
Abstract
The elderly individuals are the most rapidly growing cohort within the US population, and a corresponding increase is being seen in elderly trauma patients. Elderly patients are more likely to have a hospital length of stay (LOS) in excess of 10 days. They account for 60% of total ICU days. Length of stay is frequently used as a proxy measure for improvement in injury outcomes, changes in quality of care, and hospital outcomes. Patient care protocols are typically created from evidence-based guidelines that serve to reduce variation in care from patient to patient. Patient care protocols have been found to positively impact patient care with reduced duration of mechanical ventilation, shorter LOS in the ICU and shorter overall hospitalization time, reduced mortality, and reduced health care costs. The following study was designed to assess the impact of the implementation of 4 patient care protocols within an elderly trauma population. We hypothesized that the implementation of these protocols would have a beneficial impact on patient care that could be measured by a decrease in hospital LOS. An archival, retrospective pretest/posttest study was performed on elderly trauma patients. The new protocols helped guide practical changes in care that resulted in a 32% decrease in LOS for our elderly trauma patients which exceeds the 25% decrease found in other studies. Additionally, the “Other” category for each variable was less frequently used in the post-protocol phase than in the pre-protocol phase, suggesting a spillover effect on the level of detail recorded in the patient chart. With less variation in practices in the post-protocol phase, Injury Severity score, and admission systolic blood pressure emerged as significant predictors of LOS.
The elderly individuals are the most rapidly growing cohort within the US population, and a corresponding increase is being seen in elderly trauma patients. It is anticipated that the percentage of people over age 65 will rise from 12% in 2000 to 20% by 2030. At least one projection suggests that by 2050, up to 40% of all trauma patients will be 65 years of age or older. 1 –3
As age increases, there is also a decline in physiologic reserve. This decline leaves the elderly patient poorly equipped to withstand a challenge to any organ system. Given this, it is not surprising that elderly trauma patients are nearly 5 times more likely to die of their injuries than younger patients. 2,4,5 In addition, elderly patients are more likely to have a hospital length of stay (LOS) in excess of 10 days, 6,7 and they also account for 60% of total ICU days. 3
Length of Stay as a Valid Proxy Measure of Quality of Care in Trauma Patients
Hospital LOS is frequently used as a proxy measure for improvement in injury outcomes, 8 changes in quality of care 9 and hospital outcomes. 10 The American College of Surgeons Committee on Trauma Resources for Optimal Care of the Injured 11 specifically uses LOS as an outcome measure for performance improvement and, through the Trauma Quality Improvement Program (TQIP), provides performance benchmarks to compare LOS performance across trauma centers. 12 These benchmarks suggest that a decrease in LOS is used as a proxy measure for care that has become more efficient and effective. Several studies 10 ,13-15 identified hospital-acquired complications as a significant predictor of hospital LOS in the elderly individuals. Specifically, 95% of long-stay patients (>28 days) acquired other medical problems which were not directly linked to their admission diagnosis. 13 Sepsis was the most common medical complication, followed by pneumonia, urinary tract infections, and delays in discharge due to weaning from urinary catheters. It was estimated that the excess LOS attributed to hospital complications ranged anywhere from 7.8 days to 22 days. 14 These studies, taken as a whole, suggest reducing LOS could reduce hospital-acquired complications that accrue over long hospitalizations.
The Use of Patient Care Protocols
The goal in developing and implementing a patient care protocol is to create evidence-based guidelines that will reduce variation in care from patient to patient. 16 Effective protocols delineate an agreed-upon plan of action that can be implemented once the predetermined signs and symptoms present themselves. This improves communication between members of the health care team and allows a more dynamic response to emerging clinical issues. The benefits of patient care protocols in the critical care environment have been well documented in the research literature. 6 Protocols designed for ventilator weaning report a reduction in the amount of time on mechanical ventilation 17 as well as a reduction in the number of ventilator-associated pneumonias (VAPs) and hospital days. 18 Sedation protocols used with patients on mechanical ventilation have reported a statistically significant reduction in the number of days of mechanical ventilation, ICU LOS, and hospital LOS. 19 Research assessing the effectiveness of sepsis protocols has reported significant reductions in mortality. 20,21 Finally, massive blood transfusion protocols report significant reduction in 24-hour mortality in both blunt and penetrating trauma; a significantly reduced 30-day mortality rate was found in blunt trauma patients as well. 22 In summary, protocols positively impact patient care with reduced duration of mechanical ventilation, shorter LOS in the ICU and shorter overall hospitalization time, reduced mortality, and reduced health care costs. 2
While the beneficial effect of the implementation of individual protocols has been documented, none of the studies we found measured the impact of the implementation of several protocols simultaneously. One reason for not assessing the outcome of multiple protocols may stem from the difficulty of finding a common outcome variable to measure across different protocols. It is possible that increases in effectiveness and efficiency associated with protocolization of care can be attributed to the protocol’s ability to streamline clinical decision making. 6 If this is the case, implementing multiple protocols may have a cumulative effect across a defined group of patients with common clinical characteristics.
The following study was designed to assess the impact of the implementation of 4 patient care protocols within an elderly trauma population. We hypothesized that the implementation of these protocols would have a beneficial impact on patient care that could be measured by a decrease in hospital LOS. We also hypothesized the implementation of the protocols would reduce the amount of variability in the post protocol phase. The study was approved by the Iowa Health Des Moines Institutional Review Board (IRB).
