
Abstract
Rationale
A recent scoping review of disparities in pediatric epilepsy revealed that mortality-related outcomes, including sudden unexpected death in epilepsy (SUDEP) and suicide, are rarely studied. We addressed this gap by systematically analyzing literature on social determinants of health (SDOH) and epilepsy-related mortality/SUDEP and suicide.
Methods
The Pediatric Epilepsy Research Consortium Health Equity Special Interest Group updated a recent scoping review, incorporating peer-reviewed studies that assessed SUDEP, suicide, or mortality in populations affected by SDOH. Data were categorized by SDOH factors and corresponding disparities to identify patterns across studies.
Results
Eighteen studies were reviewed: mortality without referencing SUDEP (n = 8), SUDEP (n = 7), and suicide (n = 3). Gender was the most common SDOH; others included socioeconomic status, geography, race/ethnicity, and education.
Conclusion
Literature addressing disparities in pediatric epilepsy-related mortality is limited. Standardized SDOH data collection may improve comparability and inform equity-focused interventions.
Keywords
Introduction
Premature death, sudden unexpected death in epilepsy (SUDEP), and elevated suicide risk are the leading disease-related causes of mortality in epilepsy. These outcomes are often preventable through improved access to epilepsy care and management of neuropsychological comorbidities.1–5 Social determinants of health (SDOH) such as gender, race, ethnicity, socioeconomic status (SES), geographic location, caregiver education, and insurance status, as outlined by the National Institute of Minorities Health and Health Disparities Research Framework are integral in shaping disease and mortality outcomes by influencing access to antiseizure medications and other treatments. 6
A 2024 scoping review on healthcare disparities in pediatric epilepsy highlighted the impact of SDOH on access to care and outcomes. 7 Of the 10 000 abstracts screened, 307 studies (containing pediatric-only or mixed-age/pediatric and adult data) were reviewed, identifying 769 unique findings related to disparities or equities. Most of these publications addressed access to epilepsy surgery or neuropsychological outcomes in relation to SDOH. However, a crucial outcome in pediatric epilepsy- SUDEP and/or mortality, was rarely studied. Recognizing this gap, especially with pediatric-only studies, we elected to focus on mortality-related outcomes in pediatric epilepsy in relationship to SDOH. We thus included pediatric and mixed-age studies in this scoping review aligning with the methodology of the original scoping review. Of the 307 papers published between 1977 and 2025, only 18 addressed mortality/SUDEP in epilepsy. Building on the 2024 scoping review and including studies that contained pediatric or mixed-age data, we examined specific SDOH variables in the context of mortality in pediatric epilepsy, emphasizing the limited literature on this topic and the need for further research.
Materials and Methods
The Pediatric Epilepsy Research Consortium (PERC) is a non-profit organization dedicated to advancing research in pediatric epilepsy across the United States. Currently, PERC includes more than 90 pediatric epilepsy centers and more than 400 members, including pediatric epileptologists, neuropsychologists, and clinician researchers, and is organized into 17 Special Interest Groups (SIGs).
The PERC Health Equity SIG conducted a scoping review to identify the existing literature highlighting disparities in the field of pediatric epilepsy. Details on the methodology are available in the article Health Disparities in Pediatric Epilepsy: Methods and Lessons Learned as well as the initial scoping review titled Health and Healthcare Disparities in Pediatric Epilepsy in the United States: A Scoping Review7,8 (see Supplementary Appendix). Details on the inclusion and exclusion criteria are provided in the Supplementary Appendix. In summary, studies in English containing original, US-based pediatric-only (exclusively less than or equal to 21 years) or mixed-age (pediatric and adult) epilepsy disparity and equity data that was statistically analyzed by one or more disparity populations were included. The objective of the scoping review was to synthesize existing literature on disparities among diverse populations expanding on the National Institutes of Health (NIH)-designated “health disparity populations” (eg, race/ethnicity, gender/sexual orientation/gender identity, SES, health insurance status/type, regional/geographic residence, patient and/or caregiver education, English proficiency, and nativity/citizenship) and a range of outcomes (prevalence/incidence, healthcare access and utilization, adherence, epilepsy evaluation and diagnosis, epilepsy treatment and management, adverse events/complications, economic factors, quality of life/neuropsychological outcomes, epilepsy outcomes/severity, and mortality/SUDEP).6,8 An important goal of this scoping review was to compile the span of pediatric epilepsy disparity and equity data from a broad range of peer-reviewed articles and gray literature with a variety of study designs. Thus, the members of the PERC Health Equity SIG chose the approach of a scoping review over a systematic review, which seeks to evaluate the best empirical evidence from a relatively narrow range of quality-assessed studies to answer a focused research question. 9 A finding was defined and counted as a single result from a discrete statistical analysis of a specific clinical outcome (in this case, SUDEP, mortality, or suicide) within a disparity population. A statistically significant finding was reported as disparity, whereas a nonsignificant finding was reported as equity. These definitions of “disparity” and “equity” were agreed upon by the authors of the initial scoping review during the study design. Because of this vast undertaking, the original publication was unable to provide a granular analysis of the causal relationships between specific SDOH and individual outcomes.
