
Abstract
Objectives
This study aimed to analyze the burden of idiopathic developmental intellectual disability (IDII) attributed to lead exposure in Asian children and adolescents aged <20 years from 1990 to 2021.
Methods
We estimated the disease burden using disability-adjusted life years (DALYs). Temporal trends from 1990 to 2021 were analyzed using joinpoint regression. Decomposition analyses were performed to disaggregate changes in DALYs. Health inequality analyses and frontier analyses were applied to explore the relationship between DALYs and the socio-demographic index (SDI). The Bayesian age-period-cohort model was employed to predict the future disease burden by 2035.
Results
The number of IDII DALYs attributable to lead exposure among children and adolescents in Asia decreased from 1.11 million (95% uncertainty interval [UI]: 0.48-1.96 million) in 1990 to 0.82 million (95% uncertainty interval: 0.36-1.49 million) in 2021, which was primarily driven by epidemiologic changes. Females and the 10-14-year age group faced the highest risk. Lower-SDI regions, especially South Asia, bore a disproportionately higher burden, with absolute health inequality narrowing but relative inequality remaining prevalent between 1990 and 2021. Projections to 2035 showed a continued decline in disease burden in India and Pakistan, in contrast to rising in Afghanistan and Yemen.
Conclusions
This study underscored the critical need to strengthen targeted lead exposure interventions addressing gender, age, and regional disparities.
Keywords
Lead (Pb) is a heavy metal widely used in fuel additives, household paints, water pipes, and electronic devices. As a cumulative toxicant, lead primarily impairs the nervous, hematopoietic, and gastrointestinal system. 1 In 2021, lead exposure accounted for 1.54 million deaths and 33.9 million disability-adjusted life years (DALYs) globally, posing a significant global public health burden. 2 Among the various toxic effects of lead, its chronic neurotoxicity is particularly prominent and has long-term adverse effects on the developing nervous system. 3 Children are more susceptible to lead-induced neurotoxicity, absorbing 4-5 times more lead than adults. 4 Even when children's blood lead levels (BLLs) are maintained below 5 μg/dL, 5 early exposure to low levels of lead can still significantly impair brain and nervous system development, leading to cognitive impairment, 6 reduced intelligence quotient (IQ), 7 and difficult personality traits and multiple mental disorders in adulthood. 8
Intellectual disability (ID) has been clearly identified as one of the most profound consequences affecting children's growth and development. 5 ID is a type of neurodevelopmental disorder (NDD) characterized by deficits in intellectual and adaptive functioning, typically manifesting clinical symptoms during the developmental stage. 9 Children with ID not only exhibit below-average intelligence (IQ < 70) but also encounter significant difficulties or delays in developing movement, communication, social interaction, and cognitive skills. 10 According to the Global Burden of Diseases (GBD) 2021 study, idiopathic developmental intellectual disability (IDII), as part of the intellectual disability impairment envelop, accounted for 3.81 million DALYs (95% uncertainty interval [UI]: 1.76-6.52 million), highlighting its severe health hazards. 11 In addition, the Cost of Disorders of the Brain in Europe (CDBE-2010) study further pointed out that among health care expenditures for various mental disorders, the cost of ID ranked second only to anxiety disorders. 12 However, the needs of individuals with ID remain largely unmet. 13 A population-based epidemiologic survey from the United Kingdom indicated that only one-third of children with ID had access to specialized mental health services. 14 Even in countries that have established evidence-based service guidelines, the mental health needs of children with ID have not been adequately addressed, and the gap between service supply and actual demand remains prominent. 15
Although previous studies have outlined the global burden and trends of IDII associated with lead exposure, there has been lack of in-depth analyses focusing on specific regions and age groups.16–19 Based on the data from GBD 2021, we aimed to analyze the disease burden, temporal trends and health inequalities of IDII due to lead exposure among Asian children and adolescents from 1990 to 2021, stratified by sex, age group, country, and territory. Furthermore, we conducted a decomposition analysis based on demographic and epidemiologic factors, explored the relationship between disease burden and the socio-demographic index (SDI), and projected the disease burden of IDII due to lead exposure up to 2035.
Materials and Methods
Study Data
The GBD 2021 data employed in this study were obtained from the Global Health Data Exchange (query tool: https://vizhub.healthdata.org/gbd-results/). This study used DALYs to assess the burden of IDII attributable to lead exposure. Data on DALYs for IDII associated with lead exposure from 1990 to 2021 were obtained from GBD 2021, stratified by sex (both sexes, males, and females), age group (<20 years: <5 years, 5-9 years, 10-14 years, and 15-19 years), and 49 countries and territories in Asia. The 49 countries and territories in Asia were classified into 5 subregions by the United Nations statistical division based on geographical and epidemiologic similarity, including East Asia, West Asia, Southeast Asia, South Asia, and Central Asia. 20 The disease burden in this study was assessed using the number, crude rate, and age-standardized rate (ASR) of DALYs. The DALYs rates were expressed as the value per 100 000 population, and both indicators were reported with their corresponding 95% UIs. The 95% UIs were represented by the 2.5th and 97.5th percentile ordered estimates derived from 1000 random draws based on the uncertainty distribution.
