
Abstract
The ability of bone defects to heal spontaneously is inversely related to the size of the defect, such that defects larger than a critical size will not heal without additional therapeutic intervention. Typically, large bone defects are filled with autologous bone harvested from another skeletal site, an osteoconductive bone graft material, treated with an osteoinductive factor such as bone morphogenetic protein-2, or by a combination of these approaches. Despite these interventions, unsatisfactory success and complication rates show that alternative treatment methods are needed. Here, we test whether salicylic acid polymers can be used as guided bone regeneration barriers in conjunction with bone morphogenetic protein-2 to treat 1-cm-diameter defects in rabbit parietal bones. Porous, 1-cm round polycaprolactone scaffolds were infused with calcium sulfate–containing bone morphogenetic protein-2 and then capped on one side with salicylic acid polymers. The polymers slowed resorption of calcium sulfate that was used as a carrier for bone morphogenetic protein-2, indicating that bone morphogenetic protein-2 release into the parietal bone defect was extended by the use of the salicylic acid polymer. Microcomputerized tomography and histomorphometric analysis of the parietal bones 8 weeks after implantation showed that the salicylic acid polymer did not impair bone formation in the defect. These observations indicate that salicylic polymers paired with bone morphogenetic protein-2 can be optimized for use in guided bone regeneration to help repair large bone defects.
Keywords
Introduction
Treating large bone defects caused by traumatic injury or pathological bone destruction is clinically challenging. Bone can regenerate to heal small defects. Typically, the trauma that causes the bone defect induces a regenerative response, and new bone will form appositionally to fill the defect volume. However, in large bone defects, the center of the defect volume fills with soft tissue, and new bone formation stops prior to healing of the defect. 1 Whether the soft tissue prevents continued bone formation or whether the soft tissue invasion of the defect space represents the limits of the bone regeneration response is not known. Clinically, these so-called critical size defects are treated by filling the defect volume with bone harvested from the patient (autograft), allogeneic or xenogeneic bone tissue, or synthetic materials in order to increase the amount of bone formed. 2 The utility of autograft is limited by the amount of bone that can be harvested from a patient. Allogeneic, xenogeneic, and synthetic bone materials are readily available but are not as effective as autograft. Thus, there remains a significant clinical need for materials and methods to treat large bone defects.
One strategy to treat large bone defects would be to augment the bone regeneration response with an osteoinductive factor, such as bone morphogenetic protein-2 (BMP-2). The osteoinductive properties of BMP-2 are well established.3,4 Clinically, BMP-2 is used to promote healing of open tibia fractures and for fusion of lower spinal vertebrae.5,6 However, clinical use of BMP-2 requires the use of supraphysiological doses which can produce significant side effects including excessive tissue swelling and increased risk for cancer.7 –12 Methods that can control BMP-2 activity could alleviate these side effects.
Another strategy to treat large bone defects would be to use guided bone regeneration methods to protect the target volume from soft tissue ingrowth, while new bone formation fills the defect.13,14 This approach is used for mandible and maxilla bone augmentation prior to application of dental devices. 15 Recently, we tested the use of salicylic acid polymers as biodegradable barriers for guided bone regeneration in rabbit parietal bone defects. 16 As salicylic acid is a nonsteroidal anti-inflammatory drug (NSAID), there is concern that salicylic acid released from the degrading polymer can inhibit bone formation. 17 However, the tested salicylic acid polymers reduced localized inflammation without inhibiting overall bone formation into an osteoconductive scaffold, suggesting that salicylic acid polymers can be used as guided bone regeneration barriers.
Here, we extended testing of the salicylic acid polymers for use in bone regeneration. A device that combines the use of BMP-2 with a bone regeneration barrier made from the salicylic acid polymers was tested in a rabbit parietal bone defect model. We found that the salicylic acid polymers prolonged delivery of the BMP-2 without reducing bone formation within the defect.
Materials and methods
Scaffold fabrication
Scaffolds were cut from a 2.0-mm-thick, porous polycaprolactone (PCL) sheet (3D Biotek, Hillsborough, NJ) using a 3/8-in-diameter punch. The PCL sheet was fabricated using 300-µm-thick fibers with 300-µm spacing in seven perpendicular layers. Some scaffolds were infused with calcium sulfate or calcium sulfate–containing BMP-2. Calcium sulfate was mixed with sterile water or BMP-2 (1 mg/mL; Medtronic, Minneapolis, MN) using a 3:1 (w/v) ratio. PCL scaffolds were submerged in the calcium sulfate or calcium sulfate–BMP-2 slurry, sonicated to eliminate air pockets within the matrix and then allowed to dry. Once solidified, scaffolds were placed in a vacuum desiccator overnight to remove moisture from the solidified matrix. Scaffolds were weighed before calcium sulfate infusion and again after desiccation to determine the amount of calcium sulfate and BMP-2 in each scaffold, which was approximately 206 mg (205.5 ± 28.1 mg) and 68 µg (68.5 ± 9.4 µg), respectively. The six different scaffold configurations used in the study were scaffold only (PCL), scaffold infused with calcium sulfate (CS), scaffold infused with calcium sulfate–containing BMP-2 (BMP2), and the same scaffold types but with salicylic acid(poly(anhydride ester)) (SAPAE) caps (PCL + CAP, CS + CAP, and BMP2 + CAP).