Given the importance of SUDEP/mortality for children with epilepsy and their families, the PERC Health Equity SIG chose to highlight in detail the current literature examining its relationship to SDOH. For the current scoping review, data were selected from the list of papers identified in the original scoping review—containing pediatric or mixed-age data—where “SUDEP” or “mortality” was assigned as a study outcome for all disparity populations. From the previously published scoping review, the authors (S.B., S.P., S.H.) identified a total of 18 publications from peer-reviewed journals and extracted data from 15 of these papers; 2 were excluded because the full text could not be retrieved, and 1 was an abstract. We categorized these papers reporting death associated with epilepsy as mortality (from causes other than SUDEP or suicide), SUDEP, and suicide.
The search used in the original scoping review was updated in May 2024, as described by Skjei et al, 7 and again in July 2025. Because of the large number of results, the original search was modified to include the following terms in PubMed: (“Health Status Disparities” [MeSH Terms] OR “Healthcare Disparities” [MeSH Terms] OR disparit*[tiab] OR inequalit*[Title/Abstract] OR inequit* [Title/Abstract] OR equity [tiab] OR equities [tiab]). The [tiab] field tag limited results to terms appearing in the title or abstract. These same terms were modified for and added to the searches in the following databases: APA PsycINFO (EBSCOhost), CINAHL Plus with Full Text (EBSCOhost), Cochrane Library (Wiley), Dissertations & Theses Global (ProQuest), Embase (Elsevier), and Web of Science (not included in the July search). A health sciences librarian collaborated on the search strategy and conducted the search. The full search strings, including search dates and filters for each database, are included in the Supplementary Appendix.
The literature screening process was conducted using Covidence (Figure 1). Abstracts and full publications were reviewed independently by at least 2 reviewers to determine if they met the previously established inclusion criteria. 10 The modified and updated search in May 2024 returned 186 results across all databases (Figure 1). Of these, 46 duplicates were removed, and then 140 were screened for eligibility, resulting in a full review of 6 papers. The 6 papers were subsequently excluded because the outcomes did not include SUDEP or mortality (n = 3), data elements did not include SDOH (n = 1), or the study cohort did not involve epilepsy (n = 1) or pediatric patients (n = 1). The search in July 2025 returned 110 results across all databases, which were screened for eligibility, resulting in a full review of 17 papers (Figure 1). Fourteen papers were subsequently excluded because they were review articles (n = 4), did not include SUDEP or mortality outcomes (n = 6), or had no pediatric subjects (n = 4). Three studies from the updated search met the inclusion criteria.