Statistical Analysis
The estimated annual percentage change (EAPC) and its 95% CI were calculated to quantify changes in the IDII burden in Asia from 1990 to 2021.The joinpoint regression method was employed to reflect the trends in IDII DALYs count and age-standardized DALYs rate (ASDR) from 1990 to 2021, which were represented by the annual percentage change (APC), average annual percentage change (AAPC), and their respective 95% CIs. Decomposition analyses were conducted on population size, age structure, and epidemiologic changes to explore the factors driving changes in the IDII disease burden from 1990 to 2021. We used the Slope Index of Inequality (SII) and the Concentration Index (CI) to evaluate the health inequality of the IDII disease burden among children and adolescents in Asia. Spearman correlation analysis and frontier analysis was used to explore the relationship between the IDII burden and SDI. The Bayesian age-period-cohort model (BAPC) was used to predict the IDII burden among children and adolescents in high-burden countries up to 2035. Further details on the statistical methods could be found in the supplementary appendix (Supplemental Methods). All statistical analyses and result visualizations were performed using R software (version 4.4.1) and Joinpoint software (version 5.1.0.0). A 2-tailed P value <.05 was considered statistically significant.
Result
IDII Burden From Lead Exposure in Asia
From 1990 to 2021, Asia experienced a significant overall decline in IDII burden attributable to lead exposure (Figure 1; Figure 2). The number of DALYs decreased from 1.11 million (95% UI: 0.48 million, 1.96 million) to 0.82 million (95% UI: 0.36 million, 1.49 million), and age-standardized DALYs rate (ASDR) decreased from 53.71 per 100 000 population (95% UI: 22.83, 95.42) to 43.55 per 100 000 