Polymer synthesis and characterization
The cap of the scaffold was synthesized by layering a slow degrading SAPAE polymer at the base with a fast degrading SAPAE polymer atop. The slower degrading SAPAE was synthesized by melt polymerization from 2,2′-bis(o-carboxyphenoxy)-pentanoate and α,α′-bis(o-carboxyphenoxy)-p-xylene in a 1:2 ratio as described. 16 The faster degrading SAPAE, poly(1,6-bis(o-carboxyphenoxy) hexanoate), was polymerized as previously described. 16 Polymer structures were characterized by proton nuclear magnetic resonance ( 1 H-NMR) spectroscopy, gel permeation chromatography, and differential scanning calorimetry before use. 18 The in vitro salicylic acid release kinetics for the slow and fast degrading polymers were recently described. 16
Animal model
Male New Zealand White rabbits weighing between 3.5 and 4.0 kg were purchased from Covance, Inc. (Princeton, NJ) for this study. The number of animals used and final group size for each treatment group and time point are summarized in Table 1. Before surgery, rabbits were anesthetized with an intramuscular injection of ketamine (35 mg/kg) and xylazine (5 mg/kg), and an adhesive fentanyl patch (12.5 µg/h) was placed on the inner area of the ear for post-surgical pain relief. The surgical site was shaved, aseptically cleaned, and draped. A 4-cm incision was made through the skin and periosteum along the midline of the calvaria, and the soft tissues were retracted to expose the parietal bone. A 1-cm defect was created in the right parietal bone using a hand-powered, trephine drill. 16 Care was taken to avoid disturbing the dura beneath. The site was flushed with saline, and a scaffold was inserted into the defect. The periosteum was sutured over the scaffold, and the skin was closed separately thereafter. All animal procedures were approved by the Rutgers-New Jersey Medical School Institutional Animal Care and Use Committee and followed National Institutes of Health (NIH) guidelines for the care and use of laboratory animals. Multiple reports studying bone regeneration in rabbit parietal bones have used a 1-cm defect.19 –21
Summary of animal use.
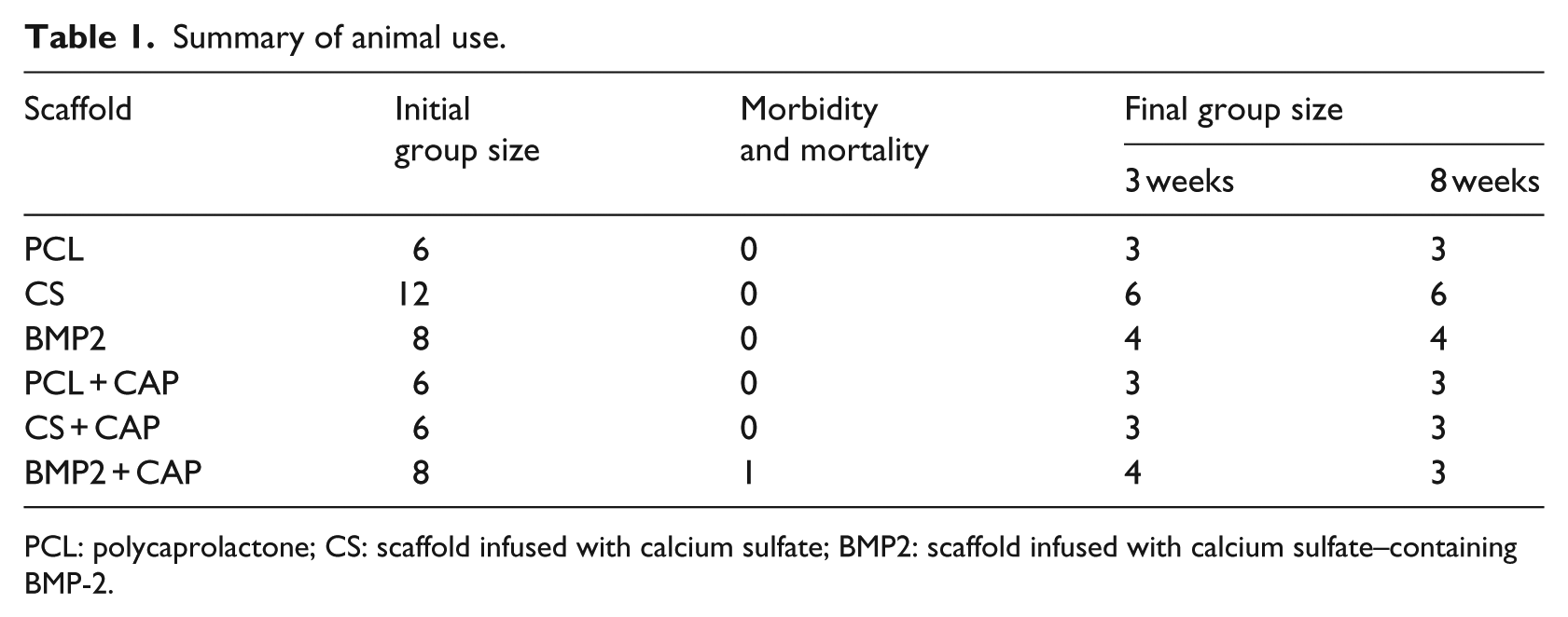
PCL: polycaprolactone; CS: scaffold infused with calcium sulfate; BMP2: scaffold infused with calcium sulfate–containing BMP-2.
Microcomputerized tomography
Three-dimensional (3D) microcomputerized tomography (µ-CT) images were generated to quantify the bone volume (BV; mm3) within the defect area using a high-resolution µ-CT system (Skyscan 1172; Micro Photonics, Inc., Allentown, PA). A portion of the parietal bone containing the scaffold was excised, fixed in 10% formalin for 7–10 days and then transferred into 70% ethanol overnight before µ-CT scanning. All samples were scanned at 70 Kvp, an intensity of 142 mA, and a voxel size of 12 µm isotropic using a 0.5-mm aluminum filter to reduce beam-hardening. X-ray images were reconstructed and analyzed using software provided by Micro Photonics, Inc. (NRecon and CTAn, respectively). Analysis was based upon a 9.0-mm cylindrical region of interest (ROI) over a fixed distance of 3.62 mm (301 slices per sample). Standard 3D analysis was performed to calculate BV.
