending a Headache Outpatient Clinic and School-Based Controls by Amalie Akulenok Berring-Uldum, Lisa Ysrea Pann, Maria J. Miranda and Nanette Marinette Monique Debes in Journal of Child Neurology
Footnotes
Author Contributions
Amalie Akulenok Berring-Uldum: Conceptualization, Methodology, Formal analysis, Investigation, Data curation, Writing - original draft, Visualization, Project administration, Funding acquisition; Lisa Pann: Investigation, Data curation, Writing - Review and editing; Maria J. Miranda: Resources, Writing - Review and Editing; Supervision; Nanette Mol Debes: Conceptualization, Methodology, Resources, Writing - Review and Editing, Supervision, Project administration.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Herlev and Gentofte University Hospital Research Grant; Tværspuljen—Sektion for Tværsektoriel Forskning (grant number: Pb-2023-1); King Christian the Tenth Foundation (grant number: 13-2024); Tømrermester Jørgen Holm og hustru Elisa f. Hansens Mindelegat (grant number: 24009).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available on request from the corresponding author. Unfortunately, they are not deposited in a research data deposit because of restrictions imposed by the ethical board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.