population (95% UI: 18.44, 79.01) with an estimated annual percentage change (EAPC) of −0.72 (95% UI: −0.81, −0.63) (Table S1). Both DALYs counts (AAPC = −0.943, 95% CI: −1.033 to −0.853) and ASDR (AAPC = −0.666, 95% CI: −0.729 to −0.602) exhibited substantial declines (Table 1; Table 2). Joinpoint regression analyses identified 5 significant turning points for both DALY number (1993, 2000, 2003, 2015, 2018) and age-standardized rates (ASRs) of DALYs (1994, 2000, 2003, 2014, 2018) (Figure 2). Notably, DALYs count showed an upward trend (APC = 0.290, 95% CI: 0.186-0.393) from 1993 to 2000 (Table 1; Figure 2A), whereas ASDR similarly demonstrated a slight increase (APC = 0.149, 95% CI: 0.040 to 0.257) between 1994 and 2000 (Table 2; Figure 2B). Regionally, South Asia carried the heaviest burden in 2021 (Figure 1). Specifically, India, Pakistan, China, Afghanistan, Indonesia, and Yemen reported the highest total DALYs, whereas India, Afghanistan, Yemen, Pakistan, Nepal, and Palestine had the highest ASDR (Table S1).
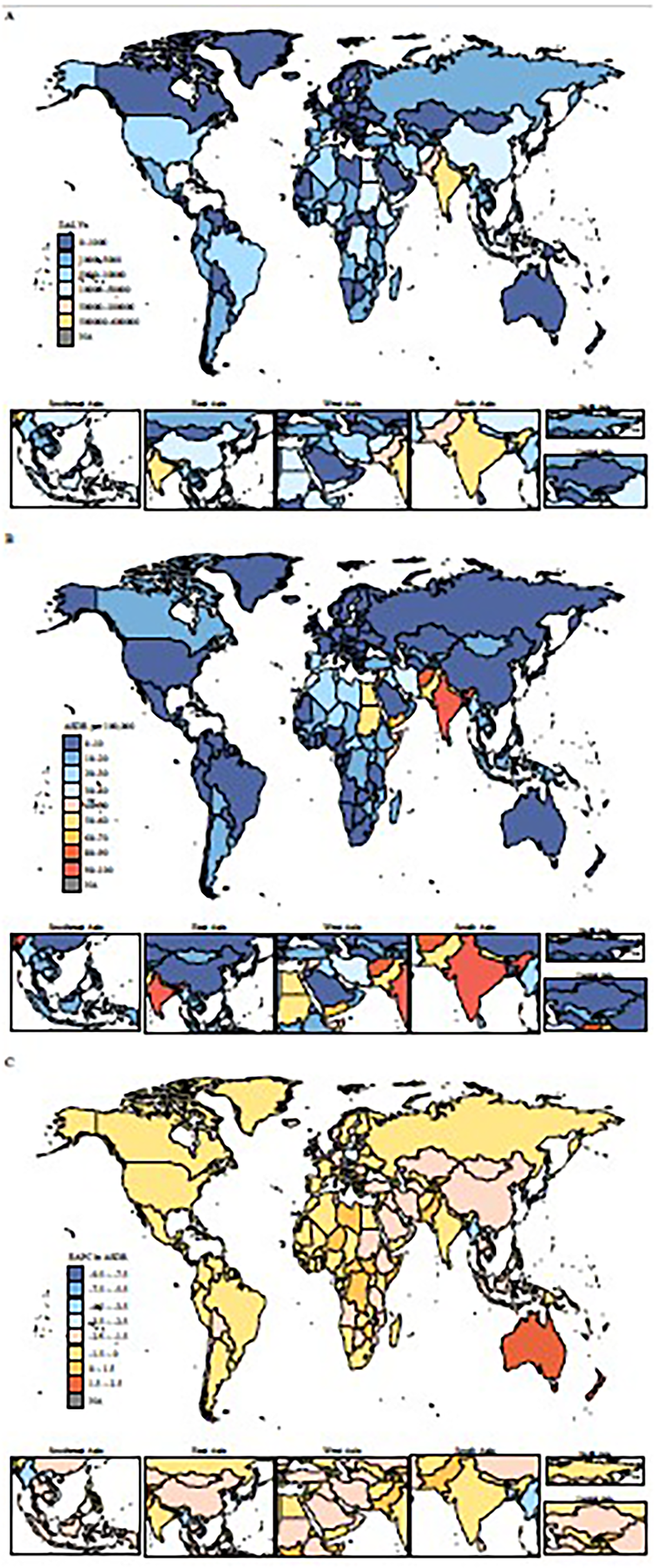
The global patterns and temporal trend of DALYs for IDII attributable to lead exposure among children and adolescents aged <20 years across 204 countries and territories. (A) The number of DALYs in 2021. (B) The ASDR in 2021. (C) The EAPCs of ASDR from 1990 to 2021. ASDR, age-standardized DALYs rate; DALYs, disability-adjusted life-years; EAPCs, estimated annual percentage changes; IDII, idiopathic developmental intellectual disability.
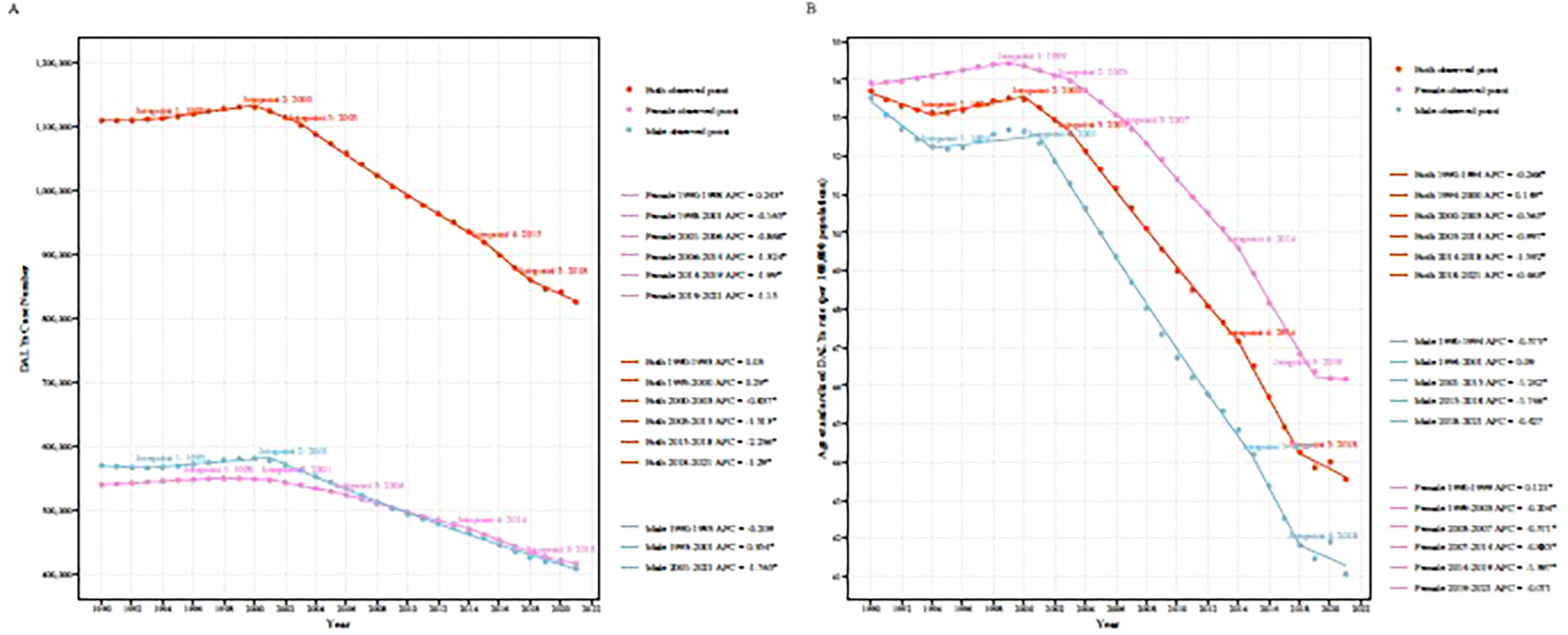
Joinpoint regression analysis of DALYs for IDII due to lead exposure in Asian children and adolescents aged <20 years from 1990 to 2021, by sex. (A) DALYs case number. (B) Age-standardized DALYs rate. DALYs, disability-adjusted life-years; IDII, idiopathic developmental intellectual disability.
