
Abstract
Objective
To characterize the clinical profile, functional and developmental status, radiologic patterns, and comorbidity burden in children aged 1-14 years diagnosed with hemiplegic cerebral palsy (HCP) at a tertiary pediatric neurology center.
Methods
This cross-sectional study included 70 children with HCP. Functional assessments were done with the Gross Motor Function Classification System (GMFCS), Manual Ability Classification System (MACS), and the Quality of Upper Extremity Skills Test (QUEST). Development was evaluated using Developmental Profile-3 (DP-3), whereas caregiver-reported health-related quality of life was assessed through the Caregiver Questionnaire (CQ). Correlations among functional measures, developmental scores, and epilepsy were examined.
Results
The mean age was 62.4 ± 38.3 months, with a male predominance (71.4%) and more right-sided involvement. Antenatal complications were present in 30% of pregnancies, and 41% of children required resuscitation at birth. Postnatal complications, including respiratory distress and neonatal seizures, occurred in 43%. Most children demonstrated mild to moderate motor impairment, with 73% classified as GMFCS levels I and II, and reduced hand function was common, with 88% falling within MACS levels II and III. The mean QUEST score was 68.1 ± 6.7, indicating mild to moderate impairment of upper-extremity quality, particularly in dissociated movements and grasp. Epilepsy occurred in 38.5%, visual impairment in 31%, and hearing loss in 7%. Poorer manual ability corresponded with higher GMFCS levels and lower developmental scores.
Conclusion
Children with HCP exhibit a consistent pattern of structural brain injury, substantial comorbidity burden, and measurable functional limitations, underscoring the need for early, targeted multidisciplinary intervention.
Cerebral palsy (CP) is an early-onset, lifelong neurodevelopmental condition with limitations of movement and posture, because of maldevelopment attributed to the dysplasia of or injury to the fetal/infant brain. 1 The phenotype of CP is complex and heterogenous.1,2 The motor impairments are frequently accompanied by disturbances of sensation, cognition, communication, behavior, and epilepsy, producing lifelong functional consequences for affected children and their families.3,4 Among its subtypes, hemiplegic cerebral palsy (HCP) is the second most common form of spastic CP, accounting for approximately 20% to 30% of cases. 5 HCP is characterized by unilateral spastic paresis/motor impairment with upper limb predominance compared with lower limbs. Motor impairment in HCP reflects early disruption of corticospinal pathway development. 6
The etiologic spectrum of HCP is broad but is dominated by in utero or perinatal stroke, cortical malformations, prematurity related periventricular white matter injuries, and germinal matrix/intraventricular hemorrhage, perinatal arterial ischemic stroke, and periventricular white matter injury, congenital brain malformations, neonatal infections, and metabolic or prothrombotic conditions.7–9 Perinatal ischemic stroke is the leading cause of HCP, and among them, periventricular venous infarction is the most common subtype of HCP for children born at term. 10 Children with HCP frequently exhibit many associated comorbidities, including epilepsy, cognitive impairment, visual deficits, especially strabismus and refractive errors, sleep impairment, and behavioral or attentional problems.9,11,12
In the setting of low- and middle-income countries (LMICs), delayed diagnosis, limited access to neuroimaging, and underrecognition of comorbidities contribute to heterogeneity in reported etiologies and outcomes.5,13,14 There is limited literature describing the integrated clinical, radiologic, and functional profile of children with HCP in LMIC settings, despite the high prevalence of perinatal complications and preventable neonatal morbidity. Hence, we aimed to study the clinical-radiologic characterization, comorbidities, and functional outcomes among children with HCP in an LMIC setting.
Methodology
This cross-sectional study was conducted over an 18-month period at a tertiary care center after obtaining ethical approval from the Institute's Ethical Committee. Children aged 1-14 years with HCP as defined by the Surveillance of Cerebral Palsy in Europe 15 were enrolled in the study. Children with progressive disorders, mixed CP, episodic or fluctuating hemiplegia, or underlying acute or chronic medical conditions that could adversely affect motor performance or preclude a clinical assessment were excluded from the study. Written informed consent from the parents was obtained prior to enrollment. Clinical and demographic data were recorded on a structured proforma, including antenatal and perinatal history, developmental and family history.