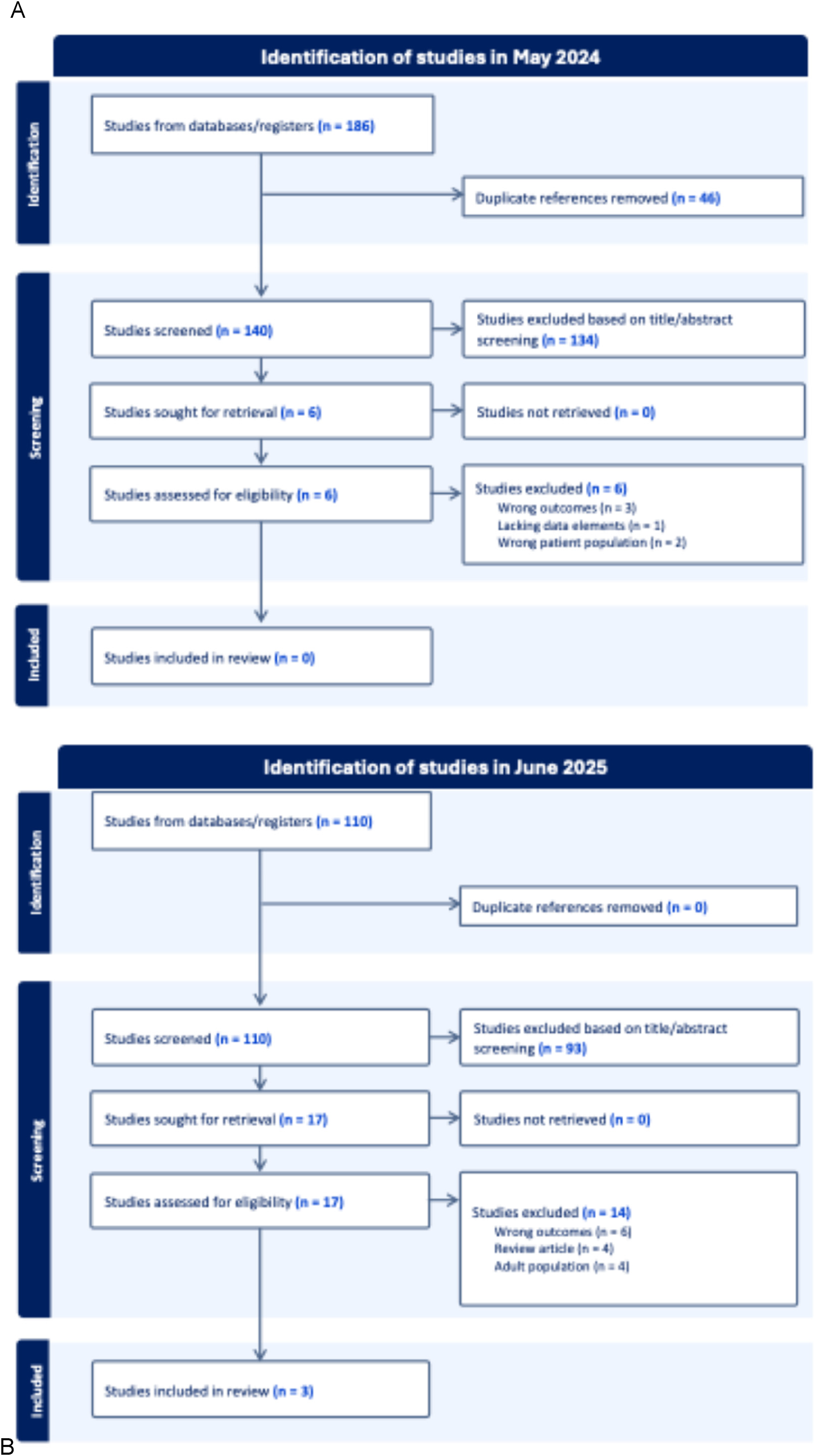
PRISMA flow diagram of the updated literature reviews. Searches were conducted using a consistent strategy, building on prior scoping review. The original scoping review (data extracted through November 2022) included 307 studies, of which 15 included SUDEP, suicide, or mortality outcomes (not shown). (A) An updated search in May 2024 identified 186 articles; 46 duplicates were removed, and 140 studies were screened. Six full-text articles were reviewed and were excluded for the following reasons: did not include SUDEP, suicide, or mortality outcomes (n = 3); lacked SDOH data elements (n = 1); or did not involve pediatric patients (n = 1) or patients with epilepsy (n = 1). No studies from the May 2024 search met inclusion criteria. (B) A subsequent updated search in July 2025 identified 110 articles; 17 underwent full-text review. Fourteen articles were excluded for the following reasons: review articles (n = 4), did not include SUDEP, suicide, or mortality outcomes (n = 6), or did not include pediatric populations (n = 4). Three studies from the July 2025 search met inclusion criteria, yielding 18 total studies across the original (n = 15) and updated (n = 3) reviews.
Results
Eighteen peer-reviewed publications were identified across the original (n = 15) and updated (n = 3) reviews that assessed “mortality” or “SUDEP” outcomes in disparity populations. Eight papers documented general mortality in epilepsy without specifically mentioning SUDEP. Seven studies reported on SUDEP; of those, 2 assessed cardiac arrhythmias as an indirect marker for SUDEP, and 3 evaluated suicide in epilepsy. Thirteen studies analyzed mixed adult and pediatric populations, whereas the remaining 5 focused exclusively on pediatric patients. Among the pediatric-specific papers, 3 addressed mortality, 1 assessed SUDEP, and 1 examined suicide. There were a total of 40 unique findings, 31 disparity and 9 equity findings. The most frequently reported SDOH finding was gender (n = 21), whereas other factors such as race/ethnicity (n = 11), SES (n = 3), geography (n = 3), and education (n = 2) were also noted. Table 1 summarizes the disparity and equity findings related to mortality, SUDEP, and suicide.
