
Abstract
Recent events and regulatory mandates have underlined the importance of medical planning and preparedness for catastrophic events. The purpose of this review is to provide a brief summary of current commonly identified threats, an overview of mass critical care management, and a discussion of resource allocation to provide the intensive care unit (ICU) director with a practical guide to help prepare and coordinate the activities of the multidisciplinary critical care team in the event of a disaster.
Introduction
A variety of natural and man-made disasters over the past decade have elevated awareness of both the US government and the American public to the importance of planning and preparing for catastrophic events. In response to the events of September 11, 2001, the Joint Commission on the Accreditation of Healthcare Organizations mandated that all accredited hospitals within the United States have written disaster plans. Although a common starting point in this planning process involves the appropriate training and allocation of prehospital and emergency department resources, it is important to recognize that many high-risk disaster scenarios identified by experts may generate significant numbers of casualties who require critical care. The purpose of this article is to briefly summarize the critical care implications of current threats and to provide a practical outline to the intensive care unit (ICU) director to guide efforts in disaster preparedness planning at individual institutions.
Threats
In 2007, the US Department of Homeland Security published their National Preparedness Guidelines. 1 These guidelines highlight 15 national disaster scenarios, 12 of which have the potential to produce large numbers of critically injured or ill patients. These 12 scenarios can be broadly divided into the general caregories of terrorist attacks, epidemic disease, and natural disaster (Table 1). 2
Catastrophic Disaster Scenarios, National Preparedness Guidelines of the Department of Homeland Security 1
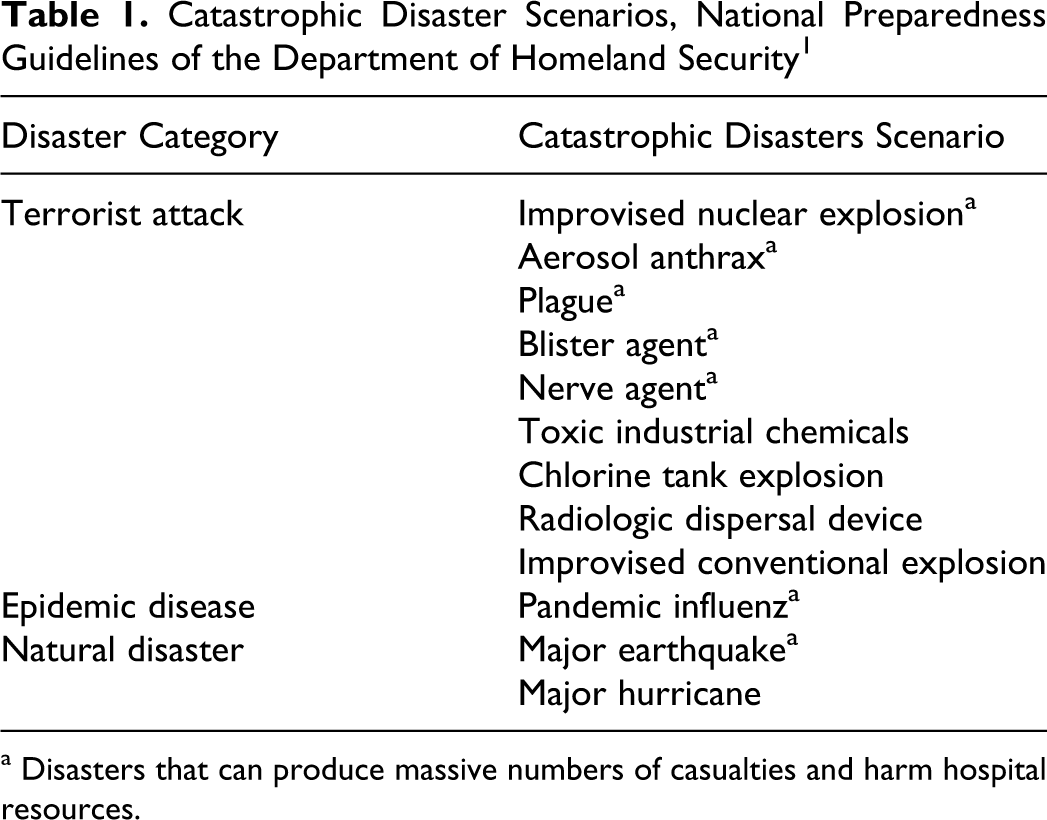
a Disasters that can produce massive numbers of casualties and harm hospital resources.