Assessments
Functional assessments
The severity of movement disability among children with CP was assessed by the Gross Motor Function Classification System (GMFCS). GMFCS was first proposed in 1997 and has ordinal levels I to V for ambulation and mobility of children with CP. 16 The expanded and revised GMFCS (GMFCS-E&R) includes an age band for youth 12-18 years of age, proposed by Palisano et al 17 in 2007. The Manual Ability Classification System (MACS) was used to evaluate bilateral hand use ability in children with CP when holding an object in daily activities. The MACS was proposed by Eliasson et al 18 in 2006, and has 5 ordinal levels I to V. The Quality of Upper Extremity Skills Test (QUEST) was used to assess hand function ability. 19 The QUEST scale was proposed by DeMatteo et al 19 in 1993 and has 4 domains, including dissociated movement, grasp, protective extension, and weight bearing.
Neurodevelopmental assessments
The assessment was done by using the Developmental Profile-3 (DP-3). 20 DP-3 was updated by Alpern in 2002 and has been used for screening and diagnosing issues in development in children aged birth to 12 years. It has 5 domains, including physical, adaptive behavior, socio-emotional, cognition, and communication. The overall General Developmental Score (GDS) generated was categorized as delayed (GDS < 70), below average (70-84), average (85-115), and above average (116-130). 20
Other assessments
The health-related quality of life (QOL) was assessed by the caregiver questionnaire (CQ), which measures the caregiver's difficulties and satisfaction with their child's progress in 4 areas-personal care, positioning/transferring, comfort, and interaction/communication-using a 29-item questionnaire. 21 It was proposed by Schneider et al 21 in 2001. Neuroimaging of the brain was done in all children. Assessment of comorbidities was done through history, physical examination, and appropriate laboratory investigations as indicated clinically as part of their routine management.
Statistical Analysis
Descriptive statistics were used to summarize demographic, clinical, and radiologic characteristics. Given the exploratory and hypothesis-generating nature of this cross-sectional study, correlation analyses (Spearman coefficient) were performed to examine associations between functional, developmental, and caregiver-reported outcomes, without adjustment for multiple comparisons.
Results
Ninety children with a clinical diagnosis of HCP were screened. Of these, 20 children were excluded: 4 had bilateral involvement, 4 had spastic diplegia, 1 child had neuroregression associated with a neurometabolic disorder, 1 child had congenital heart disease precluding a thorough clinical assessment, 8 children did not return for neuroimaging after the initial evaluation, and 2 children were lost to follow-up. Hence, n = 70 children with HCP were included in the final analysis.
Demographic and Clinical Details
The mean age was 62.4 ± 38.3 months and the median age was 50 (range 12-144) months. Majority of the children were boys (71%, n = 50/70) and had right-sided hemiparesis (53%, n = 37/70). The major concerns at presentation were difficulty in walking (35.7%, n = 25/70) and reduced hand movements (32.8%, n = 23/70). Antenatal risk factors were identified in 30% (n = 21/70) of the children. The demographics are summarized in Table 1. Majority of the children were ambulatory with or without assistance (levels I-III) and only 6 children were severely disabled and nonambulatory (levels IV and V).
Baseline Demographic and clinical characteristics in Children With HCP (n = 70).