The APC and AAPC in Number of IDII DALYs in Asia From 1990 to 2021, by Sex.
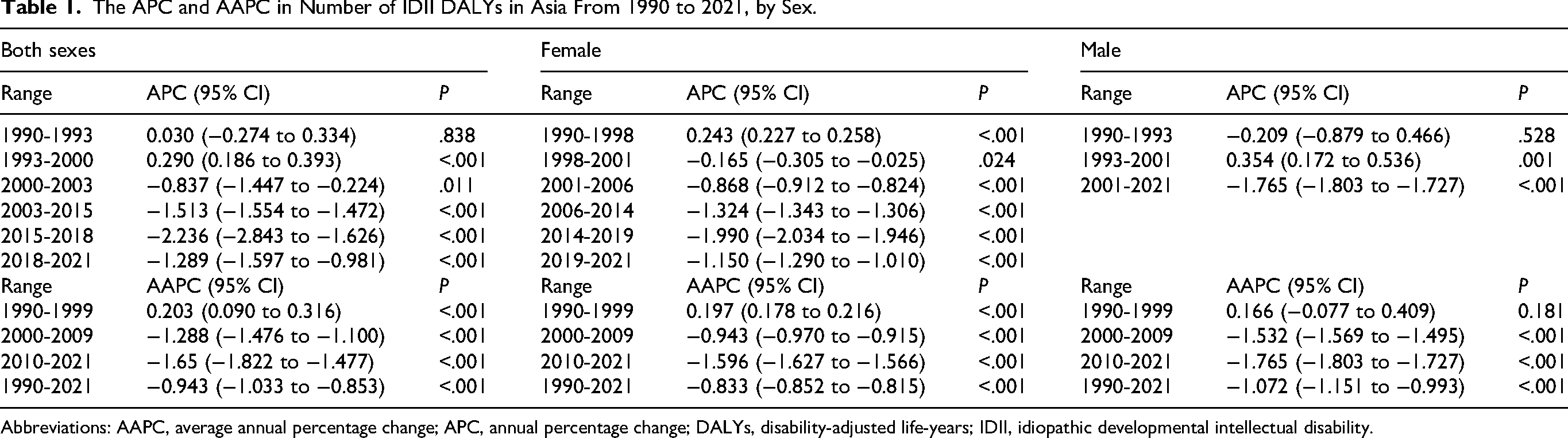
Abbreviations: AAPC, average annual percentage change; APC, annual percentage change; DALYs, disability-adjusted life-years; IDII, idiopathic developmental intellectual disability.
The APC and AAPC in ASR of IDII DALYs in Asia From 1990 to 2021, by Sex.
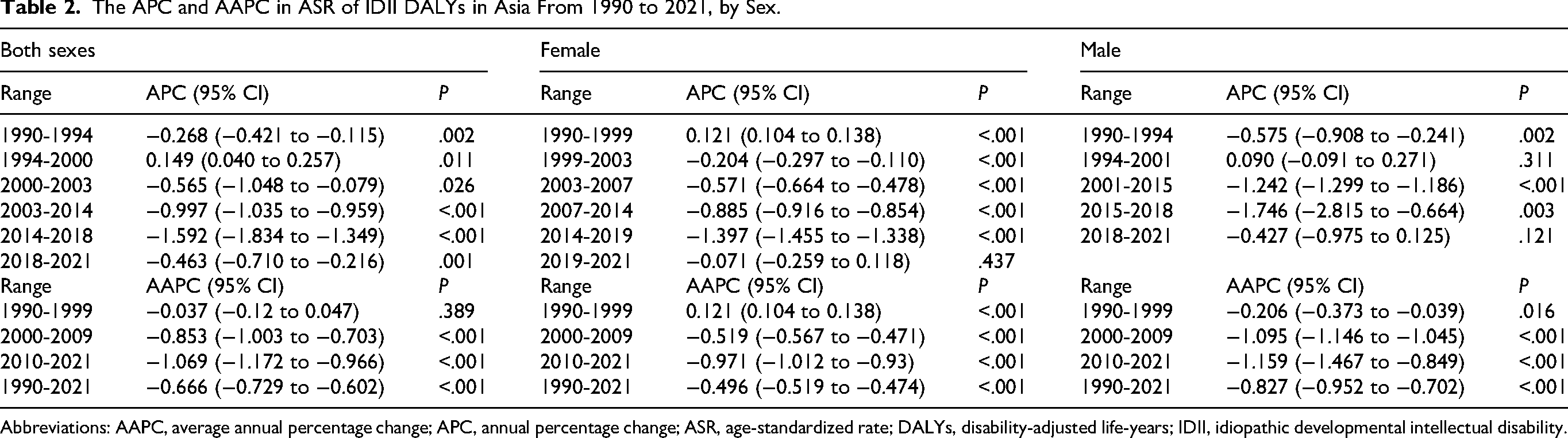
Abbreviations: AAPC, average annual percentage change; APC, annual percentage change; ASR, age-standardized rate; DALYs, disability-adjusted life-years; IDII, idiopathic developmental intellectual disability.