Recent disasters have actually demonstrated that the majority of victims of disasters does not require critical care interventions.3–6 Data from 10 worldwide terrorist attacks prior to 1995 estimate the percentage of critically injured to be approximately 16% of the overall number of survivors (range 2.5%-34%). 7 However, published experience has also demonstrated that in mass casualty situations, the ICU is also commonly utilized as an overflow area for primary triage, as well as initial and overflow postoperative management. 8 It is, therefore, important to perform critical care disaster planning in concert with other key services of the institution, and if possible, with other health care organizations within the region.
Mass Critical Care Management
A disaster can strike with little or no warning, leaving insufficient time to rally additional staff and resources. Disruption of usual communication and transportation lines may limit the opportunity to transfer current or overflow patients to nearby hospitals, and delay regional, state, and federal assistance in the initial aftermath of a disaster. These conditions may overwhelm the ability of an individual institution to provide timely, full spectrum intensive care to all patients in need, and place patients at risk of dying, without modification of usual critical care practices.9,10
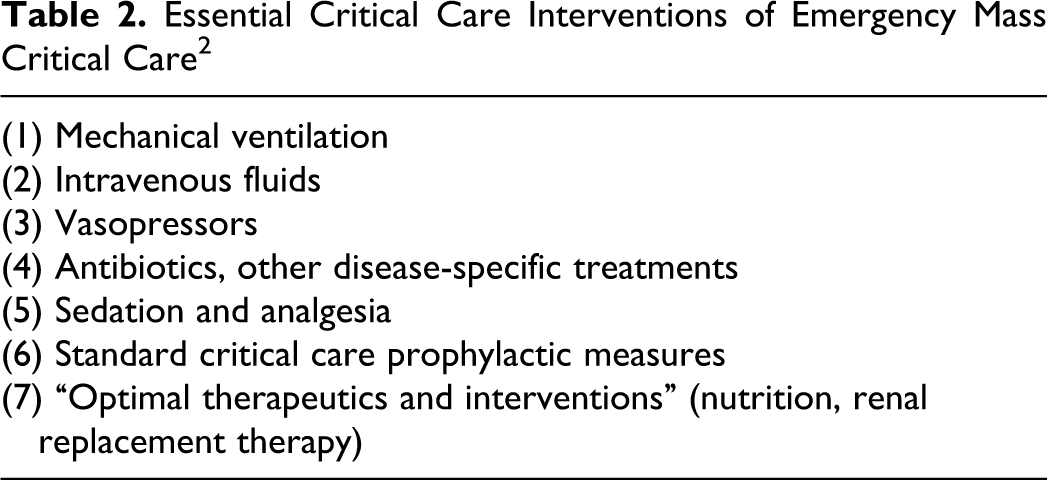
The concept of emergency mass critical care (EMCC) involves planning and provision of essential interventions to maximize the number of individuals who receive sufficient critical care (Table 2). 11 Emergency mass critical care is appropriate when the number of patients supersede a hospital’s capacity to provide standard critical care. 12 Medical resource planning for EMCC can be divided into 3 categories: treatment materials, hospital personnel, and facilities, orstuff, staff, and space. 2
Essential Critical Care Interventions of Emergency Mass Critical Care 2
Stuff: Medical Equipment and Supplies
The interventions listed in Table 2 identify baseline requirements for critical care delivery. Additional ancillary equipment will be required for many of these interventions. While disease-specific treatments may fall into short supply based on the type of disaster (ie, antiviral drugs in an influenza pandemic), 13 mechanical ventilators, and oxygen are predictable deficiencies in many disasters, and therefore deserve special focus. 14
There are an estimated total of 105 000 ventilators in the United States currently, and this number is likely insufficient to deal with a pandemic influenza outbreak or lung injury following a widespread terrorist attack. 15 Most hospitals cannot afford to stockpile ventilators, and in a catastrophic disaster, transportation and communication disruption may limit the ability to draw from regional and national stockpiles. Alternatives include the use of anesthesia machines, noninvasive positive pressure ventilation (NIPPV), and in a last resort, modification of a single ventilator to ventilate multiple patients at once.14,16,17 Each of these strategies has utility in specific circumstances, but clear disadvantages also prevent their adoption in all settings. For example, anesthesia machines may be required in the operating room, NIPPV may be inadequate in significant respiratory failure, and single ventilator modification can permit spread of infection and will not work if there are differences in lung pathophysiology between patients.