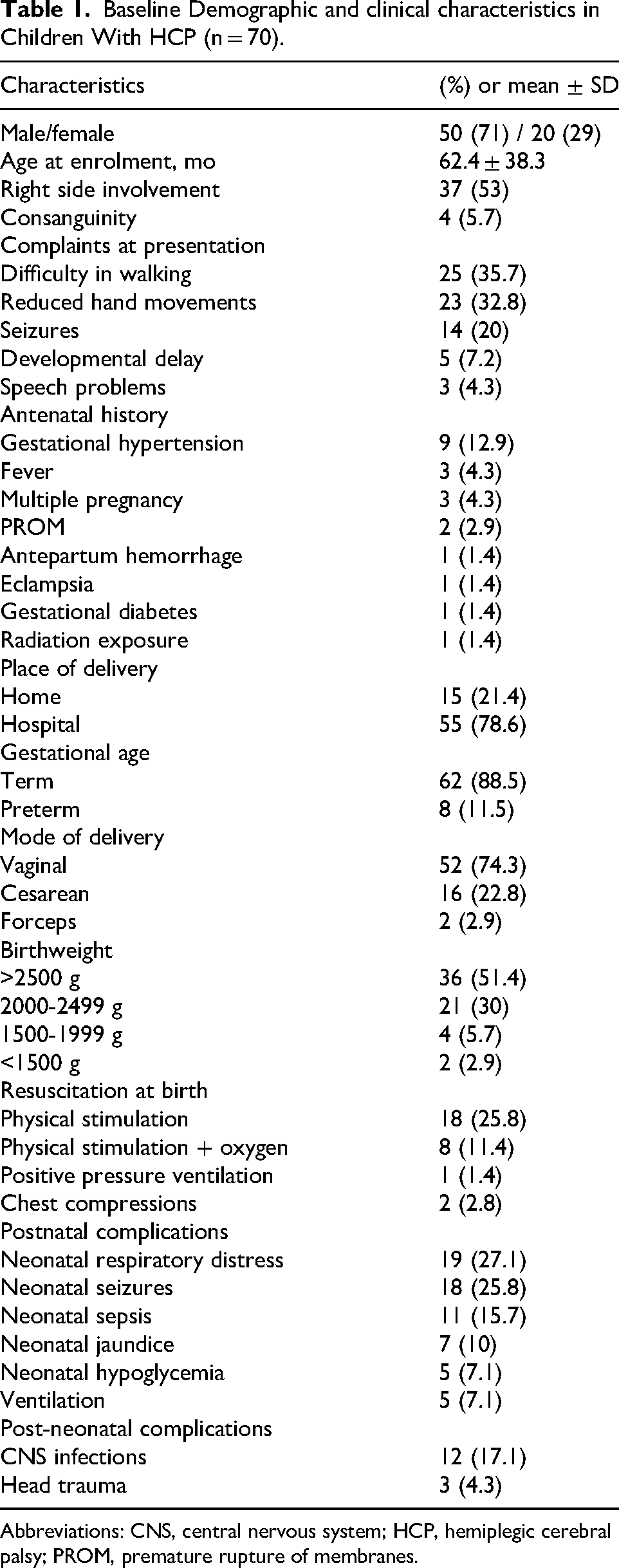
Abbreviations: CNS, central nervous system; HCP, hemiplegic cerebral palsy; PROM, premature rupture of membranes.
Most of the children 85.7% (n = 60/70) had mild to moderately reduced hand function ability. The majority of children with HCP were in level II (n = 27/70, 38.6%) of MACS. Mean QUEST score was 68.1 ± 6.7 with a median of 68 (range 48-84), indicating mild to moderate impairment of upper-extremity quality, particularly in dissociated movements and grasp. A QUEST score of less than 50 was found in only 1 child. In the spasticity rating, 61.4% (n = 43/70) of the children had moderate spasticity followed by mild grade, which was seen in 34.3% (n = 24/70) of the children. Severe spasticity noted in 3 children. The scales of assessments are summarized in Table 2.
Scales of Assessments and Neuroimaging.