Sex- and Age-Specific Trends in Burden of IDII due to Lead Exposure in Asia
Sex-stratified analyses further revealed that the burden of IDII due to lead exposure decreased significantly in both males and females between 1990 and 2021 (males: EAPC = −0.90, 95% CI: −0.99 to −0.80; females: EAPC = −0.55, 95% CI: −0.64 to −0.45) (Table S1), but the decline was more pronounced in males than females for both DALYs count (males: AAPC = −1.072, 95% CI: −1.151 to −0.993; females: AAPC = −0.833, 95% CI: −0.852 to −0.815) (Table 1) and ASDR (males: AAPC = −0.827, 95% CI: −0.952 to −0.702; females: AAPC = −0.496, 95% CI: −0.519 to −0.474) (Table 2). Age-stratified analyses showed that IDII burden due to lead exposure increased with age regardless of sex in both 2019 and 2021, with the 10-14-year age group bearing the most prominent burden. Furthermore, from 1990 to 2021, the DALY rate of IDII caused by lead exposure showed a downward trend across all age groups <20 years old (Figure 3).
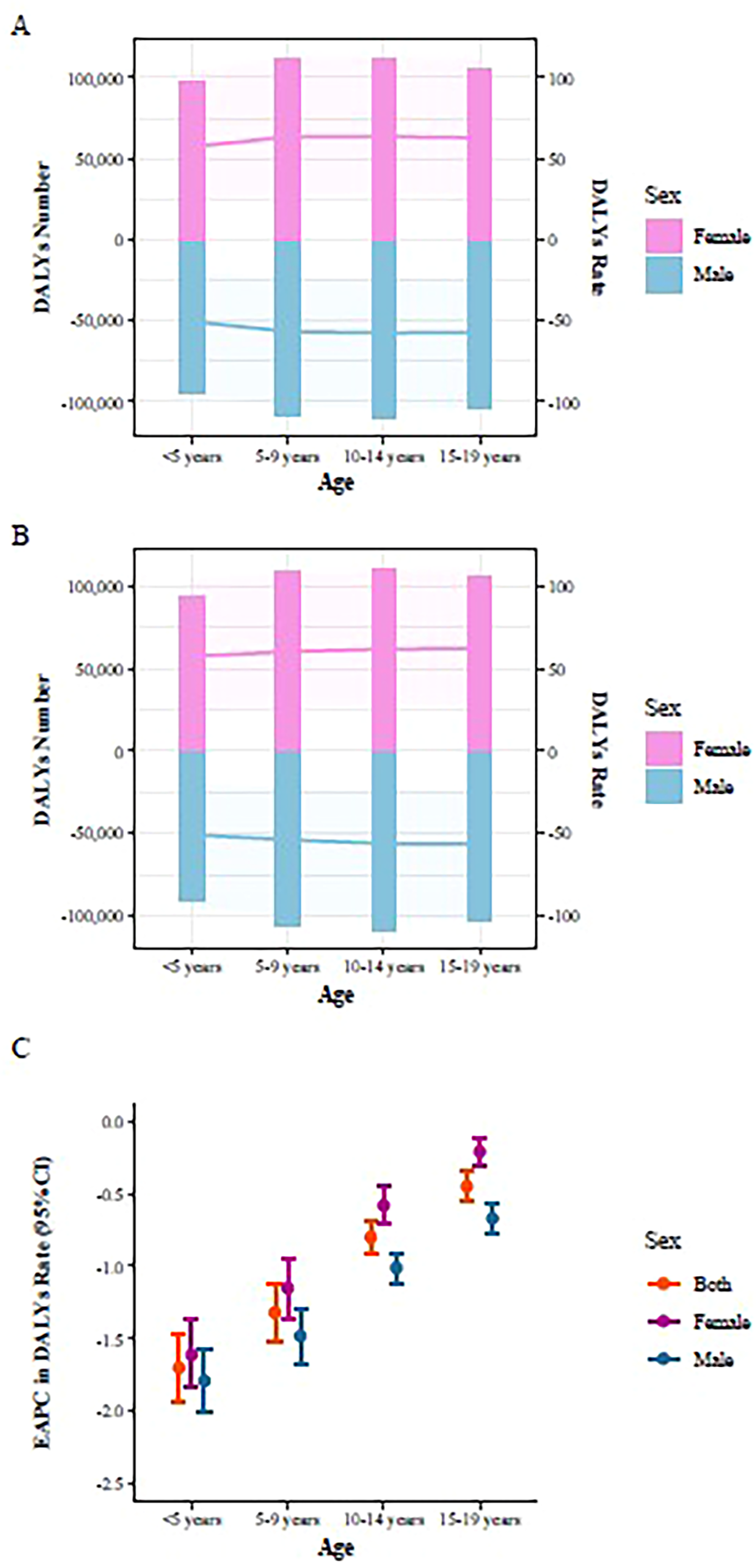
The burden of lead-attributable IDII in Asian children and adolescents aged <20 years, by age and sex. (A) DALYs case number and crude rates by age and sex, 2019. (B) DALYs case number and crude rates by age and sex, 2021. (C) The EAPCs in DALYs crude rates by age and sex, 1990-2021. DALYs, disability-adjusted life-years; EAPCs, estimated annual percentage changes; IDII, idiopathic developmental intellectual disability.