Oxygen shortages may result from consumption by large numbers of patients in respiratory failure, or on account of damage of oxygen storage and delivery systems. 14 Medical oxygen sources include bulk and portable liquid systems, compressed gas cylinders, and oxygen concentrators. 18 Most hospitals have sufficient stores of bulk liquid oxygen to support patient needs for the short term. Potential areas of concern include damage to reserve systems that are contiguous with the main system and ventilator models that require a high-pressure gas supply and cannot be supported by small oxygen concentrators.19,20
Staff: Hospital Personnel
The current shortage of critical care trained personnel is well documented.21–24 Staffing issues may be further complicated by the inability of on-call personnel at home to reach the hospital, or by staff absenteeism. 25 Current American College of Chest Physicians (ACCP) guidelines recommend that critical care trained physicians and nurses oversee noncritical care staff to extend their ability to provide direct patient care to large numbers of patients. 20 Systematic efforts to standardize interventions and reduce care variability should be strongly considered using this model.
Staff resources may also be jeopardized by illness during an influenza epidemic or bioterrorist attack.26–28 This is especially true in the critical care setting, where procedures such as endotracheal intubation and bronchoscopy can result in significant pathogen aerosolization. 14 Strategies for infection control include early identification and triage of at-risk populations, 29 and ensuring adequate supply and strict use of personal protective equipment. 30 Hospitals should also fit-test all staff with negative pressure respirators, such as the n95 mask. 30
The ACCP guidelines suggest that hospitals should be prepared to deliver EMCC for up to 10 days without external assistance, 9 placing staff at significant risk of sleep deprivation and exhaustion with time. 31 The deleterious effect of inadequate sleep on performance is well documented, and both the stress of a disaster event and the complex critical care environment will exacerbate its impact.32,33 A regimented shift schedule that balances available staff and skills with current clinical demands, as well as the likely duration of time before help arrives, should be considered and implemented within the first 24 hours.
Space: Facilities
Critical care interventions, particularly in the management of respiratory failure and shock, rely heavily on machines and equipment. 2 Critical care can only be performed in locations with electricity, oxygen, and monitoring equipment and is restricted to hospitals or specially outfitted mobile units.6,20,34 This conclusion is reinforced by the experience at Chelsea Pier during 9/11, which demonstrated that ad hoc critical care outside of a hospital is ineffective. 3 Intensive care units, postanesthesia care units (PACUs), and emergency rooms are best outfitted to provide mechanical ventilation and close monitoring, and step-down units, large procedure suites, telemetry units, and hospital wards may be used for EMCC when capacity in these spaces is exceeded. 20 Facility planning for both backup systems and expansion of services (ie, generator availability) is essential to maximize critical care capacity.31,35
Because care of noncritical patient has significantly less infrastructure requirements, strong consideration should be given to transfer of stable patients to “surge facilities” and maximize dedicated hospital space for critical care delivery in an overflow situation. 34 The Joint Commission has published a thorough guideline on surge facility strategies. 36
Resource Allocation
Triage in a disaster is inherently complex. 37 The trauma literature3,7,8,38 tends to focus on the initial triage of patients, while the disaster critical care literature12,39–42 highlights the later triage of resources. Thus, triage can be divided into patient and resource considerations. Patient triage identifies victims who require immediate care in order to survive, and aims to prevent overtriage. 38 Resource triage involves using objective, fair, and transparent decision criteria to delineate how care should be delivered if there are insufficient resources to provide critical care to all who require it to survive. 42
Patient Triage
While less applicable in disasters with a gradual onset, patient triage is vitally important in sudden events like explosions or natural disasters.2,43 Minimizing overtriage, the delivery of immediate care to disaster victims who are not critically ill or injured, is vital to ensure that critical patients are identified early enough to receive lifesaving, definitive care. In his analysis of 10 terrorist bombing incidents, Frykberg established a direct linear relationship between overtriage and critical mortality rate (percentage of critically ill or injured patients who die in the hospital). 7 This relationship demonstrates that well-executed patient triage can save lives.