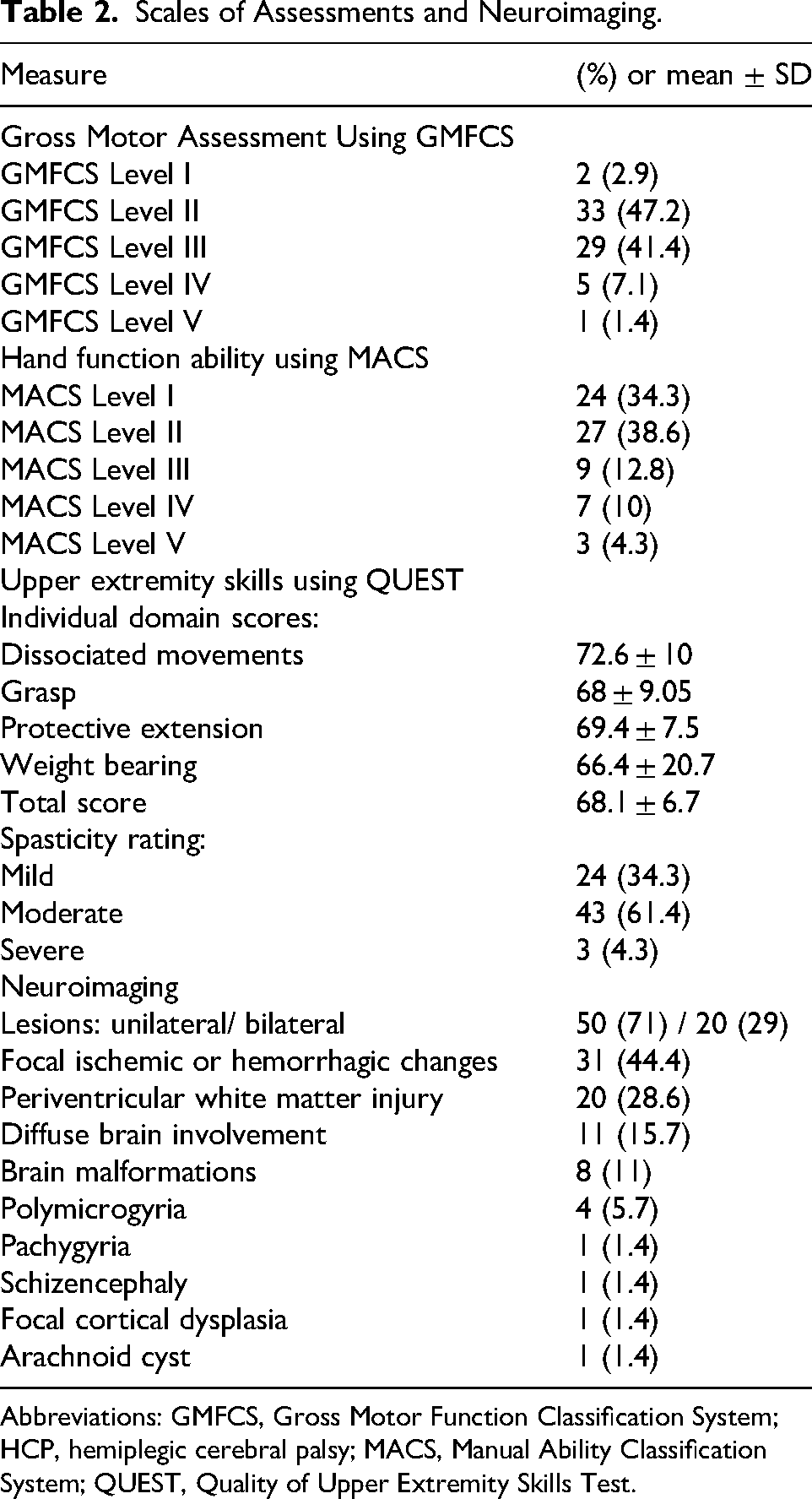
Abbreviations: GMFCS, Gross Motor Function Classification System; HCP, hemiplegic cerebral palsy; MACS, Manual Ability Classification System; QUEST, Quality of Upper Extremity Skills Test.
Comorbidities
Among the 4 subgroups of CQ, children with HCP mainly had problems in personal care and positioning/transfer areas. Epilepsy was seen in 38.5% (n = 27/70) of children. Among these, 5 children (18.5%) had only 1 episode of seizure. Status epilepticus at the onset was found in 51.9% (n = 14/27) of the children. The mean age of onset of epilepsy was 27.9 ± 23.9 months (range 3-96 months). The median number of anti-seizure medications in these children was 1 (range 1-2). The comorbidities are summarized in Table 3.
Comorbidities in Children with HCP and Caregiver Questionnaire Assessment.