Disparity and Equity Findings Related to Mortality, SUDEP, and Suicide in Persons with Epilepsy.a
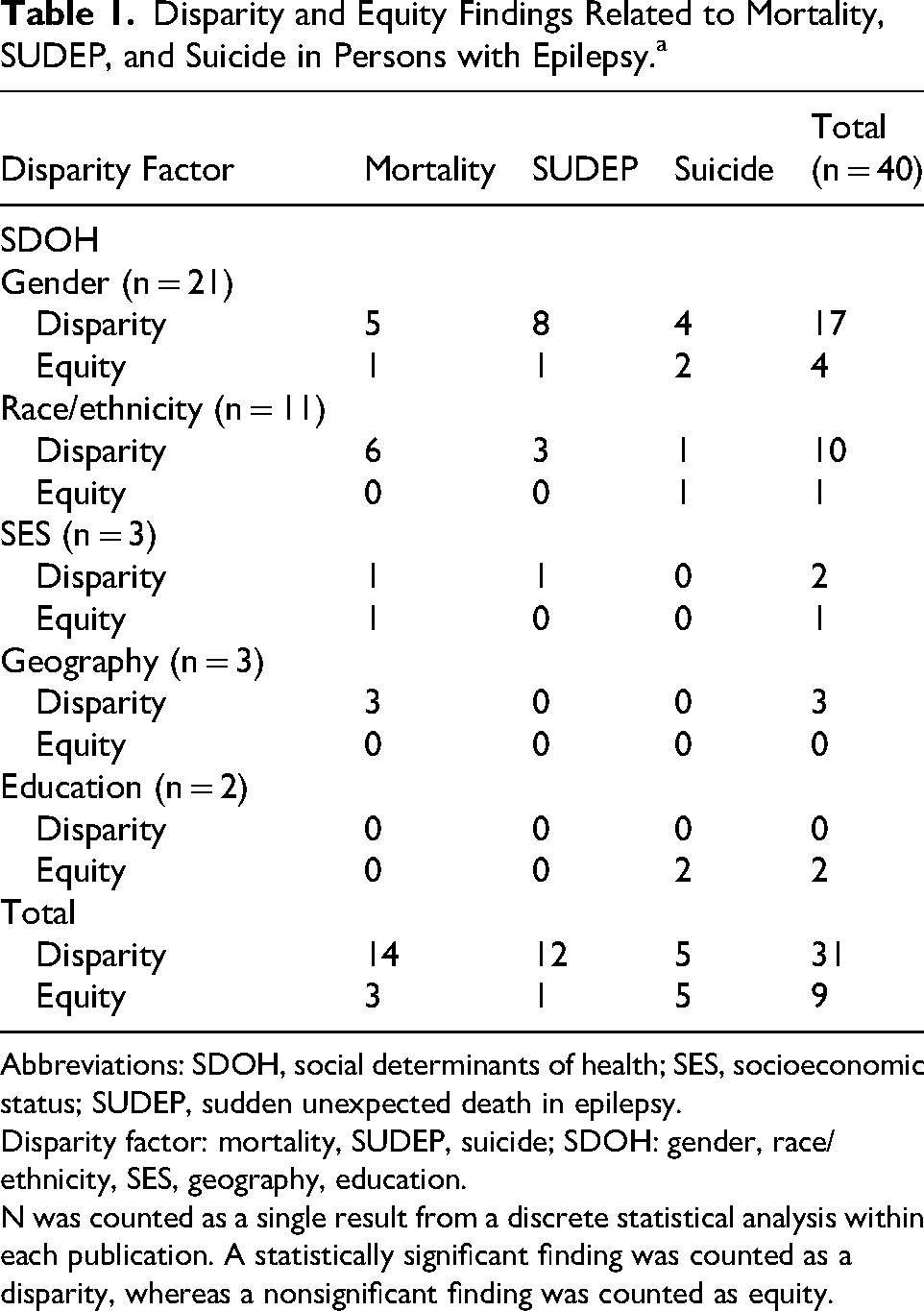
Abbreviations: SDOH, social determinants of health; SES, socioeconomic status; SUDEP, sudden unexpected death in epilepsy.
Disparity factor: mortality, SUDEP, suicide; SDOH: gender, race/ethnicity, SES, geography, education.
N was counted as a single result from a discrete statistical analysis within each publication. A statistically significant finding was counted as a disparity, whereas a nonsignificant finding was counted as equity.
Mortality
Mortality refers to the incidence of death within a specified population, context, or time frame. Applying the definition to this review, mortality refers to deaths in epilepsy excluding SUDEP and suicide, as reported in peer-reviewed publications. Eight papers assessed mortality, reporting a total of 14 disparity findings and 3 equity findings.
A pediatric study of risk factors associated with mortality in convulsive status epilepticus (SE) retrospectively reviewed the Kids’ Inpatient Database and identified 12 365 children (ages 0-20 years), of which only 345 had epilepsy and 117 died during their hospitalization. Race and SES (based on average household income determined by zip code) were the reported SDOH variables. According to this study, Black/African American children had lower mortality following a convulsive SE episode (P = .009) and decreased risk of death in SE (odds ratio [OR] 0.4, 95% CI 0.2-0.8). No differences were seen in other racial groups, and SES was not a significant risk factor for mortality. 11
Similarly, Logroscino et al12,13 evaluated short- and long-term mortality determinants among patients with SE (including symptomatic causes of seizures, those with a single unprovoked seizure, and with a diagnosis of epilepsy). Although in the short term (<30-day mortality), the risk of death for males was twice that for females, in the long term (30-day to 10-year), there were no gender-related differences.