Histology
Following µ-CT, samples were dehydrated through grades of ethanol and embedded in poly(methylmethacrylate). Sections were cut along the diameter of the scaffold to obtain a lateral view. The sections were polished and stained with Stevenel’s blue for soft tissues and counter-stained with van Gieson’s picrofuchsin for mineralized tissue. 22
Digital images of each histological specimen were collected using a compound, upright microscope (Olympus BH-2, Tokyo, Japan), a SPOT Idea camera, and Spot Basic software (Spot Imaging Solutions, Sterling Heights, MI) at 0.67× magnification. Digital images were analyzed using Image-Pro Premier 9.0 (MediaCybernetics, Inc., Rockville, MD) for total bone areas. A rectangular ROI (10,000 µm3 × 2500 µm3) was centered to encompass the scaffold area directly underneath the cap visible on the image. Bone areas were normalized to obtain the total percentage of bone formed relative to the total available area provided by the scaffold.
Statistical analysis
The µ-CT data were compared using analysis of variance (ANOVA). The histomorphometry data were compared using two-way ANOVA with scaffold type and time as the independent variables and mineralized tissue area as the dependent variable. Between-group comparisons were performed using the Student–Newman–Keuls method to control for multiple comparisons and p values of <0.05 were significant. Data are reported as the mean ± standard error of the mean for each group. Calculations were performed using the statistical functions found in Sigmaplot v12.5 software (Systat Software, Inc., San Jose, CA).
Results
Disposition of the animals
The animals used for this study are described in Table 1. No complications were encountered during the surgical procedure. One 8-week, capped experimental rabbit was euthanized 3 days after surgery due to hyperthermia.
Calcium sulfate resorption
The SAPAE cap increased the time required for resorption of the calcium sulfate infused into the scaffold (Figure 1). Lateral and radial images from the µ-CT analysis of 3-week specimens showed a hemisphere of X-ray dense material in the CS + CAP and BMP2 + CAP defects that was not present in the uncapped scaffolds (Figure 1(a)). The hemisphere of X-ray dense material is not present after 8 weeks (Figure 1(b)). Thus, the X-ray dense material appears to be calcium sulfate matrix infused into the scaffold that has not yet been resorbed. We also observed X-ray dense material at the peripheral edges of calcium sulfate infused scaffolds that we believe is precipitated calcium from the resorbing calcium sulfate and not bone.
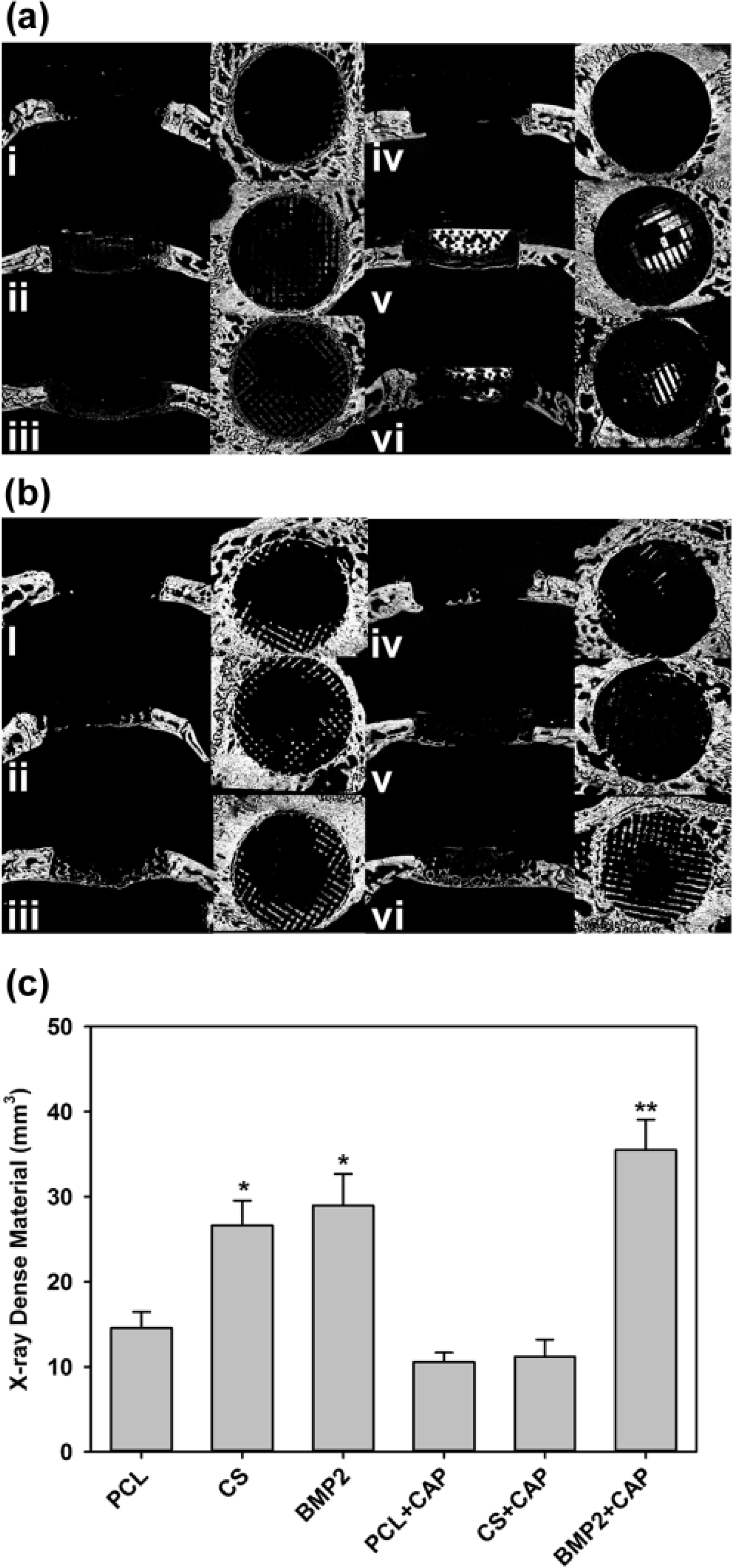