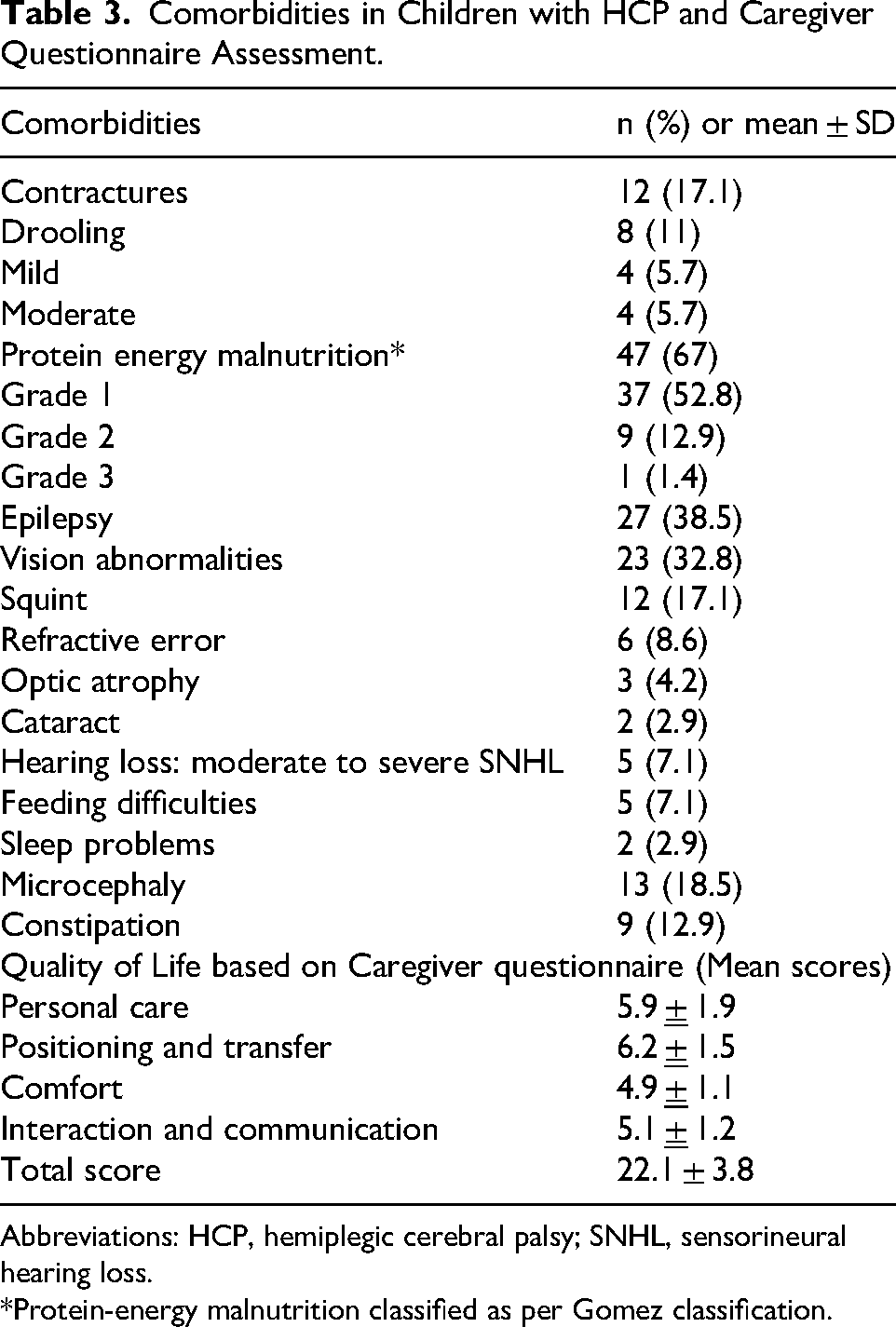
Abbreviations: HCP, hemiplegic cerebral palsy; SNHL, sensorineural hearing loss.
*Protein-energy malnutrition classified as per Gomez classification.
Neuroimaging demonstrated a spectrum of lesions, predominantly focal ischemic or hemorrhagic insults (44.4%), followed by periventricular white matter injury (28.6%) and diffuse brain involvement (15.7%). Structural malformations included polymicrogyria, pachygyria, schizencephaly, focal cortical dysplasia, and arachnoid cysts (Table 2). The types of seizures and EEG findings are shown in Figure 1A-B. On DP-3 assessment, mean GDS was 77.5 ± 18.7 (range 40-115). In 37% (n = 26/70), GDS was found in the average range (85-115). It was delayed (<70) in 33% (n = 23/70) and below average (70-84) in 30% (n = 21/70) of the children. The neurodevelopmental assessment by DP-3 is summarized in Table 4.