Vickrey et al 14 assessed a cohort of adolescents and adults undergoing diagnostic evaluation for epilepsy surgery and compared mortality in surgery (performed on a localized region) and non-surgery groups. Death in the non-surgery group was higher than in the surgery group (20% vs 7%; P < .01). In multivariate analysis, gender was the only SDOH variable associated with mortality, with female gender associated with a lower mortality (P < .03). No other SDOH variables were analyzed.
Greenlund et al 15 examined epilepsy-related deaths from 2005 to 2014 by age groups, gender, and race/ethnicity. Mortality was highest among the non-Hispanic Black/African American population (1.42 deaths per 100 000) compared with non-Hispanic White (0.86 deaths per 100 000) and Hispanic populations (0.70 deaths per 100 000). Males had higher mortality rates than females (1.01 vs 0.64 per 100 000).
Tian et al 16 examined US death certificate data from 2011 to 2021 in a national study of epilepsy-related mortality, including all ages but highlighting subgroups <24 years and >65 years. Gender, race, ethnicity, geographic region, and urban-rural location were the reported SDOH variables. Males had higher age-standardized mortality rates than females. Non-Hispanic Black/African American and American Indian/Alaska Native individuals experienced higher mortality, and non-Hispanic Asian/Pacific Islander individuals experienced lower mortality compared with non-Hispanic White individuals. Geographic and urban-rural differences were also noted. Mortality rates were lowest in the Northeast and highest in the West and Midwest. Mortality was higher in nonmetropolitan counties (except during 2011-2015) and lowest in large fringe metropolitan areas.
A 2024 study by Garrett et al 17 examined neighborhood resources and outcomes in children admitted to intensive care units with SE, evaluating SES using the Child Opportunity Index (COI). Compared with children from very high opportunity neighborhoods, those from very low, low, and moderate levels were more likely to require invasive mechanical ventilation (very low: adjusted odds ratio [aOR] 1.20, 95% CI 1.07-1.35, P = .002; low: aOR 1.18, 95% CI 1.06-1.33, P = .004; moderate: aOR 1.20, 95% CI 1.07-1.34, P = .002). Despite this increased risk of ventilation, in-hospital mortality did not differ across COI levels.
A national study of epilepsy-related mortality trends in the United States from 1999 to 2020 examined disparities by gender, race, ethnicity, and geography. Mortality was consistently higher in males than females, with the gap widening over time: in 1999, the age-adjusted mortality rate (AAMR) was 0.70 (95% CI, 0.66-0.75) for males vs 0.47 (95% CI, 0.43-0.50) for females, increasing to 1.84 (95% CI, 1.78-1.91) and 1.46 (95% CI, 1.41-1.52), respectively, by 2020. The highest mortality was among non-Hispanic Black/African American (AAMR 1.38, 95% CI, 1.35-1.41) and non-Hispanic American Indian/Alaska Native individuals (AAMR 1.07, 95% CI, 0.98-1.17), and lower in non-Hispanic White (AAMR 0.76, 95% CI, 0.75-0.77), Hispanic/Latino (AAMR 0.76, 95% CI, 0.74-0.78), and non-Hispanic Asian/Pacific Islander individuals (AAMR 0.32, 95% CI, 0.30-0.34). Higher mortality was seen in nonmetropolitan areas (AAMR 0.92, 95% CI, 0.90-0.94) compared with metropolitan areas (AAMR 0.76, 95% CI, 0.75-0.77). Overall, epilepsy-related mortality increased over time, with widening disparities across gender, race, and geography. 18
In summary, the most frequent SDOH factors associated with mortality outcomes were gender (n = 6) and race/ethnicity (n = 6), followed by geography (n = 3) and SES (n = 2), highlighting differences within these disparity populations.
SUDEP
The International League Against Epilepsy (ILAE) defines SUDEP as a sudden, unexpected, witnessed or unwitnessed, nontraumatic, and nondrowning death in PWE, with or without evidence for a seizure, and excluding documented SE, in which postmortem examination does not reveal a structural or toxicologic cause of death. 19 Seven studies addressed SUDEP, yielding 12 disparity findings and 1 equity finding.