Defect X-ray dense material (mineralized tissue) as assayed by microcomputerized tomography (µ-CT). Panels (a) and (b) show lateral sections on the left and dorsal sections on the right for uncapped scaffolds (i–iii) and SA polymer capped scaffolds (iv–vi). Panel (a) shows µ-CT images from samples collected 3 weeks after surgery. Panel (b) shows µ-CT images from samples collected 8 weeks after surgery. Samples were from (i) PCL, (ii) CS, (iii) BMP2, (iv) PCL + CAP, (v) CS + CAP, and (vi) BMP2 + CAP treated rabbits. Panel (c) shows mean values for µ-CT mineralized tissue within the defect volume of each group (±SE) after 8 weeks of healing. Mineralized tissue in the BMP2 + CAP group (**) was significantly greater than all other treatment groups except the uncapped BMP2 and CS groups. The BMP2 and CS groups (*) had significantly more mineralized tissues than all other groups except the BMP2 + CAP groups. Group sizes were 3, 6, 4, 3, 3, and 3 for the PCL, CS, BMP2, PCL + CAP, CS + CAP, and BMP2 + CAP groups, respectively.
BV
X-ray dense material within the defect volume was determined using µ-CT analyses (Figure 1(a)). The amount of X-ray dense material in the 3-week defects that were treated with capped scaffolds likely included calcium sulfate that had not been resorbed or had precipitated at the peripheral edges of the scaffold. Thus, we did not consider the X-ray dense material in the 3-week defects to be predominantly bone, which was subsequently confirmed by histological examination (see below). Consequently, a quantitative analysis of bone formation using the 3-week µ-CT data could not be performed.
After 8 weeks of healing, defects treated with BMP2 + CAP scaffolds had significantly more X-ray dense materials in the defect volume than all other groups except for the BMP2 and CS scaffold groups (Figure 1(c)). There was no evidence of residual calcium sulfate in the defect by histological examination (see below), and thus, the X-ray dense material within the defect volume was considered new bone. The BMP2 + CAP group had 22% and 33% more X-ray dense materials in the defect volume than the uncapped BMP2 and CS groups, respectively, but the differences were not significant. The BMP2 + CAP group had 3.5× more X-ray dense materials in the defect volume than the PCL + CAP or CS + CAP groups. In contrast, the amount of X-ray dense material in the uncapped CS and BMP2 defect volumes was significantly greater than all other groups except the BMP2 + CAP group (Table 2).
Between-group p values for 8-week defect mineralized tissue volume using the Student–Newman–Keuls method (ANOVA, p < 0.001).
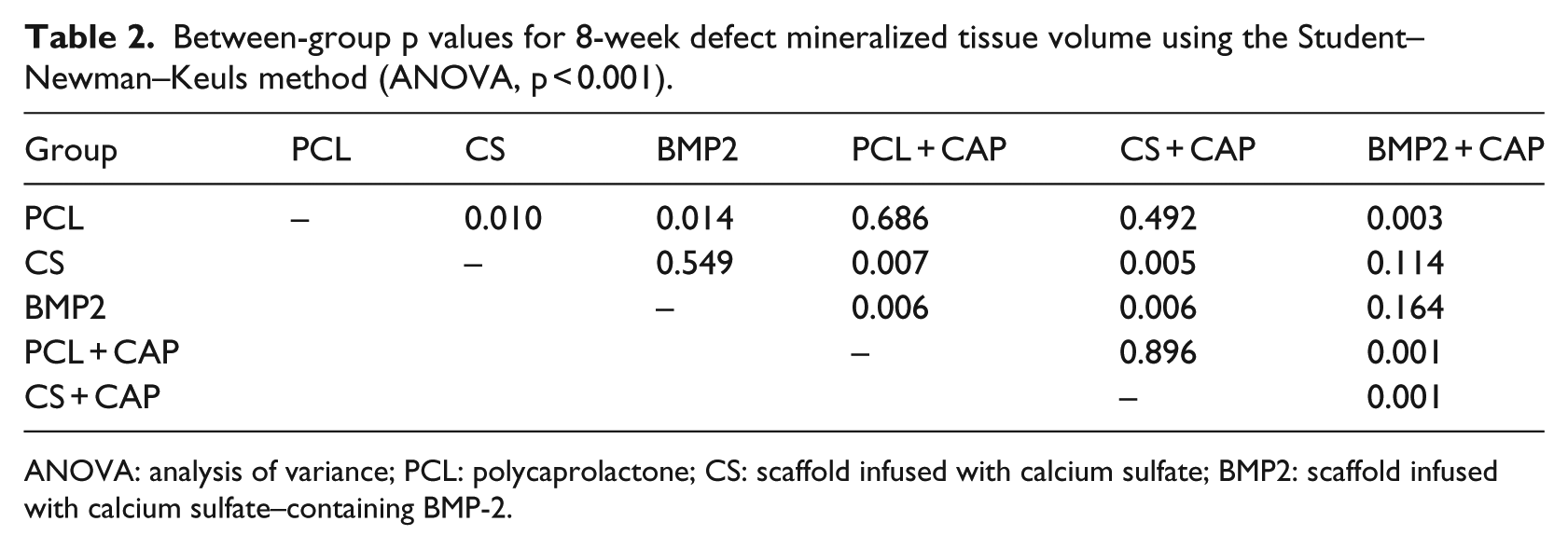
ANOVA: analysis of variance; PCL: polycaprolactone; CS: scaffold infused with calcium sulfate; BMP2: scaffold infused with calcium sulfate–containing BMP-2.