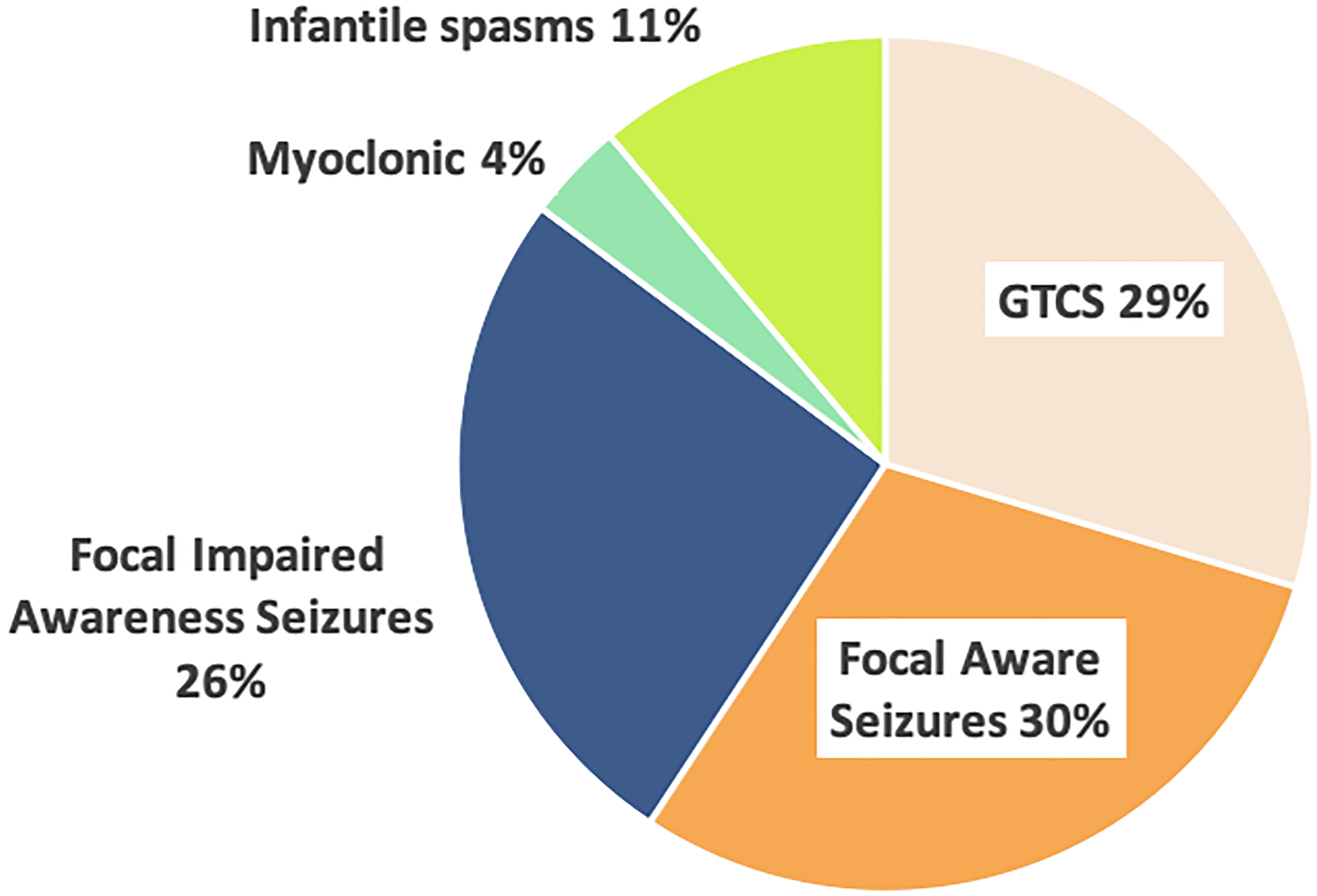
Epilepsy in hemiplegic cerebral palsy. (A) Types of seizures noted in children with hemiplegic cerebral palsy (A).
Developmental Profile-3 (DP-3) Scoring in Children With HCP (n = 70).