Methods
Patient Population and Study Design
An archival, retrospective pretest/posttest study was performed on elderly trauma patients (≥65 years of age) admitted to a level 1 trauma center. The center is a receiving hospital for the central third of a Midwestern state, serving a medium-sized city as well as rural and isolated population areas. The Trauma ICU is staffed by 4 trauma surgeons who have primary responsibility for these patients.
All elderly patients with trauma who were seen during the time period of January 1, 2004 to December 31, 2009, were included in the study. The time frame was divided into a pre-multiple protocol implementation phase (pre-protocols: January 1, 2004 until December 31, 2006) and a post-multiple protocol implementation phase (post-protocols: January 1, 2007 to December 31, 2009).
Protocols, Protocol Implementation, and Protocol Compliance
During 2007-2009, the 4 protocols that were developed and implemented in the emergency department (ED) and the ICU are as follows.
Ventilator-associated pneumonia prevention protocol (VAP)
The goal of this protocol is to reduce the incidence of VAP by using more aggressive airway protection and clearance strategies for high-risk intubated patients in adult critical care. The strategies used include head of bed elevation, oral care every 4 hours, closed suction system for secretion removal, endotracheal tube with subglottic suction, and high-frequency chest wall therapy using a vest or manual percussors. Overall compliance with this protocol during the study time period met or exceeded 90% on each of the separate strategies that comprise the protocol.
Rib fracture protocol
The goal of this protocol is to involve the trauma team in the care of any patient who has at least 3 rib fractures or has fewer rib fractures but is high risk due to a fall that was higher than ground level or who is of age 65 or older. Compliance with the protocol during the study time period was 88.89%.
Massive blood transfusion protocol
When the blood bank is notified that the massive blood transfusion protocol is activated, the blood bank automatically begins production of coolers containing blood and blood products (fresh frozen plasma [FFP] and platelet pheresis) for delivery to the patient. Delivery continues until the physician discontinues the protocol. Compliance with the protocol during the study time period was 98%.
Anticoagulation protocol
Identifies any patient who was prescribed warfarin, clopidogrel, aspirin, or dipyridamole within the last 7 days. If the patient presents with hemodynamic instability, has a positive FAST examination, and has altered level of consciousness or intracranial hemorrhage (ICH) on head computed tomography (CT), the patient is given 2 units of thawed plasma and vitamin K. International normalized ratio (INR) is checked every 4 hours. Due to the fact that this protocol represents an algorithm with which to guide treatment, compliance measures were not recorded. We included this protocol in this study as it was implemented during the identified time period.
Statistical Methodology
All analyses were performed using IBM SPSS Statistics Version 19. The z ratio for the significance of the difference between 2 independent proportions was performed to determine differences in the patient populations across the 2 time periods. An α ≤.05 was used in all tests.
For the regression analyses only, patients who died within 48 hours of admission were excluded from the analyses. An a priori decision was made to create separate multiple regression models for each phase (pre-protocols and post-protocols). The premise for this decision was based on the fact that we hypothesized the implementation of the protocols would have an impact on LOS such that a linear relationship would be in question. Since one of the basic assumptions of regression is that a linear regression exists, a regression model incorporating both time periods would violate this basic assumption. We hypothesized a drop in LOS rather than a linear decline. Given this, the design of the study resembles that of a regression-discontinuity design which requires separate regression models for each phase of the study. 23
Results
Demographics, injuries, comorbidities, and diagnoses of the patient populations are shown in Table 1 . The number of patients potentially receiving care via each protocol can be found in Table 2 . Across the 2 time periods, there was a statistically significant decrease in the proportion of patients categorized as “other” or “unknown.” The only statistically significant difference within patient demographic characteristics was race, with the proportion of caucasian patients increasing from the pre-protocol phase to the post-protocol (z (2, 035) = 39.315, P < .05).