A pooled analysis by the ILAE Commission on Epidemiology, Subcommission on Mortality, combined data from 4 case-control studies conducted in the United States, Sweden, Scotland, and England. The analysis included 289 SUDEP cases and 958 controls and identified several statistically significant predictors of SUDEP, including an increased frequency of generalized tonic-clonic seizures, polytherapy, longer epilepsy duration, and onset before age 16 years. Male gender was the only SDOH variable significantly associated with SUDEP, with males having a 1.4-fold higher risk than females. A further stratified analysis revealed that females with idiopathic generalized epilepsy were at significantly lower risk for SUDEP (OR 0.39) compared with females without idiopathic generalized epilepsy, a protective effect not observed in males. Additionally, male patients with later epilepsy onset (after age 16 years) showed a trend toward increased SUDEP risk, although this was not statistically significant. 20 Similarly, a retrospective autopsy-based study by Lear-Kaul et al 21 reviewed 67 cases of epilepsy-related sudden death and found that 72% (n = 48) of the decedents were male.
Race, along with gender, and their associations with SUDEP were evaluated in a retrospective study by Zhou et al, 22 analyzing forensic autopsy cases from Maryland between 2007 and 2009. The study reviewed 104 sudden unexpected deaths directly or indirectly related to epilepsy; 74 met the accepted criteria for SUDEP. Consistent with prior findings, males were more likely to experience SUDEP (male-to-female ratio 1.5:1). Notably, SUDEP incidence among Black/African American individuals was disproportionately higher than among White individuals (ratio 2.3:1). Postmortem blood analyses revealed subtherapeutic or undetectable antiseizure medication levels in 73% of cases, suggesting that treatment nonadherence may be a significant modifiable SUDEP risk factor.
A retrospective study of sudden and unexpected natural deaths in 207 individuals aged 1-22 years identified 32 patients with a documented seizure disorder. Among these, 23 deaths (75%) were unwitnessed, 16 (59%) occurred during sleep, and 6 (19%) followed witnessed SE. The incidence of death was significantly higher among non-White individuals compared with White individuals (P < .01). Within the subgroup of White individuals, males had a significantly higher death rate (P < .01). 23
Cihan et al 24 investigated the association between SES and SUDEP incidence using median income by zip code as a proxy. SUDEP cases from 2009-2010 and 2014-2015 were analyzed across 3 geographically diverse medical examiner offices. Decedents were grouped into low and high SES quartiles. The study identified 159 SUDEP cases in the lowest SES quartile and 43 in the highest. SUDEP rates were significantly higher in the lowest SES group, with a rate ratio of 2.6 (95% CI: 1.7-4.1, P < .0001) in 2009-2010 and 3.3 (95% CI: 1.9-6.0, P < .0001) in 2014-2015. Although overall SUDEP incidence declined over time, the gap between socioeconomic groups remained pronounced, highlighting a persistent disparity in epilepsy-related mortality.
Although not directly investigating SUDEP, 2 studies evaluated cardiac arrhythmias in epilepsy patients as indirect markers for SUDEP. Desai et al 25 examined gender-based differences in cardiac arrhythmia subtypes among epilepsy patients and found that males were more predisposed to cardiac arrhythmias compared with females (OR: 1.1, P < .001). The prevalence of most arrhythmia subtypes was higher in male patients, and life-threatening arrhythmias were more common. No other SDOH variables were assessed in this study. Standridge et al 26 examined ictal cardiac arrhythmias in the Epilepsy Monitoring Unit. Among 2066 electrographically confirmed ictal events from 139 children, seizures associated with potentially serious arrhythmias (eg, abnormal QRS complex or irregular variable rhythms) occurred more often in males (64%, P = .016) and White children (78%, P = .013). However, peri-ictal and postictal rate changes (sinus bradycardia and tachycardia) were more common in females (P = .003 and <.0003, respectively).
Overall, in the aforementioned papers, the most frequently examined SDOH factor associated with SUDEP outcomes was gender (n = 9), with males being more affected, followed by race/ethnicity (n = 3) and SES (n = 1).
Suicide
Three studies analyzed suicide patterns among epilepsy patients and compared them to those without epilepsy.27–29 Five disparity findings and 5 equity findings were reported across these studies.
In 2016, Tian et al 27 conducted a study in epileptics aged 10 to >70 years and found that males with epilepsy between the ages of 50 and 59 years were more likely to commit suicide compared with those without epilepsy. Suicide rates compared with people without epilepsy did not differ by race/ethnicity or educational level. Approximately one-third of suicides in those with and without epilepsy occurred among individuals with the lowest education level. Among these patients, females were more likely than males to commit suicide if they had been separated, divorced, or widowed (P < .01). Males with epilepsy were more likely to commit suicide if they had never been married (P < .01). In 2019, Tian et al 28 found that suicide decedents with epilepsy were more often female or non-Hispanic Black individuals compared to those without epilepsy (P < .05).