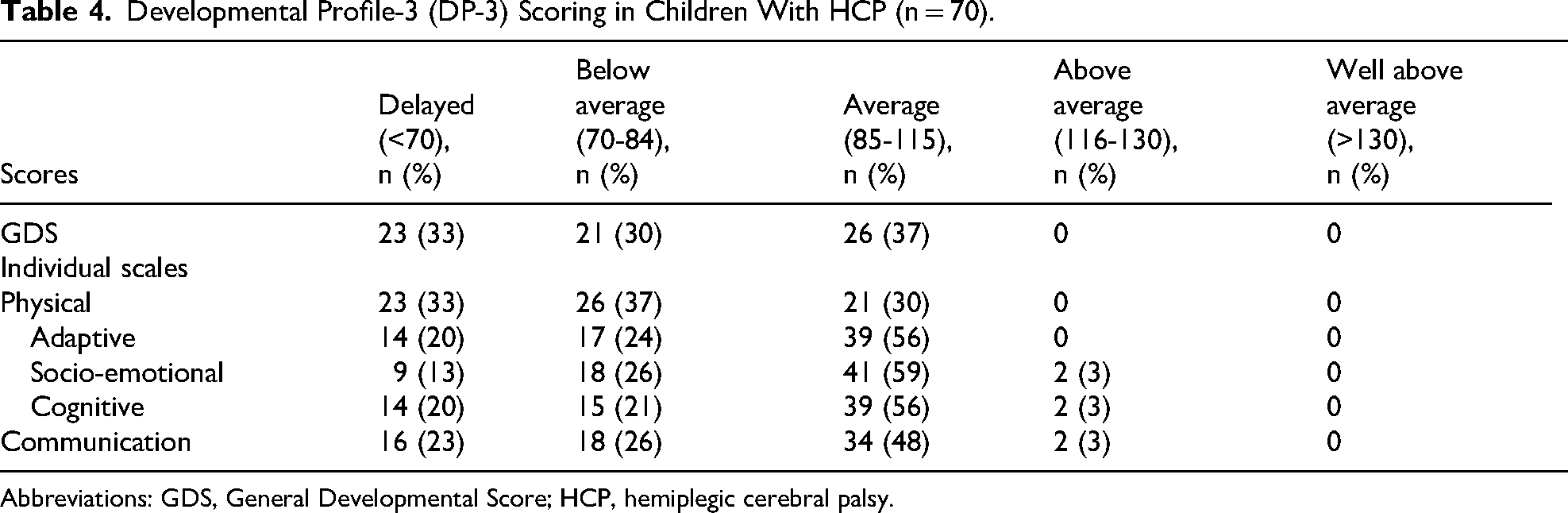
Abbreviations: GDS, General Developmental Score; HCP, hemiplegic cerebral palsy.
Correlation Analysis
Increasing age was significantly associated with better functional outcomes, as reflected by negative correlations with GMFCS (r = –0.376, P = .001), MACS (r = –0.525, P = .001), and caregiver burden (r = –0.605, P = .001), and a positive correlation with QUEST scores (r = 0.336, P = .004).
Comparison between children with epilepsy (n = 27) and those without (n = 43) revealed no statistically significant differences in gross motor function (mean GMFCS 2 ± 1 in both groups), manual ability (mean MACS 3 ± 0.5 in both groups), upper limb quality (QUEST 68 ± 6 vs 68.8 ± 7), developmental scores (DP3 73.4 ± 20 vs 80 ± 18), or caregiver burden (CQ 23 ± 3.7 vs 21 ± 3.8) (all P > .01), indicating that epilepsy did not independently influence disability severity in this cohort.
Inter-scale correlations demonstrated that poorer manual ability was significantly associated with higher GMFCS levels (r = 0.553, P = .001), lower QUEST scores (r = –0.416, P = .001), and greater caregiver burden (r = 0.325, P = .004), whereas better developmental functioning (DP3) was positively related to higher-quality upper extremity skills (QUEST) (r = 0.318, P = .007). The correlation analysis is summarized in Supplementary Table 1. Together, these findings highlight the interconnected nature of motor, manual, and developmental impairments in hemiplegic CP, and underscore the functional gains that accrue with age.
Discussion
The index study provides a comprehensive clinical-radiologic characterization of children with HCP from a tertiary pediatric neurology center, complementing the limited epidemiologic and functional data on HCP from LMICs. The common comorbidities associated with HCP reported in literature include epilepsy, microcephaly, drooling, and feeding difficulties, similar to the findings noted in the index study. In our cohort, functional outcomes were largely favorable, with most children demonstrating mild motor impairment and good ambulatory potential, consistent with earlier reports that HCP carries the most favorable functional prognosis compared with spastic quadriplegic and diplegic forms.4,22
The observed age-related differences in gross-motor, manual, and upper limb skills with parallel reduction in caregiver burden may reflect a combination of neurodevelopmental maturation, variability in severity across age groups, and ongoing therapeutic exposure in routine clinical care.11,23–25 However, given the cross-sectional design, these findings represent associations rather than longitudinal changes within individuals. These findings support the importance of early identification and structured intervention strategies in children with HCP, although the specific contribution of rehabilitation could not be quantified in this study.