Decomposition Analysis of IDII Burden Attributable to Lead Exposure in Asia
We conducted decomposition analyses at the overall Asian level and specifically for 4 Asian countries (India, Afghanistan, Yemen, and Pakistan) that demonstrated both high DALY counts and high ASDR in 2021 (Table S2; Figure S1). The results indicated that the decline in the IDII burden attributable to lead exposure in Asia from 1990 to 2021 was predominantly explained by epidemiologic changes (112.89%). Among the 4 selected countries, India showed similar trends in lead exposure–related IDII burden changes and contributing factors to the overall Asian pattern. In contrast, both Pakistan and Yemen experienced an increasing trend in lead exposure–induced IDII burden, primarily driven by population growth (Pakistan: 105.66%; Yemen: 140.97%). This trend was partially offset by population aging and epidemiologic changes, with the latter contributing more significantly to the mitigation. Afghanistan also exhibited a growing trend in the lead-related IDII burden, primarily driven by population growth (114.98%), with a burden-reducing effect from epidemiologic changes.
Health Inequalities in IDII Burden due to Lead Exposure Across SDI Levels
From 1990 to 2021, the ASDRs showed a consistent decline with increasing SDI levels, which is consistent with the observed pattern (r = –0.65, P < .001) in 2021 (Figure S2). Health inequalities analysis indicated a declining trend in both absolute and relative inequalities associated with SDI between 1990 and 2021 (Figure S3). The negative value of SII for the DALYs rate suggested that countries and territories with lower SDI levels in Asia disproportionately bore a higher burden. The disparity in the DALYs rate between the highest- and lowest-SDI countries and territories decreased from −67.89 in 1990 to −30.96 in 2021, indicating a reduction in the distributional gap of disease burden. The concentration index showed only a slight decline, from −0.48 in 1990 to −0.47 in 2021, reflecting persistent relative inequalities between low- and high-SDI countries and territories.
Frontier Analysis of IDII Burden Attributable to Lead Exposure
The frontier analysis was performed using ASDR and SDI to explore the potential for improvement in IDII burden due to lead exposure among individuals in the under-20 age group in Asian countries and territories (Figure S4). The study identified the top 12 countries with the largest gaps from the frontier (effective difference range: 15.81-88.18), including India, Afghanistan, Yemen, Pakistan, Nepal, Palestine, the Syrian Arab Republic, Iran (Islamic Republic of), Jordan, Lebanon, Bhutan, and Türkiye. Countries and territories with low SDI (<0.5) and relatively small effective differences included Bangladesh, Timor-Leste, the Lao People's Democratic Republic, and Cambodia. High-SDI (>0.85) countries and territories with significant potential for improvement were Taiwan (Province of China), Japan, the Republic of Korea, and Singapore.
Projection of IDII Burden due to Lead Exposure to 2035
Four Asian countries (India, Afghanistan, Yemen, and Pakistan) were selected to perform a BAPC model analysis, predicting the burden of IDII attributable to lead exposure from 2022 to 2035 (Figure S5; Table S3). The number of DALYs and the ASDRs in India and Pakistan are projected to show a declining trend. In Afghanistan, although the number of DALYs is expected to increase, the ASDRs will decrease. Conversely, Yemen is anticipated to experience a rise in both the number of DALYs and the ASDRs.
Discussion
This study comprehensively analyzed the characteristics, trends, influencing factors, and health inequalities of the disease burden of IDII attributable to lead exposure among individuals under 20 years of age across Asia and its 49 countries and territories from 1990 to 2021, and projected future trend of burden changes in high-burden countries and territories from 2022 to 2035. Overall, the burden of IDII due to lead exposure in Asia showed a significant downward trend from 1990 to 2021, primarily driven by epidemiologic changes. However, South Asia and countries such as India, Pakistan, Afghanistan, and Yemen continue to bear a heavy burden. Females and children and adolescents aged 10-14 years bore the highest risk. Lower-SDI countries and territories disproportionately bore a higher burden, and relative health inequality still persisted.