A population-based pediatric study compared self-injurious behavior and suicidal ideation in children with epilepsy and controls. Among epilepsy patients, females had a 1.8-fold higher risk of exhibiting any form of suicidal ideation or self-injurious behavior compared to males (hazard ratio = 1.81, 95% CI: 0.97-3.35, P = .06). Females had a 1.6-fold higher risk specifically for suicidal ideation or suicide attempt (hazard ratio = 1.65, 95% CI: 0.81-3.37, P = .17). However, neither finding reached statistical significance. Additionally, no significant differences were observed between epilepsy and control groups in terms of family structure, school placement prior to the first suicidal event, or parental education level. 29
To summarize, in the articles assessing suicide in epilepsy, gender (n = 6) was the most frequently reported SDOH followed by race/ethnicity (n = 2) and education (n = 2).
Discussion
This scoping review underscores the emerging yet still limited research on SDOH in relation to SUDEP, mortality, and suicide among epilepsy patients. Despite the critical significance of these outcomes, only a handful of studies have specifically examined the role of SDOH, mostly gender. Even fewer address the impact of SDOH in children (only 5 studies address mortality outcomes in the pediatric age group) highlighting the lack of standardized SDOH captured in pediatric epilepsy-related mortality outcomes. Thus, in accordance with the methodology of the original scoping review, we analyzed studies with pediatric-only and mixed-age (both pediatric and adult) data, as our focus was primarily on looking at mortality-related outcomes in pediatric epilepsy. Standardized SDOH for pediatric-specific epilepsy research is an urgent need.
Mortality: Studies assessing mortality in epilepsy reveal mixed and context-dependent patterns. In pediatric SE, SES showed no impact on mortality, although children from lower-opportunity neighborhoods required more intensive interventions.11,17 In contrast, national studies consistently highlight enduring disparities by gender, race, and geography. Males, individuals from racial minority groups (eg, non-Hispanic Black/African American and American Indian/Alaska Native populations), and those living in nonmetropolitan areas face higher mortality, with evidence that these gaps have widened over the past 2 decades.16,18 These findings suggest that although short-term outcomes such as in-hospital survival may appear equitable, broader population-level data underscore persistent inequities shaped by both biological vulnerability and SDOH. SDOH variables may lead to socioeconomic barriers adversely impacting timeliness of diagnosis, therapeutic interventions, and treatment adherence, thus indirectly influencing seizure control and subsequently mortality-related outcomes. The variability in findings may, in part, stem from insufficient publications on this topic, which may limit the ability to establish consistent patterns and contribute to the mixed results observed.
SUDEP: SUDEP remains the leading cause of premature epilepsy-related mortality, and emerging evidence highlights the influence of SDOH on its risk. The most consistent finding across the literature is the excess risk in males, confirmed in pooled analyses showing a ∼1.4-fold increased risk 20 and echoed in autopsy series where up to 70% of SUDEP decedents were men.20,21 Although gender-related biological factors, such as arrhythmia susceptibility, may partly explain this disparity, gender-related differences in treatment adherence or care access may also contribute. Racial disparities are also evident, with Black/African American and other non-White individuals experiencing disproportionately higher SUDEP incidence, in some reports more than twice that of White individuals.23,30 Importantly, SES has been linked to marked differences, with SUDEP rates more than 2 to 3 times higher in the lowest SES quartiles compared with the highest, 23 suggesting that structural inequities and barriers to consistent, high-quality epilepsy care remain major contributors. Despite the heterogeneity in how SUDEP was identified across these studies, the findings underscore the need to view SUDEP not only through a clinical and biological lens but also as a public health equity issue. Addressing modifiable SDOH factors, such as access to affordable medications, continuity of specialized care, and culturally responsive education, will be critical for reducing preventable epilepsy deaths and narrowing persistent disparities.