Perhaps the most important strategy to prevent overtriage includes the use of an experienced triage officer, usually a senior physician, who has a clear understanding of the medical resources at hand and the ability to recognize and, if necessary, perform immediate lifesaving measures. 8 Evacuating critical patients to the closest hospital and noncritical patients to surrounding hospitals is another frequently cited method to maximize survival in a mass casualty event.3,7,38,44,45
Triage activities should be performed outside of the hospital if possible to control the flow of only those patients who require immediate attention to traditional patient care areas. In an elegant analysis of 20 major international terrorist attacks and their own experience in managing over 20 mass-casualty incidents in Israel, Ashkenazi et al proposed a “customized plan” for patient triage. 8 The customized plan differs from the traditional unidirectional flow plan38,45 by aiming to identify and treat critical patients first, allowing stable patients with lesser injuries to wait in clearly designated and geographically distinct areas, and employing the most experienced trauma leaders—surgeons, emergency physicians, and intensivists—in the care of patients instead of in managerial roles.
Resource Triage
Resource triage is arguably the most problematic issue in disaster medicine because it inevitably raises the concern of health care rationing that will potentially impact individual survival. Because of the numerous ethical, legal, and social ramifications,resource triage should be considered only after all efforts to obtain scarce resources, transfer patients, or augment care through EMCC have failed. 12 To ensure appropriate legal and societal support, resource triage should be done in collaboration with regional and federal public health authorities using objective, fair, and transparent criteria for provision of care.12,39
Most resource triage guidelines rest on the utilitarian aim to save the greatest number of critically ill patients as possible.39-42 This goal justifies the use of explicit exclusion criteria to identify patients who are least likely to survive and/or most likely to require significant critical care resources in order to survive, at the risk of violating the principle of distributive justice and individual patients' expectation of equal access to treatment.46,47 These exclusion criteria have been the subject of significant controversy.
In a thoughtful review of the ethics of resource triage, White et al attempt to reconcile these dilemmas by offering a “multiprinciple allocation strategy” using a point allocation system based on 3 criteria: saving the most lives, maximizing life years, and the life-cycle principle (Table 3). 46 Maximizing life years is a utilitarian aim that would devote resources to patients with the fewest underlying medical conditions but has the ethical benefit of not explicitly denying access to any 1 group. The goal of the life-cycle principle is to allow individuals the opportunity to have a normal life span, and so would preferentially allocate resources to younger patients.