Histomorphometry
Representative histology specimens are shown in Figures 2 and 3. Bone formation in the scaffold was analyzed by histomorphometry (Figure 4). Bone was evident in all scaffold configurations and increased over time, so that more bones were present at 8 weeks than at 3 weeks (p < 0.001). After 3 weeks, greater bone areas in the CS and BMP2 groups were statistically different from other groups as detailed in Table 3. However, by 8 weeks, bone area in the BMP2 and BMP2 + CAP groups was significantly greater than all other groups and almost 2× more than the CS + CAP group. Bone appeared to grow appositionally from the surrounding parietal bone. Remnants and voids left by the SA polymer caps were evident in the 3- and 8-week histology.
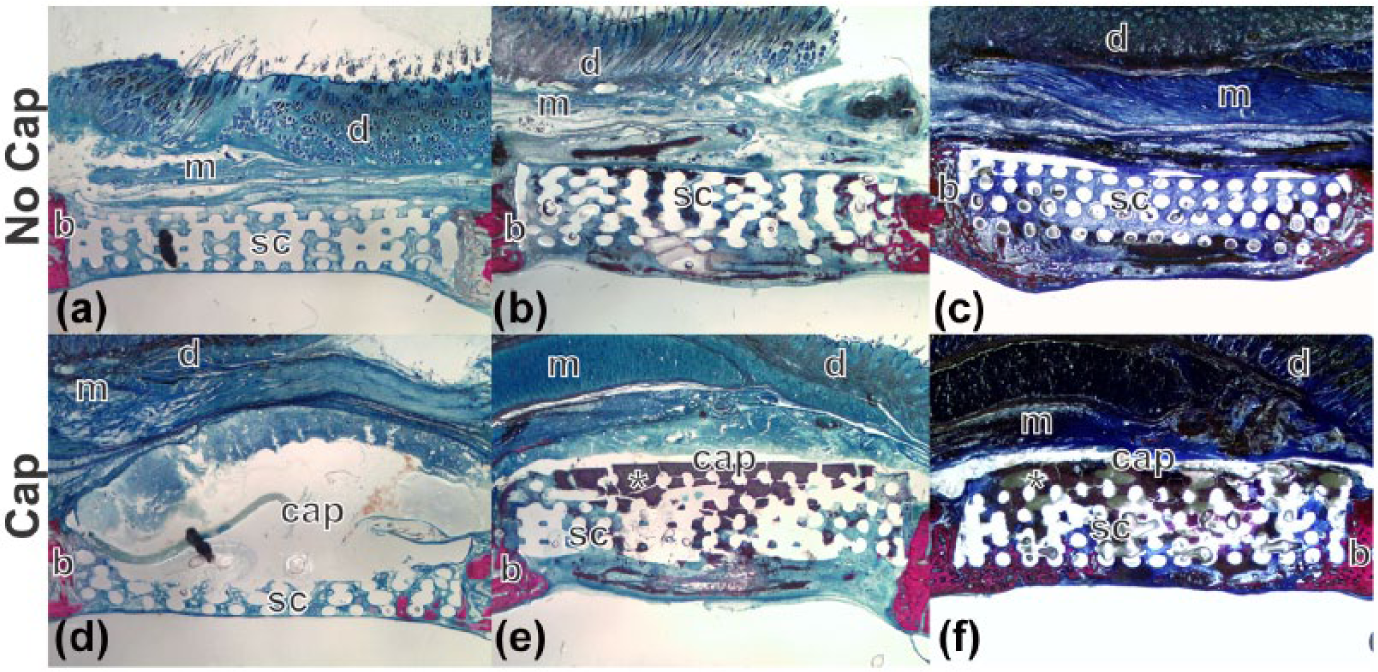
Histology images of 3-week specimens (a–c) without and (d–e) with SA polymer caps. Plastic embedded specimens were sectioned and stained for bone (red) and soft tissues (blue). Representative specimens from each treatment group are shown: (a) PCL, (b) CS, (c) BMP2, (d) PCL + CAP, (e) CS + CAP, and (f) BMP2 + CAP. The void left by the SAPAE polymer cap or remnants of the cap were evident (d–e, cap), and calcium sulfate was evident in the capped (e and f, *) specimens but not the uncapped specimens (b and c). The scaffold (sc), edges of the parietal bone (b), subcutaneous muscle (m), and skin (d) are marked.