Demographic and Clinical Characteristics
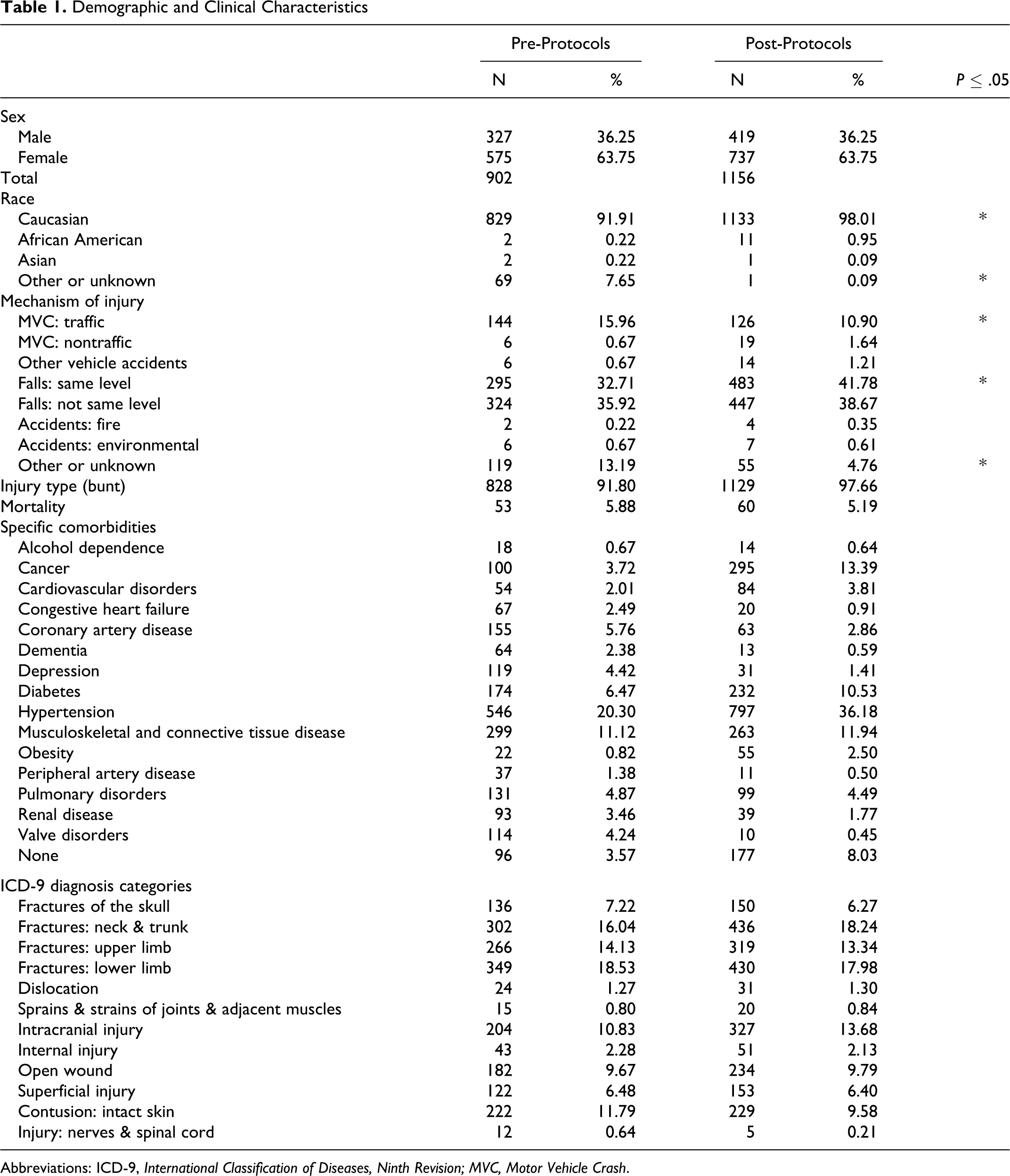
Abbreviations: ICD-9, International Classification of Diseases, Ninth Revision; MVC, Motor Vehicle Crash.
Number of Patients Receiving Care by Protocol

a Values in the pre-protocols phase represent patients that would have qualified for treatment via the protocol if the protocol were in place at that time.
From pre-protocols to post-protocols, there was a significant increase in the proportion of patients admitted due to a same-level fall (z (2, 035) = 4.165, P < .05) as well as a statistically significant increase in blunt trauma mechanism of injury (z(2, 035) = 6.003, P < .05) and a statistically significant increase in the proportion of patients who were intubated, z (2, 035) = 4.376, P < .0002). In addition, there was a significant decrease in the proportion of patients admitted due to motor vehicle crashes (z (2, 035) = 3.308, P < .05; see Table 1). Mortality was low and remained consistent across the time periods.
Table 3 displays admission clinical characteristics (ISS, Trauma Revised Injury Severity Score [TRISS], systolic blood pressure [SBP] and Glasgow Coma scale [GCS]) of the patients for both pre-protocol and post-protocol phases. Independent t tests were performed and revealed no significant differences among these variables. Table 3 also displays ICU and hospital LOS. There was no change in ICU LOS however there was a significant decrease (32%) in overall hospital LOS from pre-protocol to post-protocol phase (t (934) = 4.071; P < .01).
Admission Clinical Characteristics and Length of Stay
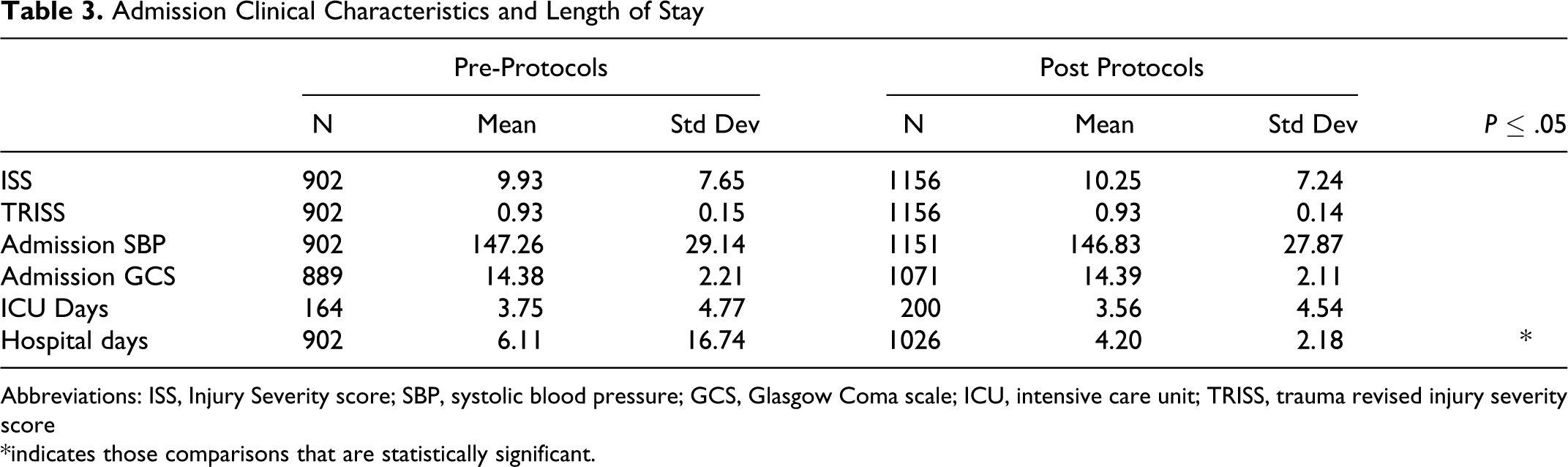
Abbreviations: ISS, Injury Severity score; SBP, systolic blood pressure; GCS, Glasgow Coma scale; ICU, intensive care unit; TRISS, trauma revised injury severity score *indicates those comparisons that are statistically significant.