“Multiprinciple” Resource Allocation Strategy 46
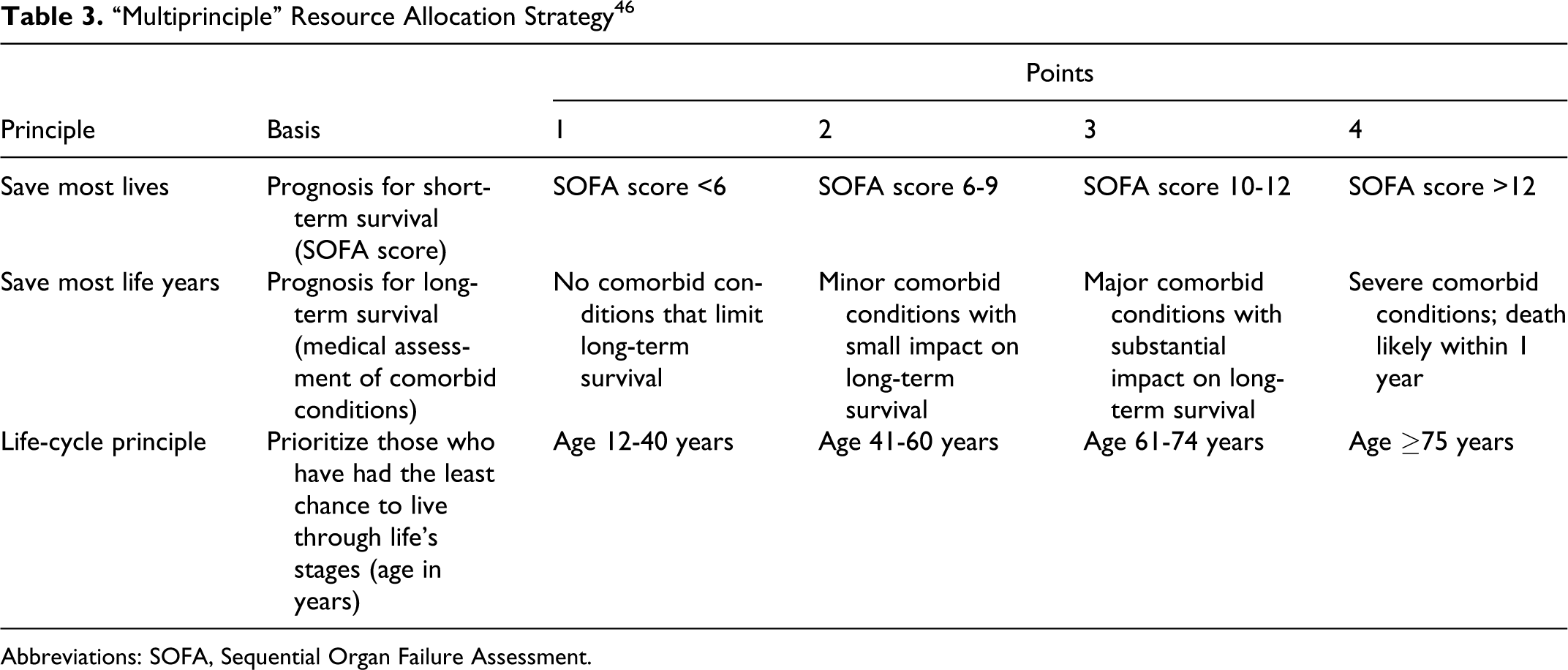
Abbreviations: SOFA, Sequential Organ Failure Assessment.
There are at least 2 difficulties with the White resource triage system. First, the life year maximization concept provides only vague delineation among patients with different chronic diseases, which may complicate resource triage during the confusion of an ongoing disaster. By contrast, the decision criteria utilized by other authors are derived from the contention that patients with more severe comorbidities frequently require more critical care resources in order to survive. 48 Second, by placing the life-cycle principle on equal footing with the other 2 criteria, White also potentially overemphasizes advanced age as a predictor of poor outcome. 49
Clearly more work in this area is needed to develop a system that is effective, reasonable, and acceptable to society. Several groups, including White, have favored employing the Sequential Organ Failure Assessment (SOFA) score to stratify patients with respiratory failure and/or shock with end-organ damage in terms of short-term survival, because it relies on objective data that are relatively easy to obtain and has been validated in a variety of critical illnesses.12,39–42,46 Additionally, removing exclusion criteria from decision making in favor of considering the overall prognosis using commonly employed and established tools to stratify chronic illness severity (Model for End-Stage Liver Disease [MELD] score, New York Heart Association [NYHA] heart failure) may be a more effective way of prioritizing critical care interventions.