Our research indicated that over the past few decades, Asia has experienced an overall decline in both the DALYs count and the ASDR related to lead exposure–induced IDII. This trend is consistent with the global pattern of the burden of IDII associated with lead exposure and is likely attributable to epidemiologic changes, including the implementation of lead exposure reduction strategies. 16 Since the gradual phase-out of leaded gasoline by countries starting in the 1970s and the complete elimination of lead from automotive gasoline worldwide by 2021, there has been a significant and rapid reduction in both lead exposure and blood lead levels in the population. 21 Relevant policies have been further extended to industrial processes, paints, food, drinking water, and household lead contamination, with corresponding limits established for lead exposure.22–24 Notably, a slight increase in disease burden was observed in Asia between 1993 and 2000, which may be linked to factors such as rapid industrialization, inadequate environmental regulation, and accelerated urbanization. The expansion of industrial activities coupled with the lag in pollution control measures during this period heightened the risk of population lead exposure.
Previous GBD studies indicated that IDII attributable to lead exposure mainly affects children and adolescents18,19; thus this study focused on populations <20 years old. Age-stratified analyses in this study showed that the disease burden increased with age, with the 10-14-year age group being the most prominent. This is closely related to lead exposure patterns, susceptibility and lead accumulation at different life stages. The adverse effects of lead exposure can be traced to fetal development, where maternal lead crosses the placental barrier, impairing fetal neurodevelopment and increasing susceptibility to later health outcomes. 25 Infants and preschool children are more vulnerable to lead poisoning because of rapid brain development and higher lead absorption rate, and frequent hand-to-mouth behaviors increased the risk of ingesting lead contaminants such as toys and dirt. 26 Moreover, lead accumulates in the human body with advancing age. Long-term follow-up data from the Port Pirie Cohort Study indicated that cumulative lead exposure during childhood and early adolescence was a strong predictor of later developmental outcomes. 27 Notably, reductions in childhood blood lead levels were not associated with improvements in developmental outcomes, suggesting that the effects of early lead exposure are persistent. 27 The HOME cohort study by Vester et al 28 also found that the neurotoxicity of concurrent blood lead may largely reflect underlying cumulative exposure. A systematic review by Halabicky et al 29 further demonstrated that early-life lead exposure was significantly associated with higher cumulative physiological burden in adolescence, indicating that the effects of lead exposure can accumulate in the body over time. These findings suggested that the prominent lead burden in the 10-14-year age group may be related to the persistent effects of early cumulative exposure, highlighting the cumulative and delayed characteristics of lead poisoning and providing evidence for early intervention to prevent lead exposure.
Sex-stratified analyses revealed a significant decline in the IDII burden attributable to lead exposure from 1990 to 2021, with males experiencing a more pronounced decrease than females. The gender gap was consistent with findings from a related epidemiologic study in China. 17 A longitudinal study on Chinese children revealed that, at similar low levels of lead exposure, males exhibited more extensive neurobehavioral impairments at the age of 12 years across multiple domains, whereas females were affected only in the episodic memory domain. 30 Similarly, a Japanese birth cohort study demonstrated a significant negative correlation between blood lead concentrations and cognitive performance in 12-year-old boys, whereas no such correlation was evident in girls. 31 These findings suggested that males may be more susceptible than females to the neurotoxicity of lead exposure. Therefore, as environmental lead exposure levels have declined globally, males have experienced a greater decline in IDII burden because of their larger potential for health improvement. On the other hand, adolescent females are more likely to be iron-deficient due to menstrual blood loss and increased iron demands for growth and development. 32 Iron deficiency can enhance lead absorption through a shared intestinal transport mechanism, which partly explains the slower decline in lead-related burden among females. 33 Future public health strategies for lead exposure prevention and control need to incorporate interventions for gender-specific risks, including long-term monitoring of neurocognitive function and targeted iron deficiency intervention, to achieve precise and equitable population protection.
This study identified a significant negative correlation between SDI and ASDR associated with lead exposure in Asia, with lower SDI countries and territories disproportionately bearing a higher burden, particularly in South Asia. This finding aligns with the global GBD study on lead exposure–induced IDII in children and adolescents. 19 High-SDI countries may have benefited from more effective interventions, stronger public health awareness, and increased access to medical services and health care systems. 34 From 1990 to 2021, SDI-related health inequalities have gradually diminished, indicating that sustained and targeted efforts could further control disease burden. Frontier analysis indicated that 12 countries, including India, Afghanistan, Yemen, and Pakistan, have substantial improvement potential and may respond effectively to well-designed public health interventions. Therefore, the implementation of strengthened intervention strategies in these priority countries, such as establishing national systems for monitoring lead exposure, improving access to health services, and strengthening governmental regulations, can accelerate progress in reducing the disease burden attributable to lead exposure and advancing health equity.
This study also predicted the trends of IDII burden attributable to lead exposure in 4 high-burden countries with significant potential for improvement (India, Afghanistan, Pakistan, and Yemen) by 2035. The decline trend between 2022 and 2035 in India and Pakistan reflected measurable progress and effectiveness of ongoing public health interventions and policy measures aimed at reducing lead exposure in these countries. In contrast, the growth between 2022 and 2035 in Afghanistan and Yemen may be associated with population expansion based on results of the decomposition analysis. Controlling population growth and addressing lead pollution are key strategies to reduce the future disease burden in Afghanistan and Yemen.