The prevalence of epilepsy (38.5%) in our cohort is comparable to previously reported ranges (25%-43%) in children with hemiplegic CP. Similarly, the predominance of mild motor impairment and MACS level II and III distribution aligns with findings from international cohorts, although variations in lesion profile and access to early intervention may influence outcomes across settings.26–31 The absence of a significant neurologic impact may reflect unilateral injury and effective seizure control, or the fact that subtle neuropsychological effects may not be captured by DP-3. Uneven cognitive profiles were noted on studies in children with HCP.29,32,33 Tillberg et al 29 reported 38% intellectual disability (ID) and uneven cognitive profile in 57% of them. They also underscored the importance of cognitive assessment in children with HCP.
Third, neuroimaging profiles in our cohort were dominated by focal ischemic lesions, particularly in vascular territories affected in perinatal arterial ischemic stroke, consistent with the established role of perinatal arterial ischemic stroke in HCP.8,10,34 The presence of periventricular white matter injury, diffuse encephalopathy, and cortical malformations underscores the etiologic heterogeneity of HCP and confirms that clinical asymmetry does not preclude the bilateral or diffuse injury.10,35 Tillberg et al29,30 noted that the intellectual disability and/or epilepsy were associated with the type or extent of underlying brain lesions in children with HCP. 31 These observations emphasize the value of routine neuroimaging in all children presenting with presumed hemiplegic CP, to refine prognosis and guide rehabilitation strategies.
The index study's findings indicate that children with HCP in this setting tend to have principally mild functional involvement but demonstrate relatively favorable functional profiles across age groups. Developmental delay was documented in one-third of children, and caregiver burden was highest in tasks requiring personal care and physical transfers. Increasing age correlated significantly with better motor and hand function and lower caregiver burden. We highlight that dedicated intervention opportunities including early motor enrichment, targeted upper-limb therapy, systematic imaging, and caregiver-support programs, to optimize long-term outcomes in children with HCP.
Limitations and Strengths
The cross-sectional design limits causal interpretation, and age-related differences should not be interpreted as longitudinal improvement. Additionally, detailed rehabilitation data were not systematically captured, precluding assessment of the independent impact of therapeutic interventions on functional outcomes. A proportion of screened children were excluded, including those who did not complete neuroimaging. In our setting, this is often related to logistical and socioeconomic constraints (e.g., need for sedation, travel, cost), although the possibility of selection bias cannot be excluded. Furthermore, incomplete data in the excluded group precluded formal comparison with the analyzed cohort. Despite these considerations, key strengths include a well-defined hemiplegic CP cohort, and use of GMFCS, MACS, QUEST, DP-3, CQ, and MRI provide a holistic functional-developmental-radiologic characterization of this population.
Conclusion
Children with HCP exhibit a consistent pattern of structural brain injury, substantial comorbidity burden, and measurable functional limitations, underscoring the need for early, targeted multidisciplinary intervention. Epilepsy, though common, does not automatically translate into worse functional or developmental status, and focal ischemic lesions remain the leading substrate. Understanding the spectrum of motor impairment, neurodevelopmental challenges, and coexisting disorders is vital for designing individualized therapy programs and strengthening multidisciplinary care.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738261456886 - Supplemental material for Clinical, Neuroimaging, and Functional Profile of Children With Hemiplegic Cerebral Palsy: A Cross-Sectional Study From a Tertiary Care Center
Supplemental material, sj-docx-1-jcn-10.1177_08830738261456886 for Clinical, Neuroimaging, and Functional Profile of Children With Hemiplegic Cerebral Palsy: A Cross-Sectional Study From a Tertiary Care Center by Tandra Harish Varma, Arushi Gahlot Saini, Pradeep Kumar Gunasekaran, Naveen Sankhyan, Prahbhjot Malhi, Niranjan Khandelwal and Pratibha Singhi in Journal of Child Neurology
Footnotes
Acknowledgment
The authors would like to thank all the children and their parents for their participation in the study.
Ethical Publication Statement
We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Patient Consent Statement
Informed consent was obtained from parents/legal guardians.
Authors contributions
Study Design, Writing, Editing, Drafting: Tandra Harish Varma, Arushi Gahlot Saini, Pratibha Singhi. Critical Revision, Final Approval: Tandra Harish Varma, Arushi Gahlot Saini, Pradeep Kumar Gunasekaran, Naveen Sankhyan, Prahbhjot Malhi, Niranjan Khandelwal, Pratibha Singhi.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Permission to Reproduce Material from Other Sources
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.