Coordination
The failure of communications systems in recent disasters, especially terrorist attacks and natural disasters, has been almost universal.3,5,35,50 The Trust for America’s Health (TFAH), sponsored by the Robert Woods Johnson Foundation, include streamlined and effective communication channels as 1 of the 8 core goals of a public health emergency response to enhance rapid and accurate transfer of information between health care workers, frontline responders, and the public. 51 Routine communications systems are likely to be subject to excessive demand and possible disruption immediately following a disaster, and the chaos that will follow a sudden surge of patients presenting to a health care facility will make identification and communication between key leaders within the organization difficult.
It is considered the responsibility of local and regional health officers to identify medical disaster communication needs and establish primary and backup systems linking response providers, health care facilities, and emergency operations centers. Scheduling regular training and exercises with these systems are important to enhance preparedness, and incorporating their use into daily operations and communications within and between hospitals would be ideal. Two-way radios assigned to key leaders responsible for coordination of services is likely the most effective way to communicate within a single institution to address events immediately following a disaster, with a well practiced protocol of communication to minimize omissions and misunderstandings that are otherwise likely to occur.
Conclusion
Intensive care unit directors are increasingly asked to develop and lead disaster planning and preparedness activities due to continuing world events and increased regulatory requirements. This summary is designed to provide a brief overview and checklist (Table 4) of common considerations and issues that a multidisciplinary critical care team is likely to confront in their planning and response to a catastrophic event. Review and coordination with other key services within the institution, other local institutions, and regional public health authorities is essential to ensure that individual critical care preparedness efforts are coordinated for maximum effectiveness.
Catastrophic Disaster Critical Care Planning Considerations: A Checklist
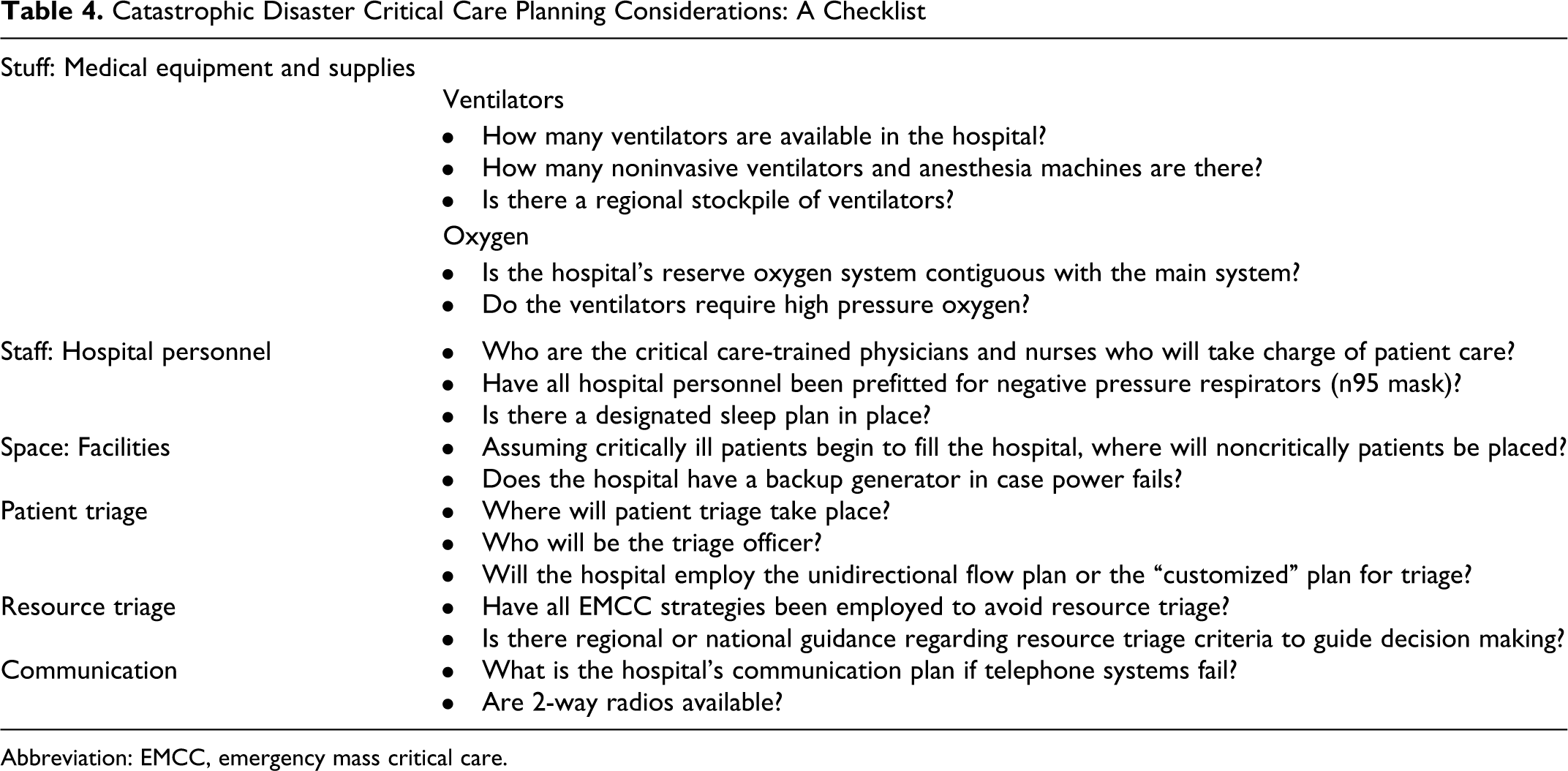
Abbreviation: EMCC, emergency mass critical care.
Based on their likelihood and topical relevance, we have selected a large conventional explosion from a terrorist attack, a major hurricane, and pandemic influenza as high-yield, illustrative examples on which to base our discussion of disaster planning efforts.
Conventional Explosion