Suicide: Suicide risk, a major contributor to epilepsy-related mortality, was assessed in both adults and children. Pediatric studies examining suicide risk and self-injurious behavior were scarce and showed trends toward higher suicidal ideation in females with epilepsy, but differences were not statistically significant, likely because of limited power to detect significance in this outcome. 29 In adults, suicide risks were associated with factors including social isolation and relationship status.27,28 Studies are warranted to assess these risks in children with epilepsy, especially given that in the general population, suicide attempts are more common in females, whereas completed suicides are more common in males. 30
Overall, this updated and detailed review aligns with findings from the original scoping review by Skjei et al, 7 which identified substantial gaps in the pediatric epilepsy disparities literature, particularly related to mortality and SUDEP. Standard inclusion of SDOH data elements in population-based registries and linkage of routinely collected health care data to mortality endpoints could help clarify complex SDOH relationships and inform prevention strategies. 30 Currently, SDOH data elements are rarely adequately captured in pediatric epilepsy research. 7 The lack of SDOH inclusion restricts comprehensive assessment and limits the ability to perform multivariate analyses of covariates (such as SES, race, or insurance status) that may influence epilepsy outcomes. The use of a set of common data elements for SDOH in pediatric epilepsy could facilitate structured and consistent data collection, enable comparisons across studies, promote equity-focused research, and improve outcomes. 31
This review has several limitations. As a scoping review, it was designed to capture the breadth of existing literature. Thus, quantitative meta-analyses, formal assessment of methodologic and/or study quality, or risk bias of included studies were not conducted. Variability in study designs, populations, and outcome measures limited direct comparison across studies. In accordance with the original scoping review, we defined terms such as disparities and equities to understand the findings of these studies; this categorization may have oversimplified more complex relationships with SDOH. Although statistically nonsignificant findings were reported as “equity” for this scoping review, we caution about interpreting these findings as not being indicative of “true” disparities. Few studies included pediatric subjects, and most did not systematically collect or report SDOH variables, restricting interpretation, intersectional analyses, and the ability to identify in-depth mechanisms by which SDOH variables may influence epilepsy-related mortality. In accordance with the NIH framework, we used the term “gender” in this review, and although gender was the most commonly reported variable, studies did not differentiate between “sex,” “gender,” and other terms that capture sexual identity.6,8 We also recognize that gender disparities may be somewhat ambiguous as a gender difference may be inherent to a certain epilepsy syndrome (eg, epilepsy with eyelid myoclonia is more common in girls). 32 Additionally, differences in how mortality and SUDEP were defined and ascertained across studies may have introduced bias. Finally, the literature in this review showcased studies only from within the United States and therefore its findings cannot be generalized to other health care systems abroad. However, this scoping review provides a comprehensive synthesis of current evidence and identifies critical gaps in the literature. Future research should prioritize the integration of common data elements that capture detailed SDOH, such as in standardized registries and in prospective cohort studies, the inclusion of pediatric populations and the intentional enrollment of diverse cohorts even across the globe to ensure that epilepsy research reflects the full spectrum of affected individuals, not only in high-income but also in low- and middle-income countries. Such approaches are critical to advancing a more comprehensive and equitable understanding of epilepsy-related mortality, including SUDEP, and to informing interventions that meaningfully address health disparities.
Conclusion
Collectively, the current literature reveals meaningful patterns in epilepsy-related mortality across SDOH categories. Pediatric-specific data remain especially limited, despite known disparities in diagnostic and therapeutic pathways, underscoring the need for more robust, intersectional, and systematic research in this age group. Most studies have disproportionately emphasized individual demographic variables, most notably, gender, while overlooking other nuanced and intersecting roles including race, ethnicity, SES, education, and geographic location. Thus, improvement in SDOH data collection, such as incorporating common data elements in research, will aid in understanding the breadth and depth of SDOH variables contributing to epilepsy-related mortality. Future research linking SDOH variables to longitudinal clinical studies may be essential in identifying modifiable risk factors for mortality in pediatric epilepsy.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738261462227 - Supplemental material for Assessing Sudden Unexpected Death in Epilepsy (SUDEP), Mortality, and Suicide in Pediatric Epilepsy from the lens of Healthcare Disparities: Data From a Scoping Review
Supplemental material, sj-docx-1-jcn-10.1177_08830738261462227 for Assessing Sudden Unexpected Death in Epilepsy (SUDEP), Mortality, and Suicide in Pediatric Epilepsy from the lens of Healthcare Disparities: Data From a Scoping Review by Senyene E. Hunter, Shital Patel and Sonal Bhatia in Journal of Child Neurology
Footnotes
Acknowledgements
The authors would like to acknowledge the following individuals for their contributions during the initial and updated scoping review: Christina Briscoe Abath, Christopher W. Beatty, Jamie Conklin, Grace Gaston, Rebecca Garcia, Rebecca Garcia-Sosa, Charuta Joshi, Gogi Kumar, B. Oyinkan Marquis, Alexandria Melendez-Zaidi, Elizabeth Ng, Rachit Patel, Chethan Rao, Kavya Rao, Nilika Singhal, Karen Skjei, Connie Taylor, Imelda Vetter, Cortney Wolfe-Christensen, Janelle Wagner, and JoJo Yang.
Ethical Considerations
This article does not contain any studies with human or animal participants.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
SB: Writing – original draft, review & editing, Methodology, Investigation, Validation, Formal analysis, Data curation. SP: Writing – original draft, review & editing, Methodology, Investigation, Validation, Formal analysis, Data curation. SEH: Writing – original draft, review & editing, Methodology, Investigation, Validation, Formal analysis, Data curation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data generated or analyzed during this study are included in this published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.