Patient location after evaluation in the ED remained similar in all areas except for a significant increase in 23-hour observation from pre-protocols to post-protocols (z (2, 035) = 4.273, P < .05; see Table 4). Finally, Medicare as the primary method of payment increased significantly from pre-protocols to post-protocols (z (2, 035) = 6.441, P < .05), while automobile insurance (z (2, 035) = 3.003, P < .05) and Medicaid (z (2, 035) = 3.557, P < .05) both demonstrated a statistically significant decrease.
Discharge Disposition and Primary Payor
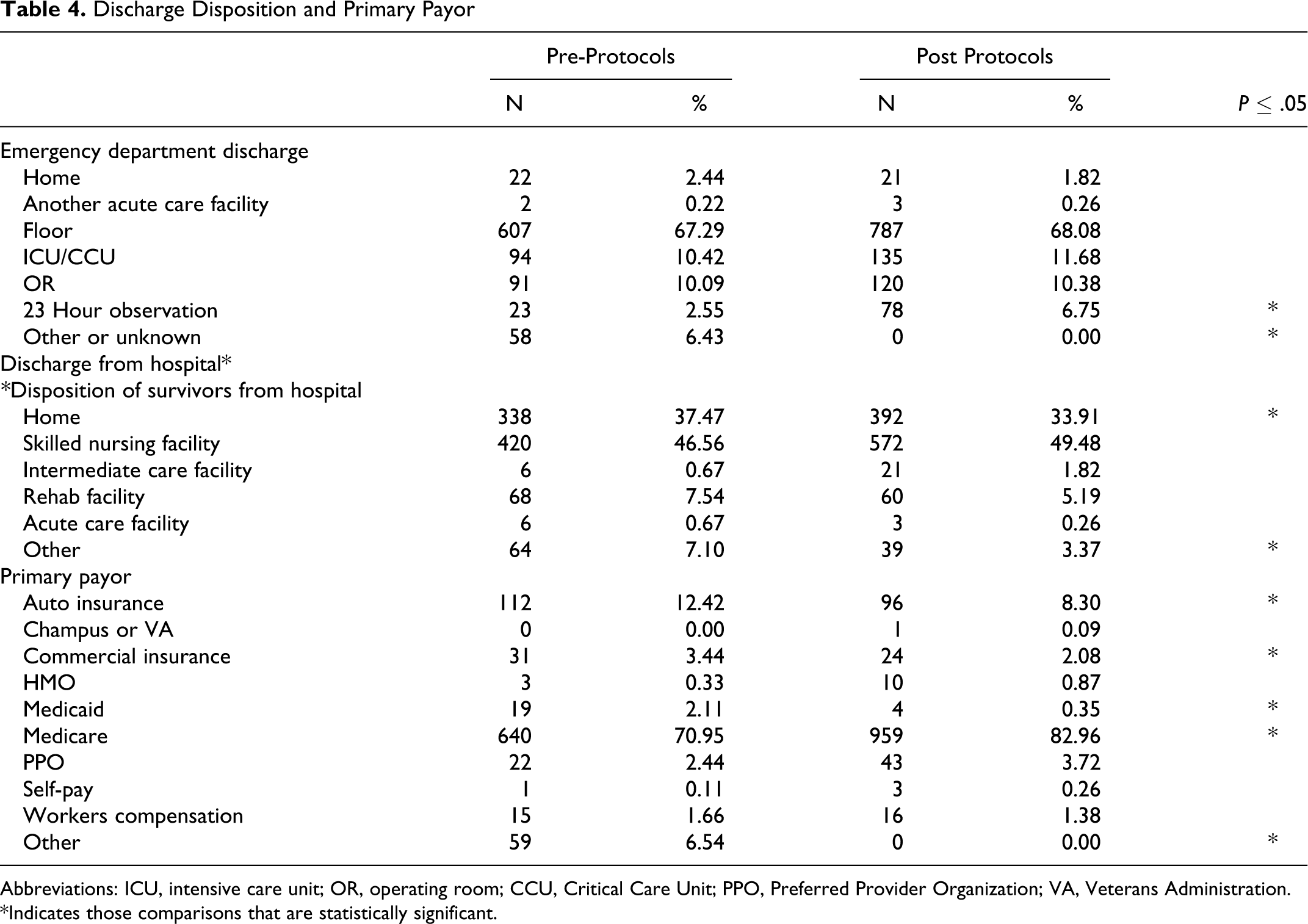
Abbreviations: ICU, intensive care unit; OR, operating room; CCU, Critical Care Unit; PPO, Preferred Provider Organization; VA, Veterans Administration. *Indicates those comparisons that are statistically significant.