Although the identification and management of casualties due to biological agents, chemical, and nuclear threats are common topics in disaster planning for a terrorist attack, recent history has demonstrated that improvised explosions are the most common tool employed by these individuals. Past experience has demonstrated that the major influx of casualties should be anticipated within 2 hours of an event, most commonly into the nearest hospital. The first wave of casualties will not be critically injured, but may jeopardize the hospital’s ability to care for the subsequent arrivals who will be critically injured and in need of immediate lifesaving care. 7
A large retrospective cohort study of multiple/mass casualty victims transferred to the 6 level 1 trauma centers in Israel over a 33-month period is perhaps the largest published experience on ICU utilization in this area. Of the 1639 patients evaluated between October 2000 and June 2003, 54% had a blast mechanism and 45% were admitted. Thirty-four percent of the admissions had a presenting injury severity score >16, and 60% required surgery (including 36% who went directly to operating room [OR]). The ICU was heavily utilized, serving both as a primary evaluation and as a resuscitation area for 11% of presenting casualties once emergency department and OR resources were saturated, and providing definitive care for 34% of these admissions at some point during their ICU stay. 8 Two thirds of the explosion victims exhibited evidence of multiorgan trauma, with traumatic brain and blast lung injury, penetrating shrapnel, burn and extremity injuries being the most common injuries observed in ICU patients in this and other studies. 52 An excellent review by Ciraulo on the trauma consequences and management of explosions and blast injury, a less familiar mechanism to most US critical care physicians, covers this issue in greater detail. 53
Major Hurricane
The complexity of responding to a major hurricane has been well documented throughout American History. Since Hurricane Katrina tragically struck on August 29, 2005, there has been ample documentation of the heroic responses by individuals and institutions, as well as the multiple failures on the institutional, local, and national levels. Multiple investigations into the Katrina response have examined the various challenges to improve the response to similar disasters in the future. The congressional investigation entitled “A Failure of Initiative,” summarized below, is a comprehensive source of information about medical preparedness and the hurricane response. 54
The first step for hospital planners facing a major hurricane is to establish an effective and safe evacuation plan for current inpatients. The advance warning of hurricanes, as opposed to major earthquakes, makes such a step possible. The logistics, planning, and equipment required to transport a critically ill patient are considerable, in addition to the risk of evacuation. These factors must be carefully weighed against the resources required to effectively care for the patient in place, and the impact (of patients who remain) on critical care capacity for hurricane casualties.