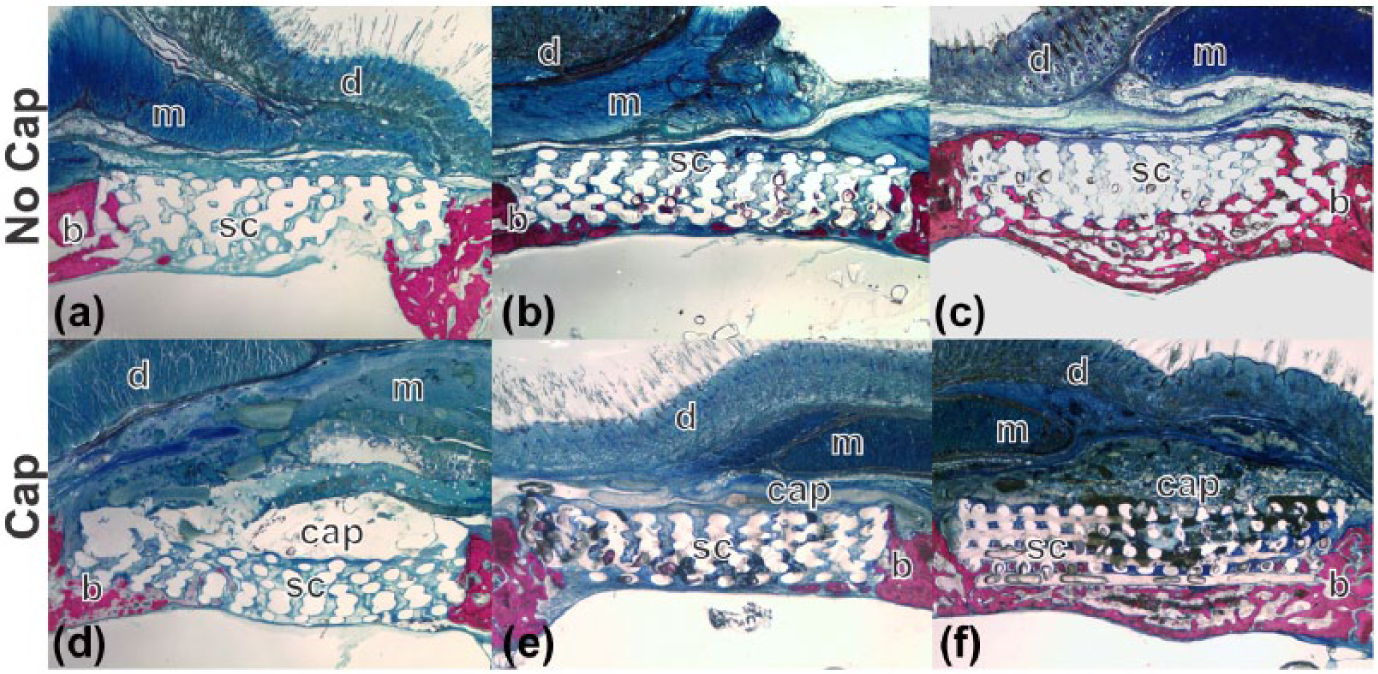
Histology images of 8-week specimens (a–c) without and (d–e) with SA polymer caps. Plastic embedded specimens were sectioned and stained for bone (red) and soft tissues (blue). Representative specimens from each treatment group are shown: (a) PCL, (b) CS, (c) BMP2, (d) PCL + CAP, (e) CS + CAP, and (f) BMP2 + CAP. The void left by the SAPAE polymer cap or remnants of the cap were evident (d–e, cap) in the specimens. The scaffold (sc), edges of the parietal bone (b), subcutaneous muscle (m), and skin (d) are marked.
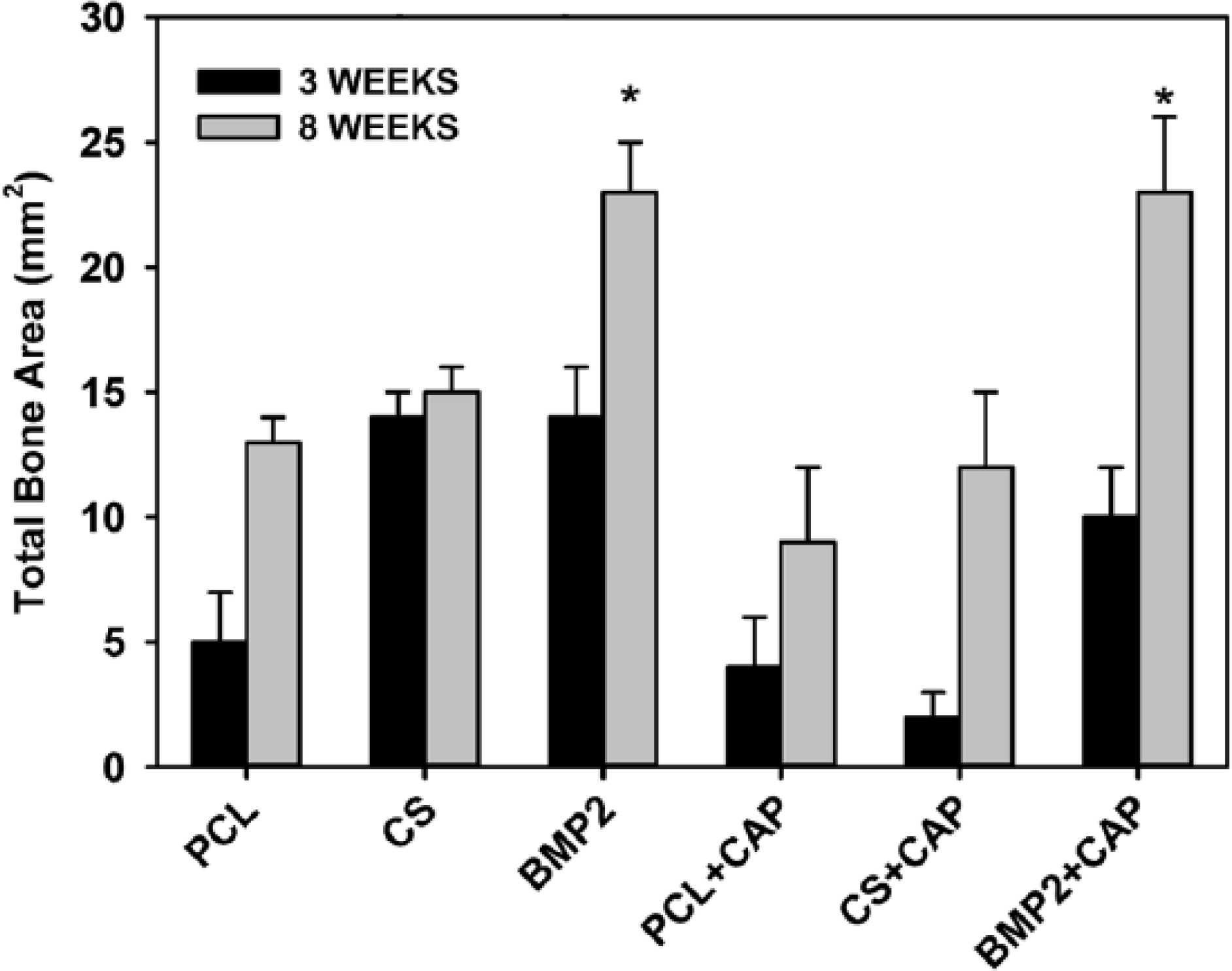
Bone formation in defect measured by histomorphometry. Shown are mean values (±SE) for bone area within the defect at 3 (black bars) and 8 weeks (gray bars). Eight weeks after surgery, the uncapped BMP-2 (BMP2) and capped BMP-2 (BMP2 + CAP) groups had similar amounts of bone that were significantly greater than all other groups (*). Group sizes for each scaffold and time point are shown in Table 1.