A multiple regression model for each phase (pre-protocols and post-protocols) was subsequently performed to determine variables that would predict LOS within each time period. Variables included in the model were those identified in the research literature as having important predictive power for LOS and include age, sex, ISS, systolic and diastolic blood pressures at admission, primary medical insurance, and injury category. Tables 5 and 6 display the regression models for pre-protocol phase LOS and post-protocol phase LOS, respectively. In both phases, the overall model was statistically significant (pre-protocols: F (7, 839) = 3.712, P ≤ .001; post-protocols: F (7, 1081) = 20.608, P ≤ .0001). However, in the pre-protocol phase none of the variables in the model reached statistical significance. In the post-protocol phase, ISS and SBP at admission were both significant predictors of LOS.
Regression Model for Prediction of LOS: Pre-Protocols 2004-2006
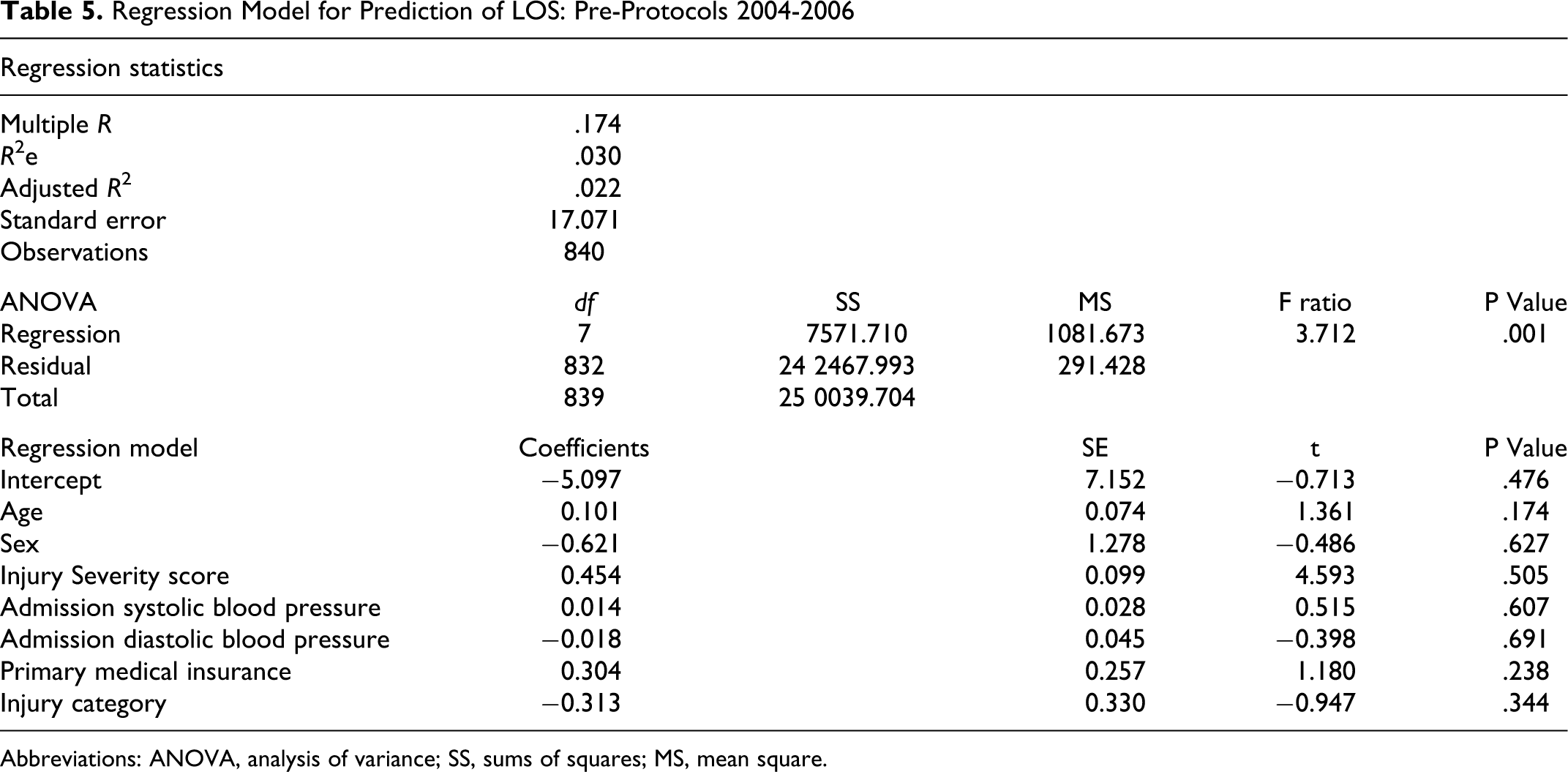
Abbreviations: ANOVA, analysis of variance; SS, sums of squares; MS, mean square.