The next step is to preposition key elements of medical care that are likely to be rapidly consumed. Examples include basic supplies such as food and water, essential equipment, and backup communications. Critical care unique elements such as ventilators, monitors, oxygen, as well as an electricity supply should be the focal elements of planning. Of particular importance is the need to designate additional areas for care due to the potential of infrastructure damage to the hospital. Given the significant resource requirements of critical care, a fixed rather than temporary structure is preferable for ICU operations. Adequate ventilation is also important to reduce the risk of carbon monoxide poisoning when all power is derived from generators with carbon-based fuel consumption.
The third and fourth steps of medical care occur after the hurricane strikes. The third phase begins after the hurricane has dissipated enough that care can be provided safely outside of damaged fortified locations. Although the hurricane winds have great potential to cause trauma through high-velocity projectiles and crush injuries, inland flooding produced the greatest number of casualties from 1970 to 1999.2,55 The final phase of medical care occurs after the hurricane has passed and a wake of destruction remains. Preventive medicine is important during this period, as infectious diseases in areas subject to flooding will be the major source of casualties.
In the latter 2 steps, the scope and volume of ICU operations will depend heavily on the capabilities and resources that remain after the hurricane, and the rapidity and scope of the relief response. A basic understanding of the National Incident Management System (NIMS) and National Response Framework (NRF) is important to be able to effectively interface with local command and control elements to determine available and incoming medical assets. 56
Pandemic Influenza
The outbreak and spread of H1N1 influenza in the spring of 2009 provided credence to the longstanding focus of critical care disaster planning on the implications and management of pandemic influenza. Early reports of H1N1 cases raised concern that the virus would mutate into a more virulent form, and that subsequent waves would cause mortality rates akin to the 1918 influenza pandemic. 57 While early analysis demonstrated that H1N1 influenza was more transmissible 58 and more damaging to the lungs 59 than seasonal flu, as of February 2010 the mortality rate of the H1N1 strain was similar to that of seasonal flu. 60
The 1918 influenza pandemic caused approximately 50 million deaths worldwide and, unlike seasonal flu, was devastating to all age groups but the elderly individuals. The extraordinary pathogenicity of the 1918 H1N1 strain may have been due to 2 clinical–pathologic syndromes: acute aggressive bronchopneumonia and an acute respiratory distress syndrome (ARDS) like syndrome. 13 While the modern ICU can offer treatments to each of these syndromes in individual patients, doing so during a pandemic outbreak would quickly overwhelm the resources of a single hospital or region.
Disaster planning for a respiratory pandemic has 2 unique areas of focus. While explosions and disasters occur suddenly with little or no warning, pandemics develop over days to weeks and permit the opportunity for more deliberate preparation.
Early planning considerations include gathering resources, coordinating with regional and national health authorities, establishing work schedules, and considering alternatives for patient and resource triage. The thrust of early planning and coordination should be obtaining ventilators from regional stockpiles and allocating PACU and step-down units for ICU-level care, and developing a plan for utilization of available antiviral medication. Second, infection control must be a priority in pandemics. All staff should be outfitted with negative pressure respirators and hospitals should obtain extra supplies and enforce the use of personal protective equipment. An excellent summary of current clinical and preparedness information on H1N1 influenza is available at the US Department of Health and Human Services Web site flu.gov, including detailed hospital planning checklists. 61
A final consideration for pandemic disaster planning must be a thoughtful and rigorous debate about resource triage. The 1918 pandemic is a humbling reminder of the shear number of patients with respiratory failure associated with a pandemic disaster. Addressing the issue of resource triage in advance can serve to alert medical staff and the communities they serve to the myriad moral issues that will inevitably arise in these difficult circumstances.
Footnotes
The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the US Government.
Acknowledgment
The authors would like to thank Dr. Eric Frykberg for his kind assistance in the preparation of this article.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.