This study has several limitations. First, variations in data reporting and recording practices across countries and territories may compromise the comparability and accuracy of the data. Second, this study primarily focused on intellectual disability attributable to lead exposure, with other contributing factors (eg, iodine deficiency) not being included in the analysis. 35 As a descriptive analysis, this study only outlined the distribution and trends of the disease burden and did not extend to an examination of specific intervention or treatment methods.
Conclusions
From 1990 to 2021, the burden of IDII caused by lead exposure among children and adolescents in Asia generally decreased. However, the burden remained heavy in low SDI regions, particularly in South Asia, with persistent health inequalities. Moreover, females and the 10-14-year age groups bore the most prominent burden. These findings provided robust evidence for targeted interventions in low-SDI countries and for specific gender and age groups to safeguard the intellectual development of children and adolescents.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738261456926 - Supplemental material for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021
Supplemental material, sj-docx-1-jcn-10.1177_08830738261456926 for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021 by Ru Fan, Taishun Li, Ruowen Qi, Bingwei Chen and Biyun Xu in Journal of Child Neurology
Supplemental Material
sj-docx-2-jcn-10.1177_08830738261456926 - Supplemental material for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021
Supplemental material, sj-docx-2-jcn-10.1177_08830738261456926 for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021 by Ru Fan, Taishun Li, Ruowen Qi, Bingwei Chen and Biyun Xu in Journal of Child Neurology
Supplemental Material
sj-docx-3-jcn-10.1177_08830738261456926 - Supplemental material for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021
Supplemental material, sj-docx-3-jcn-10.1177_08830738261456926 for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021 by Ru Fan, Taishun Li, Ruowen Qi, Bingwei Chen and Biyun Xu in Journal of Child Neurology
Supplemental Material
sj-docx-4-jcn-10.1177_08830738261456926 - Supplemental material for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021
Supplemental material, sj-docx-4-jcn-10.1177_08830738261456926 for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021 by Ru Fan, Taishun Li, Ruowen Qi, Bingwei Chen and Biyun Xu in Journal of Child Neurology
Supplemental Material
sj-pdf-5-jcn-10.1177_08830738261456926 - Supplemental material for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021
Supplemental material, sj-pdf-5-jcn-10.1177_08830738261456926 for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021 by Ru Fan, Taishun Li, Ruowen Qi, Bingwei Chen and Biyun Xu in Journal of Child Neurology
Supplemental Material
sj-pdf-6-jcn-10.1177_08830738261456926 - Supplemental material for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021
Supplemental material, sj-pdf-6-jcn-10.1177_08830738261456926 for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021 by Ru Fan, Taishun Li, Ruowen Qi, Bingwei Chen and Biyun Xu in Journal of Child Neurology
Supplemental Material
sj-pdf-7-jcn-10.1177_08830738261456926 - Supplemental material for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021
Supplemental material, sj-pdf-7-jcn-10.1177_08830738261456926 for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021 by Ru Fan, Taishun Li, Ruowen Qi, Bingwei Chen and Biyun Xu in Journal of Child Neurology
Supplemental Material
sj-pdf-8-jcn-10.1177_08830738261456926 - Supplemental material for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021
Supplemental material, sj-pdf-8-jcn-10.1177_08830738261456926 for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021 by Ru Fan, Taishun Li, Ruowen Qi, Bingwei Chen and Biyun Xu in Journal of Child Neurology
Supplemental Material
sj-pdf-9-jcn-10.1177_08830738261456926 - Supplemental material for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021
Supplemental material, sj-pdf-9-jcn-10.1177_08830738261456926 for The Burden of Idiopathic Developmental Intellectual Disability Attributed to Lead Exposure in Asian Children and Adolescents, 1990-2021: Trends, Inequalities, and Future Projections for the Global Burden of Disease Study 2021 by Ru Fan, Taishun Li, Ruowen Qi, Bingwei Chen and Biyun Xu in Journal of Child Neurology
Footnotes
Acknowledgments
The authors sincerely thank all the researchers involved in the Global Burden of Disease Study 2021 for their outstanding work.
Ethics Approval
This study used anonymous and publicly data from the Global Burden of Disease Study 2021 (GBD 2021). The original GBD 2021 study adhered to the Declaration of Helsinki and received approval from the Institutional Review Board of the University of Washington. Consequently, additional ethical approval and informed consent were not required for this secondary analysis.
Author Contributions
Concept and design of the study: F.R., X.B.Y., and C.B.W.; Data collection and analysis: F.R., L.T.S., and Q.R.W.; Drafting of the manuscript: F.R.; Critical revision for important intellectual content: X.B.Y. and C.B.W. All authors had full access to the data, contributed to the study, and approved the final version for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.