Regression Model for Prediction of LOS: Post Protocols 2007-2009
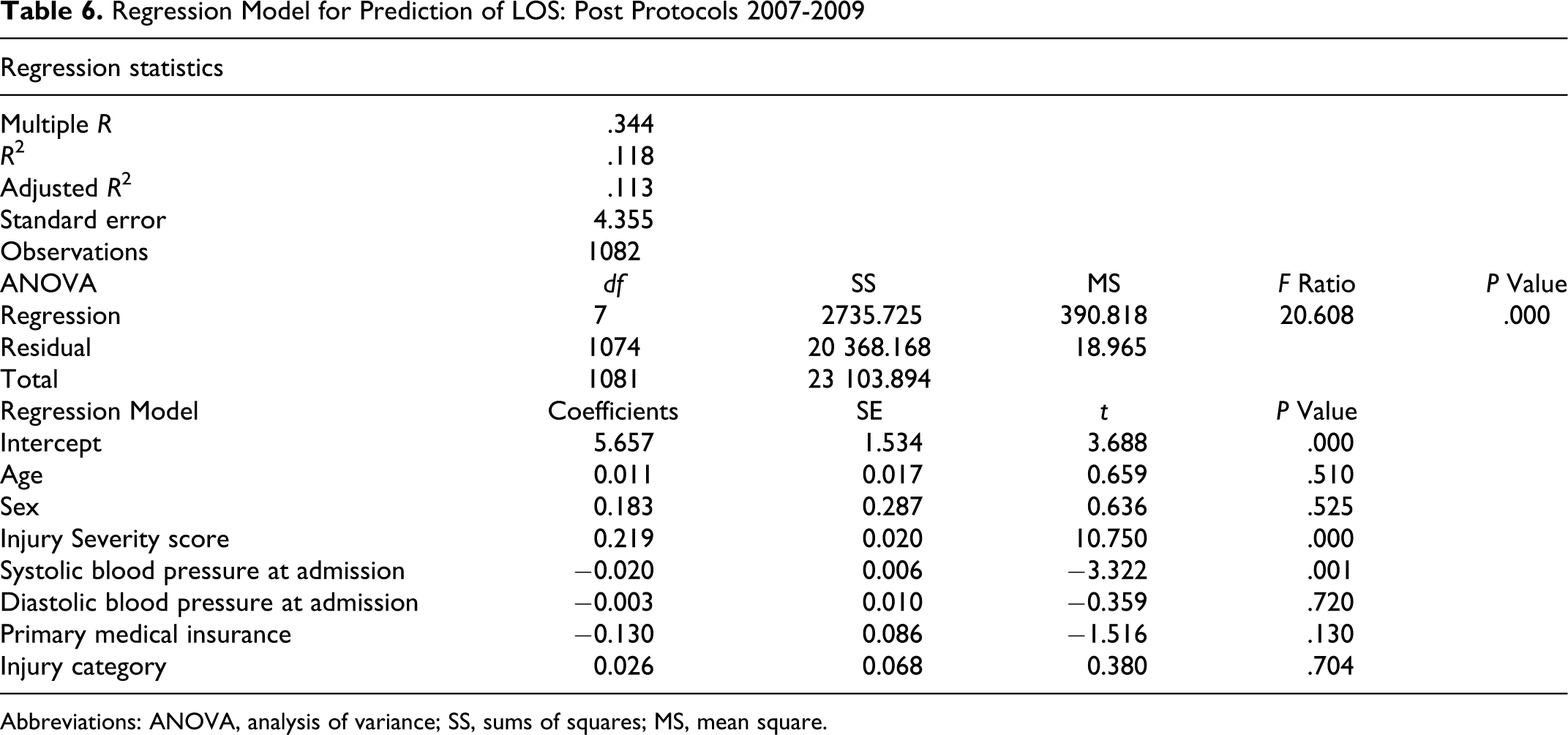
Abbreviations: ANOVA, analysis of variance; SS, sums of squares; MS, mean square.
In comparing the 2 regression models, we find the R 2 for pre-protocols was .03, with a standard error of 17.071. However, for the post-protocols the R 2 was .118, with a standard error of 4.355, suggesting the almost 4-fold decrease in the amount of error at the post-protocol phase may be responsible for increasing the predictive power of the post-protocol regression model.
Discussion
It has been established that traumatic injuries are poorly tolerated in the elderly population when compared with younger patients. Due to decreased physiological reserve, outcomes for this rapidly growing patient group, for example LOS, mortality, return to premorbid functional status, and so on are historically poorer. 2 –5 By using LOS as a proxy measurement of outcomes, the impact of specific interventions on these complex patients can be assessed and compared. A better understanding of what factors influence LOS, and a system for predicting LOS can be used to develop interventions shown to improve outcomes and enact them in a more standardized way.
The need to create consistency in practice and a more uniform approach to care in the ED and ICU provided the impetus for the development of these 4 new protocols in our institution. The new protocols, designed by physicians and staff using best evidence, helped guide practical changes in care that resulted in a 32% decrease in LOS for our elderly patients with trauma, this exceeds the 25% decrease found in other studies. 24 A reasonable question at this juncture would be “Was there a natural progression in reduction of LOS within the hospital compared to trauma patients?” Our answer to this question is no. As can be seen in Figure 1 , the overall LOS for the hospital remained stable across the study years while the LOS for trauma patients evidenced a step-down after the implementation of the protocols. While there was a decline in trauma LOS for 2005-2006, this decline was not statistically significant (P = .397). However, the decline between 2006 and 2007 (the shift from pre-protocols to post-protocols) was statistically significant (P = .012).