Between-group p values using the Student–Newman–Keuls method for 3- and 8-week histomorphometric measurement of defect bone area following two-way ANOVA using time and group as independent variables.
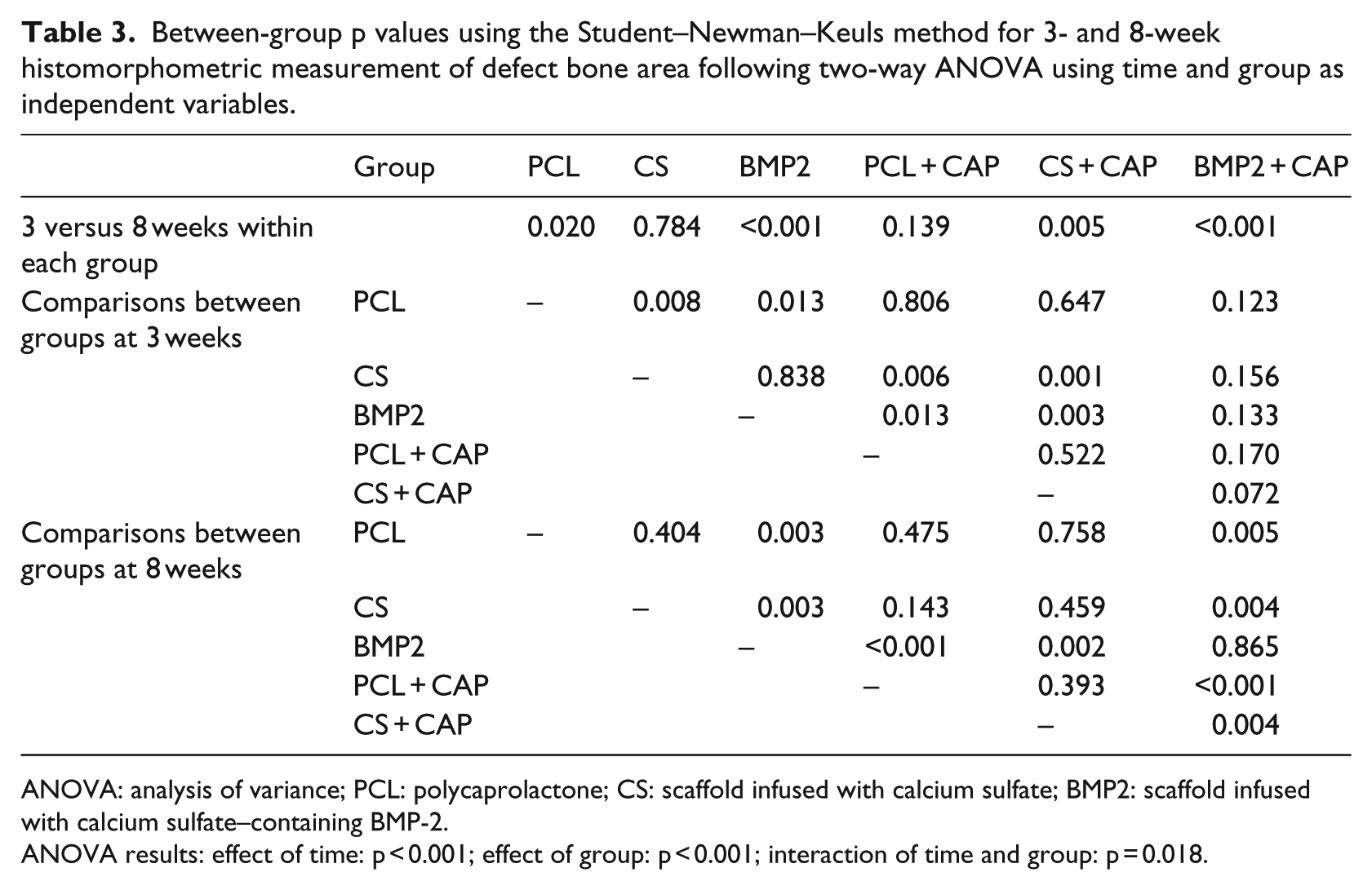
ANOVA: analysis of variance; PCL: polycaprolactone; CS: scaffold infused with calcium sulfate; BMP2: scaffold infused with calcium sulfate–containing BMP-2.