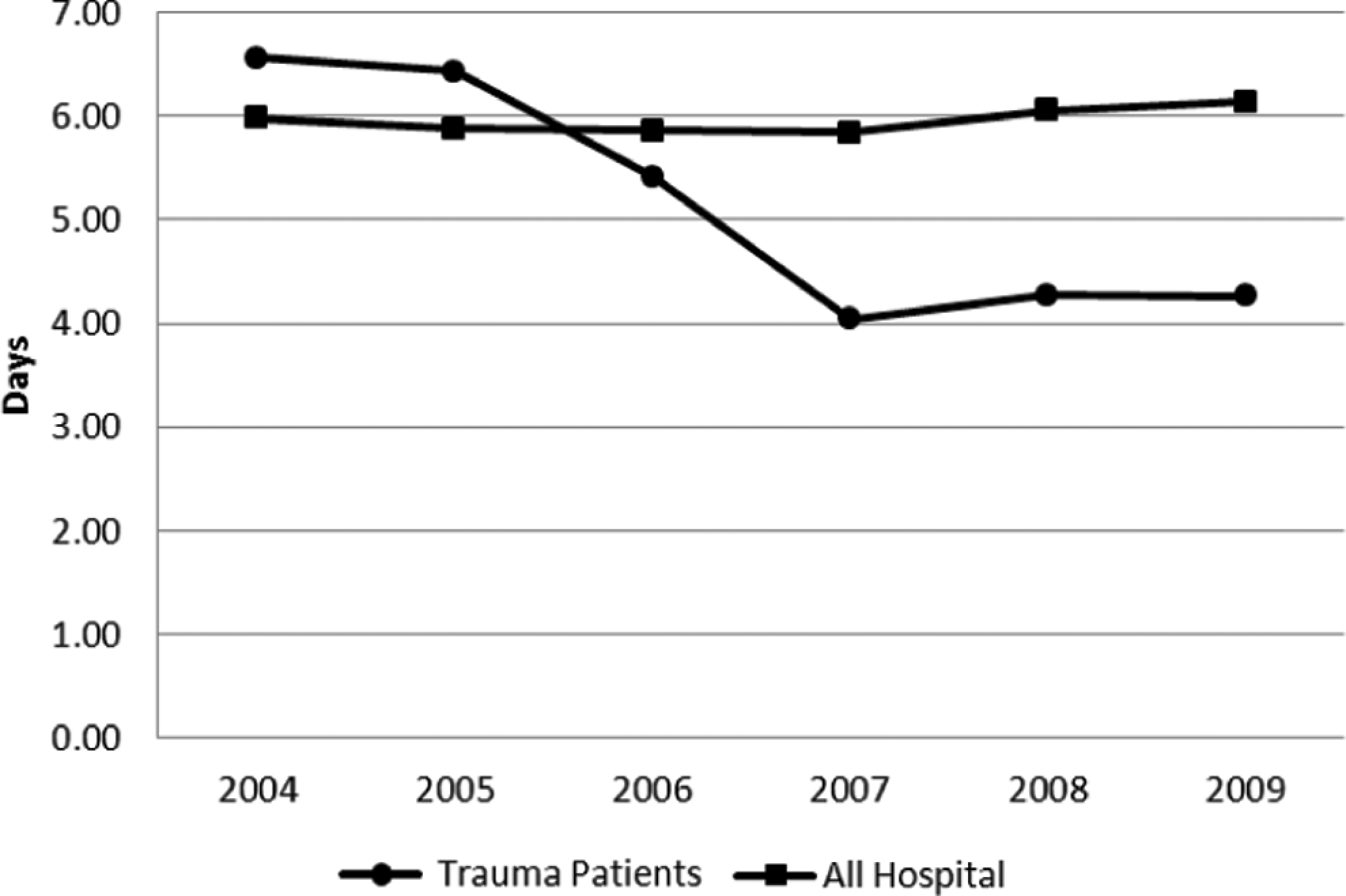
Hospital length of stay in patients of 65 years and older.
A secondary effect of the implementation of the 4 protocols appeared when the admissions and outcome data for the elderly patients with trauma were reviewed overall. In totality, variation in the data decreased from the pre- to post-protocol time periods, allowing a clearer picture of the factors affecting elderly patients' LOS to emerge. This finding is in keeping with the effects of protocols on clinical practice variation noted by other authors. 16,25 While the sample size in the post-protocol phase was larger (N = 1156) than the pre-protocol phase (N = 902), the likelihood of the unequal sample sizes being responsible for the differences in the 2 phases is small. While there is no doubt that sample size affects the distribution of variability, this impact plateaus at a sample size of about 600. 26
With less variation in our practices for ventilator management, massive transfusion, anticoagulation, and the care of patients with rib fractures, we now have the ability to better predict patients' LOS based on 2 specific variables: ISS and admission SBP. This finding supports past research that indicates higher ISS is one of the best predictors of mortality in the elderly individuals, 8,9,27 and that hypotension on admission is a late indicator of hemorrhagic shock and an independent predictor of mortality in patients with trauma. 28
It is important to note that during the study time period the patients admitted were not dissimilar in their demographics, comorbidities, and mechanisms and types of injuries. However, the “Other” category for each of the variables was less frequently used in the post-protocol phase than in the pre-protocol phase. We interpret these changes as evidence that an observation effect, similar to that of a “Hawthorne Effect” cannot be ignored. We speculate that the patient details necessary to determine whether or not the protocols would be implemented resulted in a spillover effect on the level of detail recorded in the patient chart. Consequently, it is possible that the implementation of the protocols resulted in increased vigilance for, or at least increased documentation of, these patient factors. While we did not test for this directly, we know of no other possible explanations.