ANOVA results: effect of time: p < 0.001; effect of group: p < 0.001; interaction of time and group: p = 0.018.
Discussion
Salicylic acid can inhibit inflammation, cylcooxygenase activity, and bone formation similar to other NSAIDs.16,23,24 However, high concentrations of salicylic acid are needed to inhibit cyclooxygenase-2 (IC50 of 5 µg/mL in interleukin-1 beta (IL-1β)-stimulated A549 cells). 24 In addition, a previous study found that locally applied BMP-2 was able to overcome the inhibitory effects of systemic ketorolac, an NSAID, on spinal fusion in rabbits. 25 Consequently, we theorized that by using SAPAE polymers, salicylic acid release can be kept at levels below that required to inhibit cyclooxygenase-2 and by extension bone formation. Any negative effects of salicylic acid on bone formation would be overcome by BMP-2. As shown in Figure 1(c), after 8 weeks of healing, the amount of new bone formed was 3.5-fold greater in defects treated with BMP-2 but was similar between BMP-2-treated defects with or without the SAPAE polymer cap. These data indicate that the SAPAE polymers did not significantly impair BMP-2-induced bone formation and that the SAPAE polymers can be used for guided bone regeneration applications requiring use of BMP-2.
In our previous study using SAPAE polymers to cap an osteoconductive scaffold, we noted a trend toward reduced bone formation immediately adjacent to the SAPAE polymer. 16 We hypothesized that locally high salicylic acid concentrations from the degrading SAPAE polymer were inhibiting bone formation. Unlike systemic NSAID treatment, however, the degree of bone formation inhibition was not high enough to detect a statistical difference, and no overall effect on bone formation within the defect was observed. Although we did not specifically measure bone formation within different regions of the defect volume in this study, we observed a similar effect of reduced BMP-2-induced bone formation adjacent to the SAPAE polymer (compare Figure 3(c) and (f)). Any localized inhibition of BMP-2-induced bone formation by the SAPAE polymer was not sufficient to reduce the overall amount of bone formed within the defect region (Figures 1(c) and 4). We also observed reduced new bone area in the capped scaffolds relative to the uncapped scaffolds at 3 weeks. This effect was significant between the uncapped and capped CS scaffolds (p < 0.001, Table 3). Whether the reduced bone area observed in the capped CS scaffold was caused by salicylic acid released from the SAPAE polymer or the SAPAE cap acting as physical barrier to cell access to the scaffold is not yet known. By 8 weeks, however, no effect of the cap on scaffold bone area was observed. These observations suggest that further SAPAE polymer optimization could produce an even more effective polymer for guided bone regeneration applications.
The SAPAE polymer cap also affected resorption of calcium sulfate within the scaffold and, therefore, likely prolonged the release of BMP-2 within the defect. Calcium sulfate is primarily resorbed in the body by surface erosion.26,27 µ-CT images from the 3-week specimens clearly showed residual calcium sulfate as an inverted hemisphere adjacent to the SAPAE polymer (Figure 1(a)). By 8 weeks, the inverted hemisphere of calcium sulfate is no longer present. Histology indicated that the SAPAE caps clearly present at 3 weeks had significantly degraded by 8 weeks (compare Figures 2 and 3). Thus, it appears as though the calcium sulfate surface in contact with the SAPAE polymer is being protected from erosion. Histomorphometry 3 weeks after surgery also suggests that BMP-2 is being released faster from the noncapped scaffolds as evidenced by the increased bone formation (Figure 4). These observations also indicate that SAPAE polymer composition and BMP-2 carrier can be engineered to produce a desired tissue response in terms of drug delivery and tissue response.
In addition to SAPAE polymer characteristics, optimization of scaffold material, BMP-2 dose, and BMP-2 carrier would likely be required for each guided bone regeneration application. Here, the scaffold was made of biodegradable PCL. However, in vivo degradation of PCL occurs over months, and PCL lacks osteoconductive properties.28,29 The use of an osteoconductive scaffold material or materials that more rapidly degrade in vivo may produce an overall better response. Only one dose of BMP-2 was tested in this study. Nominally, larger BMP-2 doses or more sustained dosing with BMP-2 will produce a greater osteogenic response.30,31 In some contexts, such as cervical spine fusions, large BMP-2 doses have been associated with adverse events such as excessive tissue swelling.12,32 –34 We suggest that the SAPAE polymer can be used to focus the volume in which BMP-2 acts, and therefore, higher doses of BMP-2 can be used in conjunction with an optimized delivery vehicle and scaffold material to produce robust guided bone regeneration.
Improved methods will make guided bone regeneration technology applicable to additional and more difficult bone healing problems. Currently, polytetrafluoroethylene (PTFE) membrane is used clinically for dental-related guided bone regeneration.35,36 The PTFE protects the bone healing site from fibrous tissue invasion while allowing osteogenesis to occur in the healing site. A significant limitation to use of PTFE membrane for guided bone regeneration applications is that the PTFE is not biodegradable, and consequently, additional surgery is needed to remove the membrane after bone regeneration is complete. In contrast, we recently demonstrated that biodegradable SAPAE polymers could be used for guided bone regeneration when coupled with an osteoconductive scaffold while limiting the local inflammatory response. 16 Here, we extended those studies to show that SAPAE polymers did not impair BMP-2-induced bone formation in a rabbit parietal bone trephine defect model after 8 weeks of healing. Together, our two studies demonstrate the potential utility of SAPAE polymers for use in guided bone regeneration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Award Number R01DE019926 from the National Institute of Dental & Craniofacial Research. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Dental & Craniofacial Research or the National Institutes of Health.