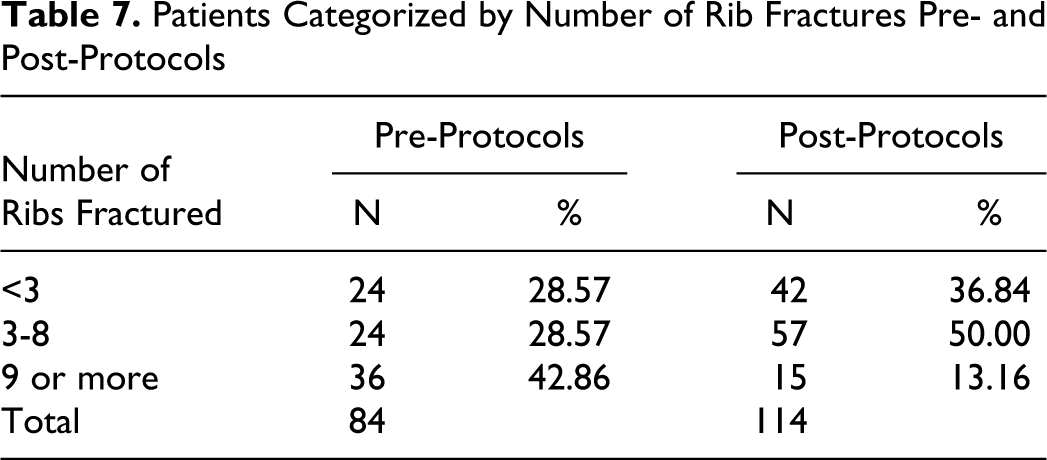
While in general there were no significant differences between the pre-protocol and the post-protocol groups, we noted a significant increase in the proportion of intubated patients in the post-protocol group. This finding was unexpected, especially given the observed decrease in LOS and the decrease in the percentage of VAPs (both of which are reasonably affected by mechanical ventilation). In an attempt to explain this finding, we conducted a post hoc analysis of intubated patients in both study groups. We hypothesized that the rib fracture protocol might have resulted in increased triage of elderly patients with rib fractures to the trauma service, leading to a higher number of post-protocol patients whose injuries required ventilator support. As can be seen in Table 7 , the number of patients with rib fractures (identified by an International Classification of Diseases, Ninth Revision [ICD-9] code of 807.01-807.09) reveals an increase in the number of patients with rib fractures post-protocols. Table 7 also reveals the number of patients in the 1 to 3 rib and 3 to 8 rib fracture groups both increased post-protocol, but the number of patients with 9 or more rib fractures dropped. We have several potential explanations for this finding. First, the rib fracture protocol is designed to triage patients who have 3 or more rib fractures to the trauma service. However, it also explicitly triages patients with fewer rib fractures to the trauma service in the presence of other risk factors (one of them is aged greater than 65). It is possible that the increase in intubated patients is due to appropriate patient identification and triage. Second, the decrease in the number of elderly patients with more than 9 rib fractures may not have had the expected effect on the number of ventilated patients in general. Severely injured elderly patients may have previously expressed their desire to avoid prolonged mechanical ventilation via “living will.” This introduces the possibility that these patients or their proxy decision makers have declined mechanical ventilation from the outset. Third, it is also possible this is a further demonstration of a Hawthorne Effect in that the increased attention to detail resulting from the introduction of the rib fracture protocol led to more careful documentation of the number of rib fractures by providers.
Patients Categorized by Number of Rib Fractures Pre- and Post-Protocols
This study is not without its weaknesses. Due to the fact that the 4 protocols were not implemented independently from each other, we were not able to determine the incremental LOS effect of each protocol. The pre- and post-protocol groups were assessed for outcomes in a global manner, without close scrutiny of how often any given protocol was applied to the patients in the post-protocol group. It is therefore also not clear how much of the decreased variation was due to the implementation of any given protocol.
Again, it is notable that even though more patients were intubated in post-protocol, the overall LOS decreased, as did the percentage of VAPs. While it is difficult in general to determine whether decreased LOS results in decreased hospital-acquired complications, or vice versa, in the specific case of mechanical ventilation and VAP, it is reasonable to conclude that the proportional decrease in VAP contributed to the reduction in overall LOS. It is tempting to further speculate that the rib fracture and VAP protocols interacted synergistically by identifying patients who would be at highest risk of intubation and triaging them to receive preventive measures targeted at the most frequent complication of intubation.
Conclusion
The protocols implemented in this study were well tailored to the environment and culture of our ED and ICU. Feedback regarding their ease of use and observed effects were welcomed from the outset. Acceptable levels of compliance with their use were achieved. As a consequence, a 32% decrease in LOS was exhibited. While we cannot deny the possibility of a Hawthorne Effect in the study, we can report that the protocols have become culturally ingrained with the patient care teams. The protocols are rapidly becoming second nature to staff physicians and residents; the latter of whom are trained using these methods and may adopt and adapt them to benefit their future practices. If the results were due only to a Hawthorne Effect, the use of the protocols should have dissipated over time rather than become embedded into patient care. Planned future research projects will be geared toward assessing the effects and impacts of each of the protocols individually. There may also be underlying significance present in the outcomes of patients who required the use of more than one protocol due to their specific injury or comorbidity patterns.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.